OSCE FINDINGS
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
clubbing causes cardiac
cyanotic congenital HD
infective endocarditis
atrial myxoma
clubbing causes resp
ILD
cancer
CF
empyema
bronchiectasis
clubbing causes GI
IBD
hepatic cirrhosis
GI lymphoma
coeliac
pitting oedema causes
raised venous pressure
right sided HF
chronic venous insufficiency
volume overload/ renal failure
pregnancy
obesity a/w Na/ H2O retention
reduced oncotic pressure/ hypoalbunemia
nephrotic syndrome
cirrhosis/ liver failure
protein losing enteropathy (i.e IBD)
drugs
calcium channel blockers
long term corticosteroids
NSAIDS
non pitting oedema causes
hypothyroid/ graves disease
malignancy
radiotherapy
lymph node clearance
how to present a stoma
site
number of lumen
spout/ flush with skin or out
nature of effluent
state of surrounding skin
evidence of complication
likely type of stoma
possible procedure/ underlying pathology
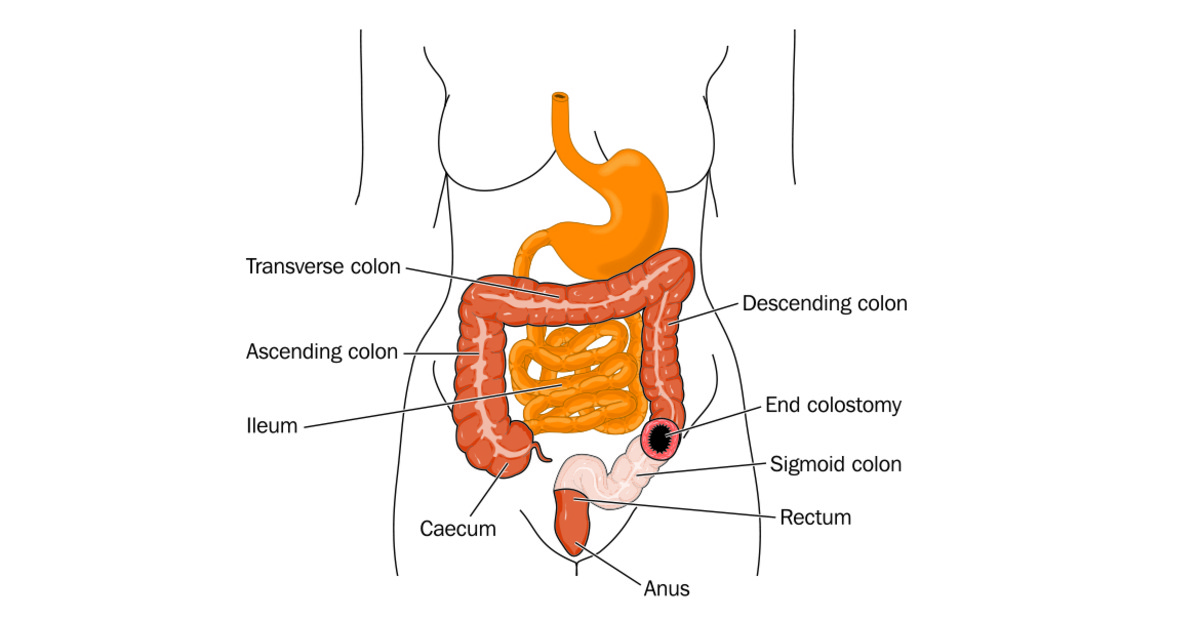
end colostomy stoma
left sided
1 lumen
no spout
effluent; hard stool
surg; hartmann w/ rectum oversewn OR abdomino perineal resection
if still pass stool; hartman, higher tumour
end ileostomy stoma
right sided
1 lumen
spout
effluent; soft/ liquid stool
surg: subtotal colectomy / panproctocolectomy (UC)
loop ileostomy stoma
usually temporary
right sided
2 lumens (joined)
spout
effluent; soft/ liquid stool
surg: to defunction chrons/ obstruction (malignancy)/ newly formed anastomosis
loop colostomy stoma
usually temporary
upper abdomen
2 joined luemns
no spout
effluent is hard stool
surg: to defunction chrons/ obstruction (malignancy)/ newly formed anastomosis
end colostomy and mucous fistula stoma
usually left sided
2 separte lumen
no spout
effluent; hard stool
surg; hartmann procedure with rectum brought to skin
urostomy stoma
can be on either side
1 lumen
spout
effluent; urine
surg; cystectomy (malignancy)
stoma complications
haemorrhage
necrosis
prolapse
retraction
obstruction
peristomal skin inflammation
parastomal hernia
high outpout
indirect inguinal hernia
passes through inguinal canal ring → inguinal canal → external ring
superior to pubic tubercle
extension into scrotum is common
can be very large
usually reducible
held by pressure on deep ring
low risk of complication
usually repaired as impossible to differentiate between direct hernia on clinical exam alone
direct inguinal hernia
through weak point in posterioir wall of inguinal canal (hesselbach triangle → inferioir epigastric artery, inguinal ligament and lateral border of rectus muscle)
superioir to pubic tubercle
rarely extennd in scrotum
moderate size
almost always reducible
not held by pressure on deep ring
moderate risk of incarceration and complication
surgical repair
femoral hernia
through femoral canal and underneath inguinal ligament
inferior tu pubic tubercle
cannot extend in scrotum
3-5cm
rarely reducible (absent cough impulse)
not held by pressure on deep ring
high risk of strangulation
urgent surgical repair
types of hernia repair
open mesh
open suture
laparoscopic
hernia risk factors
family history
older age
surgery
obesity
pregnancy
constipation
heavy lifting
causes cerebellar lesions
stroke
tumour
MS
alcohol abuse/ thiamine deficiency (wernicke encephalopathy)
anti epileptic meds
friederich’s ataxia
classic signs cerebellar lesions
DANISH
dysdiadochokinesis
ataxia
nystagmus
intention tremor
slurred/ staccato speech
hypotonia
signs central cerebellar lesions
truncal ataxia standing and sitting
poor heel-toe
slurred staccato speech
signs cerebellar hemisphere lesion
ipsilatral limb ataxia
nystagmus
unsteady gait
CNI palsy
olfactory
poor smell/ changes in smell
causes
trauma
meningitis
frontal lobe tumour
CNII palsy
optic
snellen chart
visual fields
light torch test
fundus w/ ophtalmoscopy
causes
mono ocular; MS
bitemporal; pituitary adenoma, internal carotid artery aneurysm
homonymous hemaniopia; stroke/ tumour/ abscess
CN III/ IV/ VI palsy
oculomotor/ trochlear/ abducens
eye movements
accomodation
CN V palsy
trigeminal
sensory; face
motor; jaw opening against resistance/ masseter muscle palpation when clenching
causes
idiopathic trigeminal neuralgia
acoustic neuroma
herpes zoster
CN VII palsy
facial
facial expressions
causes
bell’s palsy
parotid tumour
herpes zoster
sarcoid
stroke
CN VIII palsy
vestibulocochlear
occlude other ear and ask patient to repeat other word behing them
rinne
weber
causes
excessive noise levels
gentamycin
furosemide
CN IX/ x/ XII palsy
glossopharyngeal/ vagus/ hypoglossal
open mouth and say ahhh → deviate away from weakness
swallow water
stick tongue out → deviate toward weakness
causes
diptheria
polio
GBS
myasthenia gravis
MS
strokes
CN XI palsy
accessory
shrug shoulders vs resistance
turn head against resistance
CN III palsy causes
oculomotor
spared pupil; diabetic
complete; PCA aneurysm/ raised ICP w/ tentorial herniation
CN IV palsy causes
rare
trochlear
orbit trauma
CN VI palsy causes
abducens
petrous temporal bone fracture
nasopharyngeal carcinoma
raised ICP