O&G
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
1.most common places for ectopic pregnancy
2. risk factors
3. assessment/investigations ( assuming haemodynamically stable)
1. Tubal - ampulla of fillopian tube 70% , isthmus 12%, non tubal rare
2. Tubal damage / altered motility
prev ectopic, PID, pelvic surg, maternal age >35, smoking, endometriosis, IUD
3.
-physical exam,
- hx,
-transvaginal US - BHCG 1500-3000 gestational sac should be present , if empty uterus ectopic until proven otherwise
- beta HCg every 48hrs - >53% rise is normal ( slow or fall indicates ectopic)
1.clinical features of ectopic pregnancy
2. treatment
1. lower abdominal guarding/ pain ( similar presentation to appendicitis) colicky -> constant, +-PV bleeding, symptoms of pregnancy, shoulder tip pain, hypotension, taccy, presyncope, rebound tenderness -suggest rupture
2.
- expectant managment - requires b-hcg until 0
Medical management
- methotrexate ( not on live ectopic) bHCG <5000
- SE's avoid alcohol and folate, abdopain, photosensitivity
surgical management
- salpingectomy ( surgical laparoscopy) indicated in haemodynamically instabilty/ ruptured
ovarian torsion
1.definition of ovarian torsion
2.epidemiology
3.risk factors
1. twisting of the ovary around adnexal ligaments
2. child bearing age women
3. ovary enlargement : cysts, tumours,PID, pregnancy, laxity of pelvic/suspensory ligament, strenuos exercise
ovarian torsion
1. presentation
2. assessment
3. mangement of ovarian torsion
1. sudden onset unilateral lower abdominal pain( can fluctuate - intermittent torsion), nausea vomiting, +- palpable adnexal mass
2. ultrasound :
- symmetrical ovariaes of normal volume, torsion unlikely
- absence of doppler flow is late sign of torsion
3. emergency exploratory laparoscopy - adnexal detorsion
aetiology and high risk age group for PID
upper gential tract infection which can cause endometriosis, perotinitis, salpingitis, tubo-ovary abcess
pathogens : chlamydia trachomitis , gonorrhea neisseria
high risk age group - 16-24
epidemiology - 18-44
PID
1. risk factors
2. assessment
3. treatment
4. complications
1. multiple sexual partners, STIs, vaginal douching, unprotected sex, IUDs
2. bimanual exam - cervical motion tenderness minimum criteria ( low threshold for diagnosis), adnexal tenderness
clinical diagnosis
3. remove infection - empiric antibiotics ( start if PID suspected), STI screen,
counselling, follow up, partner screening, no intercourse
4. infertility , chronic pelvic pain , ectopic pregnancy
cord blood tests at delivery
cord blood tests at delivery:
fetal blood group ( check for rhesus D +)
antibodies attached to fetal red cells - coombs test
fbc
bili rubin - only if severe
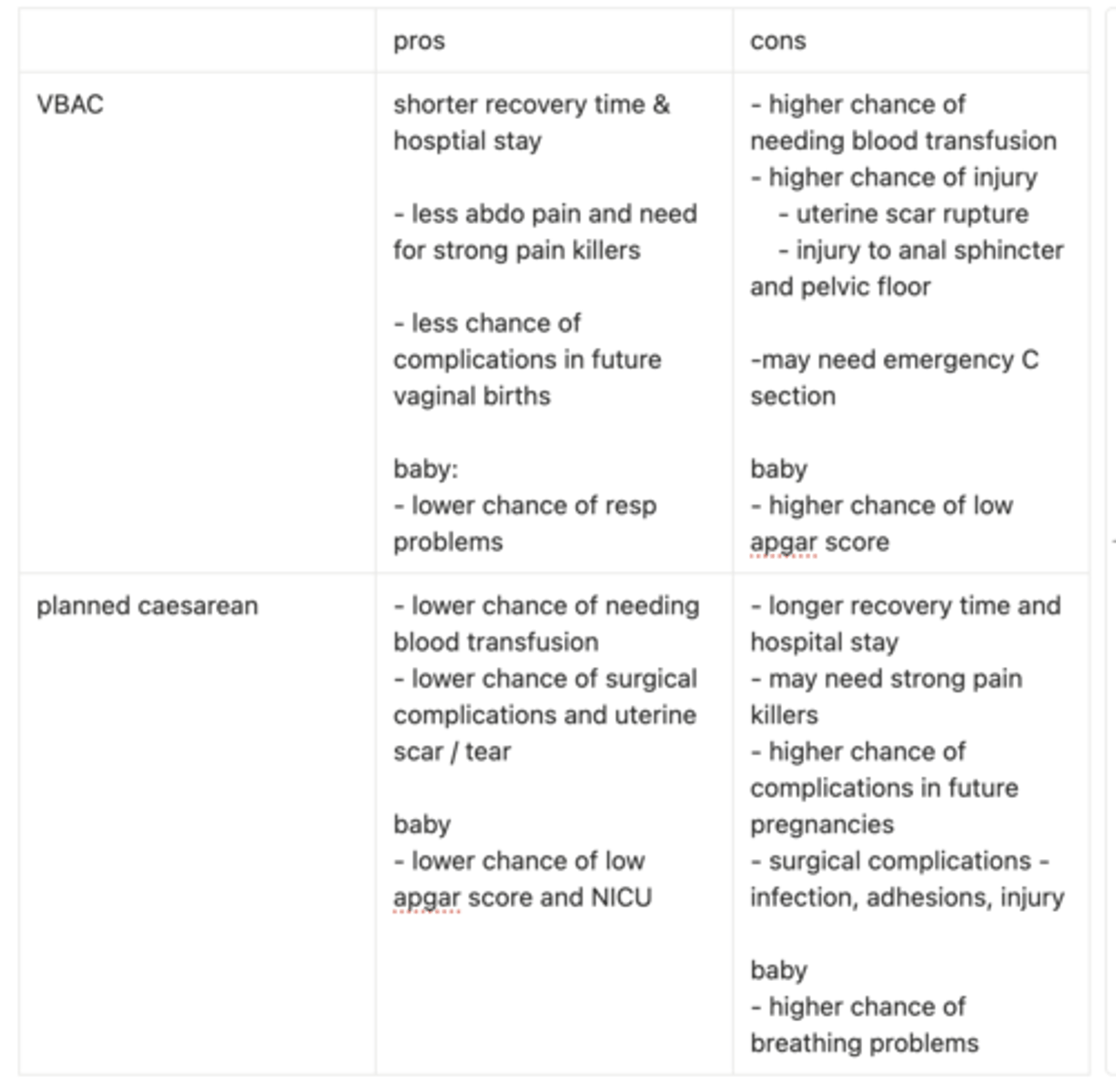
complications of VBAC
complications of VBAC
1. uterine scar rupture influence by type of cesarian ( high uterine, inverted T or low vertical uterine) and labour inducing medications
2. chance of needing assisted birth - forceps
3. chance of emergency c section
4. risk of injury to perineum and/or pelvic floor
suitabiltity for VBAC
factors supporting and against
supportive factors
- previous vaginal birth
- c section was due to breech or non head down postion
- c section was not from prolonged labour due to maternal hypertension or preterm birth
factors resulting in higher likely hood of emergency C section
- labour augementation ( meds to help speed up labour)
- BMI >40 at start of pregnancy
- gestational diabetes
- age >35
- baby size > average gestational age
pros and cons VBAC vs planned caesarean
don’t forget general surgical complications
5 common genetic screenings and purpose for screening
1.CF
2. spinal muscular atrophy
3. fragile x
4. thalassemia
5. sickle cell
6. duchenne/becker muscular dystrophy
tests persons DNA to pathogenic variants, identifies reproductive risk, allows informed choices ( IVF, preparation, termination), reduce risk and mortality from congenital born disease
what are the principles of Autosomal recessive genetic inheritance
both parents carriers = 25% affected, 50% carriers, 25% unaffected
e.g CF, SMA, thallesemia
prenatal testing for both parents
what are the principles of Autosomal dominant genetic inheritance
one affected parent = 50% chance of affected child
e.g marfans, huntingtons
what are the principles of x linked recessive recessive genetic inheritance
* affects sons more ( male to male transmission cannot occur)
- carrier mother = 50% affected sons, 50% carrier daughters
- carrier father = carrier daughters, no affected sons
e.g duchenne, haemophilia A
what are the principles of x linked dominant genetic inheritance
- Affected mothers → 50% affected children
- Affected fathers → all daughters affected, no sons affected
Examples: Fragile X syndrome
Card 1 — Physiology of Labour
Q:What hormonal and mechanical factors initiate and maintain labour?Include roles of oxytocin, prostaglandins, Ferguson reflex, and myometrial gap junctions.
A:
Prostaglandins (PGE2, PGF2α) soften and ripen the cervix + increase uterine contractility.
Oxytocin from the posterior pituitary increases contraction strength; also stimulates prostaglandin release.
Ferguson reflex: fetal head stretches cervix → ↑ oxytocin → ↑ contractions (positive feedback).
Myometrial gap junctions increase → coordinated contractions across uterus.
Stages of Labour
Q:What are the three stages of labour, and what defines the latent vs active phase of Stage 1?
A:
Stage 1: Onset of contractions → full dilation.
Latent: ≤4 cm dilation, painful contractions.
Active: ≥5 cm dilation, painful regular contractions, rapid cervical change.
Stage 2: Full dilation( 10cm) → delivery of baby (passive + active/pushing phases).
Stage 3: Delivery of baby → expulsion of placenta (physiological or active management).
Stage 4: monitor for PPH or preeclampsia
Q:What are the key management steps during the first stage of labour?
A:
- Offer analgesia on request.
- CTG (intermittent or continuous).
abdo exam
- Assess fetal position/lie ( if unclear use ultrasound)
how many 5ths palpabable is the head ( 2/5ths means engaged with pelvis)
ask about fetal movements
- vaginal exam
BISHOP
cervix effacement
station of baby ( 0 = at level of ishial spines)
hardness/soft consistency of cervix?
opening- how dilated
position of uterus - retro(-1 point) or anterverted
Q:What are the key management steps during the second stage of labour?
A:
Assist the mother to find comfortable, safe positions for pushing.
Guide fetal delivery through the vaginal canal (support cardinal movements).
Delay cord clamping for at least 30–60 seconds.
Q:What are the key steps in active management of the third stage of labour ( delivery of placenta)
A:
Active management reduces risk of postpartum haemorrhage.
Give oxytocin → increases uterine tone, reduces blood loss.
Perform controlled cord traction (Brandt–Andrews manoeuvre) if placenta not delivered spontaneously.
Inspect placenta for complete cotyledons, intact membranes, and three cord vessels (1 vein, 2 arteries).
Repair any obstetric lacerations.
Normal Labour Progress
Q:What characterises normal progress in the first and second stages of labour?
A:
First stage: Steady cervical dilation from 5 cm onward; contractions become stronger/closer; progressive fetal descent.
Second stage: Descent + rotation → effective pushing; delivery within ~2 hr nulliparous, ~1 hr multiparous (longer acceptable if maternal/fetal status reassuring).
Abnormal Labour Progress
Q:What defines slow/arrested labour in Stage 1 and Stage 2?What are common causes?
A:
Stage 1 slow labour: <2 cm dilation over 4 hr after reaching ≥5 cm.
Stage 2 arrest: No descent despite adequate contractions/pushing.
Causes (3 Ps):
Power: inadequate contractions
Passenger: malposition (OP, asynclitism), macrosomia
Passage: cephalopelvic disproportion (CPD)
list pharm and non pharm pain relief options during labour
risks of opioids and epidural
A: non pharm
Support / continuous labour companion → reduced fear; improved coping.
Water immersion → buoyancy, relaxation.
TENS → gating pain pathways.
Hypnobirthing, breathing, relaxation → reduces sympathetic tone.
Heat packs, massage, position changes → reduce muscle tension and improve comfort.
A: pharm
Nitrous oxide: quick, self-administered; mild analgesia.
Opioids (morphine, fentanyl): moderate analgesia; cross placenta → neonatal resp depression.
Epidural: most effective; risks: hypotension, prolonged second stage, instrumental birth.
Pudendal block / local infiltration: used in second stage or for instrumental birth.
4 components of CTG and etiology of FHR alterations
Baseline rate,
- 110 -160 bpm
Variability
- reduced or absent = concerning
Accelerations
- >2 accerlations over 20 mins = reactive FHR tracing
Decelerations.
- a temporary decline in the FHR of > 15 bpm for a maximum duration of 3 minutes
VEAL CHOP
Variable decelerations→ Cord compression/prolapse
Early decelerations→ Head compression
Accelerations→ OK
Late decelerations→ Placental insufficiency/Problem
Maternal Indications for Unplanned Caesarean
Q:List maternal reasons for unplanned intrapartum caesarean.
A:
-Failure to progress (Stage 1 arrest or Stage 2 arrest).
-Obstructed labour (CPD, shoulder dystocia ).
-Maternal exhaustion inhibiting progress.
-Severe maternal illness (eclampsia, haemorrhage, sepsis).
Fetal/Placental Indications
Q:List fetal and placental indications for unplanned caesarean delivery.
A:
-Abnormal CTG / non-reassuring fetal status.
-Failed instrumental delivery.
-Malpresentation (transverse, brow, unstable lie).
-Cord prolapse.
-Significant placental abruption.
-Vasa praevia with bleeding.
fetal and maternal life threatening complications of delivery
Life-threatening complications
-Prolonged second stage of labor
- Obstructed labor, e.g., due to shoulder dystocia
- Umbilical cord complications,
including nuchal umbilical cord
- Uterine rupture
- Uterine inversion
- Postpartum hemorrhage
- Amniotic fluid embolism
perineal tear laceration classification
1 - cutaneous to subcutaenous - no involvement of perineal muscles
2 - 1st degree plus laceration to perineal muscles
3 - 2nd degree plus involvement of external (+- internal) sphincter ( may lead to faecal incontinence)
4 - 3rd degree plus laceration to anal mucosa
Treatment for perineal lacerations 1& 2nd stage vs 3rd & 4th
complications of 3rd & 4th stage repairs
1st & 2nd
Conservative - nsaids & sitz baths
suture - local anesthesia - continous sutures or surgical glue
3rd & 4th
regional or GA used
reconstructive surgery
Complications Primarily associated with third- and fourth-degree lacerations.
- Pain and dyspareunia
-Rectovaginal fistulae
-Hemorrhage
- Infection
-Wound dehiscence
Prevention: application of warm compress to perineum during delivery
epidemiology and risk factors for perineal tears
Epidemiology: most common obstetric injury of the pelvic floor
Risk factors
-Macrosomia
- midline episiotomy
-Forceps delivery
-No previous delivery
-Prolonged second stage of labor
-Occiput posterior delivery
-Rapid delivery of head in breech presentation
-Head extension before crowning
-Lack of perineal elasticity (e.g., perineal edema)
define gestational hypertension vs preeclampsia vs eclampsia
Gestational hypertension = new BP ≥140/90 mmHg after 20 weeks with no proteinuria or end-organ dysfunction.
Pre-eclampsia = new hypertension plus either proteinuria, or maternal organ dysfunction, or foetal growth restriction/placental dysfunction
Eclampsia = generalised tonic-clonic seizures in a woman with pre-eclampsia, not explained by another neurological cause.
* chronic hypertension = hypertension during pregnancy present <20 weeks
List major maternal complications of pre-eclampsia.
Eclampsia, HELLP syndrome, AKI, pulmonary oedema, DIC, placental abruption, stroke/cerebral haemorrhage, ICU admission, increased long-term CV risk.
what is HELLP syndrome
What is the cure?
what siezure prophylaxis is given in this condition along with eclampsia?
Preeclampsia with thrombotic microangiopathy involving the liver
HELLP = Hemolysis, Elevated Liver Enzymes, and Low Platelets
(clots in liver causing liver dysfunction -> liver failure, DIC)
cure = delivery of placenta
IV magnesium sulphate 4mg infusion over 20 mins
List major fetal complications of hypertensive disorders of pregnancy.
Fetal growth restriction
Preterm birth
Seizure-induced fetal hypoxia
Fetal death
oligohydramnios ( amniotic fluid lower than normal = poor nourishment - premature birth)
Q:What investigations are required for a pregnant patient with new hypertension?
BP measurement:
Urinalysis: urine protein:creatinine ratio (uPCR) or 24-hr protein if required
- uPCR ≥30 mg/mmol = proteinuria
Bloods: FBC (platelet count), renal function (creatinine, electrolytes), LFTs
Foetal assessment: CTG if concerns,
Baseline observations: fluid balance, oxygenation, neurological status.
Q:What antihypertensive agents are used in pregnancy, and when do you urgently treat?
A:Urgently treat BP ≥160/110 mmHg.
First-line agents:
Hypertensive Moms Need Love
hydralazine (IV) - urgent
Methyldopa for chronic BP control ( oral)
nifedipine (oral IR),
labetalol (IV/oral) - urgent
prophylaxis for high risk pre eclampsia
aspirin 100-150mg daily ( racgp guidelines)
initiated between 12-28 weeks gestation
delivery plan/timing in hypertensive Pregnancy disorders
- immediate stabilisation for patient with preeclampsia with severe featuers, eclampsia or HELLP
-assess gestational age:
Severe pre-eclampsia ≥34 wks → deliver after stabilisation.
Severe pre-eclampsia <34 wks → intensive monitoring; deliver if maternal/fetal deterioration.
Mild pre-eclampsia ≥37 wks → deliver.
Gestational hypertension → expectant management until term unless it progresses.
Q:What are the key steps in the acute management of eclampsia?
ABCs + left lateral position + oxygen
Magnesium sulfate (4 g IV loading, then 1 g/h infusion; repeat 2 g if seizure recurs)
Control severe BP ≥160/110 with labetalol/nifedipine/hydralazine
- Monitor for mag toxicity
- reflexes, respiratory rate, urine output; have calcium gluconate ready
-Blood tests (FBC, LFTs, renal function, coagulation)
- Plan delivery once stabilised (definitive treatment)
pathophys of preeclampsia
abnormal placental invasion/ development -> hypoperfused placenta releases inflammatory cytokines and anti angiogenic factors systemically
-Capillary leak (→ oedema, pulmonary oedema)
-Vasoconstriction (→ hypertension)
-Platelet activation & microangiopathy (→ HELLP, organ dysfunction)
-Cerebral endothelial dysfunction → impaired cerebral autoregulation , disruption of BBB- cerebral oedema- eclampsia
Q: What is the definition of primary and secondary postpartum haemorrhage?
A:
Primary PPH:
≥500 mL blood loss in first 24 hrs postpartum
≥ 100mls after c-section
or any blood loss causing haemodynamic instability.
Secondary PPH: Abnormal bleeding from 24 hrs to 6 weeks postpartum
Q: What are the 4 Ts causes of PPH, and what do they represent?
A:
Tone: Uterine atony - cant contract/compress vessels (most common ). prolonged labour, mag sulfate, overdistended uterus, infection 70-80%
Tissue: Retained placenta, membranes, cotyledons, clots. 10%
Trauma: Genital tract tears, episiotomy, uterine rupture. 10-20%
Thrombin: Coagulopathy (DIC, pre-eclampsia, HELLP). 1-4 %
Q: What are key strategies for PPH prevention and early recognition?
A:
Prevention: Active management of third stage — oxytocin, controlled cord traction, uterine massage.
Recognition: Quantify blood loss, monitor vitals, assess uterine tone, inspect genital tract, recognise boggy uterus or persistent bleeding.
Q: What is the stepwise management of PPH?
A:
1.Call for help, ABCDE, 2x large-bore IV access, fluids ( warmed crystalloid), bloods ( FBC, coags, fibrinogen, group and hold).
2.Identify 4 Ts, empty bladder, uterine massage.
3.Uterotonics: oxytocin → ergometrine ( not in hypertension) → carboprost (not in asthma)→ misoprostol.
4. Tranexamic acid (1 g IV) within first 3 hours, repeat after 30mins if still bleeding .
5. Mechanical measures: bimanual compression, balloon tamponade.
6. Surgical/IR: EUA + repair tears, manual removal, curettage, uterine artery ligation, B-Lynch sutures, uterine artery embolisation, hysterectomy.
Q: What are the indications for surgical intervention in PPH?
A:
Failure of uterotonics + mechanical methods + TXA.
Retained placenta/products needing removal.
Genital tract trauma requiring repair.
Suspected placenta accreta spectrum or uterine rupture.
Life-threatening haemorrhage → peripartum hysterectomy if conservative measures fail.
Q: What are the indications for blood transfusion in PPH
A:
Ongoing significant bleeding or haemodynamic instability.
Hb <70 g/L (or higher threshold if symptomatic).
FFP: INR >1.5 or massive haemorrhage.
Platelets: <50 ×10⁹/L with bleeding.
Cryoprecipitate: Fibrinogen <2 g/L or DIC
Massive transfusion protocol if large/rapid blood loss.
- plus calcium
ratio 1 RBC: 1 FFP : 1 platelets
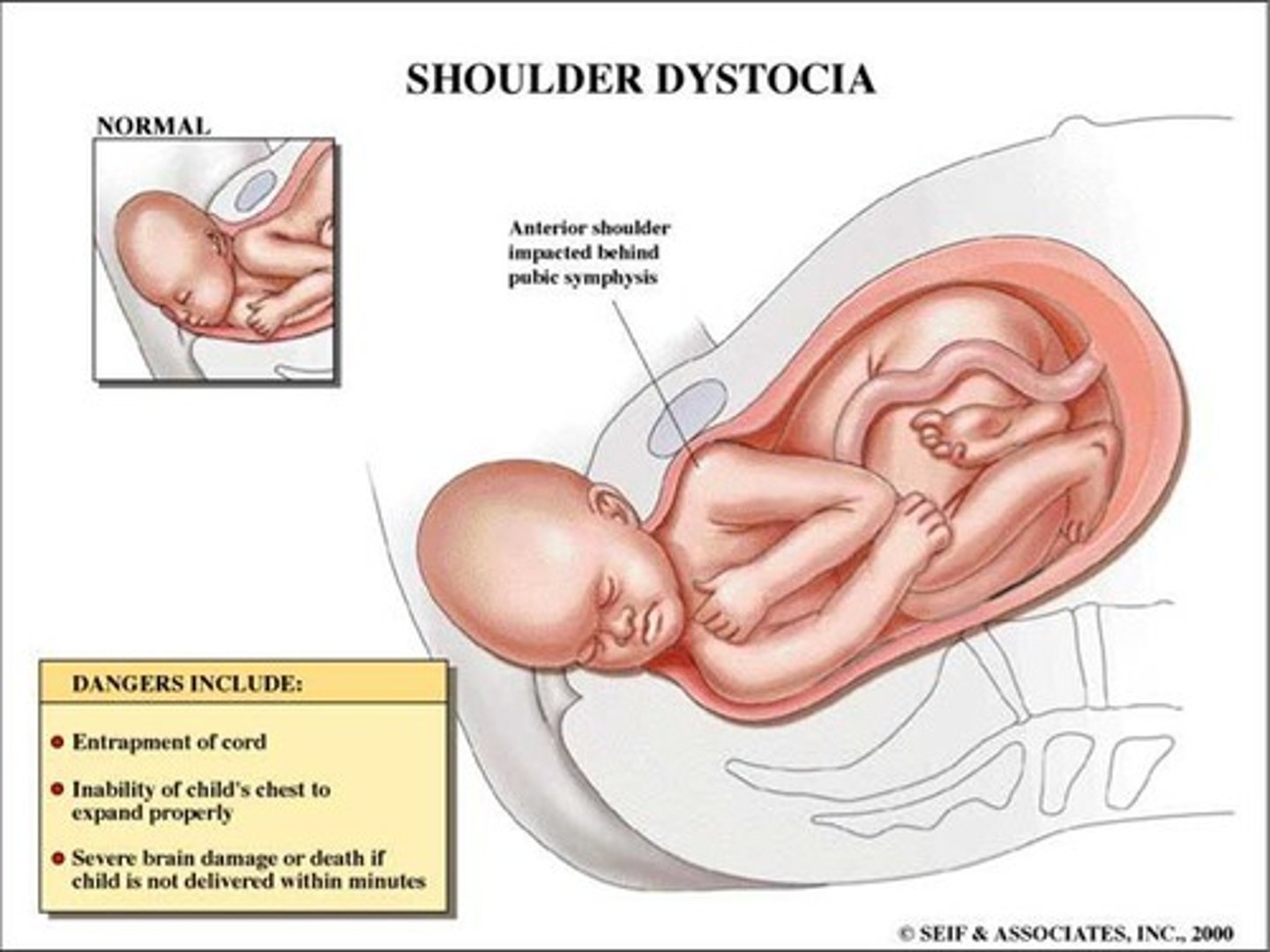
Q: What is shoulder dystocia?
An obstetric emergency in which the anterior shoulder of the fetus becomes impacted behind the maternal pubic symphysis during vaginal delivery, or, less commonly, the posterior shoulder becomes impacted against the sacral promontory
risk factors and a clinical sign for shoulder dystocia
1.History of shoulder dystocia
2 anything that could make baby big:
-Fetal macrosomia, Maternal diabetes mellitus or gestational diabetes, Maternal obesity
Prolonged second stage of labor
*many cases occur in absence of risk factors
clinical sign
- turtle sign - retraction of partially delivered head against perineum
fetal and maternal complications of shoulder dystocia
Maternal: PPH, 3rd/4th degree tears, symphyseal injury, uterine rupture (rare).
Fetal: Brachial plexus injury (Erb palsy C5-6 brachial plexus), clavicle/humerus fracture, hypoxia, HIE hypoxic ischemic ecephalopathy, death.

management of shoulder dystocia
first line
internal
last resort
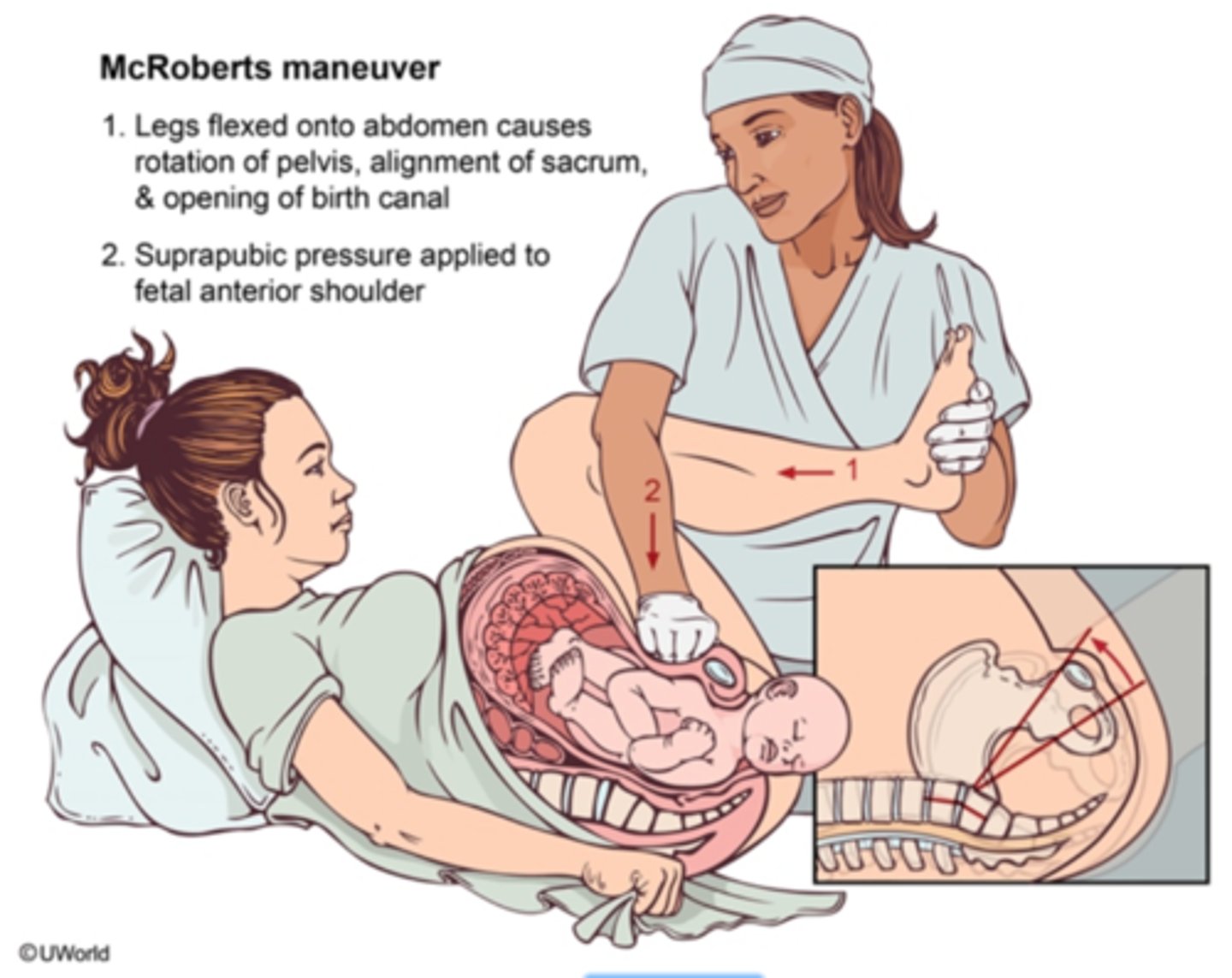
FIRST LINE
McRoberts manoeuvre (hips hyperflexed - flattens sacrum)— resolves ~40–50%.
+
Suprapubic pressure (downward/lateral to disimpact shoulder)
.Never apply fundal pressure.
INTERNAL
Rubin II: Pressure behind anterior shoulder → rotate.
Woods Screw: Pressure on posterior shoulder → rotate like a corkscrew.
Gaskin : mother on all fours
LAST RESORT
Cleidotomy (fracture clavicle),
Zavanelli manoeuvre (flex head → replace → emergency CS),
definition of still born vs death of a neonate. where do you legally report?
still born = no signs of life at ≥20 weeks of ≥400g birthweight ( if gestation unknown)
neonate death:
between 0-28 days
0-7 early, 8-28 late
report a still born or neonatal >20 weeks or 400g death with registry of births deaths and marriages
- provide stillborn certificate
causes of stillbirth
1. congenital anomolies
- structural (anencepaly, tet of fallot, gastrochesis, or chromosonal )
2. placental pathology
- ruptured, insufficiency, infarction, cord accident
3. maternal conditions
- HTN, diabetes, uterine rupture, Fetal maternal haemmorage ( alloimunisation), heavy smoking
4. feotal conditions
- hypoxia, FGR, alloimmunisation
5. infection
congenital, MUM , bub , placenta , infection
investigations after stillborn and management
1. hx ( find out risk factors or symptoms)
2. maternal ix
- fbc, blood group , antibodies
- Hba1c
- thyroid
- thrombophilia
3. placental exam
- Cord insertion, knots, thrombosis, infection, infarction.
- macroscopic and histopath
4. baby exam
- autopsy or xray .
how to determine feotal growth restriction ( FGR)
risk factors
estimated feotal weight or abdo circumference is <10% for gestational age.
maternal: smoking, hypertension , autoimmune
placental: abnormal implantation, infarct
fetal: aneuploidy/chromosomal, infections ( Toxoplasmosis, syphilus, CMV, malaria)
TORCH infections are vertically transmitted and can cause feotal pathology and death. what does the mnemonic stand for
Toxoplasmosis - cats host- chorioretinitis, diffuse brain calcificaitons
Other ( syphilius, listeria, HIV, varicella)
Rubella
Cytomegalovirus ( CMV) - herpes latent infection , sensoneural hearing loss and periventricular brain calcifications
Herpes simplex virus (HSV)
management of stillborn
spontaneous labour often occurs within 2 weeks of intrauterine death
misopristol or oxytocin IV infusion
Define PROM and PPROM.
clinical presentation and management of chorioamniotnitis
PROM: Prelabour rupture of membranes at ≥37 weeks before labour begins.
PPROM: Preterm Prelabour rupture of membranes <37 weeks.
- fever, uterine tenderness, maternal and fetal tachycardia
- broadspectrum antibiotics + delivery
Q: What are the key maternal and fetal risks associated with PROM/PPROM?
A:
Maternal: Chorioamnionitis, sepsis, endometritis, placental abruption.
Fetal: Infection, cord prolapse/compression, prematurity (in PPROM), pulmonary hypoplasia (early PPROM), perinatal morbidity/mortality.
Outline the key management strategies for PROM and PPROM.
A:
PROM (≥37 weeks):
- speculum, check for pooling of fluid, signs of choriamnionitis, assess maternal vitals and fetal wellbeing
- deliver / expectant or IOL within 24hrs
- check if GBS postive - intrapartum antibiotics
PPROM (<37 weeks):buy time .
deliver if infection, fetal compromise, or at appropriate gestation.
1. corticosteroids - bethamethasone 12mg IM ( given up to 36 +6 weeks)
2. tocolytics - nifidepine - stop contractions
3. mag sulfate if <32 weeks
4. antibiotics - amoxycillian 2g IV + azythromycin 1g PO once
Antenatal corticosteroids: indications, mechanism, and dosing
Purpose: Accelerate fetal lung maturation in threatened preterm birth
Benefits:
-↓ Neonatal respiratory distress syndrome (RDS)
- reduce risk of Intraventricular haemorrhage (IVH)
- reduce risk of Necrotising enterocolitis (NEC)
Mechanism: Stimulates type II pneumocytes → ↑ surfactant production.
Dosing:
Betamethasone: 11.4 mg IM × 2 doses, 24 h apart
Dexamethasone: 6 mg IM × 4 doses, 12 h apart
Indications: preterm labour, planned early delivery -pre-eclampsia
frequency of contractions in active labour
stage 1 - every 10 mins
stage 2
- early - every 4-10mins
- late - every 2 mins
what are braxton hicks
benign contractions helping with the position of fetus
- often occuring in 2nd/3rd trimester
- duration for <1min
epidemiology and risk factors for breast cancer
occurs in 1:7 women
92% survival >5 years
RF
1. increased estrogen exposure 85% of all cancers
- nulliparity
- late first pregnancy
- early menarche/ late menopause
- HRT
- OCP
2. Genetic
- BRCA 1/2 . P53 mutations
- first degree relative breast Ca hx
- previous breast CA
3. Other
- alohol
- obestiy
- dense breast tissue
- previous radiation hx
Screening is available for which age group and what is its purpose.
50 -74 mammogram ( every 2 years)
- can start by age 40 upon request
purpose is to reduce development to palpable mass
What is the most common breast cancer and how it spreads
Invasive Ductal Carcinoma
lymphatic:
axillary lymph nodes, internal mammery, supraclavicular
haematogenous
- bone - most common symptomatic site
- lung
- live
-brain
* lobular carcinoma- more diffuse - GI and peritoneoum, ovary involvemnt
Management for breast cancer
Triple Assessment
1. hx & clinical exam
2. Imaging
< 35 - US
> 35 mammogram -+ US
3. core biopsy ( diagnostic)
triple test is positive if any of 3 components supicious
* use MRI in dense breasts
Staging - TNM
CT abdo chest pelvis if symptoms or node positive
PET - CT in higher stages
Key molecular drivers in breast cancer and their cancer treatment
why does triple neg have the worst prognosis
estrogen receptor - estrogen inhbitor - Tamoxifen or aromatase inhibitor ( post menopausal)
progesterone receptor
Human Epidermal growth FActor HER2 - Trastuzumab/ herceptin
^^ easy drug targets
when breast cancer is negative ER, PR , HER2 the only treatment option is chemo
risk difference between BRCA1 vs 2 mutation
BRCA1 - triple neg tendancy + ovarian
Lifetime breast cancer risk: 60–85%
Lifetime ovarian cancer risk: 40–60%
Cancers tend to be triple-negative and high-grade
Earlier onset
Also increases prostate cancer risk in males
Exam trick: BRCA1 → “1 letter away from TN” → Triple Negative tendency
BRCA2 - lower risk for breast higher for other
Lifetime breast cancer risk: 50–85%
Ovarian cancer risk: 10–30%
Cancers more often ER-positive
Also increases pancreatic and prostate cancer
prognosis and treatment for luminal a, B HER2 , triple neg
luminal a - BEST - endocrine therapy
luminal b - MODERATE - endocrine + -chemo
her 2 positive - GOOD with treatment - anti her 2 + chemo
triple neg - WORST - chemo +- immunotherapy
clinical features , investigations, management of inflammatory breast cancer
rapid-onset red ≥ 1/3rd of breast
swollen breast with peau d'orange from dermal lymphatic invasion;
no response to antibiotics within 7-10 days
high metastatic potention
investigations
punch biopsy
mammogram/ultrasound (<30)
Management:
requires neoadjuvant chemo → mastectomy → radiation.
* often misdiagnosed as mastitis
sensation to the external genitalia/perineum is provided by which nerve
pudendal
First trimester - key physiology + risks
0-13 weeks
Organogenesis (5-10 weeks) → highest teratogen risk
hCG maintains corpus luteum → progesterone support
Spiral artery remodelling begins
Main risks: miscarriage, ectopic, hyperemesis
First trimester - essential tests & why
1.Dating scan ( US crown - rump length) → most accurate GA within 5-7 days. done at weeks 7-10
2. FBC, group & antibodies → anaemia + HDFN( haemolytic disease of fetus & newborn) risk
3. Infectious screen (HIV, Hep B/C, syphilis, rubella) → prevent vertical transmission
4.MSU → asymptomatic bacteriuria - increased risk of pyelonephritis and preterm delivery
5. NT ± NIPT (10-13 w) → aneuploidy screening
NIPT vs NT, when best done
NT - nuchal translucency providing first physical anatomy check of baby - US measuring neck fluid for chromosomal and structural/cardiac abnormalities
10-16 weeks best done
NIPT - most accurate genetic screening for Downs
syndrome - measure free fetal maternal DNA
12 /13 weeks
Second trimester - key physiology + complications
Weeks 14-27
Placenta fully functional
Rapid fetal growth
hPL (human placental lactogen)→ ↑ insulin resistance
Plasma volume expansion peaks
compilcations:
Gestational diabetes
Cervical insufficiency- uncommon cause of SAb
Placenta previa
Preterm labour (viability ~23-24 weeks in Aus)
Second trimester - major screening
18-22 w morphology scan → structural anomalies + placenta location
24-28 w OGTT → gestational diabetes - prevent neonatal hypoglycemia
Maternal quad screen ( if no prev NIPT) - AFP, hCG, estriol, inhibin A
Fundal height (from 24 w) → growth screening
Amniocentesis (if indicated) → diagnostic genetics
Third trimester - physiology + surveillance focus + major complications
how to determine between placental abruption vs previa
Weeks 28-40
Rapid fetal weight gain
Hypercoagulable state
surveillance focus:
BP + urine each visit → preeclampsia screen
Monitor movements + presentation
complications:
Preeclampsia
FGR
PPROM
Placental abruption- cause of haemorrage - painful , rigid uterus
placenta previa - cause of haemorrage- painless ,soft uterus
Third trimester - key interventions
treatment for GBS positive mum?
28 w give Anti-D (if Rh-)
28 w FBC → anaemia
35-37 w GBS swab → intrapartum IV penicillin if positive
Growth scan if risk (GDM, HTN, FGR)
ECV( external cephalic version) at 36-37 w if breech
Rotterdam's criteria for PCOS
1. irregular/absent periods - oligo/anovulation
2. hyperandrogenism - clinical or biochemical
- clinical : acne, hirsutism
3. polyystic ovaries - ≥12 follicles on ultrasound
* need 2/3
pathophys of PCOS and what hormone levels you would expect to see in FSH + LH
PCOS = Fast GnRH → High LH → High Androgens → Follicles Arrest → no ovulation = No Progesterone from CL
increased androgens = increased visceral adiposity , impaired insulin signalling - pancreas compensates with increased insulin secretion
Insulin directly stimulates theca cells - increased androgen production
high LH and normal/low FSH
* high antimullarian hormone (AMH) - hinder maturation of follicles
treatment and complications of PCOS
OCP ( DIane 35) - regulates cycles, reduces free testosterone and endometrial hyperplasia
if wanting pregnancy - letrozole - aromatase inhibitor - decreases estrodial production = increased FSH = ovulation
BMI >25 - metformin - increase insulin sensitivity
hirsutism - spironolactone (androgen receptor blockade) - teratogenic - must give with contraception
first line always - exercise ( 5% weight loss can cause ovulation) , mediteranean diet
- gestational diabetes, T2DM
- infertility
- metabolic syndrome, dyslipedemia
- endometrial hyperplasia ( cancer) - unopposed estrogen
normal range for baseline fetal HR?
blood vessels in umbilical cord?
normal range for fetal hr variability?
1. 110-160
2. 2 arteries 1 vein
3. 5-25 bpm
depth of invasion
placenta accreta, increta, percreta?
accreta - chorionic villi adheres to myometrium
increata- chorionic villi invades myometrium
percreta - chorionic villi growth through myometrium
complications of PPH
Hypovolaemic shock
DIC
Renal failure
Sheehan syndrome - ischemic pituitary necrosis ( agalactorheaa earliest sign)
Maternal death
Risk factors for PPH
Antenatal :
Previous PPH
Multiple pregnancy
Polyhydramnios - chronic uterine distension - atony
Anaemia - poorer tolerance of blood loss
Fibroids- impaired uterine contractility
Intrapartum :
Prolonged labour
Induction/augmentation - myometrial fatigue - atony
Instrumental delivery
Caesarean section
Chorioamnionitis - reduced contractilty - atony
mifepristone vs misopristol
cut off for at home medical abortion?
surgical abortion preferred gestation dates
Mifepristone → progesterone antagonist ( stop pregnancy process) - egg detaches from uterine wall , uterus contracts
Misoprostol →synthetic prostaglandin - cervical ripening and uterine contractions -
9 weeks for at home ( later cut off at specialist hospitals)
14-22 weeks for surgical ( under GA or local)
complications of abortion
1. failure of abortion (1 in 100)
2. retained tissue ( 3-5 in 100 - medical)
3. infection <1-100
4. haemorrage - 1-1000
which ultrasound is used to detect fetal anemia?
what gestational age is this appropriate?
serial MCA - middle cerebral artery doppler - starting 16-18 weeks
- common in twin to twin transfusion syndrome, red cell alloimunisation
contraception options for breastfeeding women
progestrone only
- oestrogen can interfere with milk supply
what liver enzyme physiologically increases in pregnancy
name 3 liver dysfuncitons to be aware of in pregnancy
ALP
- presence of placenta ALP
ICP
intrahepatic cholestasis of pregnancy - increased oestrogen, impaired bile acid transport - maternal accumulation in blood - crosses placenta - risk of fetal arrythmia, still born.
itchy palms and soles
preeclampsia HELLP
- RUQ pain + thrombocytopenia in 3rd trimester → HELLP until proven otherwise.
AFLP
Acute fatty liver of pregnancy - fatty acid oxidation defect - fat depositions on liver - hypoglycemia cant produce ketones when fasting - liver failure - immediate delivery
( serum bile acid ≥10)
differentials for non pregnant/ abnormal uterine bleeding vaginal bleeding
PALM COEIN
structural
Polyp (endometrial polyp)
Adenomyosis
Leiomyoma (uterine leiomyoma)
Malignancy and hyperplasia
Nonstructural causes
Coagulopathy: e.g., Von Willebrand disease
Ovulatory dysfunction -anovulatory bleeding e.g., secondary to hyperprolactinemia, thyroid disorders, PCOS, obesity
Endometrial : endometrial dysfunction in a structurally normal uterus with regular cycles (diagnosis of exclusion)
Iatrogenic: e.g., estrogens, progestins, IUD, antithrombotic agents
Not otherwise classified : e.g., cesarean scar defect, uterine arteriovenous malformations (AVM)
adenomyosis vs leiomyoma
impact on uterus shape , pain, imaging, fertility
adenomyosis
- bulky uniformly enlarged uterus
- painful , heavy periods
- diffuse myometrial change
leiomyoma ( fibroid)
- focal mass/ irregular contour
- heavy periods but painless
- discrete mass
- submucosal impact on fertility
describe uterine hyperstimulation and management
excessive contractions of the uterus - ≥5 in 10 or a contraction >2mins
can be caused by induction agents - prostaglandins, syntocin
managent
remove inducing agents
position px to left lateral position ( improve blood flow)
give tocolytic
- IV or SC turbutaline 0.25mg
or nitroglycerine 60- 180 micrograms
when to give Anti D in pregnancy
and dosing for rhesus D prophylaxis
give at:
28 & 34 weeks
within 72 hours if baby RH+
any event with bleeding/procedure
< 12 weeks 250 IU
≥12 weeks 625 IU
don't give:
-if mother already sensitised
- baby confirmed negative
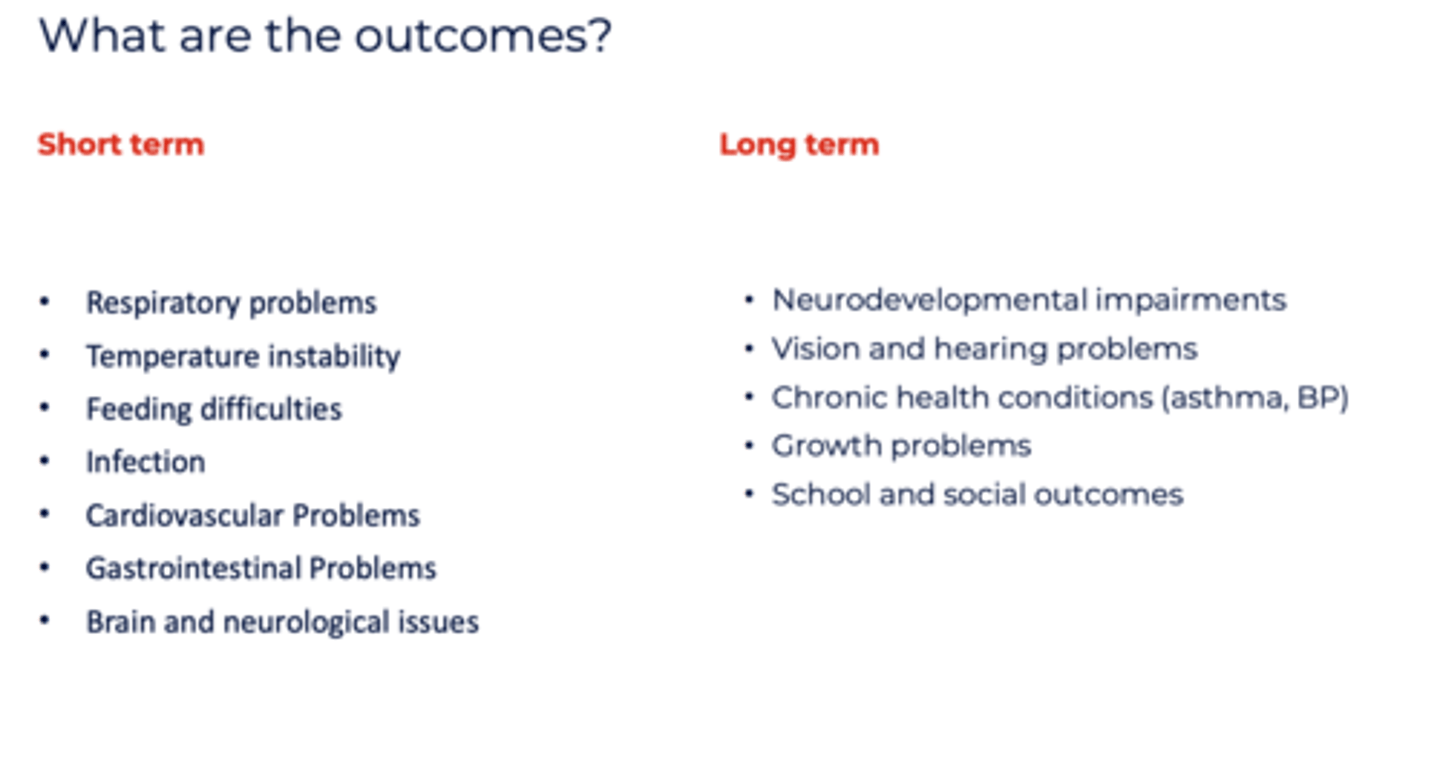
complications for preterm labour short
low birth weight
explain transient thyroid hyperemesis gravidarum
physiological response in pregnancy up to 12 weeks as HcG ( from corpus luteum) stimulates TSH receptors on thyroid causing increased free T4 - increased catecholimines sensitivity - activates vomiting centre, anxiety, tachy.
what RSV vaccine can be given to mother
mechanism of action?
benefits, side effects
abrysvo
given at 24-36 weeks to prevent RSV in infants
mechansim
targets pre-fusion F protein on RSV virus before it infects cell
must be given 2 weeks before birth for effectiveness protective for first 6 months
minimal side effects , no evidence on BW, prematurity, still births
50% less likely to be hospitalised with RSV during 6 months
* no maternal protection
* active immunity ( b&t cell activation) + passive immunity to fetus ( no memory cells)
Which RSV vax can be given to infants?
mechanism ?
when is it given?
benefit?
nirsevimab
a monoclonal antibody which binds to prefusion F protein inhibiting RSV from infecting cells
given at birth - if mother not effectively immunissed
given 7months-2 years at RSV season IF RISK FACTORS:
<32/40
congenital heart disease
immunosuppresion
chronic lung disease ( CF)
trisomy 21
* 80% risk reduction of hospitalisation in first year of life.
Types of Miscarriage
Q: What are the main types of miscarriage and how do they present?
🩸 Types
Threatened
Bleeding + cramping
Cervix closed
Viable pregnancy
Inevitable
Bleeding + cramping
Cervix open
No passage yet
Incomplete
Bleeding + cramping
Some products passed
Cervix open
Complete
All products passed
Cervix closed
Heavy Bleeding will settle
Missed
Fetal demise, no symptoms
Cervix closed
Often minimal bleeding
🧠 Exam memory line:
Closed = threatened/missed
Open = inevitable/incomplete
management of miscarriage
Unstable = surgery
Stable = expectant / medical / surgical
⚖️ Stable patients — 3 options
1. Expectant
Watch and wait
Suitable if mild symptoms
2. Medical
Misoprostol
Used for incomplete or missed miscarriage
* not necessary for mifepristone as pregnancy already nonviable
3. Surgical (definitive)
Suction curettage (vacuum aspiration)
Indications:
Heavy bleeding
Infection
Failed medical
⚠️ Always consider
Anti-D if Rh-negative
Infection → antibiotics
Follow-up to ensure complete evacuation