Public Health Final
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
John Snow
English physician (1813–1858), pioneer of epidemiology.
Proved cholera spread via contaminated water, not air.
Used mapping/data to trace London outbreak to one water pump.
His work led to modern sanitation and clean water systems.
Poor Law of 1601 (elizabethan poor law)
England’s first welfare system; parishes cared for the poor, sick, and elderly.
Funded by local taxes (“poor rate”).
Early foundation for public health and social responsibility.
Ada Mayo Stewart
First US occupational (industrial) nurse (1870-1945)
Worked for Vermont Marble Company; cared for workers and families.
Expanded nurse’s role to workplace health and safety.
Inspired the growth of occupational health nursing.
clara barton
Founder of the American Red Cross; “Angel of the Battlefield.”
Provided wartime relief and pioneered disaster response.
Promoted first aid readiness and preventative care.
Lemuel Shattuck
Author of 1850 Massachusetts Sanitary Commission Report.
Advocated public health data collection, sanitation, prevention.
Laid groundwork for modern public health departments.
Dorothea Dix
Reformer for mental health and prison conditions.
Superintendent of Army Nurses (Union, Civil War).
Set professional standards for nurses and humane care.
Mary Breckinridge
Founded Frontier Nursing Service in rural Kentucky.
Pioneered nurse midwifery, prenatal, and child health care.
Greatly reduced maternal and infant mortality.
Lilliam Wald
Founder of public health nursing.
Created Henry Street Settlement in NYC for community care.
Promoted accessible home health and social services.
boom and bust
describes a pattern of panic and neglect. Massive spikes in crisis-driven funding (e.g., during the COVID-19 pandemic) lead to rapid hiring, only to be followed by brutal budget cuts, workforce layoffs, and infrastructure erosion as public attention wanes
Dr Chokshi Podcast
boom and bust
misinformation units
making the invisible visible
Social determinants of health
Economic stability (income, employment, poverty)
Education access and quality
Health care access and quality
Neighborhood and built environment (housing, safety, transportation, pollution)
Social and community context (social support, discrimination, social cohesion)
Health Disparities v. Health Equities
Health disparities = the unequal differences in health outcomes between groups.
Health equity = the effort to eliminate those differences by ensuring fair access to opportunities and resources for health.
A group of researchers conducted a study on a particular population and found that individuals from lower-income neighborhoods had higher rates of cardiovascular disease compared to those from wealthier neighborhoods. What term best describes this situation?
Health disparities
A nurse, aware of the social injustices related to healthcare access in her city, collaborates with local stakeholders to develop a free city-wide vaccination program that specifically targets underserved neighborhoods. This nurse's actions primarily demonstrate a commitment to:
Heath Equity
A city government implements initiatives to improve access to healthy food options in low-income neighborhoods, build safe recreational spaces, and promote educational opportunities. What term best describes these efforts? Select all that apply.
health equity and social determinates of health
Windshield Survey
Driving through a community to observe it firsthand
Strengths: descriptive overview of community
Limitations: requires 2 people, time-consuming, only visual — no direct community input
Community Health Needs Assessment
Views the community as the client, not individuals
Goal: provide benefit to the community/population as a whole
Foundation for all program planning and change
Uses the nursing process or Plan-Do-Study-Act (PDSA) cycle — assessment always comes first
Community Health Nurse Role
Establish contacts with community partners
Witness interactions between community programs and client responses
Identify future services based on the visible needs of community members
Data collection methods
informant interviews
open public meetings
secondary data
focus groups
surverys
windshield survey
informant interviews
Strengths: low cost, builds participant buy-in/future supporters, may elicit unexpected details
Limitations: possible bias, difficulty finding willing participants
Open Public Meeting (community Forum)
Strengths: community input, low cost
Limitations: difficult to find a venue, focus can drift with too many ideas, less vocal members may not speak up, and participation varies
Secondary Data
Strengths: existing databases, can identify trends
Limitations: may not reflect current trends, time-consuming
focus groups
Small group discussions to gather community perspectives
Surveys
Strengths: aggregate data, random sampling, written format, anonymous, no direct contact required
Limitations: low response rate, expensive, time-consuming, requires reading ability
After the assessment (process)
Analysis (diagnosis)
Planning intervention/program
Implementation
Evaluation
Components of the Epidemiological triad
Agent 2. Host 3. Environment
Agent (epidemiology)
The biological, chemical, or physical cause of a disease or injury.
In the provided examples, this includes specific bacterial strains responsible for gastrointestinal illness.
Host (epidemiology)
The human or animal that harbors the disease or is susceptible to it.
This component is associated with the mode of transmission, such as human-to-human spread via respiratory droplets.
Organisms that harbor and transmit disease, such as mosquitoes serving as vectors for malaria, are also classified as hosts in this model.
Enviornment (epidemiology)
The external factors (physical, biological, or social) that allow the agent and host to interact.
Examples include crowded living conditions, climate, or contaminated water sources that facilitate the spread of an agent.
Three Levels of Prevention
Primary
Secondary
Tertiary
Primary Prevention
Goal: Prevent disease or injury before they occur.
Methods: Preventing hazard exposure, altering unsafe behaviors, and increasing resistance to disease.
Examples: Immunizations, health education (tobacco use, safe sex), seat belt laws, and creating safe environments in schools or workplaces.
Secondary Prevention
Goal: Reduce the impact of a disease or injury that has already occurred.
Methods: Early detection and treatment to slow progress, and implementing programs to return individuals to original health/function.
Examples: Screenings (mammograms, blood pressure tests), low-dose aspirin or diet/exercise to prevent further heart attacks, and modified work duties for injured employees.
Tertiary Prevention
Goal: Soften the impact of an ongoing illness or injury with lasting effects.
Methods: Helping people manage long-term, complex health problems to improve function, quality of life, and life expectancy.
Examples: Cardiac or stroke rehabilitation programs, chronic disease support groups, and vocational rehabilitation to retrain workers.
endemic
constant presence or usual prevalence of a disease or infectious agent in a population within a specific geographic area
epidemic
an increase, often sudden, in the number of cases of a disease above what is normally expected in apopulation in a specific area
Pandemic
an epidemic that has spread over several countries or continents, usually affecting a large number of people
Outbreak
sudden increase in the number of cases of a disease above what is normally expected in that population in a specific area; can be a single community or school
Compondents of Epidemiology
public health survelence
field investigation
analytical studies
evaluation
linages and collaboration
policy development
public health surveilance (compondents of epidemiology)
Ongoing, systematic collection, analysis, interpretation, and sharing of health data to guide public health decision-making
Acts as an early warning system for reportable diseases, behaviors, violence, etc.
Detects health problems/trends quickly to allow prompt intervention
Examples: COVID-19 case monitoring, tracking TB/HIV/AIDS/malaria, cancer reporting, air pollution levels, water quality testing, lead exposure monitoring
Field Investigation (compondents of epidemiology)
Collecting data to identify the source of an illness and understand the occurrence and spread of disease
Begins creating methods to control outbreaks
Includes studying outbreaks, identifying sources of infection, devising strategies to prevent further transmission
Examples: E. coli food contamination studies, interviews of ill individuals, animal migration tracking, STI contact tracing
Analytical Studies (compondents of epidemiology)
Examines relationships between exposures and health outcomes to understand why diseases occur
Fills gaps between surveillance and field investigation
Identifies causes, modes of transmission, and validates epidemiologic hypotheses
Focuses on risk factors, causes of disease, and effectiveness of interventions
Supports evidence-based nursing practice and public health policy
Examples: Epidemiologic triad, chain of infection, case-control studies, cohort studies, randomized controlled trials
Evaluation (compondents of epidemiology)
Determines the relevance, effectiveness, efficiency, and impact of public health activities
Helps identify what works, what doesn't, and where improvements can be made
Examples: Assessing proportion of target population immunized and impact on vaccine-preventable disease rates; during COVID-19 — evaluating vaccine effectiveness, masking, treatment trends, mortality rates, and booster potential
Linkages and Collaboration (Compondnets of epidemiology)
Epidemiology is a team sport — involves labs, infection control nurses, clinical staff, and computer information specialists
Spans local, state, federal, global, academic, and clinical sectors
Sharing information across all areas is essential for effective outcomes
Examples:
AIDS epidemic — lack of collaboration among scientists delayed discovery of antivirals and knowledge about transmission
Opioid epidemic — surveillance data (ED visits, EMS calls, overdose deaths) was linked with healthcare interventions (naloxone distribution, harm reduction education) to target highest-risk areas
Policy development (components of epidemiology)
Uses epidemiologic data to create laws, regulations, and guidelines
Supports public health mandates and funding decisions
Translates evidence into actionable rules that protect population health
Examples: Meningococcal ACWY vaccine mandate for college students, mask mandates during outbreaks, FDA food safety regulations
Healthcare Policies
Health in All Policies (HiAP): Integrates health considerations into decision-making across all sectors.
Focus: Recognizes health as shaped by social, economic, and environmental factors, not just healthcare access.
Collaboration: Involves sectors like transportation, education, housing, and agriculture to promote health equity.
Goal: Create healthy, sustainable communities and reduce health disparities through shared responsibility.
Vision Zero: Strategy to eliminate all traffic fatalities and severe injuries.
Principle: Views crashes as preventable events caused by system design, not just individual error.
Approach: Promotes safe, equitable, and healthy mobility for all.
Collaboration: Requires participation from both public and private sectors using a multidisciplinary approach.
Pathogen
the infectiious agent that causes disease (bacteria, fungi, virus)
Chain of Infection
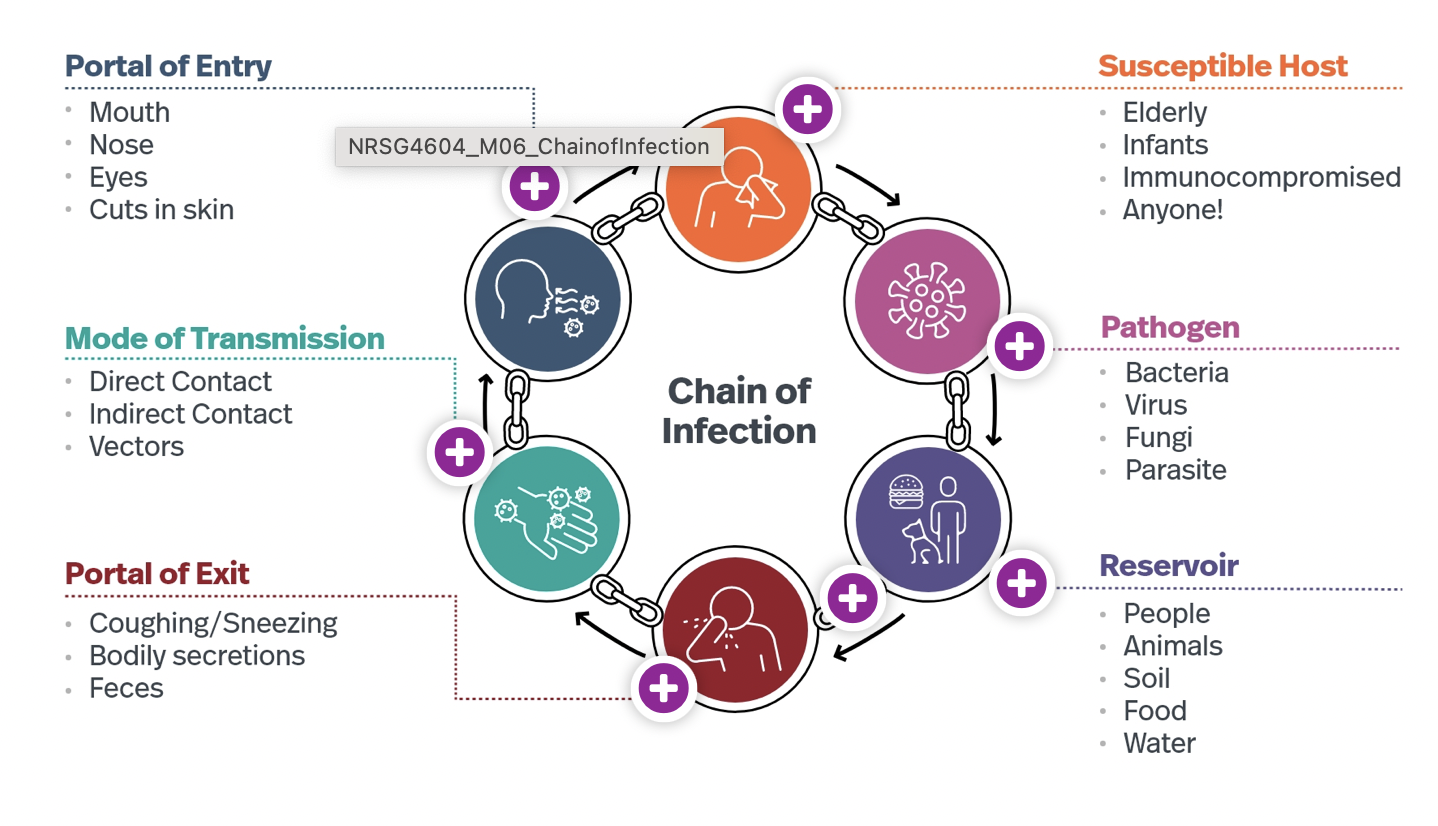
Reservoir
where the pathogen naturally lives and multiplies (people, animals, soil, food, water)
Portal of Exit
how the pathogen leaves the reservoir (coughing, bodily, feces)
mode of transmission
how the pathogen tracels to a new host (direct contact, factors, indirect)
portal of entry
how the pathogen enters the new host (mouth, nose, eyes, cuts)
Suseptible host
A person able to be infected by the pathoegn (elderly, infants, immunocompromised,)
Elder abuse and Neglect
Limited data on prevalence
Females abused at higher rates than males
The older you are, the more likely you are to be abused
Most commonly reported type: financial abuse/mismanagement
Signs of elder abuse:
Unexplained or repeated physical injury
Physical neglect, unmet basic needs, poor hygiene/appearance
Financial mismanagement
Withdrawal, passivity, depression
Mandatory reporting (MA)
Nurse suspects abuse → immediately report orally to supervisor/employer
Supervisor must immediately notify Department of Public Health (DPH)
Written report must follow within 48 hours to DPH
Intimate parter violence
Nursing barriers: lack of knowledge/training on warning signs, how to ask, legal options, and social services
First-line support: attentive listening, nonjudgmental care, referrals to trusted resources, legal protection, housing
Lethality/Danger Assessment: developed by J. Campbell PhD, RN — assesses women's risk for homicide
Greatest risk factor for homicide: partner has a gun in the home
Human Trafficing - red flags
Does not speak English OR someone accompanying them supervises and resists leaving them alone
Doesn't know their location, has no address or job information
No ID or money — someone else is holding it
Signs of physical abuse/neglect, malnutrition, dehydration, drug use, poor hygiene
Tattoo that may signify "branding" by trafficker
Nursing care for victems of violence
Build trust and confidence
Focus on the client, not just the situation
Assess for immediate danger
Provide emergency care as needed
Develop a safety plan with the client
Make referrals for community services and legal options
Complete mandatory reporting following state and agency guidelines
specialized models of care
SANE: Certified Sexual Assault Nurse Examiners — forensic nursing specialty
Forensic nursing: formal education pathway for nurses working with victims of violence/trauma
Most children's hospitals have multidisciplinary maltreatment teams (doctors, nurses, social workers, advocates)
Community resources
Women's shelters, law enforcement, advocacy/justice centers, WIC, mental health agencies (DMH, BEST), food banks, support groups (AA/NA), forensic nursing, unemployment offices, churches/faith communities
therapuetic attidute (SUD)
Any drug/substance can be used in an unhealthy way
Anyone can develop Substance Use Disorder (SUD)
No one chooses to have a SUD
People can be successfully treated
Accept the client where they are in their recovery process
Reflect on your own attitudes, triggers, and frustrations when working with SUD clients
Key phrases: "I'm here to help you, not judge you" / "You're here now, and that's a big first step"
stigma reduction (language matters)
Say This |
Person with a substance use disorder |
Drug use/misuse |
Person living in recovery |
Person arrested for a drug violation |
Reoccurrence/setback |
Maintained recovery |
Not That |
Addict, junkie, druggie |
Drug abuse |
Ex-addict, clean |
Drug offender |
Relapse |
Stayed clean |
Most Common SUDs
Alcohol use disorder, Tobacco use disorder, Opioid use disorder, Cannabis use disorder
SBIRT Model (screening, breif intervention, referral to treat)
Purpose: Identify individuals at risk for SUD, provide early intervention, and connect them with treatment
SUD screening tools
Quickly assess severity of substance use and identify those needing further intervention
CAGE quentioneer (alcohol deoendence screening)
CRAFT (teen screening)
CAGE questioneer (alc dependence screening)
C – Ever felt the need to Cut down on drinking?
A – Have people Annoyed you by criticizing your drinking?
G – Ever felt Guilty about drinking?
E – Ever had a morning Eye-opener to steady nerves or cure a hangover?
2+ "yes" answers → suggests potential alcohol dependence, warrants further evaluation
CRAFT teen screening tool
C – Ridden in a Car driven by someone (or yourself) who was high/drinking?
R – Used substances to Relax, feel better, or fit in?
A – Used substances while Alone?
F – Forget things done while using?
F – Family or Friends told you to cut down?
T – Gotten into Trouble while using?
Breif intervention (SUD)
Short, focused conversation providing feedback and advice
Increases awareness, motivates the person to reduce or stop unhealthy use
Encourages reflection on substance use and its consequences
Referral to Treat —> Connects the person to specialized care
Harm reduction model (SUD)
Public health approach that minimizes negative consequences of substance use rather than requiring abstinence
Pragmatic, compassionate, nonjudgmental — meets people where they are
core principles of SUD
Accepts that drug use exists — people use substances for complex reasons; abstinence not required for support
Prioritizes safety and dignity — reduce health, legal, and social harms (overdose, infection, incarceration); emphasizes human rights
Respects individual autonomy — supports informed choice; encourages incremental change, not all-or-nothing
Focuses on reducing harm, not necessarily use — e.g., continued heroin use but with sterile needles to prevent HIV/Hep C
Harm reduction practices
Practice | Goal |
Needle exchange programs | Prevent HIV/HCV & abscesses |
Naloxone distribution | Prevent opioid overdose deaths |
Safe consumption sites | Medical oversight & link to care |
Fentanyl test strips | Avoid unintentional overdoses |
Medication-Assisted Treatment (MAT) | Reduce cravings & overdose risk (buprenorphine, methadone) |
Safer sex education & supplies | Prevent STIs |
Housing First programs | Prioritize housing stability over sobriety requirements |
take aways and barriers to treatment (SUD)
Easier access to illegal drugs than to treatment programs
Hard to get help
Lack of insurance coverage for SUD programs
Programs often low quality, not evidence-based
Unproven approaches (scams) exploit desperate families
The Opiod Epidemic
U.S. opioid crisis unfolded in waves: prescription opioids → heroin → synthetic opioids (fentanyl)
Sackler family / Purdue Pharma:
Developed and launched OxyContin in 1996
Aggressively marketed it as safe, downplaying its addictive nature
Promoted to doctors and influenced the FDA
Aggressive promotion and over-prescribing were major drivers of the crisis
Family amassed billions in profits
Faced numerous lawsuits; reached multi-billion-dollar settlements with states
Behavioral Red Flags with SUD in healthcare workers
Frequent absences from the unit, frequent bathroom trips, medication errors
Tardiness (especially after breaks or before shifts)
Mood swings, irritability, unexplained emotional outbursts
Isolation from colleagues; avoiding patient/staff interactions
Confusion, memory lapses, difficulty concentrating
Erratic behavior (euphoric one moment, lethargic the next)
Defensiveness/secrecy about work performance or medication handling
CM of SUD in healthcare workers
Shakiness, unsteady gait, slurred speech
Dilated or constricted pupils; red or glassy eyes
Frequent nosebleeds (possible sign of snorting substances)
Sudden weight changes
Unusual body odor, sweatiness, poor hygiene
Tremors or involuntary movements
Drug Diversion
Occurs daily in healthcare settings
Example: MGH paid $2.3 million to resolve drug diversion allegations
Hospitals implement drug diversion prevention programs and compliance measures
Support resources: MA Nurses Association Peer Assistance Program, AANA Helpline
URAMP (Unified Recovery and Monitoring Program): In MA, the Board of Registration in Nursing's SARP transitioned to URAMP in 2024 — supports healthcare professionals in recovery
Enviornmental health nursing - key roles
Health Impact Assessment — assess potential health risks from environmental changes (new industries, climate change, new housing developments)
Disease Prevention — reduce risks from environmental factors (ex: poor air quality → asthma); intervene through policy and direct action
Regulation & Policy Development — develop, implement, and enforce environmental health policies (ex: industrial emissions regulations, waste management policies)
Health Education & Promotion — educate the public and stakeholders on environmental health issues; promote protective behaviors
Research — study how environmental changes impact human health and how those impacts can be mitigated
climate change and health impacts
heat related
vector borne disease
food security and malnutrition
air quality
population displacement
Heat related illnes and death
rising temperatures increase heat-related illness and death; exacerbates chronic cardiovascular and respiratory conditions
vector borne diseases
warmer/wetter climates expand mosquito and tick habitats → increased spread of malaria, dengue, Lyme disease
food security and malnutrition
changes in temperature and rainfall affect crop yields and livestock → food insecurity, malnutrition, altered nutrient content in crops
air quality
warmer temperatures increase ground-level ozone → worsens smog, triggers respiratory illness
Popultion displacement
extreme weather events and rising sea levels displace populations → cascading health issues: poor sanitation, limited healthcare access, social dislocation
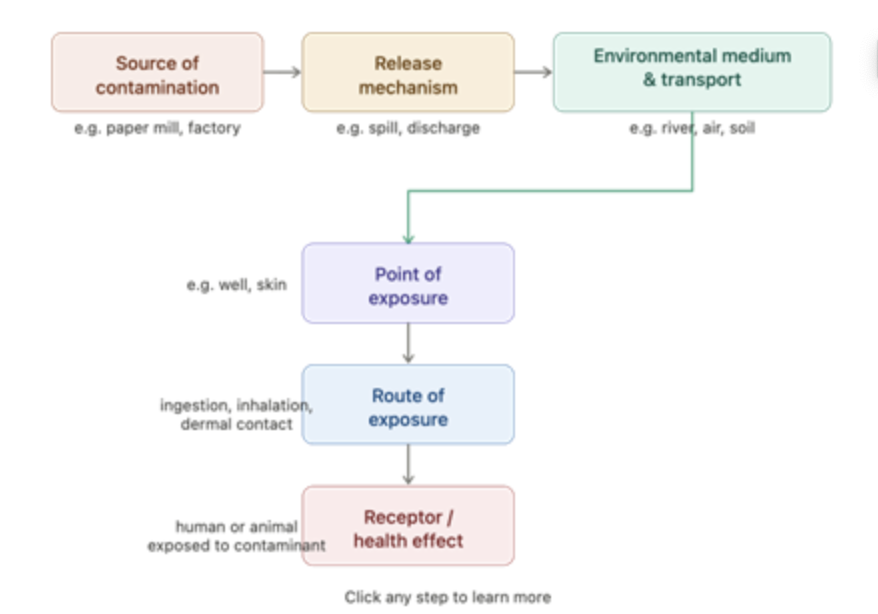
enviornmental exposures process visual
enviornmental health overview
Field of public health science focused on how the environment influences human health
Key areas: water quality, toxics/waste, outdoor air quality, global environmental health, healthy homes & communities, infrastructure/surveillance
exposure pathway
Source → Release Mechanism → Environmental Medium → Exposure Point → Exposure Route
Release mechanisms: volatilization, spills, leaching
Environmental media: air, soil, soil gas, groundwater
Exposure points: food chain, direct contact
Exposure routes: inhalation, ingestion
Exposure pathway: Describes how people are exposed to an environmental contaminant that originates from a specific source.
bioavailability
The amount of a substance that is absorbed or becomes available at the site of physiologic activity
Not just how much contaminant is present — it's how much the body actually absorbs
Example — Lead in soil:
Child ingests contaminated soil → risk depends on how much lead is absorbed through the GI tract
Lead tightly bound to minerals = low bioavailability = lower risk
Lead in easily dissolved form (e.g., lead acetate) = high bioavailability = higher risk
Helps public health officials prioritize remediation and assess actual health risk
risk assessmen for enviornmeal contaminants
Risk = Hazard × Exposure
common contaminants
lead, mercury, radon, PCBs, mold, benzene, asbestos, pesticides, arsenic
GOAL of enviornmental justice
no group bears a disproportionate share of negative environmental consequences
Public health nurses must understand diverse communities and the varying vulnerabilities and adaptive capacities of different populations
climate change inpact on health
Climate Issue | Health Impact |
Intense heat waves | Heat exhaustion, heatstroke, dehydration (high risk: older adults, outdoor workers, infants, chronic illness) |
Ozone / air quality / fires | Worsening asthma & COPD; urban & vulnerable populations most affected |
Warmer climates | Increased vector-borne diseases — Lyme, West Nile, Dengue, Zika (mosquitoes/ticks) |
Droughts, flooding, changing climate | Disrupted food supply, reduced crop yields, food insecurity, increased costs |
Climate-related disasters (hurricanes, wildfires, flooding) | Stress, anxiety, depression, PTSD — especially in those with prior trauma |
Types of disasters
natural, accidental, terrorism, emergency
natural disasters
Earthquakes
Flooding
Hurricanes
Tornadoes
Wildfires
Blizzard (1978)
accidental disasters
Chemical spills
Nuclear accidents
Industry explosions
Oil spills
terrorism
9/11 (2001)
Boston Marathon (2013)
Sarin gas attack, Tokyo (1995)
Emergency disasters
Housing fire
Local power outage
Water main break
direct effects of natural disasters
Physical injury or death (falling debris, floods, fires, structural collapse)
Loss of shelter
Interruption of basic services (power, water, roads)
Displacement / forced evacuation
Property damage
Indirect effects of natural disasters
Mental health issues — anxiety, depression, PTSD
Loss of livelihood — businesses destroyed, jobs lost
Educational disruption — school closures affecting child development
Increased disease risk — poor sanitation, overcrowded shelters → outbreaks (cholera, respiratory infections)
Social disconnection — separation from family/community
Economic hardship — rebuilding costs, loss of income, lack of insurance
Delayed healthcare — interrupted care for chronic conditions or pregnancy
are nurses mandated to report IPV
NO
purpose of the danger assessment tool for IPV
A validated screening tool used to assess the risk of severe intimate partner violence (IPV) and femicide (homicide of a woman by an intimate partner).
Developed by Jacquelyn Campbell.
Helps healthcare providers identify individuals at high risk and develop safety plans.