language (bio psych)
1/53
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
54 Terms
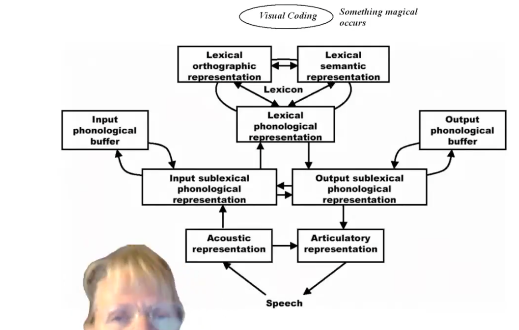
lexicon
"He took his vorpal sword in hand." Nonsense words do not exist in our lexicon (mental dictionary), yet we understand what they're saying because of maintained grammar / sentence structure, that's how we extract meaning from a word.
Mental lexicon is the knowledge of words shared by speakers of a language. We don't know where it is, not in some specific area. But it includes word entries, with grammar, etc. It's personalised.
why look at language
Human language development represents a unique abstraction. Animals don't use it in a unique, generative way like we do.
Language is important part of information processing. We understand concepts not visually but in language-based concepts.
Language is the main means of human communication, and language is not just speech.
Language and perception are interdependent. The way we construct the world around is influenced by language. But also, we change our language to fit with how we understand the world, too.
Language processing is neurologically modular. This allows us to understand how lots and lots of other things happen in the brain.
Everything we do is in language-based code, not as in just speech.
Steve Pinker: language allows us to know.
language as central to identity
For Indigenous populations but also us. How does language contribute to our identity?
There is a growing recognition of Australia's Indigenous languages not only for communication, but also to strengthen identity and self-esteem. Languages are central to our identity, and remaining connected with them is critical to our wellbeing. Need research on link between language and wellbeing.
What about if we lose our language? 250 languages 200 years ago, 145 100 years ago, 120 languages today, with 60 considered 'healthy'.
language is not what we say
It is communication, multi-modal.
It is the way we understand the world, and can be: visual, written, signed, spoken.
Our sense of speech is also strongly dependent upon what our mouth is doing. If you dub a sound such as "ba" onto a video of a mouth saying "ga" what you hear is "da" which is a compromise of the two. This is the McGurk effect which shows that we look at what their whole face is saying, not just speech.
We understand also body language, the world, context.
Our ability to understand language is highly dependent upon top-down processes. So, context is very important.
Top down is the ability to process word depends on other factors in our head. Like the McGurk effect (bottom up wouldn't have it).
e.g. word context. Subsequent context is also important. It was found that the Meal was on the TABLE. It was found that the Heel was on the SHOE. It was found the Peel was on the ORANGE.
This shows ability to understand language is not linear. This word comes 300ms later, yet tells us what that previous word was. It goes back and forth, not linearly step by step.
Word identification is not instantaneous but highly influenced by top down processing. This is dynamic, cascaded, interactive. This is the same with memory, reading, attention, for brain processes.
ASD with language disorders, is more affected by how they use language,
the lexicon and spreading activation model
Morphemes and phonemes are some of the info which is in human mental lexicon. The lexicon is a knowledge of words shared by speakers of a language. The lexicon includes a word's phonemic representation, morphological structure, and meaning.
The lexicon is an abstraction. Clearly something like the lexicon must exist, but how, where, how we access it, and the neurological correlates are still unknown.
We know, as an educated adult, 10-20k words, but you'd recognise about 30k. We stick to tried and true language words, a few thousand. It's how we communicate.
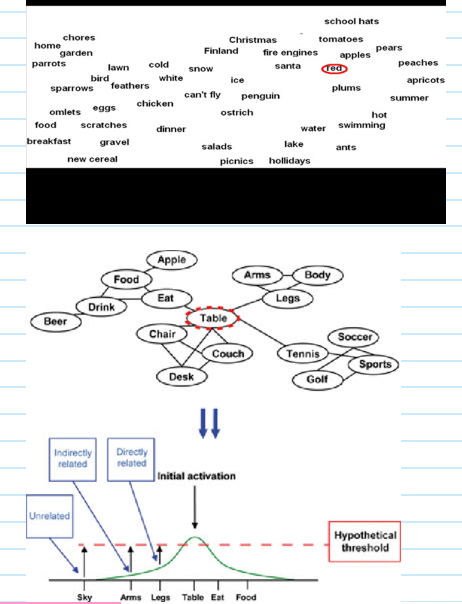
Spreading activation model.
Concepts (and words) are organised in semantic categories.
Semantically related words 'activate' each other so that you will be faster recognising semantically related words (e.g. bread / butter).
Words with similar orthographic 'neighbours' are recognised more slowly.
Some words are easier to access then others (word frequency effect).
That we go from one concept all the way to another.
Some words have a high threshold. But words that come across frequently, have a high initial activation, so will be easily accessed.
It's how our language networks are designed.
Rules of language help us understand the world, but it's specific to us.
neurolinguistics
Language and the brain
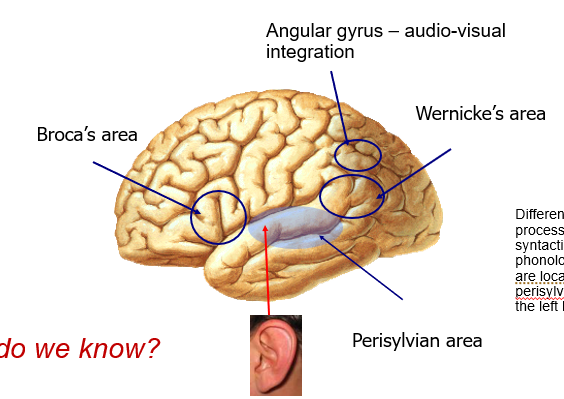
Our very first understanding about the role of brain in language processing was back in 19thC, from Broca and Wernicke.
For the first time Broca and Wernicke identified specific parts of the brain responsible for different aspects of language processing.
We recognised modularity of the brain through recognising language. This extended to other concepts that we recognised are organised, a brain area has a specific function, and is not just 'mush' in the brain. That different parts of the brain are responsible for different things.
Different linguistic processes such as lexical, syntactic and phonological processes are in perisylvian regions of left hemisphere.
lateralisation of language
Language is predominantly a left hemisphere (LH) function.
For most people, language is processed in the left hemisphere.
Pink areas show those most commonly used, even if say occipital lobe, is used in speech.
In deaf people, the cortical areas devoted to sign language are the same as for spoken languages. Same parts light up.
Therefore, the regions of the brain devote to language are specialised for symbolic representation and communication (not specifically spoken, heard, signing language).
Left handed people are less likely to be solely left hemisphere for language, but more spread out. That's why experiments use right handed people.
Ambidexterity is not having consistent left or right hand. They're a scale. You do different things with different hands. Write on paper with right hand, on board with left.
Deaf people would have more visual stuff, blind people would have more motor / touch stuff. But gesture activates Broca's area and visual cortex.
This links to theory of language evolution- that we gestured before we spoke. Use of gesture predates use of tools. Children who sign use the same errors of grammar as speaking kids. We all naturally gesture, even when others aren't looking.
People with damaged Broca's area often also have right-side paralysis, because Broca's area is next to motor cortex.
how we know about wernicke’s and broca’s areas
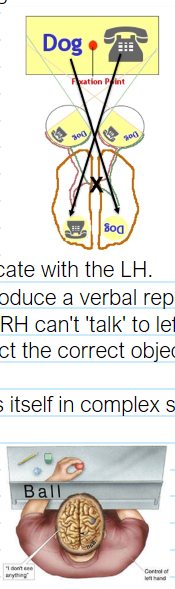
Because of split-brain research.
Commissurotomy for intractable epilepsy. We first identified LH function when epilepsy would get corpus callosum cut.
Information presented to left visual field goes to right hemisphere.
This is lateralisation. This does not show contralateral function here. A thing like left hemisphere controlling right side does.
The RH here can’t communicate with the LH.
So, patients are unable to produce a verbal report of the stimuli.
"ball" projects to the RH, but RH can't 'talk' to left so he will report having not seen it. however, he will select the correct object because RH does not control left arm.
Thus, the RH cannot express itself in complex sentences, but can recognise words / concepts.
To produce and understand as language you'd have to get it to LH. They know the concept but they don't have the language to say the word.
Well, we can do the same thing experimentally without lopping out a piece of your brain. Through behavioural research. Tachistoscopic presentation to left or right hemisphere. Then record aspects of stimuli that subjects can report. Measure RT and accuracy.
Also through neuroimaging. By identifying all sorts of parts of the brain.
what’s the RH for then
Split brain subjects can only make simple semantic judgements.
Disconnect from RH means they have problems with pragmatics (social communication). RH gives you all that stuff, besides the language and context of LH: humour, metaphor, sarcasm, basically difficulties with non-literal / figurative meaning, the reason why singing and prose often spared in aphasia.
The LH figures predominately in the comprehension and production of language, the RH is needed to generate the full richness and ‘colour’ of language.
sensitive period
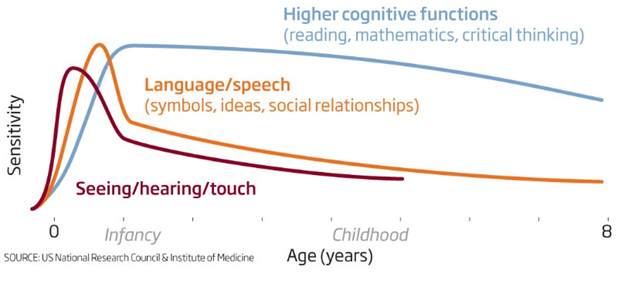
The brain may be especially receptive to language for a short period of time during development. However, if no linguistic input is received, non-linguistic representations may be formed in those cortical areas.
What kind of important is important for normal language development?
Language must be interactive.
And exposed to within sensitive periods. There is one for the acquisition of syntax, between 2 and 4 years. After puberty it may be impossible to acquire fluent syntax.
Genie eventually developed a reasonable vocab, but little to no syntax (she was exposed to language in her teens).
Chelsea from a loving home was diagnosed as retarded. But at 30 she was given hearing aids (was actually deaf) and developed excellent language skills, except no syntax ("the small a hat", "the boat sits water on", "woman is bus going").
But Isabelle, from a similar environment like Genie, was rescued at 6 years and went on to develop near normal language skills.
bilingualism
That aphasia can affect one language but not another, suggests different structures.
But there are some common regions and language-specific regions in the brain.
Electrostimulation studies found both common and language-specific regions.
prosody
Rhythmic, emphatic, melodic aspects of speech.
Prosody in Wernicke's aphasia is normal, not in Broca's.
But it seems even damage to right hemisphere can affect it- they failed to stress a word / stress the wrong one
recognition of people’s voices
Besides language conveying information, prosody about emotion / stress, it also carries identity of the speaker.
Phonagnosia- difficult recognising voices. Usually caused by brain damage in right hemisphere.
is reading innate
Brain innately takes in language. To speak, etc. But, brain is not designed to read! We have to learn.
If we understood what the brain does when we read, it could show us how the brain works. Could tell us about attention, memory, too, and apply to lots of people.
The development of reading and writing makes it possible to communicate over space and time, to understand another person's experiences.
process of reading
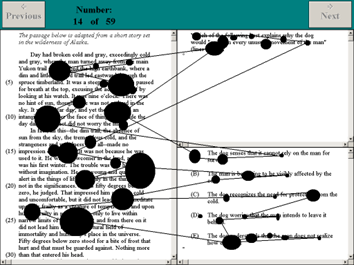
When reading a page of text, the eye moves in a series of small jumps and pauses called saccades and fixations.
The eye also jumps backwards in regressions.
This is evidently not smooth, but occurs very quickly. And only in those few hundred millisecond fixations do we actually take stuff from the page, then process it, etc.
Typical fixation frequency is 3 Hz. Common words get shorter fixations and all information is acquired during fixations.
Bigger circle means longer fixation. See how our eyes move.
Average saccade is 20-50 ms. A fixation can be 150 ms to 1 sec or more, depending on content. Similarly, number of regressions also depends on context.
Fixations are fast and saccades are longer, with fewer regressions, for texts that are 'easy'. Shows that we're working harder to process.
Only during fixation do we have access to information on the page and thus extract.
what happens during a fixation
During a fixation, peripheral cues are important, particularly to the right with up to 15 characters, with about 3 -4 characters to the left. Our attentional window is longer on the right, because we read from left to right. Because this is dependent on the language you are reading in. But also your reading skill and difficulty of the text (we make 10-15% regressions).
Different ways to speed read. But Rapid Serial Visual Presentation (RSVP) isn't a good technique for learning to read faster with such pages of texts.
Reading music is similar to process of reading words.
Adapting a spotlighting mechanism of visual processing and shifting it to allow us to read. This spotlight mechanism / attentional window that shifts us here to the right exists regardless, but we have adapted it to reading. When we learn to read, we learn to use it for this.
models of reading
At some level, reading must involve the accurate recognition of words. We do this through models of reading and word recognition. One is the Dual Route model.
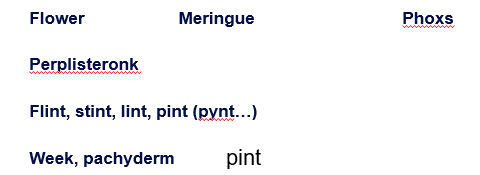
The brain processes all these words differently.
In row three, pint is pronounces pynt because of the context of previous words.
For meringue, we know it's meringue, not meringyou, even though letters don’t reflect it, because we know the word.
Phoxs makes sense for us, because it sounds like a word we know.
Perplisteronk is pronouncable to us.
Week and pachyderm are real words, but week comes easier to us, because it's a higher frequency word.
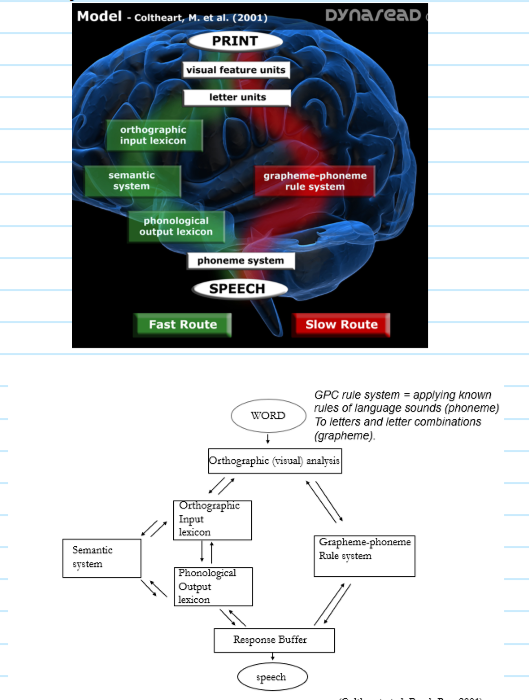
what is the dual route model
The Dual Route model of reading. That there are three routes- lexical semantic route, lexical non-semantic route, GPC route (grapheme-to-phoneme, i.e. sounding out).
The computational version of the dual route model is based on the interactive activation model (spreading?). Each route consists of layers, connections are excitatory and inhibitory.
We either sound words out (GPC, because they're unfamiliar, what letter looks like you sound out its matching phoneme, phonetic reading) or recognise words directly (words you're really familiar with, whole word reading). Meringue doesn’t work through GPC, you have to use the left pathways.
how do we know about this
We know about this because people with acquired brain injury lose the ability to read particular words.
disorder of reading and writing. Relation to aphasia. Wernicke's aphasia and Broca's aphasia, etc. translate to their reading and writing skills.
Acquired phonological alexia means they can't use phonological route. Can only use direct pathway, so this is what happens with an unfamiliar word:
Acquired surface alexia means they can’t use the lexical route. Can't access words directly, and can only sound them out. And so, you can make some regularisation errors with words like meringoo. All happening in 100ms.
Same thing in dyslexia, that one of the pathways was damaged, shows that we have two different ways to process words in the brain.
what about pure alexia
Pure alexia involves damage to left primary visual cortex causes blindness in right visual field. Can't read words at all, but if spelled out, knows them. And could still write. A perception of disorder, like pure word deafness (but visual input). Lesions prevent the visual info to get to visual association cortex of LH.
Damage to left primary visual cortex, but can still read aloud. Because visual word-form area still receives information from left visual field (from right primary visual cortex) through corpus callosum. VWFA is a region of let visual association cortex that analyses info further, and transmits to speech mechanisms in left frontal lobe. Would read slower, needs to turn head. Now, additional damage to posterior corpus callosum interrupts flow of info and produces pure alexia.
Similar thing happened with sign. 'Sign blindness' caused by similar damage to pure alexia.
phonological wars
The phonological wars was that it was inappropriate to teach how to sound words out supposedly, given readers only use direct pathway. So, why teach GPC, especially with so many English words are often so irregular orthographically.
But now, we say we should teach them to sound out, but also…
Children should be exposed to different types of reading material.
Children should be exposed to multiple teaching methods to maintain interest. "Look-see" or "whole-word" methods are necessary for children to develop their lexical route and develop a sight vocabulary (from dual route).
All the scientific research indicates that explicit and systematic instruction in phonics to be intrinsic in learning to read. So, teaching children phonics (decoding, segmenting, blending) both before, during and after instruction in the alphabetic code, is vitally important in children learning to read. Phonics instruction helps develop the phonological route, and give children a life-long strategy to learn new words.
Teach and strengthen both pathways.
The brain did not evolve to read. It's not natural in the way language is. Unlike spoken (or otherwise) language, when reading, the brain recruits different cortical areas otherwise specialised for different functions.
reading as understanding brain mechanisms
Reading is intrinsically interesting, but it is also a valuably way for understanding basic brain mechanisms. The neural dynamics involved in reading can help us understand the way the brain performs in other complex tasks.
like with the word identification problem
word identification problem
We each know as many as 100k word forms. A typical reader identifies 2 or 3 a second. Even with presentation rates as high as 10 per second, word meanings get activated. Identification takes 200 ms.
How is this done?
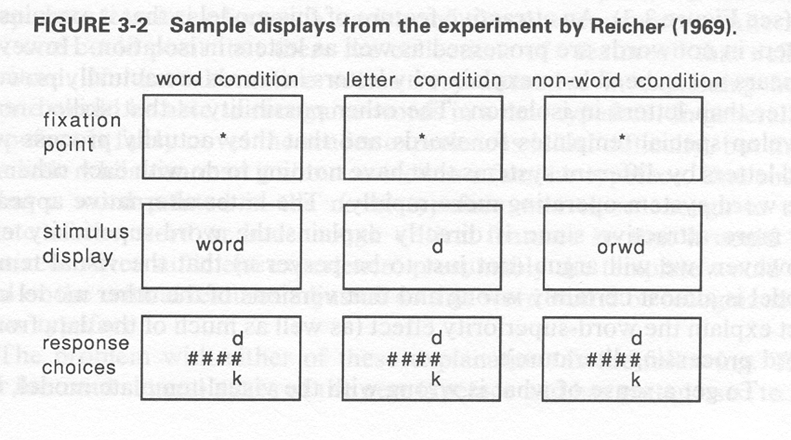
Here, a fixation point is given. Then a word, then hashtags and either a d or k (e.g.) to say which (single letter) was in that location. You have to know what the word was to know whether d or k.
There was also a letter condition and non-word condition.
Word condition was fastest, then non-word, then letter. Because context that it is presented in, makes all the difference. We do not recognise word as W-O-R-D, letter by letter, but spreading activation means that by the time you get to D, the whole WORD is activated. It is not linear, that is why.
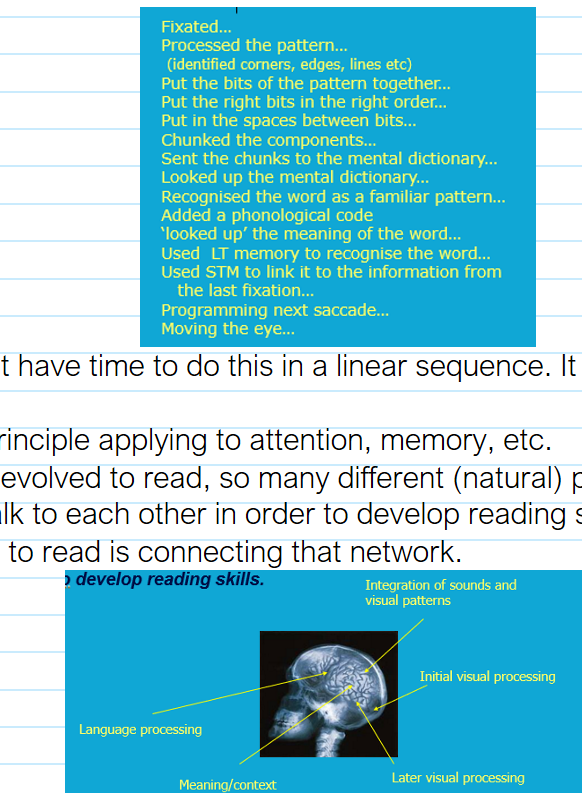
Recall how fast the saccades and fixations happen. Therefore, within about 350 ms has…
The brain does not have time to do this in a linear sequence. It has to be interactive.
This becomes a principle applying to attention, memory, etc.
The brain has not evolved to read, so many different (natural) parts of the brain need to learn to talk to each other in order to develop reading skills. Creating a network. Learning to read is connecting that network.

First letter consistently preserved, as well as often end ones. We can read this, because of context. Like a dyslexic reader, reading this way slower- more fixations, more regression, shorter saccades.
aphasias
Diminish or abolish the ability to comprehend and/or produce language, while sparing the ability to perceive relevant stimuli and to produce intelligible words
Is NOT a result of hearing loss, and is NOT the result of damage to motor control.
Successful treatment dependent on: Time after trauma, Age, Education level, Handedness (?).
Intervention: speech therapists, Fast ForWord (?) is controversial and scientific outcomes have proven difficult to replicate.
broca’s aphasia
Paul Broca conducted an autopsy on a man, Tan (Mr Leborgne), who had been mute for 29 years. He could understand most of what was said to him, but would only ever respond with "tan tan " and various gestures.
Realised something was going on here with language processing.
Mr Leborgne has sustained and severe damage to inferior left pre-frontal cortex. That's the first clue for localisation of language function in the brain, that the brain was modular. That knocking out a specific area, meant you would lose a specific function.
Left precentral gyrus of insula (deep in lateral sulcus, the fissure separating temporal lobe from frontal and parietal), it's critical to speech articulation. Those with apraxia of speech had damage to same general area of brain (impairment in ability to program movements of tongue/lips/thought needed to produce speech).
Tip of the tongue phenomenon, difficulty getting a word out. And if they often have a TOT experience, showed loss of gray matter in left insular cortex.
characteristics of broca’s aphasia
Speech is agrammatical.
Speech is effortful, telegraphic, sparse, repetitive.
E.g., “well I had trouble with…oh, almost everything that happened from the…eh, eh…golly…the word I can remember, you know, is ah…when I had the…ah…biggest…a…that I had the trouble with, you know…that I had the trouble with,…" (told to tell a story based on an image as a test; the ability to produce speech is impaired, everything else is fine but this (production), through a damaged Broca's area).
Word finding difficult is anomia. They have articulation difficulties.
But comprehension is maintained.
So this is a problem in the production of speech.
wernicke’s aphasia
Carl Wernicke, practising around the same time, recognised this was not the whole story
He was particularly interested in patients who had comprehension problems, rather than production problems.
Such patients consistently showed brain damage to left poster, temporal lobe, mid temporal gyrus. Wernicke's area.
An over-ability to create speech, but you can't understand because you Wernicke's area is damaged.
characteristics of wernicke’s aphasia
Language production is maintained.
Language if fluent and effortless.
Problem with understanding (spoken word recognition). Consists of symptoms of pure word deafness- different in that their own speech makes sense but also can't understand what people are saying. Caused by either disruption of auditory input to superior temporal cortex or damage to it itself. Our brain has mirror neurons- activated when we either perform an action or see others do it. Seems to affect speech perception, as well as feedback from speech movements.
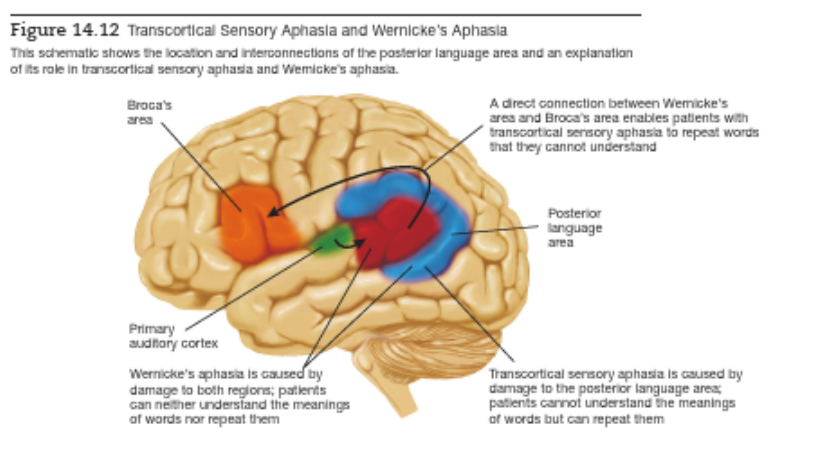
And it appears devoid of meaning. They don't know they're not making sense. Deficits in language comprehension- can't comprehend meaning of words nor express meaningfully. Damage beyond Wernicke's area, to posterior language area.
Damage to posterior language area alone is transcortical sensory aphasia (so Wernicke's aphasia also consists of symptoms of this). They can repeat what other people say to them (they can recognise word), but they still can't comprehend the meaning of it, nor produce meaningful speech. Can repeat because it doesn't involve this part of the brain. There must be direct connection between Wernicke's and Broca's that bypasses posterior language area.
Can't convert thoughts into words. One type of aphasia is pure anomia (anomic aphasia)- fluent and grammatical, but comprehension is excellent, and also can't find appropriate words, so they use circumlocutions (speak in a roundabout way). Almost like a partial amnesia for words. Anomia, alone, seems to be left temporal / parietal lobe, sparing Wernicke's area. See the differences and similarities with Wernicke's.
E.g., “Boy, I’m sweating, I’m awful nervous, you know, once in a while I get caught up, I can’t mention the tarripoi, a month ago, quite a little, I’ve done a lot well, I impose a lot, while, on the other hand, you know what I mean, I have to run around, look it over, trebbin and all that sort of stuff…”
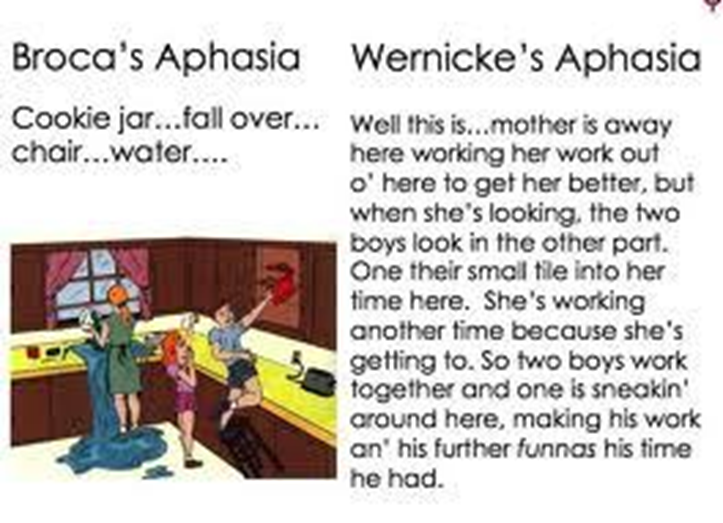
Also told to tell a story as a test from an image. They make up words and have a word salad.
compare wernicke’s and broca’s aphasia on quality of spontaneous speech, word comprehension, repetition, naming, reading comprehension, writing, location of lesion
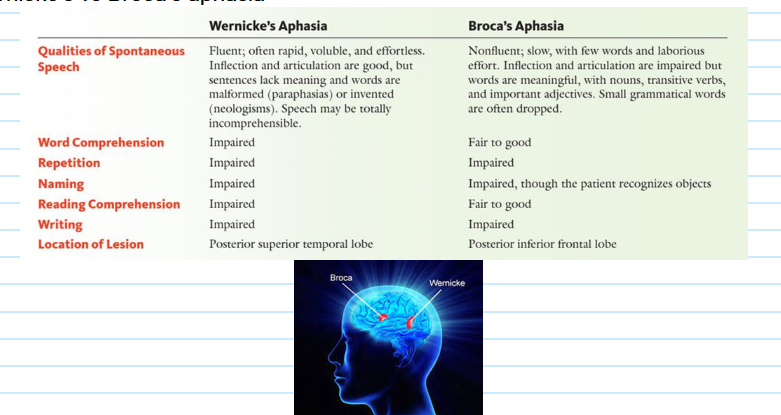
wernicke’s and broca’s aphasia
They have quite distinct behavioural manifestations. Often we get something among the two, etc., so these two aphasia are the most 'extremes' allowing for most specific mapping onto specific areas in the brain. Shows that cognition isn't just distributed throughout the brain. There's modularity.
People with Broca's aphasia are aware they're not getting their point across. Wernicke's aphasia doesn't realise, so they don't really struggle as much with anxiety. Broca’s has significant anxiety because immediacy of expression struggle.
This is acquired language impairment.
Possible transient version of Broca's aphasia.
Aphasia affects both reading and writing.
When you damage Broca's area, you often also damage motor cortex, too, because it sits next to it. That's why they often have paralysis on right side of their body.
Broca's aphasia might try writing to read something but doesn't work. Trying.
Experience varies of aphasia, where you just say tan to struggling to say real words (B), or expressing full words to just babbling (W).
Non-fluent aphasia, AKA Broca’s aphasia.
conduction aphasia
That connection / pathway between Wernicke's area and Broca's area is the arcuate fasciculus. Bundle of axons, in both directions, the phonological loop.
Conveys info about sounds of words not meanings.
Evidence from conduction aphasia- meaningful, fluent speech and good comprehension but very poor repetition. Can't repeat non words or three unrelated word phrase. Or will repeat a word related to it (house, will say home).
Implies an important role in STM of words and speech sounds just heard.
Transcortical sensory aphasia and conduction aphasia show that there are pathways connecting the speech mechanisms of temporal lobe with those of frontal lobe.
Arcuate fasciculus conveys speech sounds from Wernicke's to Broca's area.
That second but INDIRECT pathway is with posterior language area, based on meaning of words.
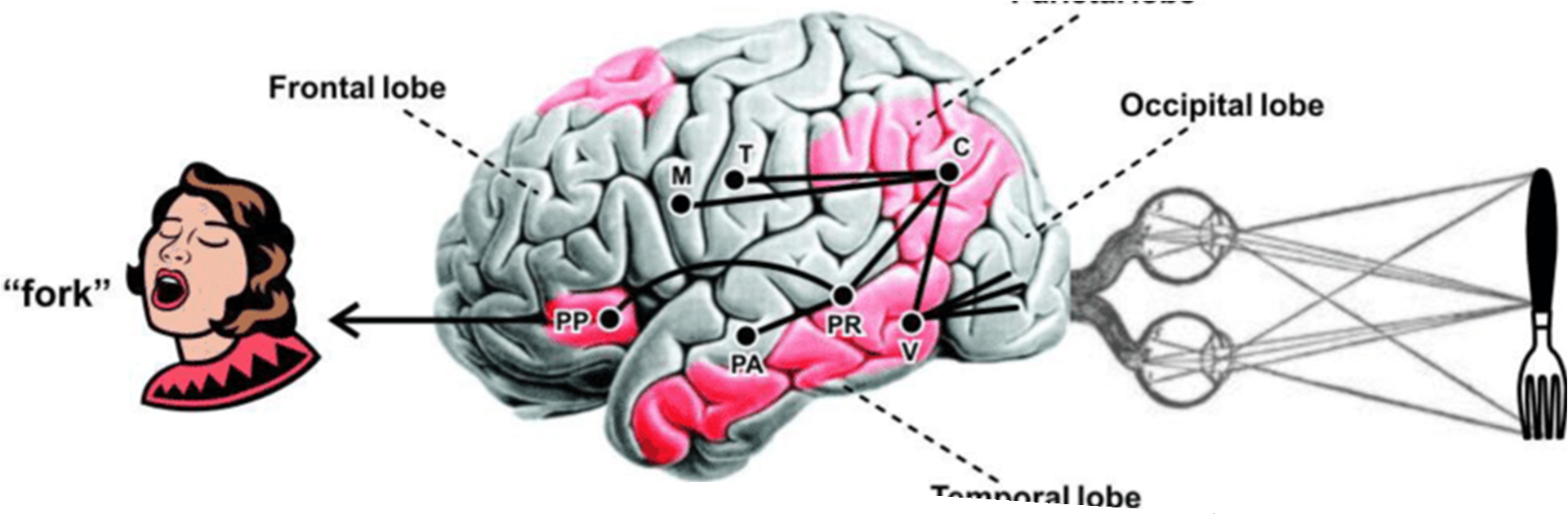
Comprehension of speech: flow of info from Wernicke's to posterior language area to various regions of sensory and motor association cortices containing memories that provide meaning to words.
Production of spontaneous speech: flow of info concerning perceptions and memories from sensory and motor association cortices to posterior language area to Broca's area.
We talk to ourselves through Broca's area.
aphasia in people who are deaf
Deaf kids also babble in sign. Wernicke’s aphasia struggle is not to create speech, but to create comprehensive speech (because they can't understand speech). There appears to be different degrees of understanding other people’s speech (probably making gestures could help?).
Some of these neurons for learning hand gestures, observing and imitating, are in Broca's area.
That spoken language evolved from hand gestures.
That grammar of ASL is spatial suggests that aphasic disorders in people who use sign language exclusively might have lesions in right hemisphere (spatial perception and memory).
But still things that involve language activate same regions of LH.
SLI
SLI is developmental(ly normal?). The delayed language, as either receptive (following basic instructions, understanding sentences) and expressive (generating language, RAN (rapid automatic naming), category naming).
Difficult with understanding or producing language shows it's based on those language areas that exist ^.
50% comorbidity with dyslexia.
Same sort of definition as dyslexia (definition of exclusion), but for language rather than reading.
Not speech apraxia, or pragmatic language impairment.
About 7% of the population. Males more than females. Genetic.
possible cause of SLI
Are the networks misaligned? Not firing quick enough? Dyslexia and SLI questions.
Auditory Sampling Hypothesis (may also apply to dyslexia).
Language has a rhythm to it, with highs and lows, peaks and troughs at about 3 Hz. Auditory parts of brain perhaps don’t sample that as well as they should. But, understanding or picking up on those subtle differences is vital for language network to be developed, so this might be impaired.
stuttering
Characterised by repeating movements and fixed postures of the speech mechanisms.
Tends to run in families, so genetic component. Especially if your father has it.
Onset is in childhood and affects about 5% of children. Most grow out of it.
Recovery characteristics are unclear. Girls tend to recover more often than boys, recovery prognosis is better if recover starts soon after onset.
Stuttering is also developmentally normal, brain trying to figure out how to use it. so what is developmentally normal vs problem.
cause of stuttering
Cause is unknown.
Stutters do not seem to differ from non-stutterers in any other sense (IQ, coordination). Except for the presence of social anxiety.
Causes are likely to be the result of difference in the brain involved in starting and/or stopping motor signals involved in speech.
Movement release. Stronger activation in motor cortex on right side on stutterers. May represent interruptions in speech-motor programs (overactivation, impaired).
Mouth movement. Stutterers may fail to develop LH control (dominance) of speech, instead with bilateral activation.
Movement coordination. They might also have overactivation of cerebellum. Timing and motor control by cerebellum is impaired.
See that this is a less of a deficit, but an overactivation.
Therapy. Have stutterers listen to their stutter but slowed down, so it helps them to reprogram, for that onset offset. Delayed auditory feedback.
william’s syndrome
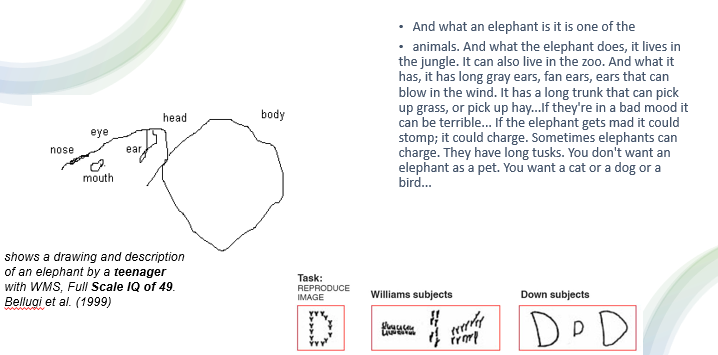
Not strictly a disorder of language. A genetic disorder with a number of physical characteristics, mental retardation (low IQ), below average visuo-spatial skills / awareness (can't draw, do arithmetic, use scissors/ knives), poor social cognition (no fear of strangers, highly social and empathetic).
That's why we would use down syndrome as control group (low IQ).
cause of william’s syndrome
A consequence of missing some genetic material.
Spontaneous deletion of 26-28 genes on chromosome #7.
One of the 25 missing genes is the gene that produces elastin, a protein that allows blood vessels and other tissues in body to stretch. Likely to account for some of the presentation.
language skills of william’s syndrome
Intriguing thing, is despite mental retardation, language skills are normal. Huge discrepancy between their IQ and language skills.
Excellent vocabulary, normal grammar, expressive and articulate: E.g., Downs syndrome child (“Dogs, cats, fish, bird, fish”), WS child (“Brontosaurus, tyranadon, brontasaurus rex, dinosaurs, elephant, dog, cat, lion, baby hippopotamus, ibex, whale, bull, yak, zebra, puppy, kitten, tiger, koala, dragon"). When asked to think of all the animals they can think of (generating language).
Rich and expansive story-telling skills. This creating story based on image is the Boston aphasia test and is also used here.
Although semantics often are slightly off: “I will have to evacuate it” in describing pouring out a jug of water.
Modular preservation of language, they are also highly musical.
Can barely hold a pen. See the difference in drawing versus verbal expression of a concept (e.g. elephant).
dyslexia
Applied aspect of bio psych as dyslexia.
About 10% of population can be diagnosed as dyslexic.
For an individual to be diagnosed as dyslexic they must show: read substantially below average for their age, adequate teaching exposure, adequate socio-economic opportunity (reading is a reasonably normal expectation there, no adverse experiences that could deprioritise reading), no disturbance of an organic origin (mental retardation, autism), normal to above average IQ.
So, we consider child a dyslexic when there's no other obvious explanation for reading difficulty.
This is a definition of exclusion- it's an experimental one / for research purposes, useful for identification and communication purposes, but impractical for the real world. e.g. can a child from an emotionally challenging background, or a child with ADHD, have dyslexia? This type of definition is important for understanding brain mechanisms, what's in the brain for a dyslexic vs non-dyslexic reader, because you need to know that that's what you're looking at. If we allow comorbidity with other factors and disorders it makes it difficult to isolate.
Thinking that they're stupid. But they're not. They just struggle to read.
Help dyslexia by… Working out your own strategy, compensating. Reading difficulty is still there. Also trying to find a thing that they're passionate about and giving them that to read, makes a huge difference. Developing neural networks necessary to read. Because in dyslexia they don’t develop as well as they could (it's a developmental disorder).
how dyslexia works (language-based problem)
People think dyslexia is reading backwards or the words moving over the page or not being able to see words properly. But in most cases this actually describes a different disorder- visual discomfort.
Dyslexia is primarily a difficulty in phonics / phonological awareness / phonological decoding. Phonemic awareness is the awareness that language is made up of individual and unique sounds. Reading ultimately involves associating sounds that we know (phonics) with squiggles on a page.
It's about recognising that each word we use is unique. Sounds are concatenated to form full word. Ability to manipulate and pull apart those sounds is phonemic awareness. Because learning to read is to associate sounds in our head with arbitrary squiggles on a page.
Most dyslexic readers have problems in tasks that require phonological decoding. e.g. In pre-readers phonological awareness is the best predictor of later reading ability. Problems in blending, segmenting, odd-one-out tasks, spoonerisms, rhyme, reading non-words. Phonological intervention strategies seem to be most successful. Difficulties discriminating between similar phonemes (sounds). These are difficulties in pulling apart and manipulating language (above ^, e.g. take 'c' out of 'cat' what is the sound now?).
phonological dyslexia
Now why do they have these difficulties? Not just adults with ABI, but kids with dyslexia show same difficulties with dual route model. Dyslexic have one route undeveloped. GPC rules is the route we use when learning to read, reading unfamiliar words. Phonological dyslexia (remember it's developmental disorder, not acquired, born with), can't use the phonological route. Can't sound out new words, thus learn new words, and manipulate sounds of language. They rely on knowing what words look like. That's more okay for when you already know how to read, but to learn those words in the first place, to learn to read, is really difficult.
Most kids have a version of phonological dyslexia.
surface dyslexia
Surface dyslexia is much rarer, where they can't use lexical route. So they can't visually recognise words. Most children have a bit of both. But you would get more pure form of phonological dyslexia.
Difficulty in phonological processes is because of a deficit.
direct dyslexia
Direct dyslexia resembles transcortical sensory aphasia, but the words are written not spoken. They can read aloud, but not understand the words they are saying.
dyslexia is also a visual problem
Most research has been language-based. That this is a language problem. That's true. But there is also a visual part.
There are complex mental models of word recognition, but an assumption that something visual also happens. Not that it just goes from visual cortex straight to brain. Something could be happening there. If there was something up with the visual coding, it would have impacts for later brain mechanisms in reading. If visual coding isn't right, which is at the start of this process, then when learning to read, it'll have a knock on and affect all the other processes when trying to read.
Dyslexia was originally considered to be a difficult in visual processing! But this belief was abandoned when dyslexic readers were consistently shown to have normal vision (so moved to language-based processing).
dorsal stream deficit theory of dyslexia
Interest in a visual basis for dyslexia was re-ignited in the 70s and 80s, when it was demonstrated that many dyslexic readers show a deficit in processing visual info carried by dorsal stream of visual system (this part isn't normally measured by optometrists). Called transient deficit theory of dyslexia, then magno-deficit theory of dyslexia, dorsal stream deficit theory of dyslexia.
Process of reading in dyslexia.
Eye fixation pattern differs in a characteristic way from those of normal readers. Dyslexic readers fixate longer on words (and saccades are shorter) and demonstrate more regressive eye movements. Fixations are less stable in dyslexic readers. Abnormal eye movements, compared to normal readers. Poor binocular convergence.
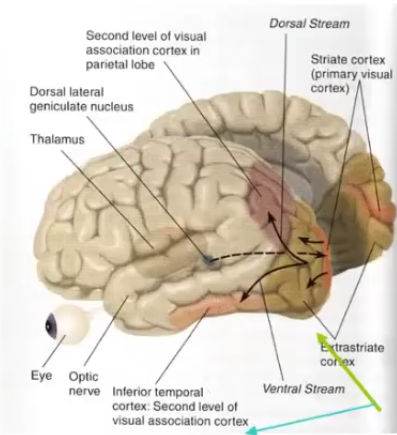
We have two pathways from the eyes to the visual cortex- dorsal (magno cells) and ventral pathways (parvo cells). Each of these carries different types of information.
Ventral stream: colour sensitive, detail, movement insensitive, higher contrast, slow. The what and where, the details.
Dorsal stream: colour insensitive, global form, movement sensitive, spatial processing, lower contrast, fast.
Evolutionarily, when something is new and catches your attention, it picks up movement (dorsal stream), reporting that something is there. Then ventral stream kicks in, it's slower, and gives the detail (it's a leopard over there).
Yet it's dorsal stream that's impaired. They have difficulty processing info that needs to be transmitted by dorsal stream. Doesn't make sense why it's not ventral stream.
how do we know it’s the dorsal stream?
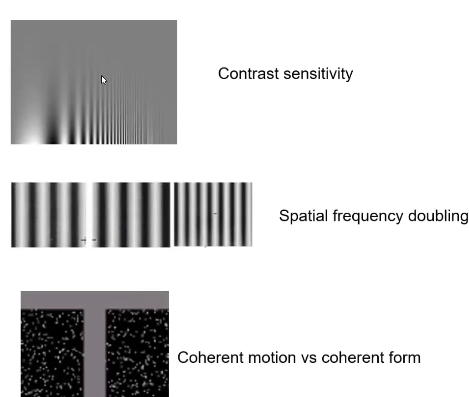
We use tasks that tap into one of the pathways.
Contrast sensitivity is how sensitive eye is to black and white contrast at different spatial frequencies (something that's high detail is high spatial frequency). Variations tap into the two different pathways. So, dyslexic kids have difficulty with the context sensitivity that is unique to dorsal pathway.
We also use coherent motion vs coherent form. Showing dots moving across the screen, we can measure how sensitive they are to it (because dorsal stream is responsible). Less sensitive to it, more likely to have impaired dorsal stream. Have to say in which direction the dots are moving (what is your psychophysical threshold, they're all moving randomly, but a group are moving in one direction, if you're highly sensitive you only need a few to see movement, if you're not sensitive you'd need a lot to say they're moving in a direction). Normal is 15 -20% of the dots moving coherently, dyslexia would need 80%- thresholds.
And tasks show no problem with ventral stream.
do we know how dorsal stream contributes to learning to read
no.
Could be: The dorsal stream may provide feedback information in the form of pre-attentive spatial coding. Because it has to take all these squiggles on the page and arrange in the mind as the letters, and in the order for the word, and the order of words, which requires sophisticated spatial processing. Must know where things are relative to each other.
So, the dorsal stream isolates important regions of space, and feeds this info to the ventral system. The ventral system then uses this info to spotlight text and construct words.
And/or… Also possible idea that dorsal stream may guide saccades across the page. That it is the spotlight mechanism. Because you're learning to control that spotlight. That's why their eye movements in dyslexia are squirrelly.
Children at risk for dyslexia (haven't even learned to read yet, don't have reading pathways yet, so no reading difficulty) also less sensitive to tasks that require magnocellular processing. And such sensitivity can predict subsequent reading skill. Also, people who are illiterate (never learnt to read, not a reading difficulty) don't have dorsal processing problem ('normal').
So, the visual impairment impacts the subsequent development of reading pathways. Not that failing to read affects development of visual system. Because this visual processing through dorsal pathway exists before they can read. Something causal about visual processing in dyslexia.
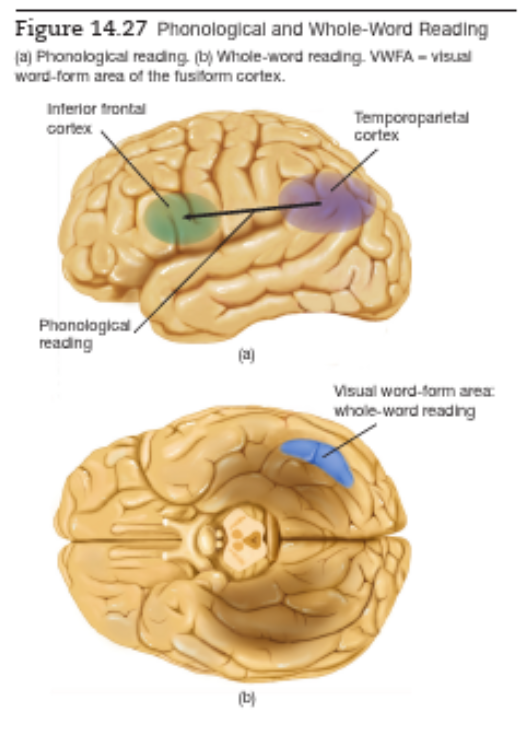
visual word form area vwfa
Whole word reading follows ventral stream to a region, fusiform gyrus, at base of temporal lobe. This is the VWFA.
Fusiform gyrus, part of it, also involves perception of faces and other shapes that require EXPERTISE to distinguish. Must be an expert at things, not that it's face-specific. And recognising whole words requires expertise.
Yet people with visual agnosia (can't recognise objects) can still read, so involves different mechanisms still.
Damage to VWFA alone produces pure alexia. While phonological reading uses temporoparietal cortex (hearing, sounding out), VWFA is essential in both forms of reading.
That phonological / phonetic reading uses Broca's area suggests it uses articulation, not so much that we hear them in our heads. Remember how FEEDBACK from inferior frontal cortex plays a role in speech perception.
Once words have been identified, by either way, the two pathways converge on regions of brain involved in recognition of word meaning, grammatical structure, semantics.
Damage to VWFA producing surface dyslexia, whole-word reading.
Plasticity in visual word form area. That we co-opt / appropriate brain regions for new purpose and allows us to learn to read and write. That VWFA- originally that region- for recognising objects by learning configuration of lines (straight, curved) and their conjunctions, and then evolved with us writing, it recycled into VWFA. Writing is a new invention.
developmental dyslexias
Specific language learning disorders. Never become fluent readers, but intelligent. Suggests a genetic component. Genes on chromosomes 3, 6, 15.
That writing is a new invention shows that natural selection didn't give us brain mechanisms whose only role is to interpret written language. Don't expect development dyslexia only involves deficits in reading.
Also deficient in phonological awareness (blending / rearranging sounds), difficult in writing.
Likely has more than one cause, but found most had phonological impairments. Saw hyperactivation of left inferior frontal cortex, including Broca's area, see the effort to decode phonology of incomplete information received from poorly functioning regions of more posterior regions involved in reading.
dysgraphia
f they can’t express themselves, they'll likely have difficulty writing (dysgraphia). Dyslexia often also has dysgraphia.
A type of writing disorder involving motor control, ability to spell words. Resulting from aphasias.
Writing involves more than one method.
Audition. Learn to recognise sounds of words, learn to say them, learn to read (and subvocalization), learn to write it.
Vision. Copying a visual mental image. Some might not use phonologically spelling but write on whether it look correct- visual not acoustical memories.
Memorisation. Memorising sequence of letter names, not translating sounds into corresponding letters.
Motor memory. Memorising motor sequences of very familiar words, like our name / signature. While the other three methods are the same to writing or typing. Motor memory is different for writing and typing. You can have typing disturbed (distypia), but still write fine.
Neural basis. Brain damage can impair phonetic / audition writing- phonological dysgraphia. Can't sound out words and write them phonetically, but can use visual. Any brain damage to phonological processing and articulation (Broca, ventral precentral gyrus, insula). Orthographic dysgraphia is for visually based writing. Like surface dyslexia is due to damage to VWFA. Also memorisation shown to have neural basis, damage to LH. If one method is damaged, they could use another method.
Direct dysgraphia is like direct dyslexia but for writing.
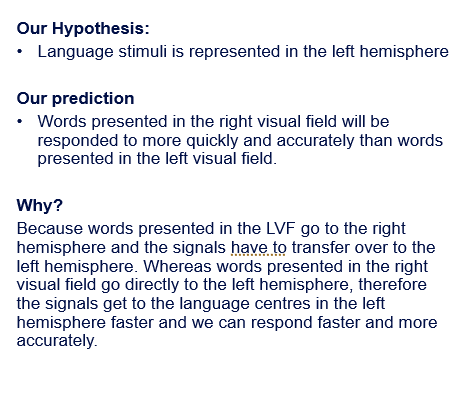
week eight tute- visual half field experiment
fixating on cross and not looking at word, so we don’t make a saccade to the word. Would be important because both visual fields would get access to it. Not one visual field that we're trying to test at a time.
lexical decision task- is it a real or non word? Would be important because we're testing the speed with which we recognise / decide something as a word or not shows the speed with which what we see from our visual field has gotten processed. Language lateralisation.
you’d expect RVF to do better?