BIPC Week 7 (Eating Disorders)
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
biological factors contributing to eating disorders
NT: 5HT, DA, NE
Neuroendocrine: thyroid function
Hormonal: estrogen, progesterone and testosterone
Brain structure: medial orbitofrontal cortex, insula, and striatum involved
Infection: PANDAS (Pediatric Autoimmune Neuropsychiatric Disorder associated with Streptococcal infection)
psychological factors contributing to eating disorders
- perfectionism
- body image dissatisfaction
- behavioral instability
- PMH of anxiety
Categories of Eating Disorders (that we are focused on)
1) Anorexia nervosa (AN)
2) Bulimia nervosa (BN)
3) Binge eating disorder (BED)
anorexia nervosa dx criteria
- restriction of energy intake (FOOD) relative to requirements, leading to significantly low body weight ("less than minimally normal")
- intense fear of gaining weight
- lack of recognition of the seriousness of the current low body weight
restricting type anorexia nervosa
weight loss is accomplished primarily through dieting, fasting and/or excessive exercise, no binging/purging in the last 3 months
binge eating/purging type anorexia nervosa
during the last 3 months the individual has engaged in recurrent episodes of binge eating or purging behaviors (i.e. self induced vomiting, or the misuse of laxatives, diuretics, or enemas)
what accounts for most deaths from anorexia nervosa
medical complications (the heart shuts down)
Mortality rate of anorexia nervosa is 5-10%... one of the highest in psychiatric disorders
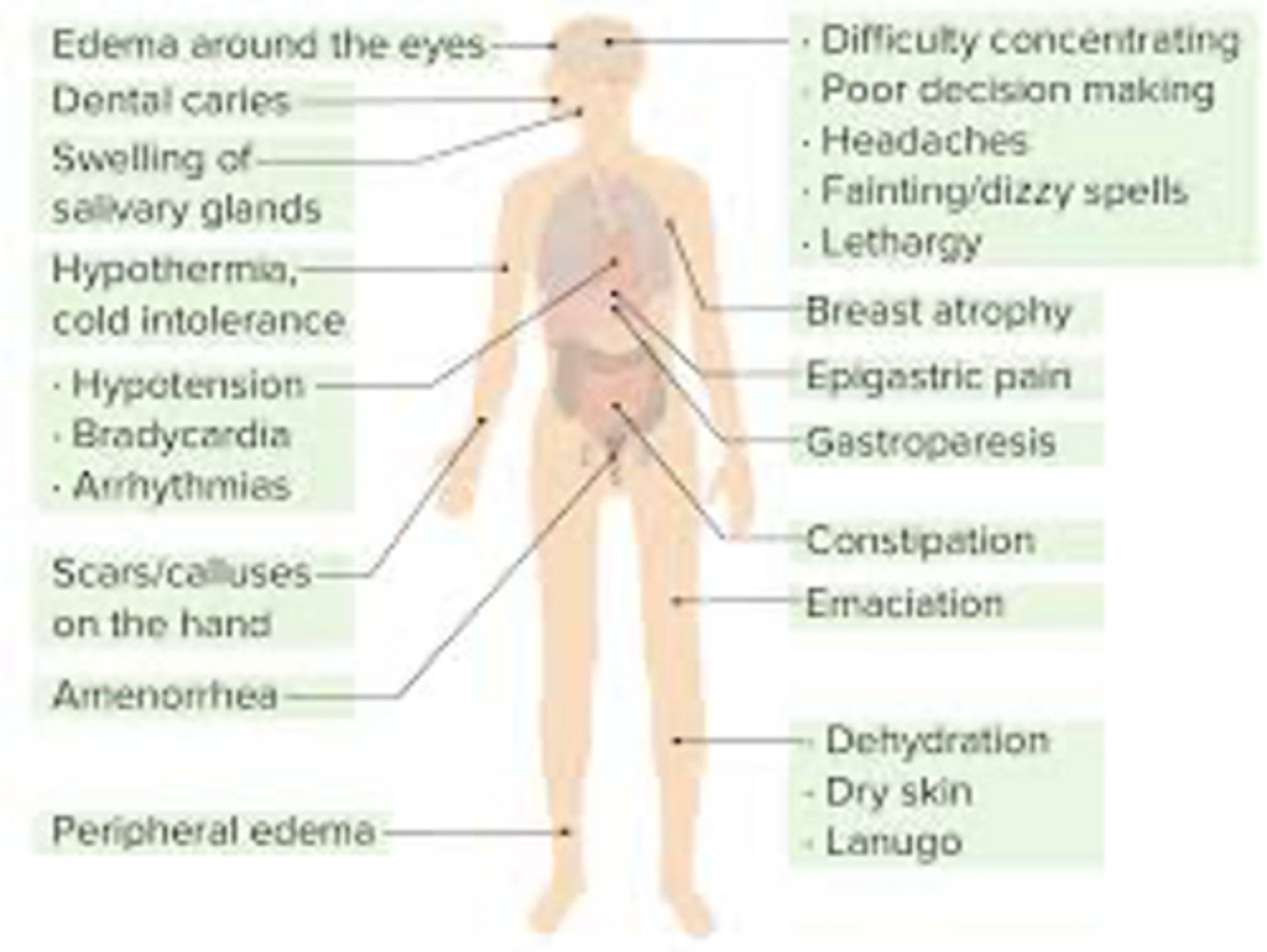
anorexia nervosa sx
- Marked weight loss, gain, fluctuations or unexplained change in growth curve or BMI percentiles in a child or adolescent
- Delayed or interrupted pubertal development
- Cold intolerance
- Hypothermia
- Weakness
- Fatigue or lethargy
- Presyncope
- Syncope
- Difficulty concentrating
- Amenorrhea
Clinical features of AN - Signs (know this well)
BMI <17.5, or <5th percentile amenorrhea
hypothermia
bradycardia
QTc prolongation
heart blocks, MVP, orthostasis,
osteopenia, stress fractures
lanugo (face/trunk), hair thinning, nail/skin changes
erosion of teeth enamel
parotid gland swelling elevated cholesterol, cachectic, increased bony prominence (decreased fat)
tests for anorexia nervosa (know this well)
VS - hypothermia, bradycardia, hypotension and/or orthostatic hypotension + BMI!
Labs - CBC with diff (leukopenia, anemia), INCR amylase bc vomiting, TFT's - T3 can be low, r/o hyperthyroid, r/o T1DM, r/o neoplasm etc.
electrolytes (hypokalemia, hyponatremia, hypochloremia, hypophosphatemia*), renal function (elevated BUN - dehydration), elevated cholesterol, urinalysis- dehydration, + ketones - starvation
- Hormonal levels if menstrual irregularities, testosterone in males
- DEXA scan: osteopenia (late sign)
- ECG: especially in electrolyte abnormalities
anorexia nervosa tx
medical treatment:
- weight restoration (avoid re-feeding syndrome) often inpatient but may be partial hospitalization
behavioral therapy: CBT and interpersonal therapy
pharmacotherapy: antidepressants (fluoxetine), anti-anxiety meds, pro-motility meds (Reglan), antipsychotics (olanzapine)
*treat any co-morbid conditions*
most common cause of death with AN?
cardiac events
difference between binge eating/purging type anorexia nervosa and bulimia nervosa
the anorexia one will have extremely low body weight
bulimia nervosa - usually normal to overweight
bulimia nervosa
Recurrent episodes of binge eating. Characterized by both:
1. Eating within 2 hours a large amount of food.
2. Lack of control over the eating during the episode.
Recurrent compensatory behaviors to try and prevent weight gain (purging, fasting, excessive exercise)
Behaviors occur at least 1x a month for 3 months.
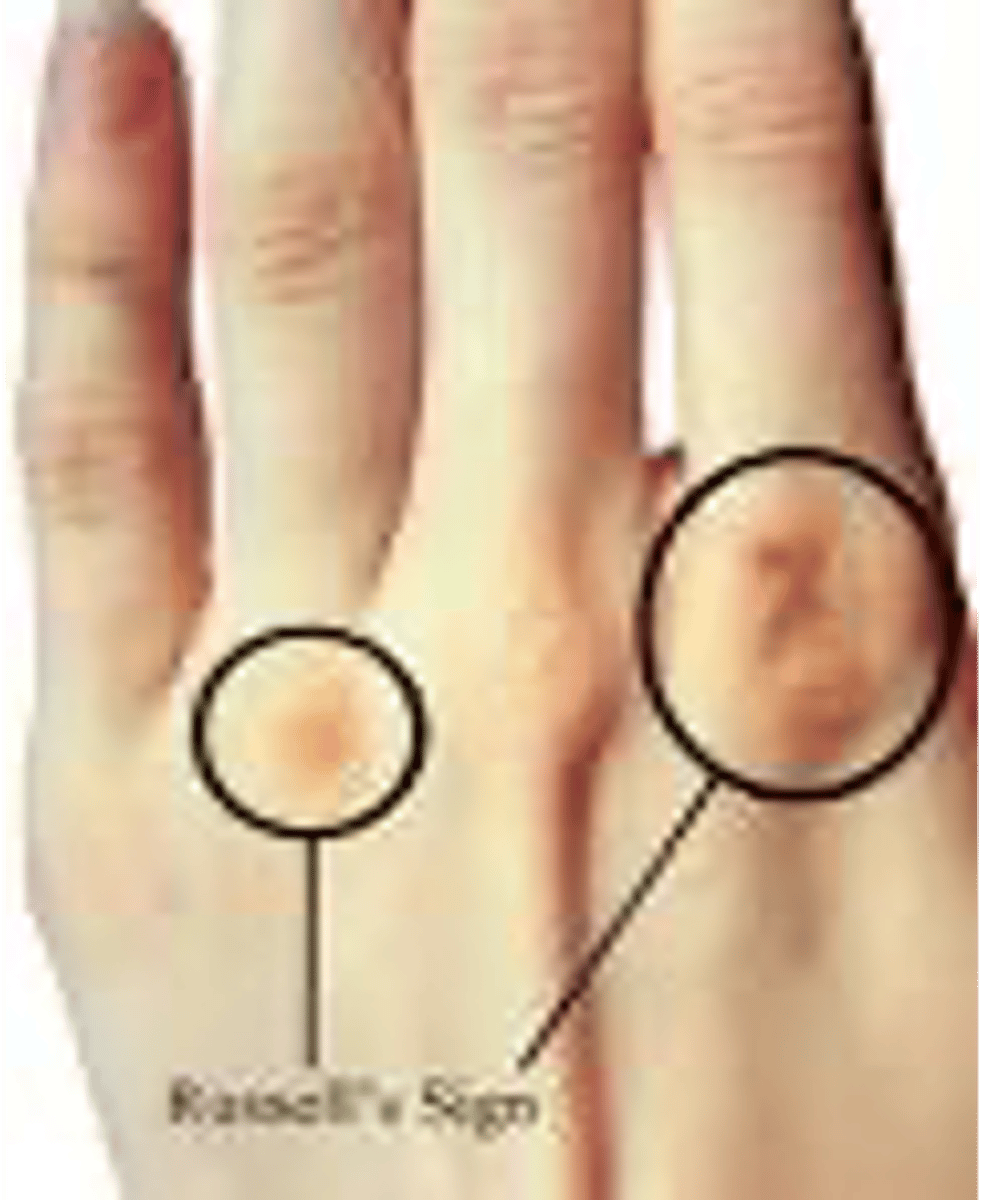
clinical features of bulimia nervosa (KNOW)
Similar to AN as well as:
Oral and Dental issues: parotid gland enlargement, periodontal disease and dental caries
Russell's sign (dominant hand - cause of self induced vomiting)
clinical features of bulimia nervosa labs
Electrolytes: hypokalemia, elevations in serum bicarbonate.
Hypomagnesemia
Higher serum amylase.
Laxatives abuse > chronic diarrhea > metabolic acidosis resulting in hypophosphatemia and hyponatremia
________ is common in bulimia nervosa
prognosis?
relapse
Poorer prognosis in pts with untreated co morbidities like SUD, depression and personality disorders.
symptom picture of bulimia nervosa
what is the most common eating disorder in the US?
binge eating disorder
binge eating disorder criteria
A. Recurrent episodes of Binge Eating
• Eating w/in 2 hr large amt of food
• Lack of control over eating
B. Other sx (3 or More):
-Eating much more rapidly than normal
-Until uncomfortably full
-Eating large amounts of food when not physically hungry
-Eating alone due to embarresment
-Feeling disgusted w/ oneself, depressed/ very guilty afterward.
C. Marked distress regarding binges
D. Binges occur at least 1x a week for 3 months
Clinical features of BED - PE
• Blood pressure
• BMI
• Blood glucose
• Examine for physical or sexual abuse if there is high suspicion
• Eating disorder scales/inventories
SCOFF eating disorder screening
S Do you make yourself SICK (vomit) because you feel uncomfortably full?
C Do you worry that you have lost CONTROL over how much you eat?
O Have you recently lost > ONE stone (14 lbs) in a 3-month period?
F Do you believe yourself to be FAT when others say you are thin?
F Would you say that FOOD dominates your life?
levels of care for eating disorders
- Inpatient Treatment
- Residential Treatment
- Partial Hospitalization Program
- Intensive Outpatient Program
- Outpatient Treatment
multidisciplinary team approach to eating disorders
- Primary care/medical
providers
- Psychiatry/psychopharmacology providers
- Psychotherapy providers
(individual & family)
- Nutrition therapy providers
pharmacotherapy for anorexia nervosa (KNOW)
treat coexisting disorders with SSRIs or antipsychotics
pharmacotherapy for bulimia nervosa (KNOW)
Only FDA approved med is fluoxetine (Prozac)
*Avoid the use of bupropion (Wellbutrin) -> lowers seizure threshold
pharmacotherapy for binge eating disorder (KNOW)
- stimulants (Vyvanse)
- antidepressants (Effexor)
- antiseizure
psychotherapy for eating disorders
- Cognitive behavior therapy
- Dialectical behavior therapy
- Interpersonal therapy
- Family therapy
what is the role of the PA in managing a patient with an eating disorder?
Recognize - "dieting", weight fluctuations, co-morbidities
Educate - family, societal, media pressures, healthy eating
Refer - if you suspect refer to psychiatry
Monitor - "gatekeeper"
Support/encourage: patient and family
Offer thorough, ongoing preliminary screening