Projections
1/25
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
26 Terms
AP Humerus
greater tubercle in profile proximally, epicondyles in profile distally (external rotation)

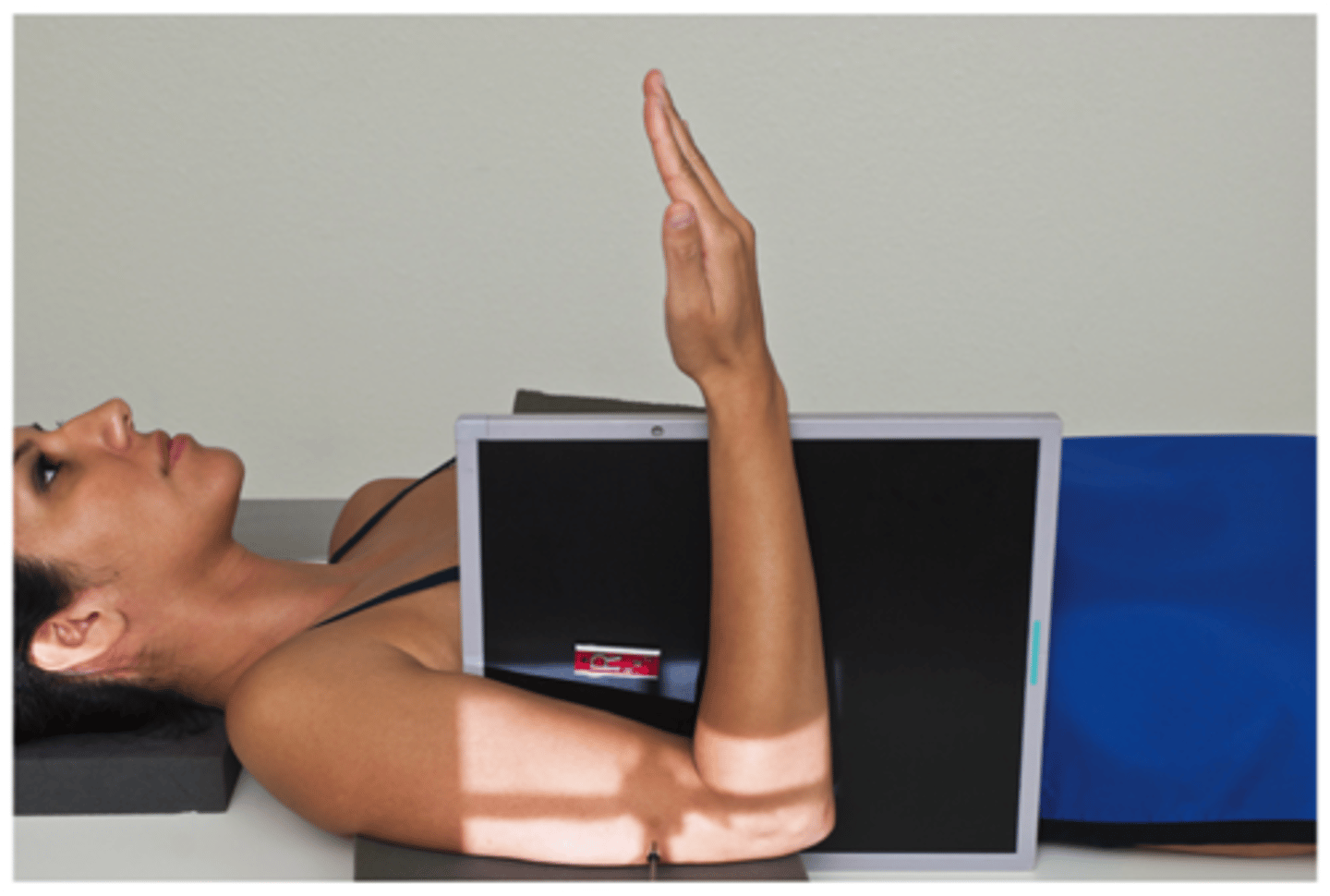
Mediolateral Humerus
used to see top of humeral head
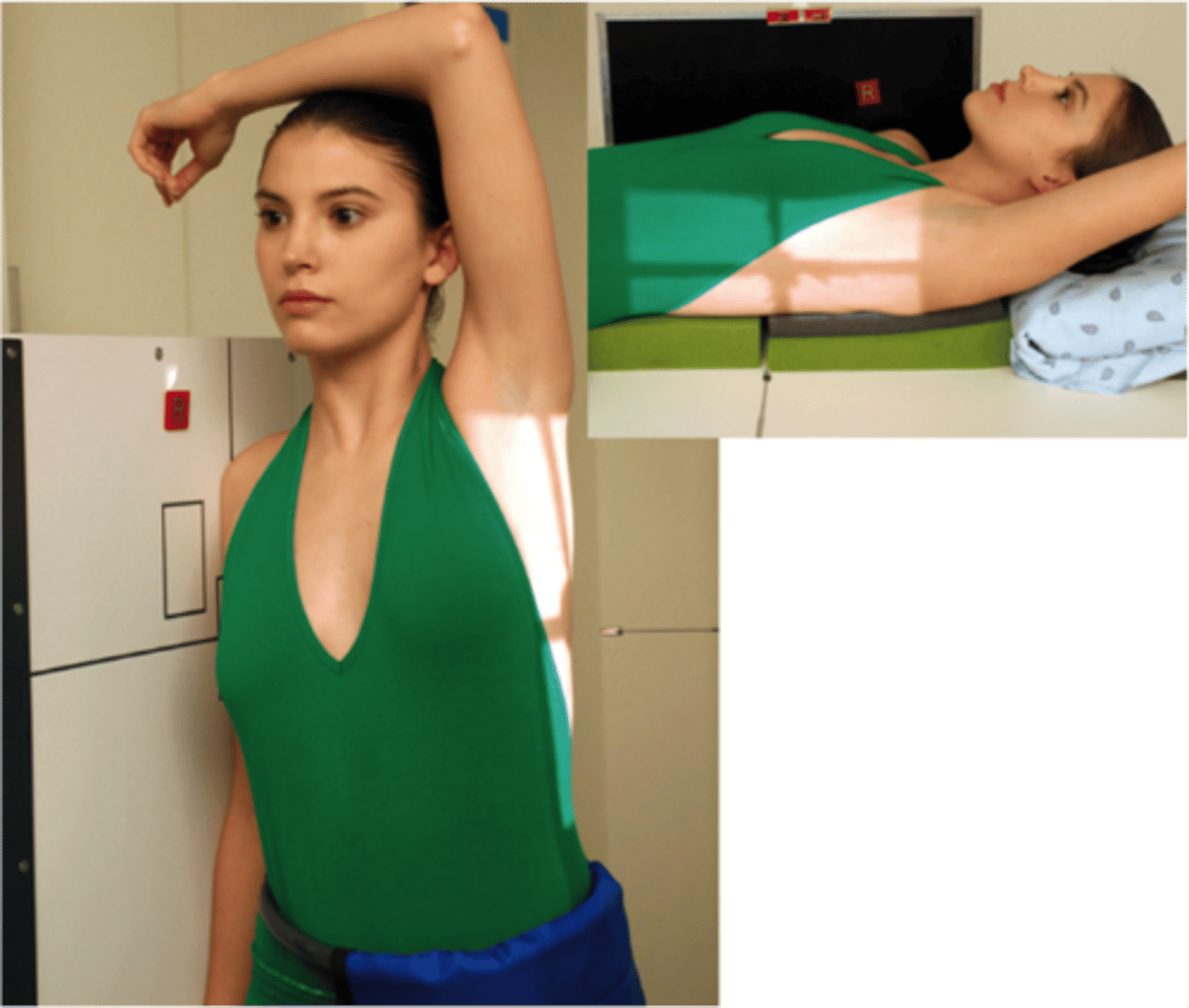
Lateromedial Humerus
lesser tubercle in profile medially (internal rotation)
Trauma Lateral Distal Humerus
should be able to see 3 concentric circles
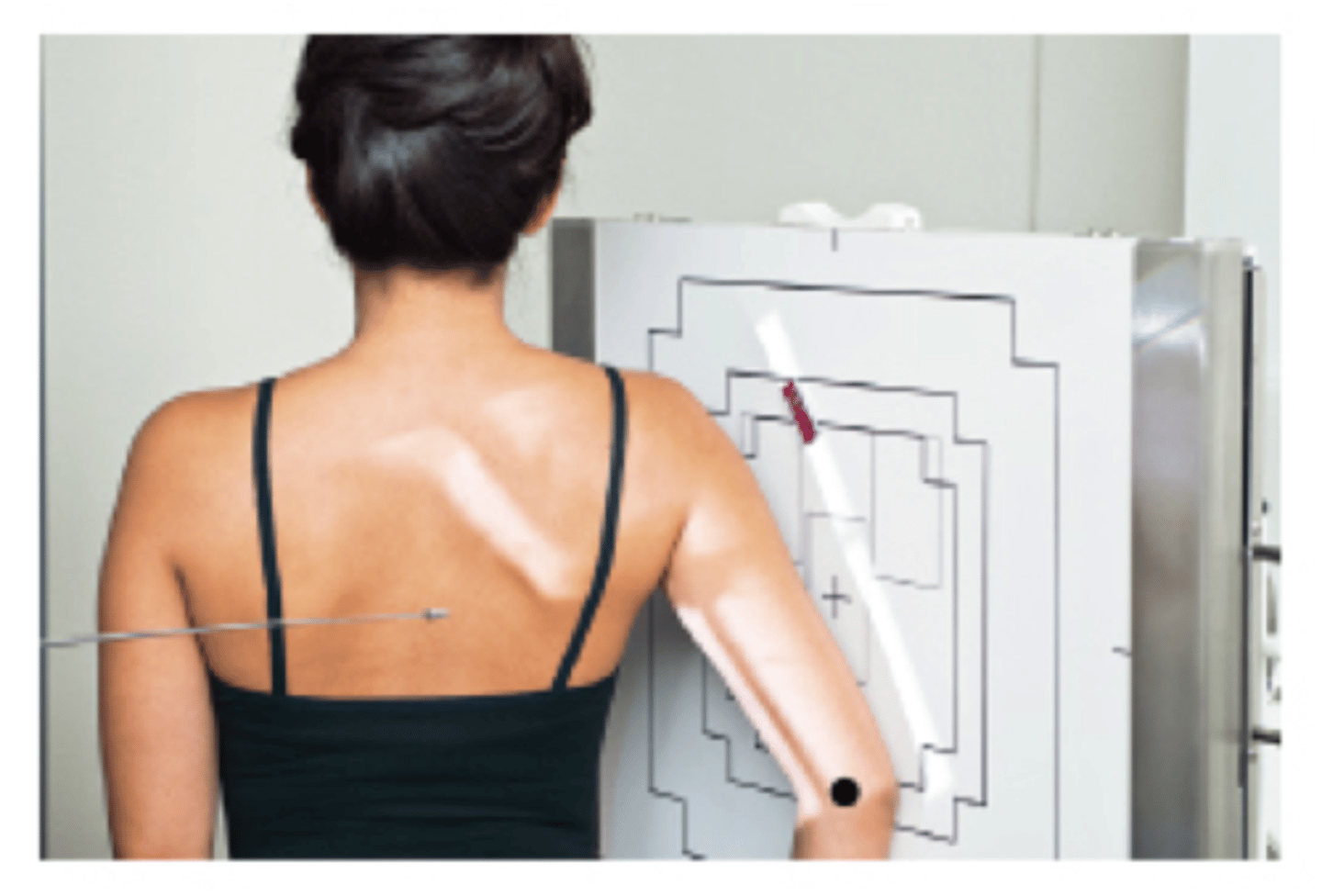
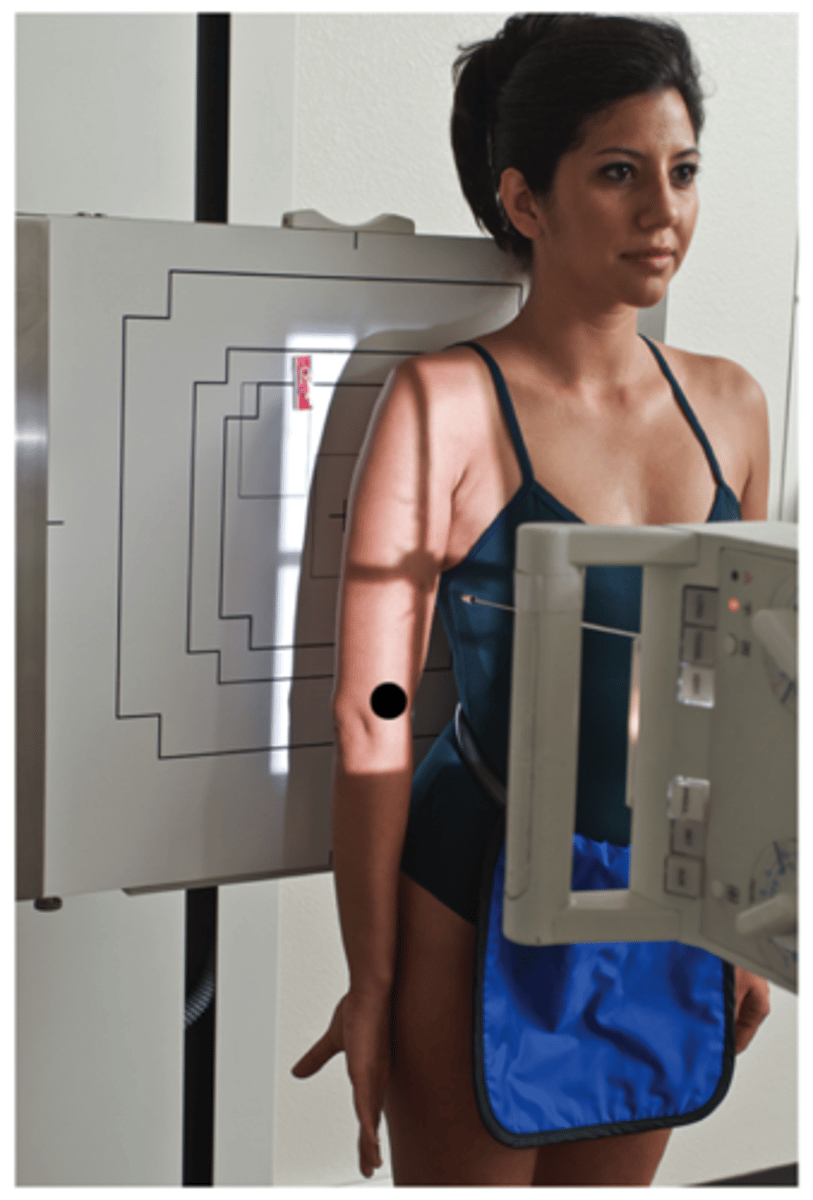
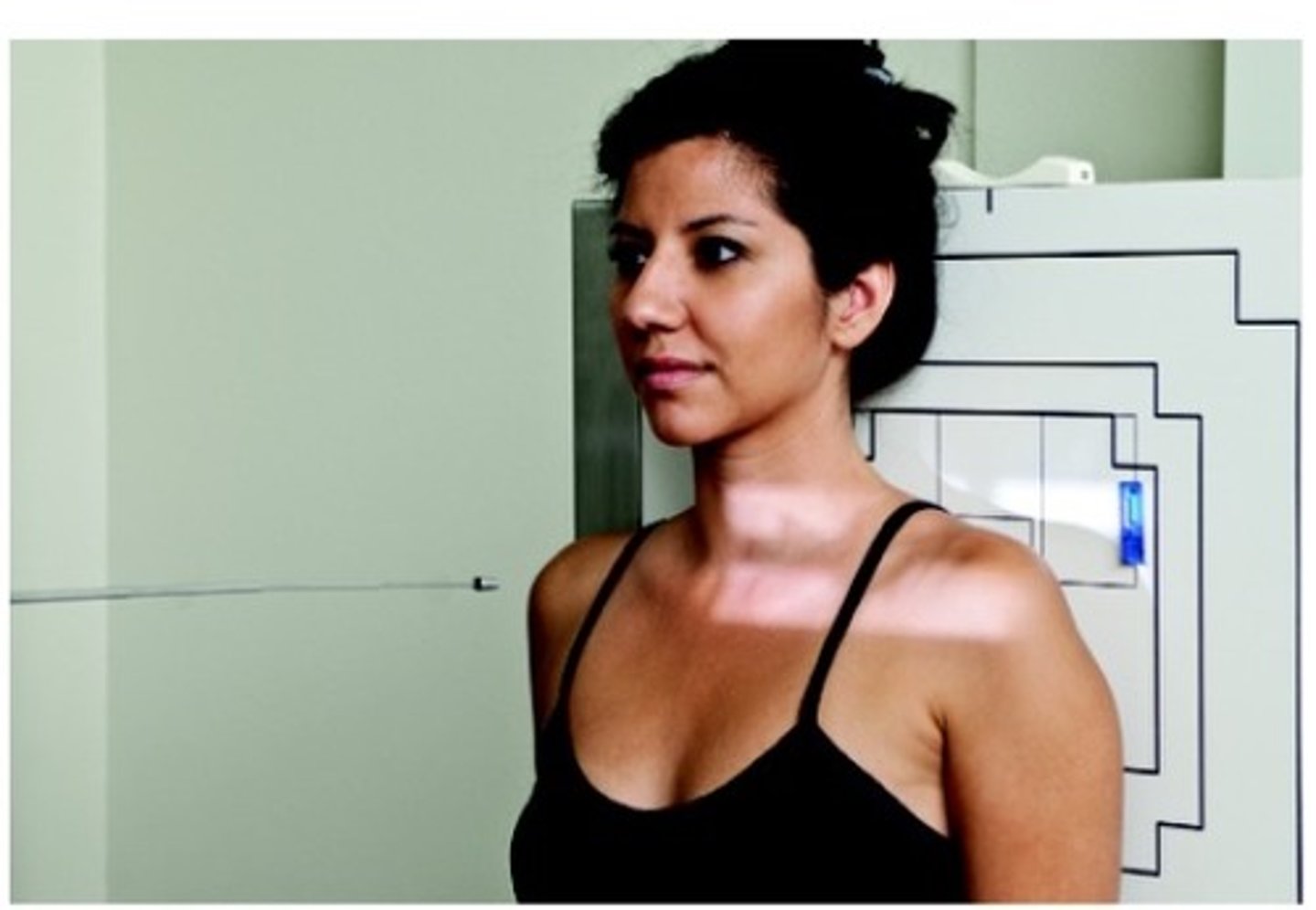
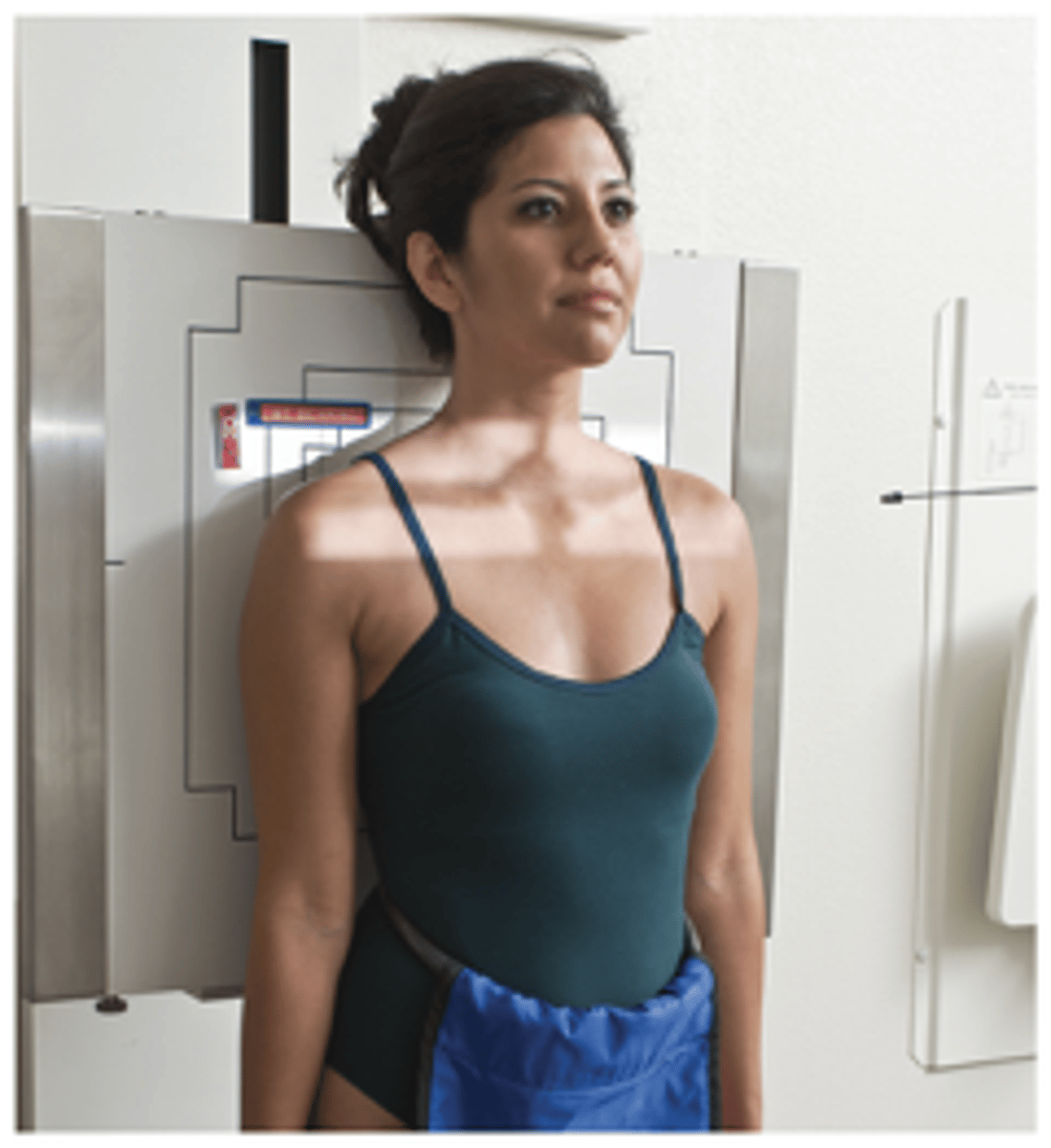
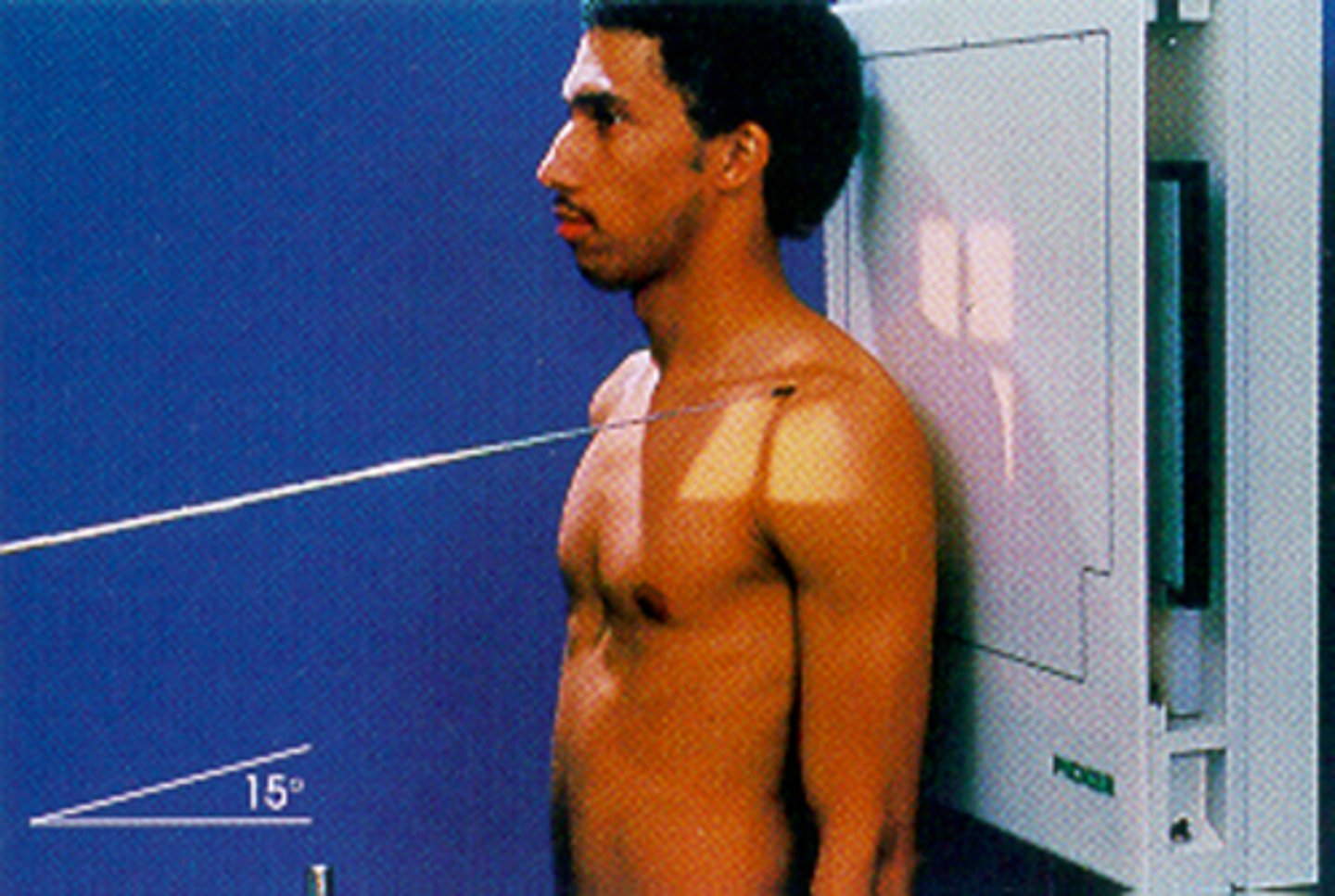
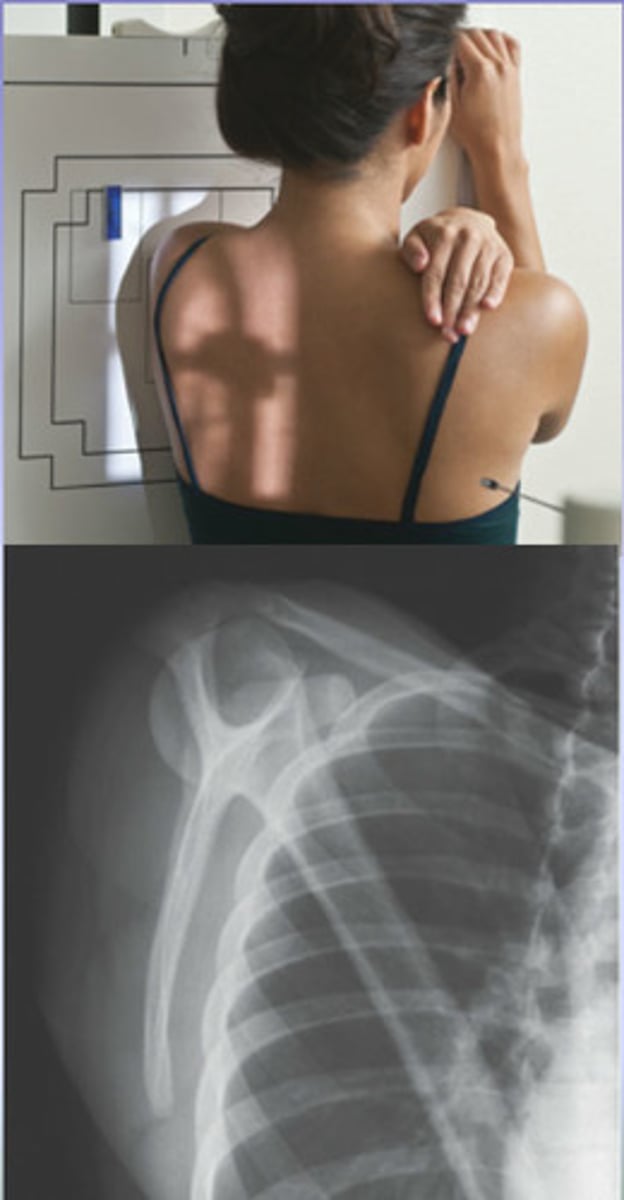
Trauma Transthoracic Lateral Humerus
used to see shaft fractures of the humerus, orthostatic breathing technique, 10-15° cephalic angle if patient cannot raise arm
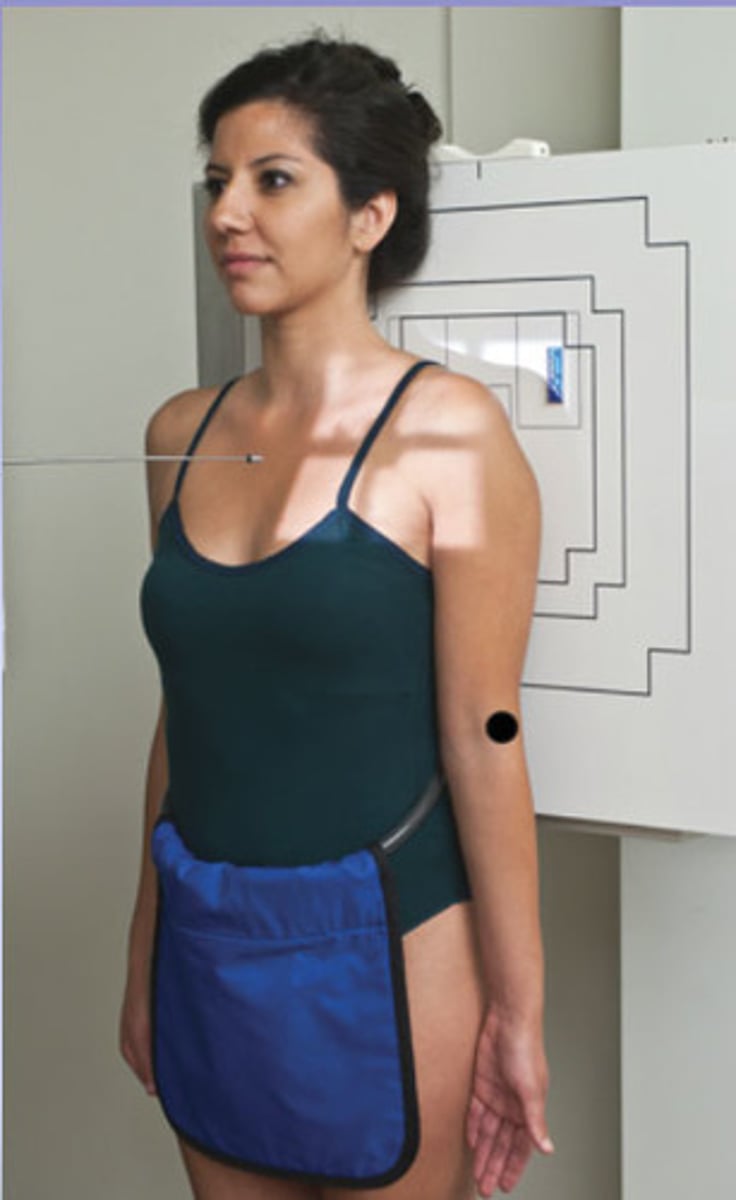
AP shoulder external rotation
used to see the relationship of the humeral head to the glenoid fossa, greater tubercle in profile on lateral humerus, lesser tubercle superimposed over humerus
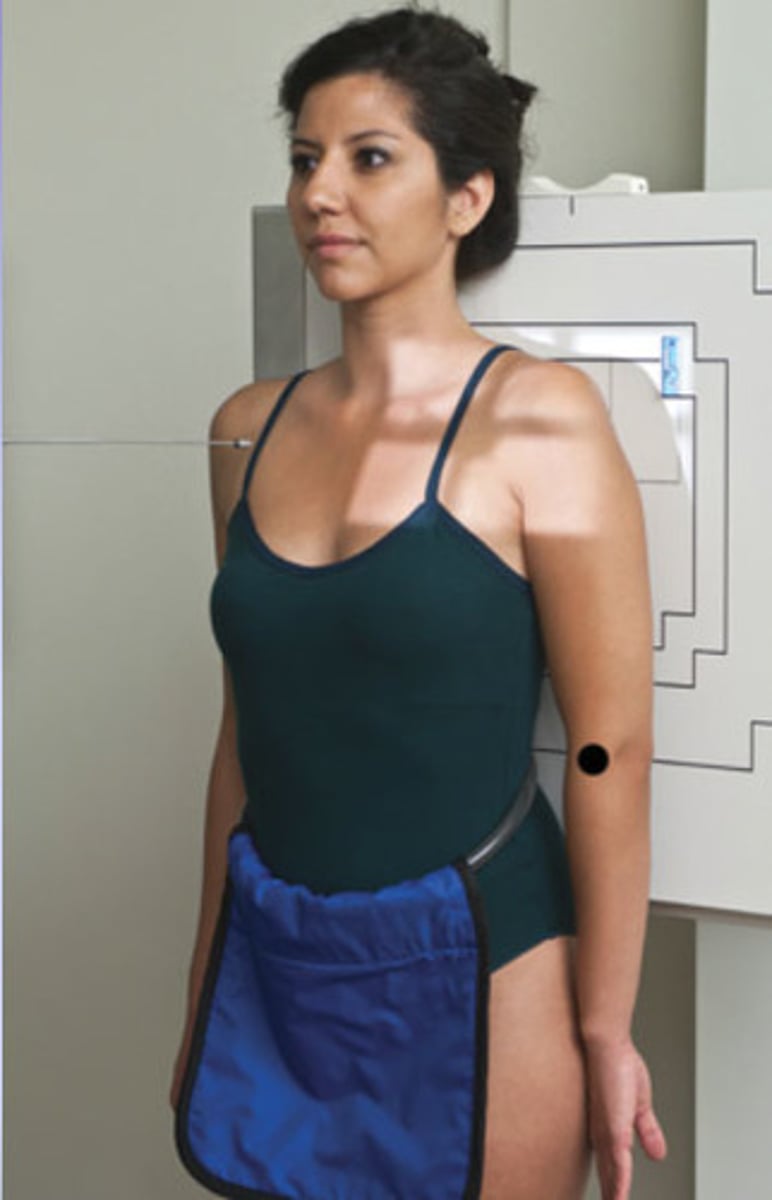
AP shoulder internal rotation
used to see the relationship of the humeral head to glenoid fossa, lesser tubercle in profile on medial humerus, greater tubercle superimposed over humerus
Lawrence Method (inferosuperior axial shoulder)
CR angled 25-30° medially, coracoid process and lesser tubercle in profile (can see Hill-Sachs defect if it is exaggerated)

Hobbs Method (PA transaxillary shoulder)
Patient is 5-10° anterior oblique, lateral proximal humerus in relation to glenohumeral joint, coracoid process seen on end
Clements Method
hill-sachs defect, if patient cannot abduct arm 90° then angle CR 5-10°
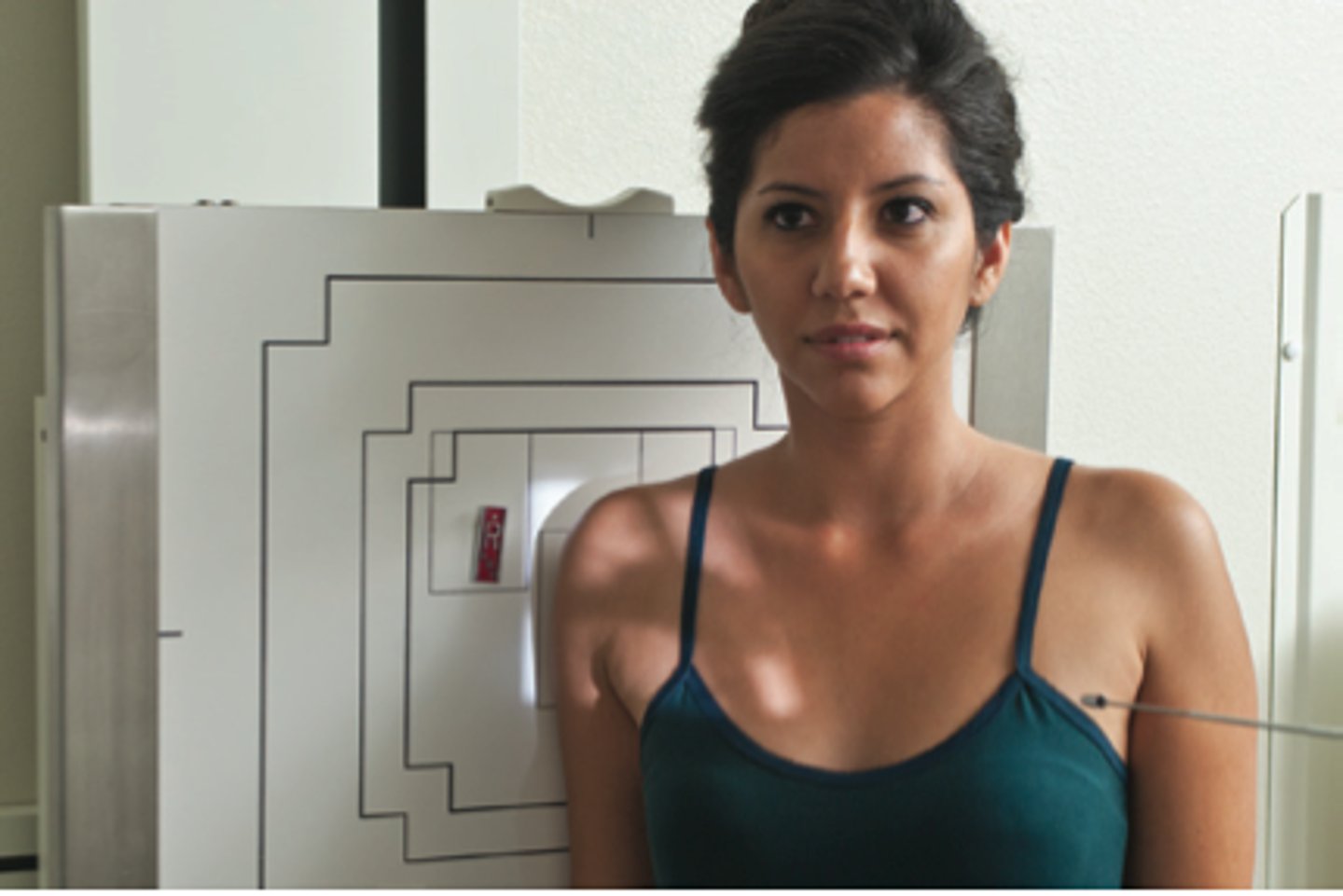
Grashey Shoulder
Patient angled 35-45° toward affected side, used to rule out bankart lesion, glenoid cavity in profile
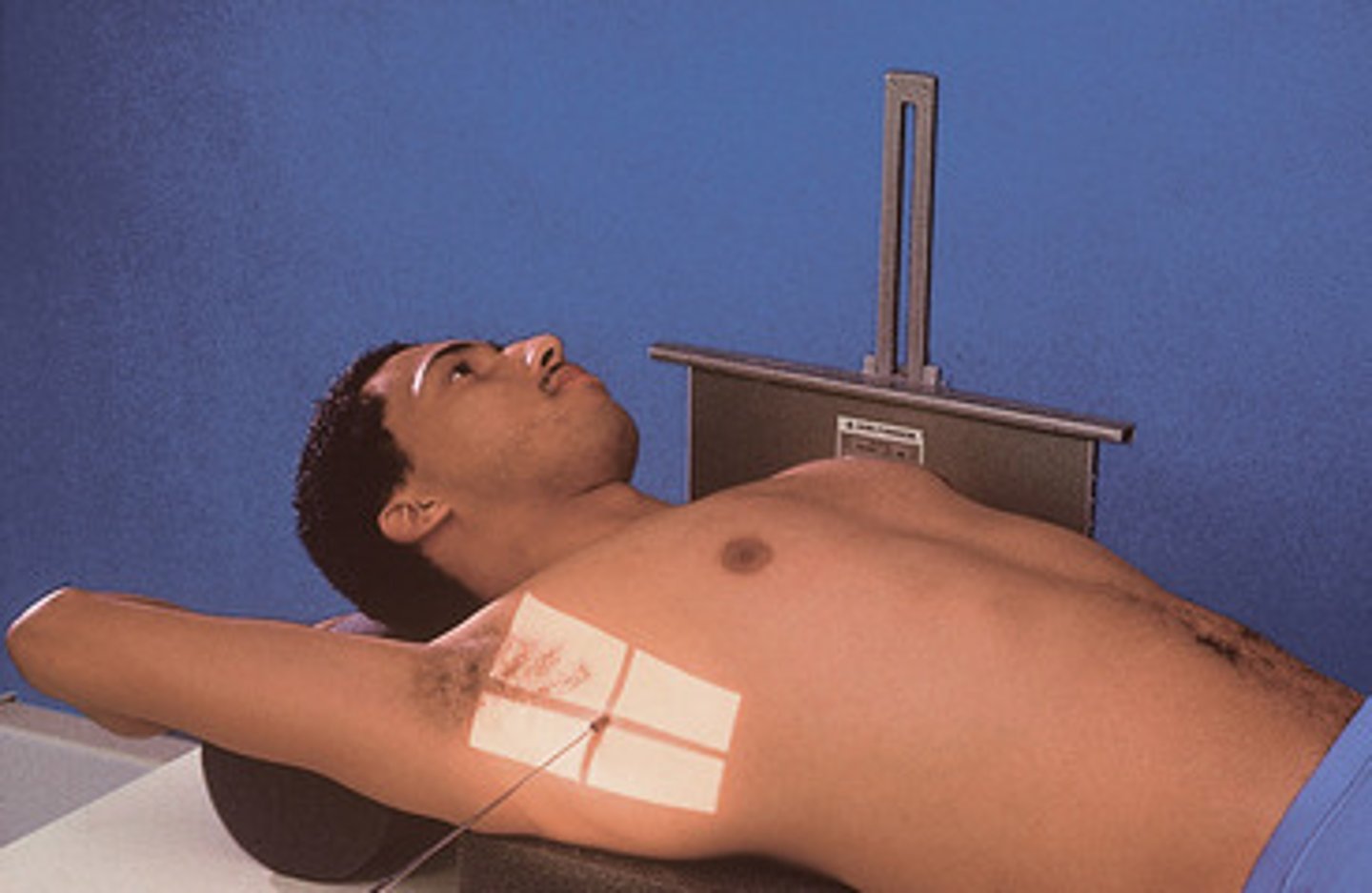
Fisk method (tangential bicipital groove)
used to visualize the intertubercular groove, greater and lesser tubercle in profile with bicipital groove
AP trauma shoulder neutral rotation
used for trauma patients, neutral rotation, proximal humerus with lateral clavicle and humeral head to glenoid fossa in profile

Lawrence Method (transthoracic lateral trauma shoulder)
can demonstrate possible Hill-Sachs defect with CR angled 25-30° medially, orthostatic breathing used
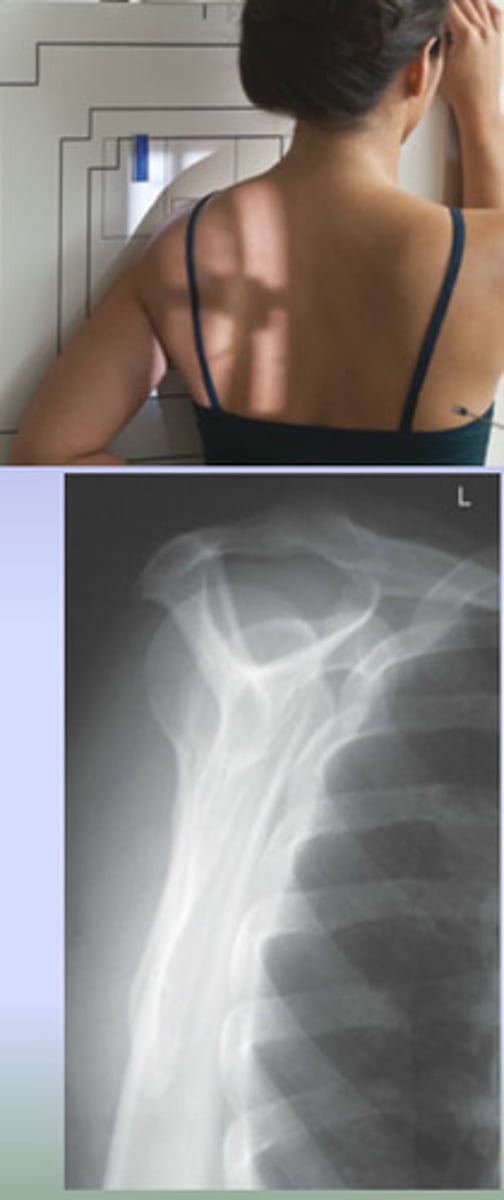
Scapular Y Shoulder trauma
used to rule out dislocations of humeral head (posterior and anterior), PA oblique projection, center mid scapula, lateral scapula
Neer Method (tangential shoulder supraspinatus outlet)
coracoacomial arch in profile, similar to lateral scapula, CR angled 10-15° caudal, suprasinatis outlet free of superimposition

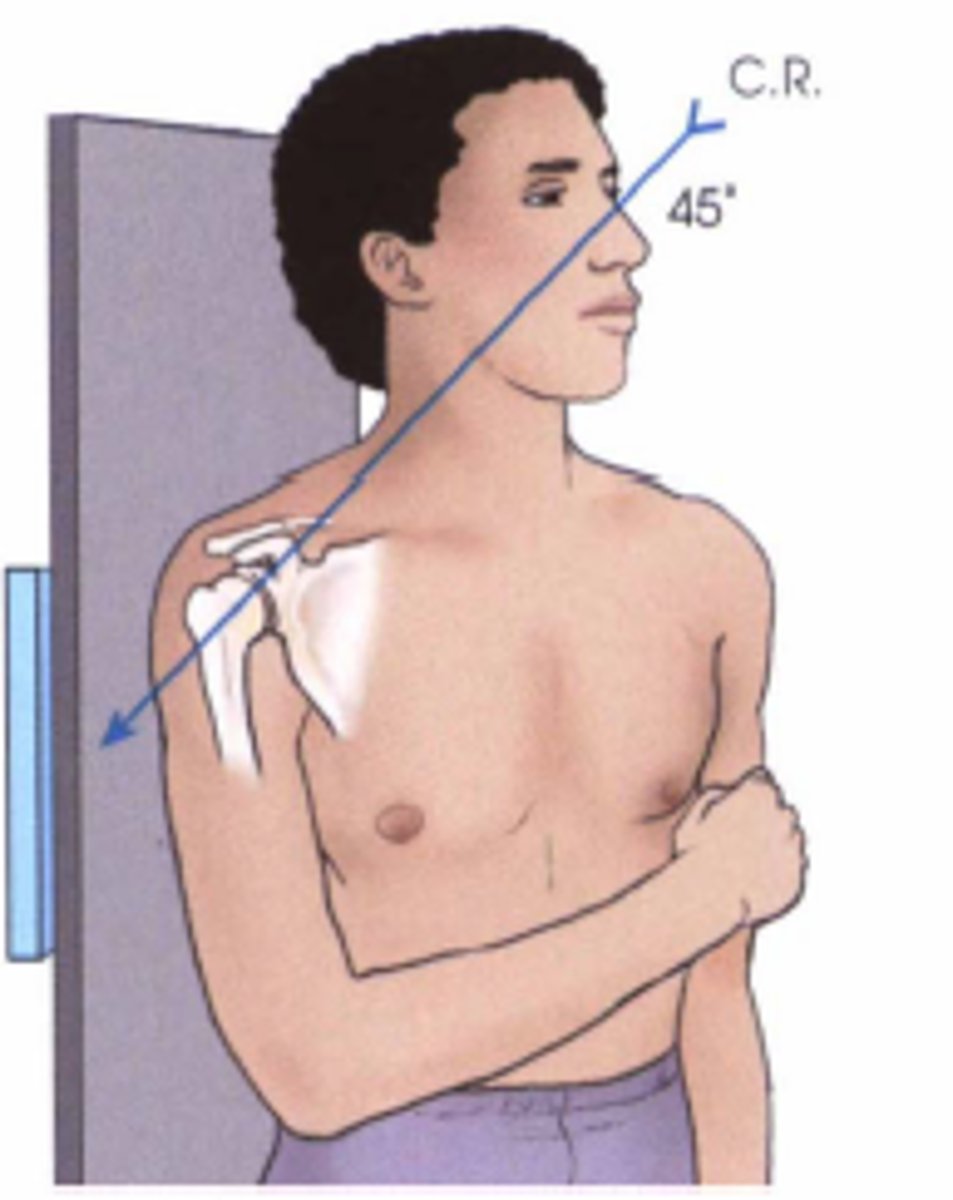
Garth Method (AP axial oblique shoulder trauma)
used to see glenoid fractures, Hill-Sachs, and humeral dislocations, posterior oblique, CR 45° caudal to scapulohumeral joint
AP clavicle
Included AC and SC joints, CR perpendicular to mid clavicle
AP Axial Clavicle
include both AC and SC joints, CR angled 15-30° cephalic

AC joints bilateral w/ & w/o
weights
both AC joints included on one view, use 72 SID, CR perpendicular to jugular notch
AP axial AC joints
CR angled 15° cephalic, alternate to AC joint bilateral, projects AC joints superior to acromion
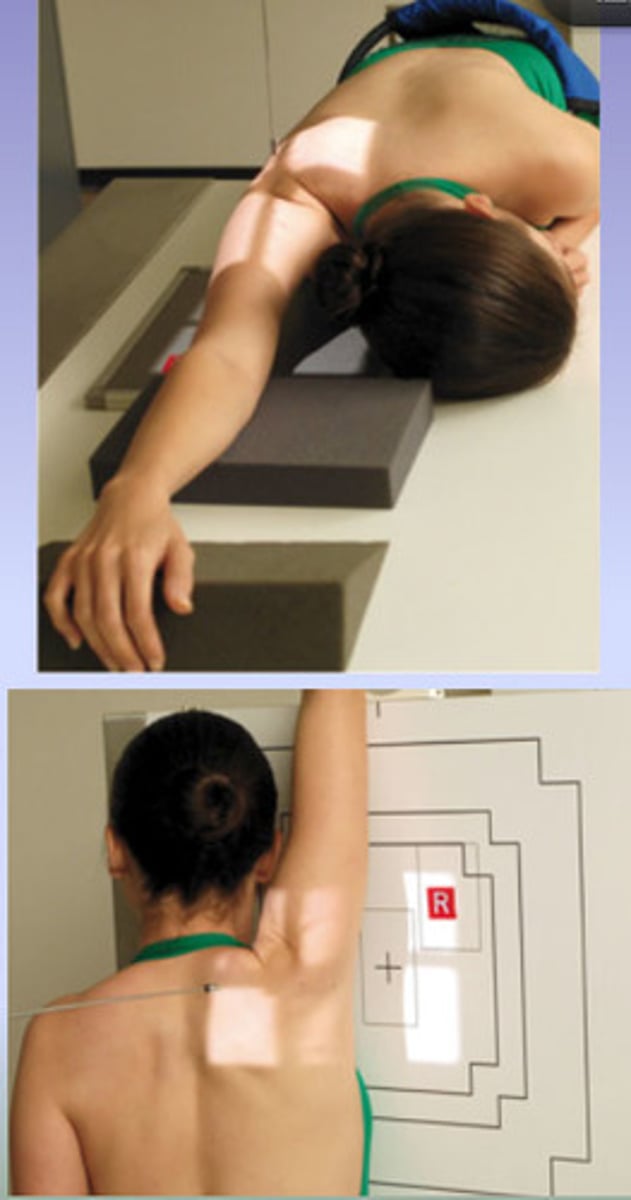
AP Scapula
CR perpendicular to mid scapula, orthostatic breathing used, rotation towards affected side for true AP

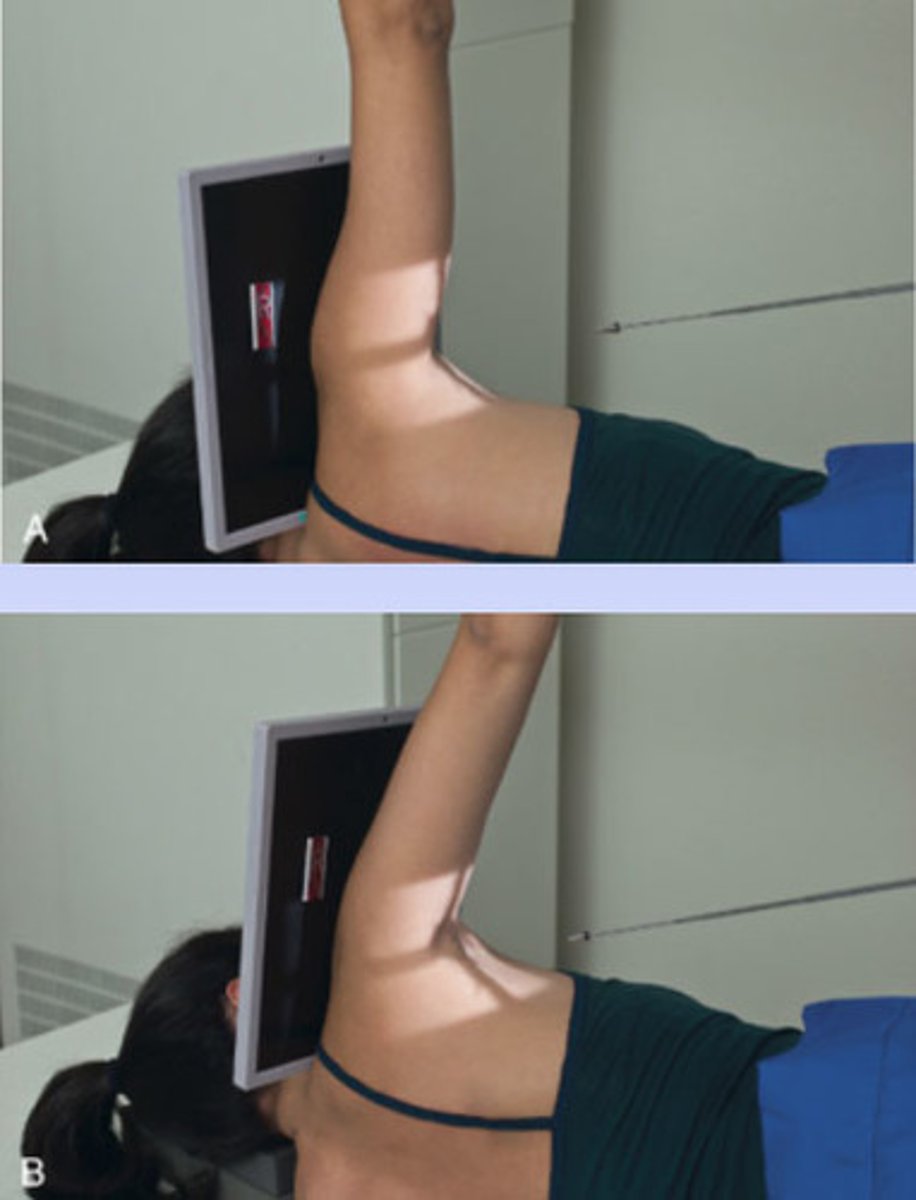
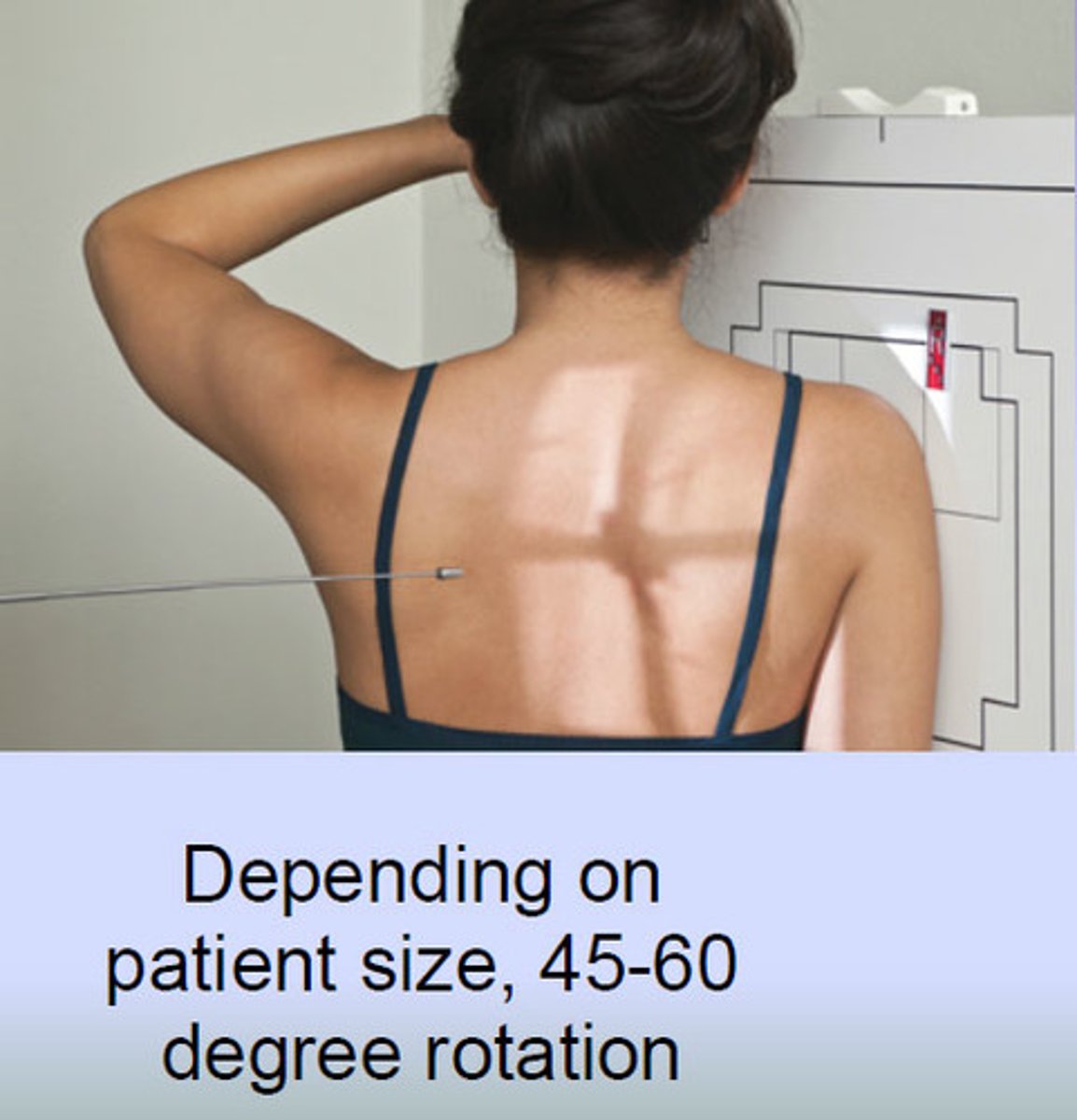
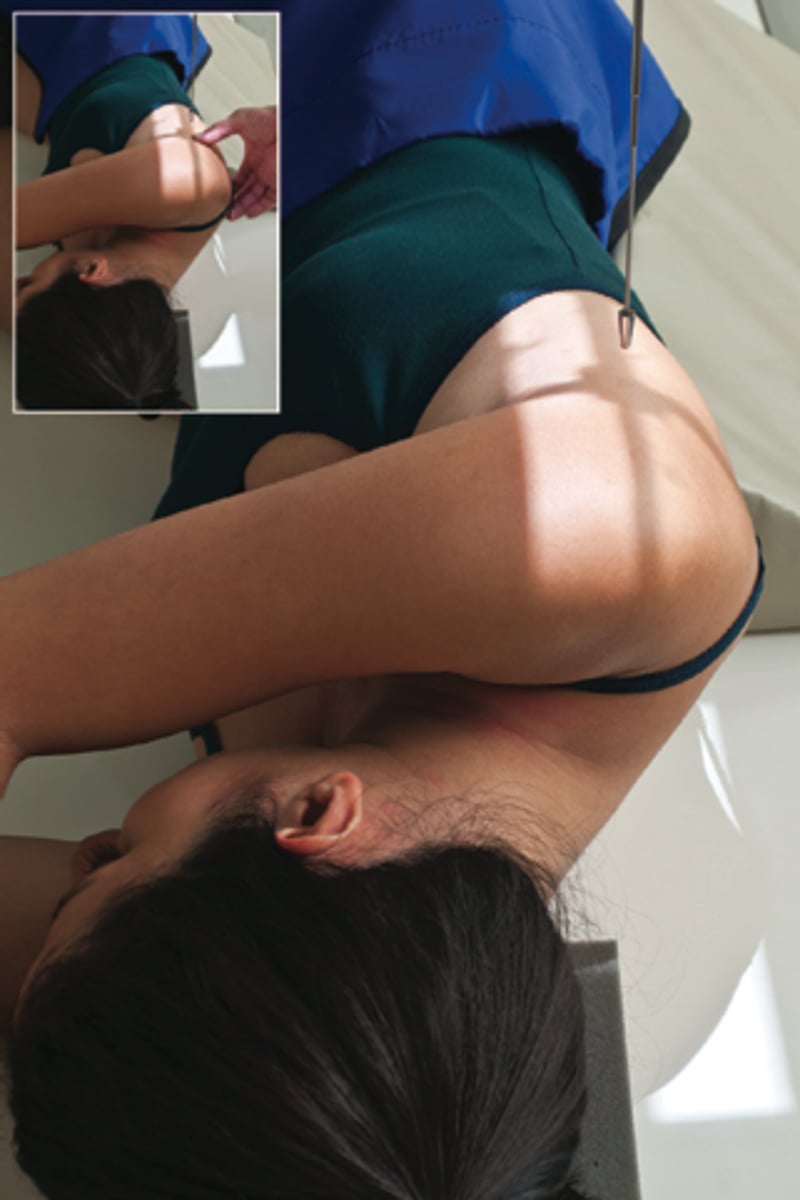
Scapular Y Scapula (lateral scapula for body)
patient in 45° anterior oblique, cross affected arm onto shoulder to remove humerus from scapular body
Lateral Scapula for Acromion or Coracoid
patient in 60° anterior oblique, CR perpendiclar mid body of scapula
Lateral Scapula Recumbent
Routine Scapular Y
• still lateral scapula (body perpendicular
to IR)
• 45 degree anterior oblique for body, affected arm opposite shoulder
• 60 degree anterior oblique for coracoid & acromion, affected arm behind body
• CR perpendicular to mid scapular body