Large intestine, constipation, diaeehoea and lactose intolerance
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
How is gastrointestinal motility created?
mostly smooth muscle (involentary) but skeletal muscle is important in the mouth, pharynx, upper oesophagus and external anal sphincter
What are the different types of GI smooth muscle and what do they do?
Logitudinal muscle contraction - lumen becomes shorter and fatter moving food
Circular muscle contraction - lumen becomes narrower and longer to break down food
Muscularis mucosae contraction - change in absorptive and secretory area of mucosa - secretory glands
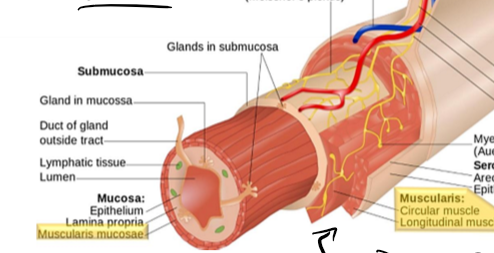
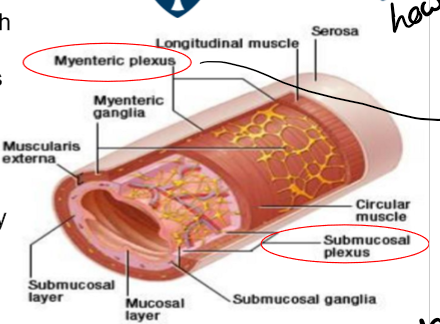
What is the enteric nervous system?
neurones whos cell bodies are located in the ganglia largely in the myenteric and submucous plexus, interganglionic fibre tracts connect the two plexuses, they form a complete reflex circit that can operate indepently of the rest of the nervous system but strongly modulated by hormones and extrinsic nerve imput, contains sensory, effector and interneurones
what happens in the parasympathetic autonomic innervation of the GI?
preganglionic fibres synapse with postganlonic neurones within the enteric nervous system
excitary influences: increased gastric, pancreatic and small intestinal secreation, blood flow and smooth muscle contration
inhibitory influences: relaxation of some sphincters, receptive relaxation of stomach
dominant system
what happens in the sympathetic autonomic innervation of the GI?
preganglionic fibres synapse in the prevertebral ganglia, postganglionic fibres innervate mainly enteric neurones, more contraction
inhibitory influences: decreased motility, secreation and blood flow
only in fight/flight, adrenaline in system
What can the smooth muscle in the GI tract do?
it can have spontaneous electrical and contractile activity, adjacent smooth muscle cells are coupled by gap junctions, electrical currents spread forming a functional syncytium - lots of cells are depolarised and contract at the same time, this spontaneous activity is modulated by intrinsic (enteric) and extrinsic (autonomic) nervous system and hormones
How does the spontaineous electrical activity in the smooth muscle in the GI system occur?
as slow waves - rhythmic pattern of membrane depolarisation and repolarisation, driven by interstitial cells of cajal which are pacemaker cells, contraction only occurs if the slow wave aplitude is sufficient to trigger action potentials, mainly mediated by voltage-activated Ca²⁺ channels, the force is related to the number of action potentials discharged
How are ICCs releated to the general smooth muscle structure of the GI tract?
they form gap junctions with each other and smooth muscle cells, they are located between the longitudinal and circular muscle layers in the submucosa
What is the BER?
basic electrical rhythum determind by slow waves, the frequency varies along the length of the GI tract
What determines whether a slow wave amplitude reaches the threshold?
neuronal stimuli, hormonal stimuli and mechanical stimuli
What is the BER frequency in the stomach?
3 slow waves per minute
What is the BER frequency of the small intestine?
1-12 slow waves per minute in the duodenum, around 8 waves per minute in the terminal ileum - this tends to drive luminal contents in the aboral direction
What is the BER frequency of the large intestines?
favours the retention of luminal contents faciallitating the absorbtion of water and electrolytes
If you are eating how does this cause slo waves?
if you are eating, sensory neutone is activated, motor nurone is activated, contract occurs
What is a slow wave?
a small change in charge, not a contraction, that are always present in the GI tract
What are the majot motility patterns in the GI tract?
peristalsis - series of wave-like muscle contractions that move food through the digestive tract-triggered by distention of the gut wall, it involved contraction of longitudinal muscle layers - contract behind the food and relaxed in front
tonic contraction - sustained contractions found in the spincters of the GI tract
segmentation - rhythmic contractions of the circular muscle layer that mix and divide luminal contents
How is water absorbed in the GI tract?
passive process driven by transportation of solutes from the lumen of the intestines to the blood stream, around 90% is absorbed, water ingested and secreated is normally in balance with water absorbed
What is diarrhoea defined as?
loss of fluid and solutes from the GI tract in excess of 500ml per day
What are the normal contents of faeces?
100mL water along with 50mL cellulose and bacteria
What is the general mechanism of water absorbtion?
driven by absorbtion of Na⁺, intestinal fluid movement is always coupled to solute movement, water may move via transcellular or paracellular routes, absorbtion of Na⁺ provides osmotic force for the absorbtion of water, sodium is absorbed from the lumen to the intersitial fluid,
What does electrogenic mean?
carrier proteins, protein channels, etc. that change the charge
How do Na⁺/amino acid co-transport and Na⁺/glucose co-transport in the GI tract work?
electrogenic transporters Na⁺/glucose co-transport and Na⁺/amino acid co-transport which are found in the small intestine in the post-prandial period, they absorb water and glucose/amino acids, makes blood more positive when sodium is absorbed
What does Na⁺/H⁺ exchange (protein?) do?
found in the duodenum and jejunum, electroneutral, as absorb sodium to the blood, secreate H⁺, activated by presence of bicarbonate, this makes the lumen more neutral as H⁺ has been secreated
What are the water absorbtion channels found in the large intersitine?
the parallel Na⁺/H⁺ and Cl⁻/HCO₃⁻ exchange - found in the ileum and colon, electoneutral, need cAMP/cGMP and Ca²⁺
epithelial Na⁺ channels (ENaC) - found in the distal colon, electrogenic, regulated by aldosterone, absorbs sodium
How is Cl⁻ absorbed in the GI tract?
intestine to blood to make the blood the same charge due to the sodium making the blood positive
Cl- is also reabsorbed by Na⁺/glucose co-transport, Na⁺/amino acid co-transport and epithelial Na⁺ channels
also absorbed by: parallel Na⁺/H⁺ and Cl⁻/HCO₃⁻ exchange found in the ileum and colon and Cl⁻/HCO₃⁻ exchange - electroneutral, activated by bicarbonate, found in the ileum and colon
in small intestine force provided by lumen negative potential due to electrogenic transport of Na⁺, in large intestine force provide by lumen negative potential due to electrogenic transport of Na⁺ through ENaC
What is the cellular mechanism of Cl⁻ secreation?
this shouldn’t happen, we want to absorb it but it does, occurs at basal rate, but normally overshadowed by higher rate of absorbtion, occurs from crypt cells (bottom of villi) rather than villus cells, on basolateral side there are channels: Na⁺/K⁺/2Cl⁻ co-transporter - when activated absorbs these into the epithelial cells of the intestine from the blood - low intracellular Na⁺ drives inward movement, Na⁺/K⁺ATPase, K⁺ channels - these channels allow the sodium and potassium to be absorbed back into the blood, intracellular Cl⁻ increases provides electrochemical gradient for Cl⁻ to exit the cell on the apical membrane via the CFTR, these are normally closed or not present, lumen negative potential develops voltage-dependent secreation of Na⁺ through paracellular pathway
Why don’t you want Cl⁻ moving back into the intestine?
intestine becomes negative so sodium follows and then water follows by osmosis, if this happens at higher rate causes diarrhoea
What does CFTR stand for?
cystic fibrosis transmembrane regulator
What is CFTR activated by?
activation of CFTR occurs indirectly as a result of the generation of second messangers: cAMP, cGMP and Ca²⁺
bacterial enterotoxins - increases levels of cAMP or cGMP, hormones and neurotransmitters- increased calcium, immune cells products - prosterglandins activate cAMP, some laxatives - increased calcium levels
Cl⁻ conductance mediated by CFTR results from opening of channels at the apical membrane or insertion of additional channels from intracellular vesicles into the membrane, Cl⁻ secreation in lumen causes Na⁺ paracellular secreation and water secreation, overall effect is secretory diarroea
What are the causes of diarrhoea?
excessive secreation, impaired absorbtion of NaCl, non-absorbable or porly absorbable solutes, hypermotility
How does hypermotility cause diarrhoea?
excessive peristalsis of the GI with reduced absorbtion of solutes and water - not enough chance for water absorbtion
How does non-absorbable or poorly absorbable solutes cause diarrhoea?
when in intestinal lumen, causes osmotic diarrhoea - if not absorbed attracts water back into the lumen especially if lots of OH groups, lactose intolerance is this
How does impaied absorbtion of NaCl cause diarrhoea?
water follows chlorine and sodium, caused by congenital defects - some channels don’t work, infection - enterotoxins from some bacteria damage channels - they go back tho, inflammation and destruction of the intestinal absorbtive epithelium - exudative diarrhoea - causes damage to cells but will do back eventually
How does excessive secreation cause diarrhoea?
secreatory diarrhoea, most commonly caused by E.Coli, example cholera: increase cAMP amount, cholera toxin enters enterocyte enzymaticaly inhibits GTPase activity of the Gsα subunit, increased activity of adenylate cyclase, increased concentration of cAMP, cAMP stimulates CFTR, hypersecretion of Cl⁻, with Na⁺ and water following
What are the concequences of diarroea?
can result in dehydration, metabolic acidosis due to HCO₃⁻ loss, hypokalaemia (K⁺ loss), can be fatal if severe
What three treatments can you give for severe acute diarrhoea (groups not specific)?
maintance of fluid and electrolyte balance - 1st priority, use of anti-infective agents - if appropriate, use of anti-motility agents (if hypermotility)
How does rehydration therapy work?
uses Na⁺/glucose channel - two Na⁺ bind that then increases affinity for glucose, glucose binds, Na⁺ and glucose translocate from extracellular to intracellular, 2 Na⁺ dissociate and the affinity for glucose falls, glucose dissociates, water follows the sodium, with just water it wouldn’t be absorbed, so glucose, sodium and potassium are given
What do oral rehydration salts contain?
glucose, sodium chloride, trisodium citrate, potassium chloride, dissolve in 1L of drinking water
How can you make a basic rehydration solution at home?
glucose 6 teaspoons, salt 0.5 teaspoons, dissolved in 1 L drinking water
How do opiates work as anti-motility agents?
actions on the alimentary tract include:
inhibition of enteric neurones - hyperpolarisation via activation of u-opioid receptors, promotes Cl⁻ to go into cells making them negative, decrease movement allowing absorbtion
decreased peristalsis, increased segmentation
increased fluid absorbtion,
constriction of pyloric and anal sphincters
What opiates are used in diarrhoea?
codeine - has a CNS effect
diphenoxylate - low CNS penetration, blocks the release of acetylcholine in the synaptic cleft
loperamide - first choice for E.Coli, relatively selective for the GI tract, reduces peristalsis, decrease the passage of faeces, no CNS effect
atropine - blocks muscarinic receptor, reduces motility, however effects heart and eyes as side effects
What is lactose intolerance?
disorder caused by impaired carbohydrate digestion, common, comes from the inability to adequately digest lactose caused by lactase insuffciency, varible degree of lactase persistance, partially due to polymorphisms in the MCM6 gene that regulates expression of the lactase gene
What can cause lactose intolerance?
primary lactase deficiency - due to lack of the lactase persistance (LP) allele - most common cause worldwide
secondary lactase deficiency - caused by damage to/infection of the proximal small intestine
congenital lactase deficiency - rare autosomal recessive disease - no ability to digest lactose from birth
What are the consequences of lactase insufficiency?
hypolactasia causes no problem unless lactose containing food is consumed and the activity of the remaining enzymes is overwhelmed, if lactose is delivered to the colon from the ileum, conlonic microflora produce: short-chain fatty acids (which can be absorbed), hydrogen (H₂ which can be detected in the breath), carbon dioxide, and methane
symptoms - bloating, abdominal pain, and diarrhoea
How is lactose intolerance diagnosed?
based on deit observation
association of symptoms with lactose consumption, hydrogen breath test, lactose/milk tolerance test - give lactose - take blood - test level of glucose, it should be increased if normal, if don’t increase suggests lactose intolerance
What is constipation?
difficult/infrequent defecation
What are the causes of constipation?
neurogenic disorders of the large intestine leading to reduced persistalsis, abdominal muscle weakness - doesn’t contract enough, diet poor of fibres - fibre not absorbed, cellulose and fibre contain water in their structure which keeps faeces hydrated, sedentary lifestyle - doesn’t contract enough, constant supression of the urge to empty - muscle gets tired, antidepressant drugs - anticholinergics, opiates, aging - effects muscle contraction
What are the lifestyle changes you should suggest around constipation?
more water and less alcohol should be consumed, some wheat bran can be added to the diet, increase activity, improve toilet routine - keep to regular time and give yourself time, don’t delay, feet can be rested on a low stool - contract muscle that makes it easier to empty bowel
What are the pharmaceutical treatment options for constipation?
Bulk laxtives e.g. methylcellulose - polysaccharide polymers not digestable
osmotic laxatives e.g. magnesium hydroxide, lactulose - poorly absorbed solutes
faecal softeners e.g. arachis oil, docusate sodium- enema
stimulant laxativees e.g. senna, dantron - drugs that directly increase peristalsis - this damages epithelial cells
antiemetics - increase GI motility without purgation e.g. domperidone, metoclopramide - increase gastrointestinal motility and gastric emptying