Thyroid and Anti-Thyroid Drugs
1/167
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
168 Terms
-calcitonin
-thyroxine (T4)
-triiodothyronine (T3)
What are the 3 main thyroid hormones?
-levothyroxine
-liothyronine
What are the 2 main thyromimetic drugs?
-propylthiouracil
-methimazole
-radioactive iodide
-potassium iodide
-propranolol/atenolol
-diltiazem
What are the 6 main anti-thyroid drugs?
teprotumumab
What is the main drug used for thyroid eye disease?
tyrosine
What amino acid is involved in forming thyroid hormone (TH)?
2 iodinated tyrosine molecules come together to form the backbone of thyronine
How is tyrosine involved in forming TH?
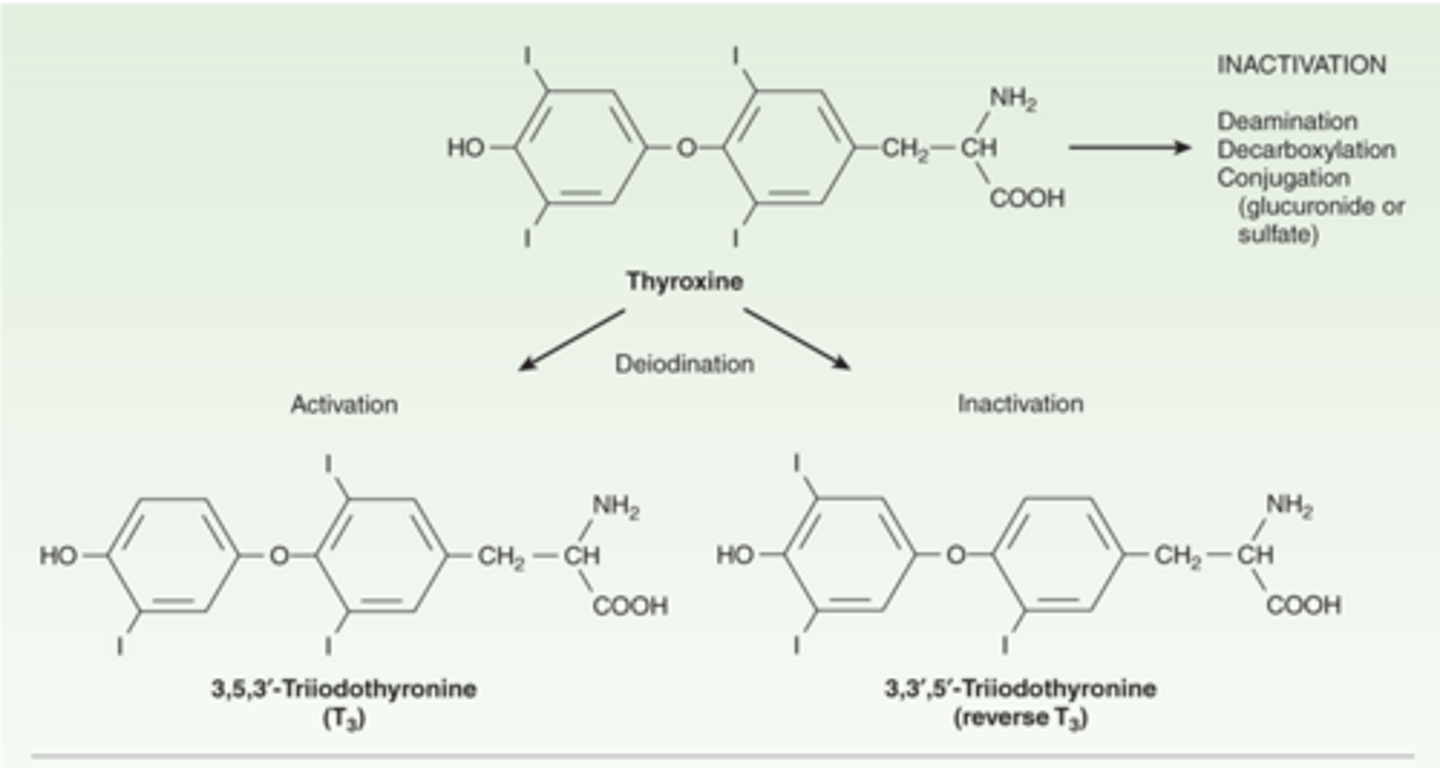
T4 has 4 iodines, while T3 has 3 iodines
How do the structures of thyroxine (T4) and triiodothyronine (T3) compare?
T3 of reverse T3 -> the structural difference is where the iodine is removed from, and the functional difference is reverse T3 has little activity
What can be formed by the deiodination of thyroxine (T4), and explain?
chemistry/metabolism of thyroid hormones:
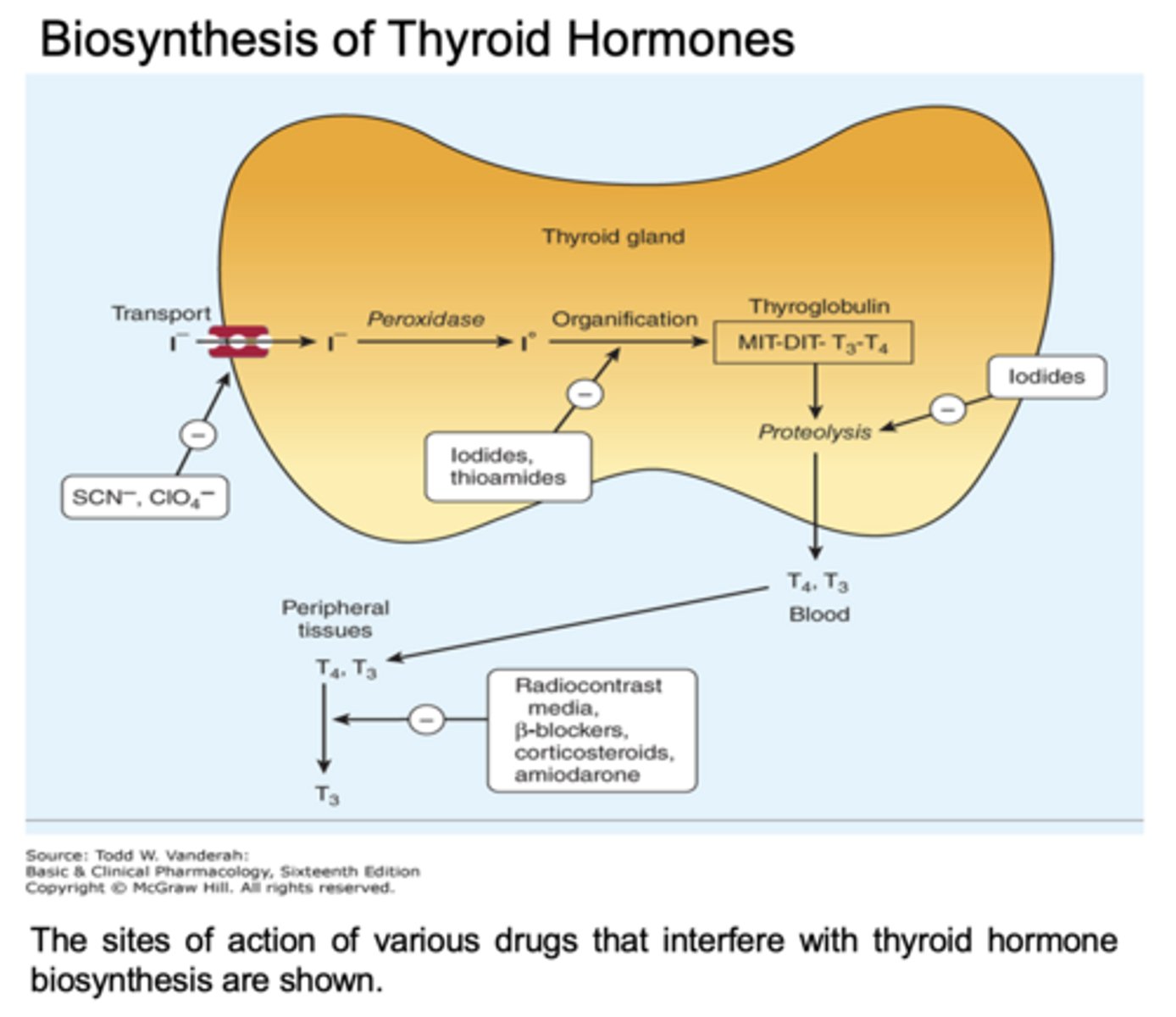
Thyroid hormone synthesis is a multiple step process.
Thyroid hormone synthesis is a ______ step process.
iodide uptake (150-200 micrograms)
What is the 1st step in TH synthesis?
oxidation of iodide and iodination of thyroglobulin
What happens after iodide uptake in TH synthesis?
coupling of iodotyrosine to form iodothyronines
What happens after the oxidation of iodide and iodination of thyroglobulin in TH synthesis?
transport of thyroglobulin into lumen of the cell
What happens after the coupling of iodotyrosine to form iodothyronines in TH synthesis?
proteolysis of thyroglobulin and release of TH into bloodstream
What happens after the transport of thyroglobulin into the lumen of the cell in TH synthesis?
iodide from the diet comes in, and 50% is taken up by the thyroid gland
What does TH biosynthesis begin with?
peroxidase -> forms an iodide intermediate
What enzyme acts on the iodide brought into the thyroid cell, and explain?
via organification, it becomes covalently attached to tyrosine residues to form DIT (2 iodides) or MIT (1 iodide)
What is the function of the iodide intermediate, formed by peroxidase?
2 DIT = T4
1 DIT/1 MIT = T3
How do the MIT and DIT, formed via organification, give rise to TH?
more T4 is produced than T3
How do the numbers of T3 and T4 produced compare?
in the thyroglobulin protein
Where are T3/T4 formed and stored within the thyroid cell?
150-200 micrograms
What is the recommended baseline dose of iodine for adults to properly synthesize thyroid hormones?
80-90% absorbed
What is the absorption of dietary iodine like?
75-100 micrograms/day (50%)
What amount of dietary iodine is taken up by the thyroid?
5:1
What is the ratio of T4:T3 in thyroglobulin?
60-80% (most) in the urine, 20-40% (some) in the feces via bile
What is the excretion of iodine (T3/T4) like?
T4 -> 10 L
T3 -> 40 L (wider volume of distribution)
How does the volume of distribution (Vd) of thyroxine (T4) and triiodothyronine (T3) compare?
T4 -> 7 days (longer)
T3 -> 1 day
How does the half-life of thyroxine (T4) and triiodothyronine (T3) compare?
T4 -> 99.96% bound
T3 -> 99.6% bound
->VERY little free TH circulating
How does the percent of bound thyroxine (T4) and triiodothyronine (T3) compare?
T4 -> 80% oral absorption
T3 -> 95% oral absorption
->both pretty good oral bioavailability
How does the oral absorption of thyroxine (T4) and triiodothyronine (T3) compare?
T4 -> 1
T3 -> 4 (better binding to produce effects
How does the potency of thyroxine (T4) and triiodothyronine (T3) compare?
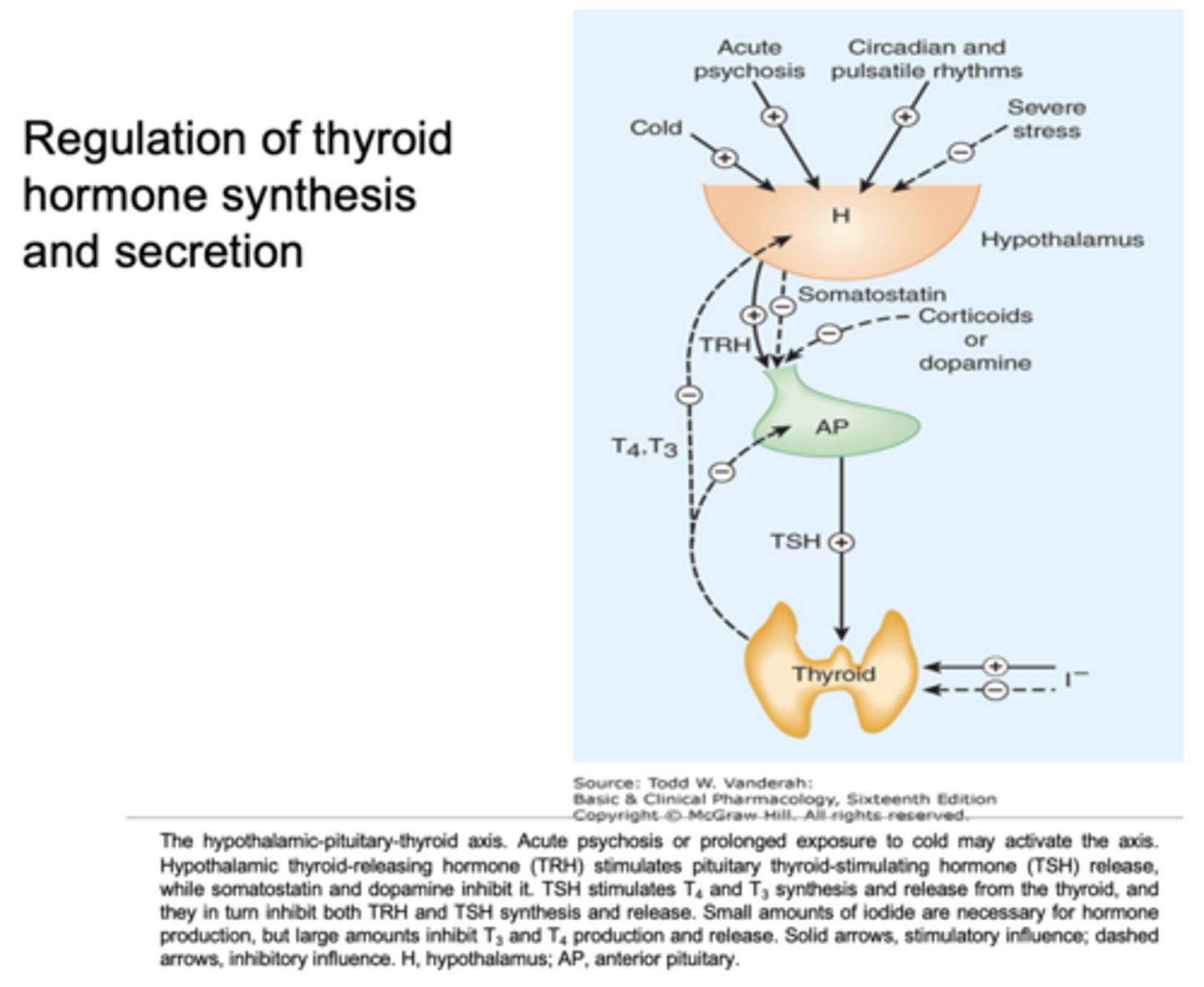
-hypothalamus/TRH
-anterior pituitary/TSH
What 2 things are mainly involved in the regulation of TH synthesis and secretion?
increases the size and number of cells in the thyroid and the production of T3/T4
What effects does TSH have on the thyroid?
they bind to receptors to produce effects
How do T3/T4 function?
they feedback negatively on the hypothalamus and pituitary
How are T3/T4 involved in feedback?
-severe stress
-somatostatin
-corticoids or dopamine
What are 3 other things that negatively regulate TH secretion, besides T3 and T4 themselves?
-cold
-acute psychosis
-circadian and pulsatile rhythms
What are 3 things that positively regulate TH secretion, besides TRH and TSH?
increased iodide can increase levels of T3/T4 BUT too much iodide can shut off production
How can iodide intake affect levels of T3/T4 produced?
hypothalamus; stimulates release of TSH
Where is thyrotropin-releasing hormone (TRH) secreted from, and what is its function?
anterior pituitary; stimulates release of TH
Where is thyroid-stimulating hormone (TSH) secreted from, and what is its function?
thyrotropin
What is thyroid-stimulating hormone (TSH) also known as?
glycoprotein pituitary hormone
What type of hormone is TSH/thyrotropin?
increases cAMP to increase the synthesis/secretion of T3 and T4
How does TSH function?
recombinant human TSH; used in diagnosis by allowing measurement of T3, T4, and TSH levels
What is rhTSH, and what is its function?
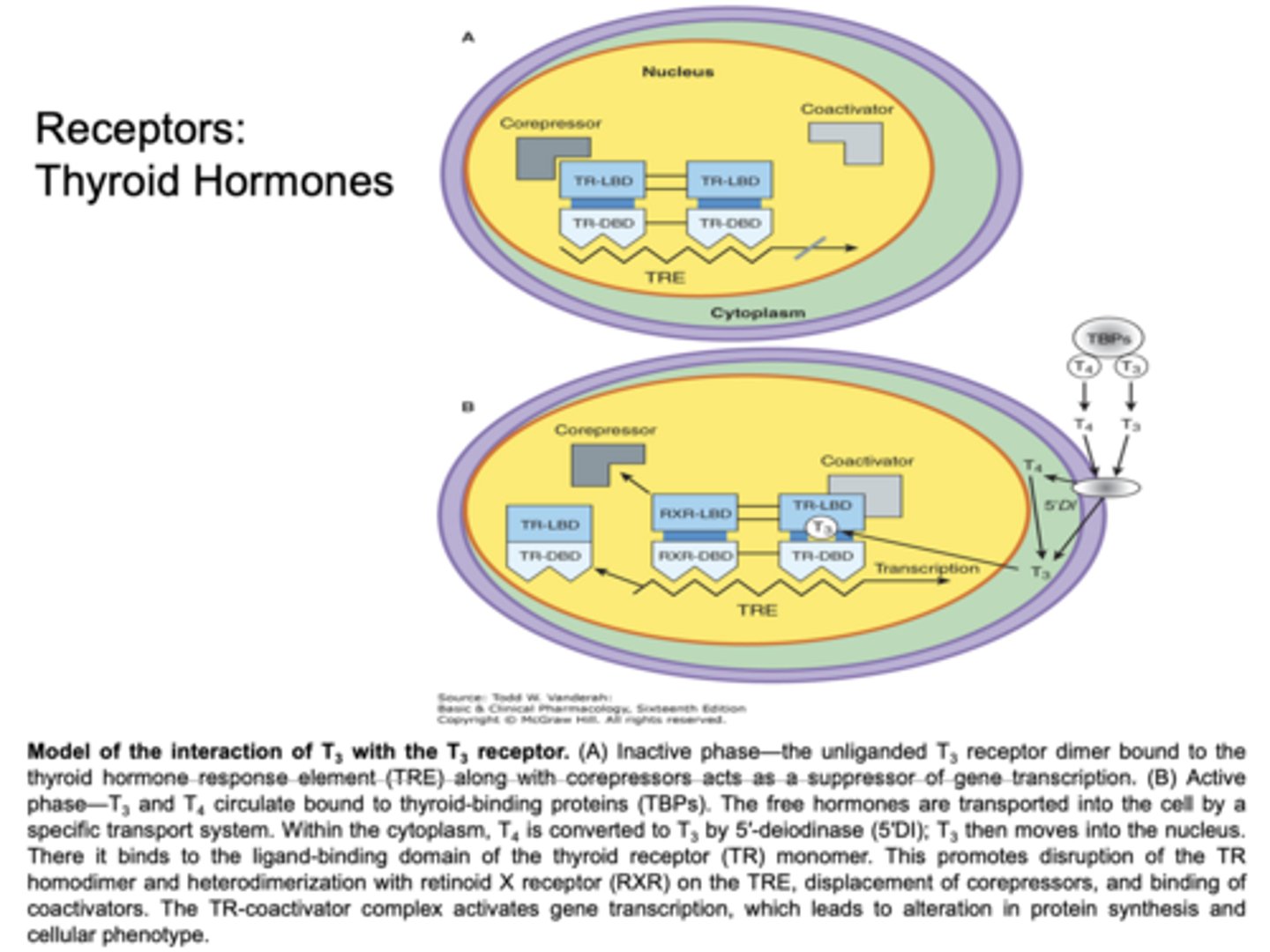
similar to steroid hormone receptors; both are very lipophilic molecules
What are TH receptors similar to, and explain?
lack of T3 (or T4) keeps the receptor bound to corepressors that suppress gee transcription and translation
What is the TH receptor like in the inactive phase?
when T3 (or T4) binds, the receptor gets rid of the corepressor, and transcription and translation can occur, thus increasing protein synthesis
What is the TH receptor like in the active phase?
TH receptors:
-normal growth and development (CNS)
-increase in BMR, cellular metabolism/protein synthesis
-thermogenic/calorigenic effect -> increases NaK ATPase, cell metabolism, heat production
-increase in plasma glucose (production and uptake)
-reduction in plasma cholesterol (dextrothyroxine decreases cholesterol)
-increase in cardiovascular activity (HR, force of contraction)
-maturation of the CNS
What are the 7 main effects/functions of thyroid hormones?
CHF -> because the heart pumps too hard
What cardiovascular effect can hypothyroidism lead to, and explain?
L-form (levothyroxine) has a greater effect than D-form (dextrothyroxine)
How do the L-form and D-form of thyroid hormone compare?
-cardiovascular
-CNS
-metabolic
What are the 3 main functions of TH?
-increase cardiac output
-increase HR
-increase stroke volume
-decrease vascular resistance
What are the 4 main functions of TH in the cardiovascular system?
-brain development
-neuronal development
What are the 2 main functions of TH in the CNS?
-increase gluconeogenesis
-increase glycolysis
-increase cholesterol breakdown
-increase thermogenesis
What are the 4 main functions of TH in the CNS?
-tiredness
-sensitivity to cold
-constipation
-dry skin
-weight gain (slowed BMR)
-puffy face
-hoarse voice
-coarse hair/skin
What are the 8 main symptoms associated with hypothyroidism?
primary is deficiency in the thyroid itself (aka not producing enough T3/T4), while secondary is a deficiency not in the thyroid (aka the pituitary not secreting enough TSH or hypothalamus not secreting enough TRH)
How do primary and secondary hypothyroidism compare?
-levothyroxine
-liothyronine
(-thyroid USP)
What are 2 main examples of thyromimetic drugs?
pure synthetic thyroxine, T4
What is levothyroxine?
pure synthetic triiodothyronine, T3
What is liothyronine?
the OG thyromimetic drug used -> comprised of animal thyroid, thus risk of allergic reaction
What is thyroid USP, and explain?
by observing decreased TSH levels (due to negative feedback of TH) and observing positive changed in how the patient is feeling
How can clinicians assess whether a thryomimetic drug is working in a patient?
80% bioavailable
What is the oral bioavailability like for levothyroxine?
6-7 days
What is the half-life of levothyroxine?
99% bound to TBG
What is the percent of levothyroxine bound to TBG?
symptoms of hyperthyroidism
Generally, what are the adverse effects of levothyroxine like?
-insomnia
-anxiety
-fever
-weight loss
-tachycardia
-angina
-rash
-urticaria
-intolerance to heat
-elevated plasma glucose
What are the 10 main adverse effects of levothyroxine?
-increased TBG
-decreased TBG
-displacement from plasma proteins
-increased metabolism
-decreased metabolism
-decreased absorption
What are the 6 main types of drug-drug interactions that levothyroxine is affected by?
-estrogen
-heroin
What 2 drugs cause increased TBG, thus causing drug-drug interaction with levothyroxine?
androgens
What drugs cause decreased TBG, thus causing drug-drug interaction with levothyroxine?
salicylates
What drugs cause displacement from plasma proteins, thus causing drug-drug interaction with levothyroxine?
-rifampin
-nicardipine
What 2 drugs cause increased metabolism, thus causing drug-drug interaction with levothyroxine?
*PTU
*beta-blockers
What 2 drugs cause decreased metabolism, thus causing drug-drug interaction with levothyroxine?
-antacids
-PPIs
-cholestyramine
What 3 drugs cause decreased absorption, thus causing drug-drug interaction with levothyroxine?
because levothyroxine is taken orally and requires some stomach acid to be absorbed
Why do antacids, PPIs, and cholestyramine cause decreased absorption of levothyroxine?
-painless lump in neck
-trouble swallowing; hoarseness
-difficulty breathing
-swollen lymph nodes in the neck
What are the 4 main symptoms associated with thyroid cancer?
surgical removal of the thyroid or radioactive iodine (I-131, gives off both beta particles and gamma radiation), followed by levothyroxine for TH replacement therapy
What is the treatment for thyroid cancer?
-nervousness, anxiety, irritability
-mood swings
-difficulty sleeping, persistent tiredness
-sensitivity to heat
-swelling in neck/goiter
-tachycardia/palpitations
-twitching
What are the 7 main symptoms associated with hyperthyroidism?
no, it is also seen in hypothyrodism -> in hypothyroidism, thyroid gland is not producing enough T3/T4, thus TSH keeps stimulating the thyroid to grow, while in hyperthyroidism (ex: Graves' disease) there is continual secretion of TSH-like globulin, which stimulates the thyroid to grow
Is swelling in neck/goiter only seen in hyperthyroidism, and explain?
-potassium iodide (OG drug, not used much anymore)
-radioactive iodide (I-131)
-thioamides
What are the 3 main types of antithyroid drugs for treating hyperthyroidism?
-propylthiouracil
-methimazole
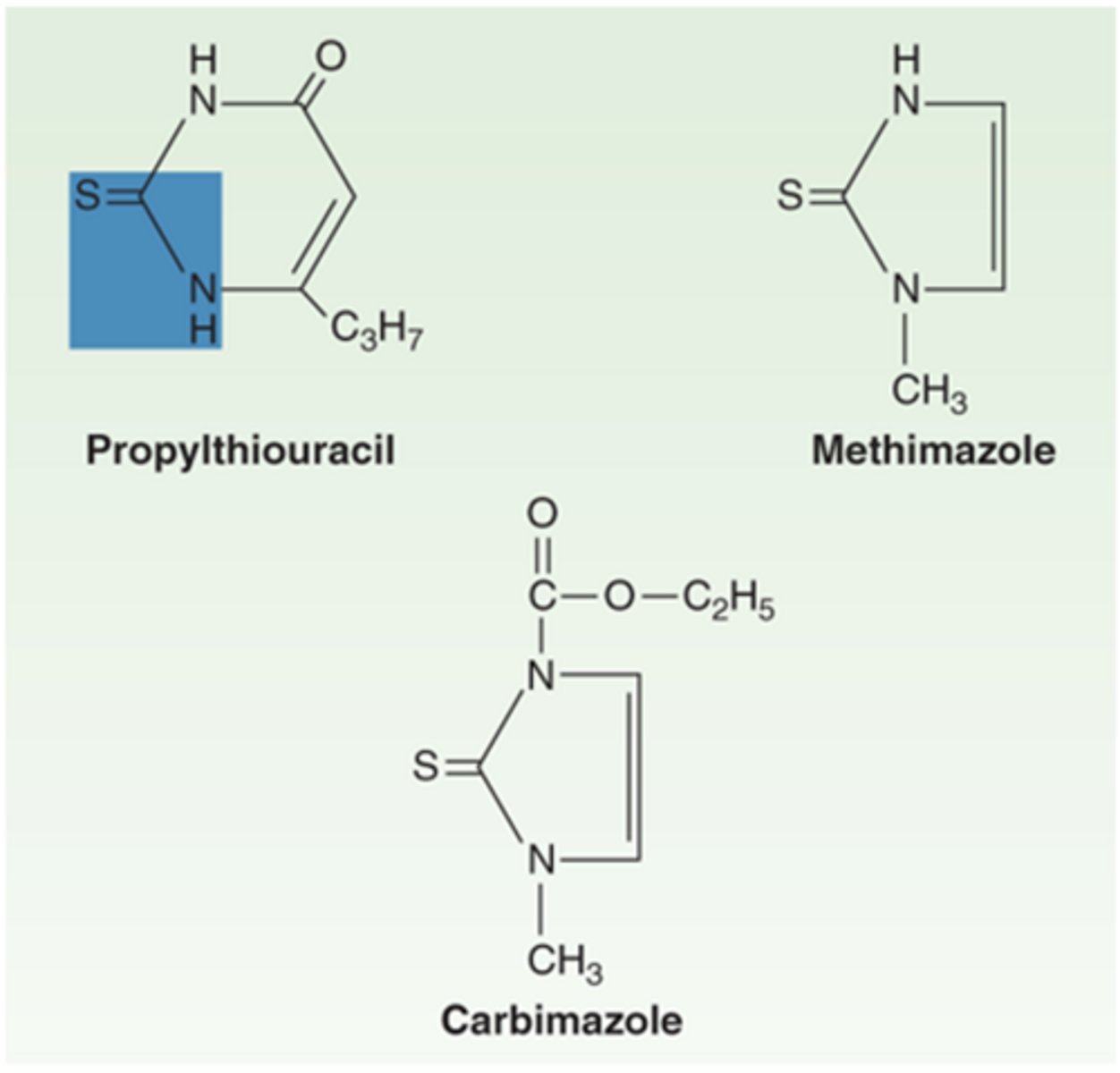
What are the 2 thioamides used to treat hyperthyroidism?
-allergic reactions (shellfish allergy is often Iodide allergy!)
-head cold-like symptoms
-acne
-swollen, tender salivary glands
What are the 4 main adverse effects associated with potassium iodide (antithyroid drug)?
not useful for long-term therapy -> if given for too long, get a sudden outpouring of TH, called "thyroid storm"
What type of therapy is potassium iodide not useful for, and explain?
used before surgical removal of thyroid because it decreases blood flow, allowing for easier removal
What is potassium iodide often used for in short-term therapy?
takes 6-12 weeks for clinical effect, will not see an immediate effect
What is the effect of radioactive iodide, I-131 (anti-thyroid drug) like?
-should not be given to pregnant patient or patient planning to become pregnant within 9 mo/1 yr
-can destroy too many thyroid cells, leading to hypothyroidism
What are 2 considerations for the use of radioactive iodide, I-131?
-propylthiouracil
-methimazole
-carbimazole
What are the 3 main examples of thioamides?
treatment of mild to moderate hyperthyroidism
What are the thioamides, propylthiouracil, methimazole, and carbomazole indicated for?
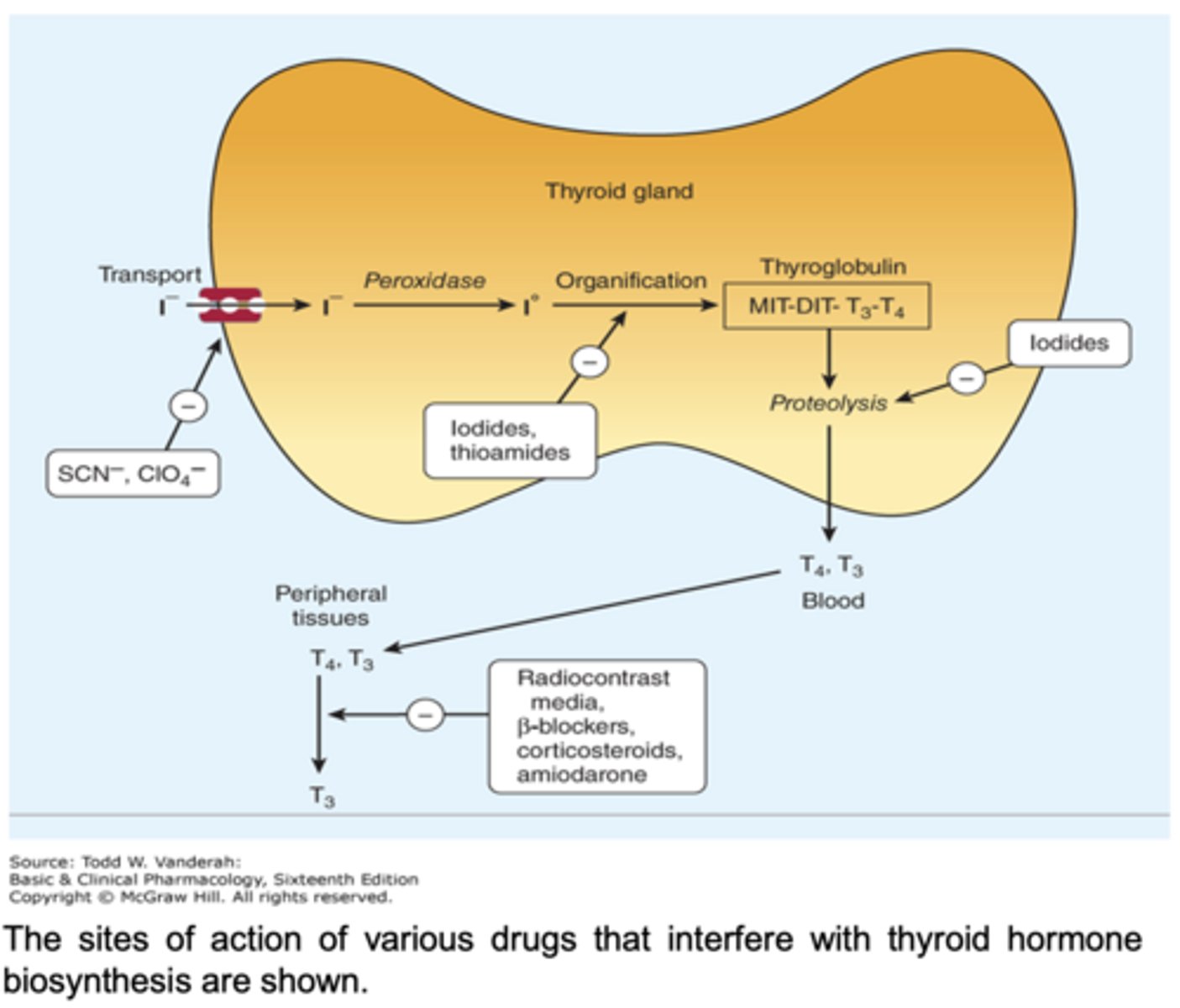
they reduce synthesis of TH
Generally, what is the mechanism of anti-thyroid drugs?
they do not work immediately -> effects are only observed after current levels of TH are metabolized
What is significant about anti-thyroid drug function, considering they reduce TH synthesis, and explain?
they reduce the oxidation steps in TH synthesis
How do anti-thyroid drugs, like thioamides, function to decrease TH synthesis?
it reduces the deiodination of T4 to T3
How else does the thioamide, propylthiouracil, function to decrease TH synthesis?
mechanism of anti-thyroid drugs:
delayed onset of 3-4 weeks
What is the onset of action for the thioamides, propylthiouracil, and methimazole?
-maculopapular pruritic rash (most common)
-GI upset
-hypothyroidism
-agranulocytosis (0.3-0.6%) (important effects on blood, would see effects within 1st 3 months)
-liver damage
-cross placenta, get into breast milk (shouldn't be used during breastfeeding)
What are the 6 main adverse effects associated with the thioamides, propylthiouracil, and methimazole?
occurs more with use of PTU than MTX, which is why MTZ is USUALLY preferred to PTU
How does liver damage differ with the use of propylthiouracil versus methimazole?
during the 1st trimester of pregnancy -> less PTU crosses the placenta than MTZ and PTU can be supplied with levothyroxine to ensure fetus has enough TH to develop
In what case is PTU preferred to MTZ, and explain?
-beta blockers -> propanolol, atenolol
-calcium channel blockers -> diltiazem
What are 2 drug types that act as adjuncts to anti-thyroid drugs in treating hyperthyroidism, and explain?