Pharm - Venous Thromboembolism
1/104
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
105 Terms
What does VTE stand for?
Venous thromboembolism
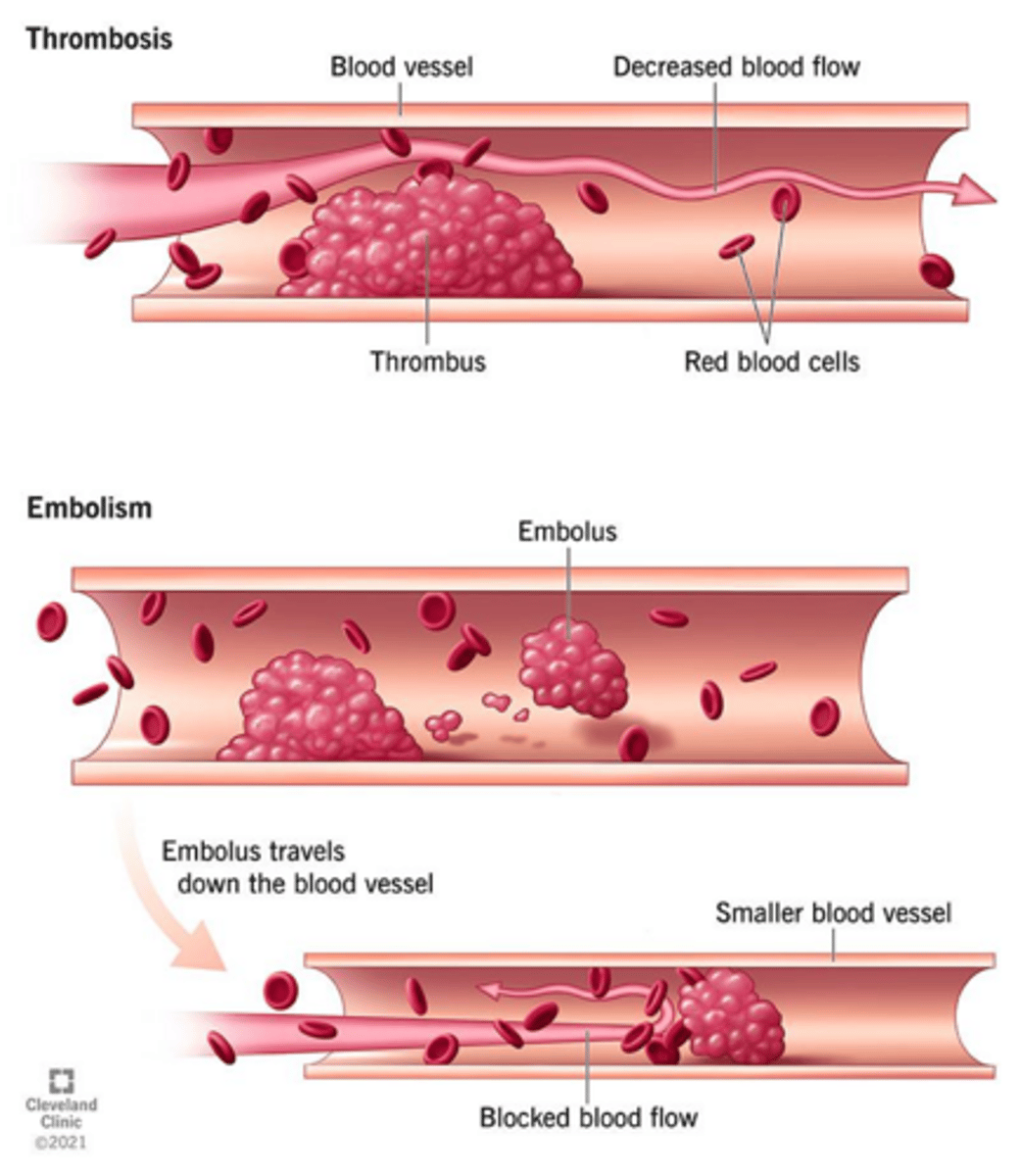
What are the two main components of VTE?
Deep vein thrombosis (DVT) and pulmonary embolism (PE)
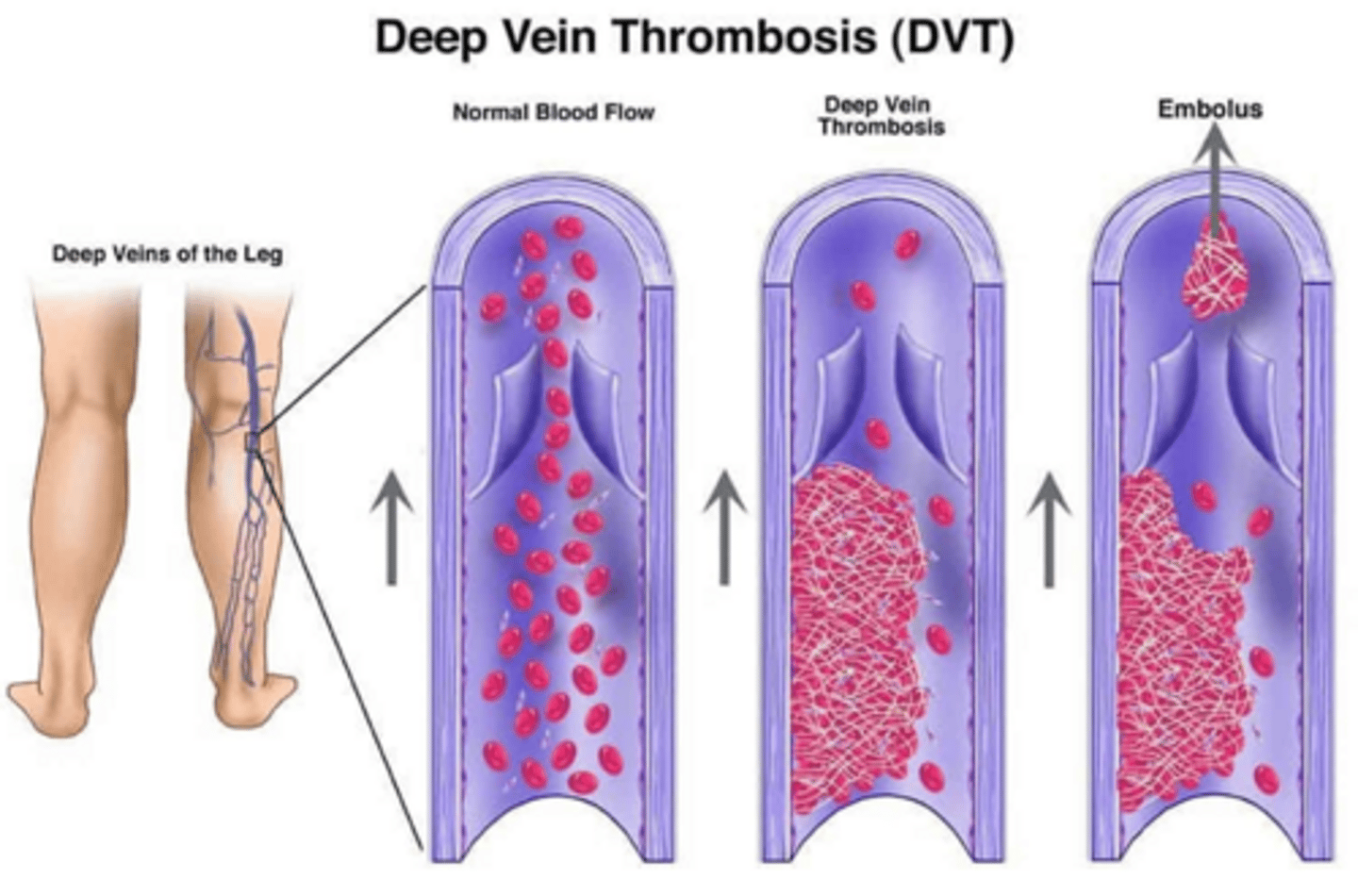
What is the primary symptom of DVT?
Unilateral leg pain, warmth, swelling, redness
What diagnostic test is used for DVT?
Compression ultrasound (CUS)
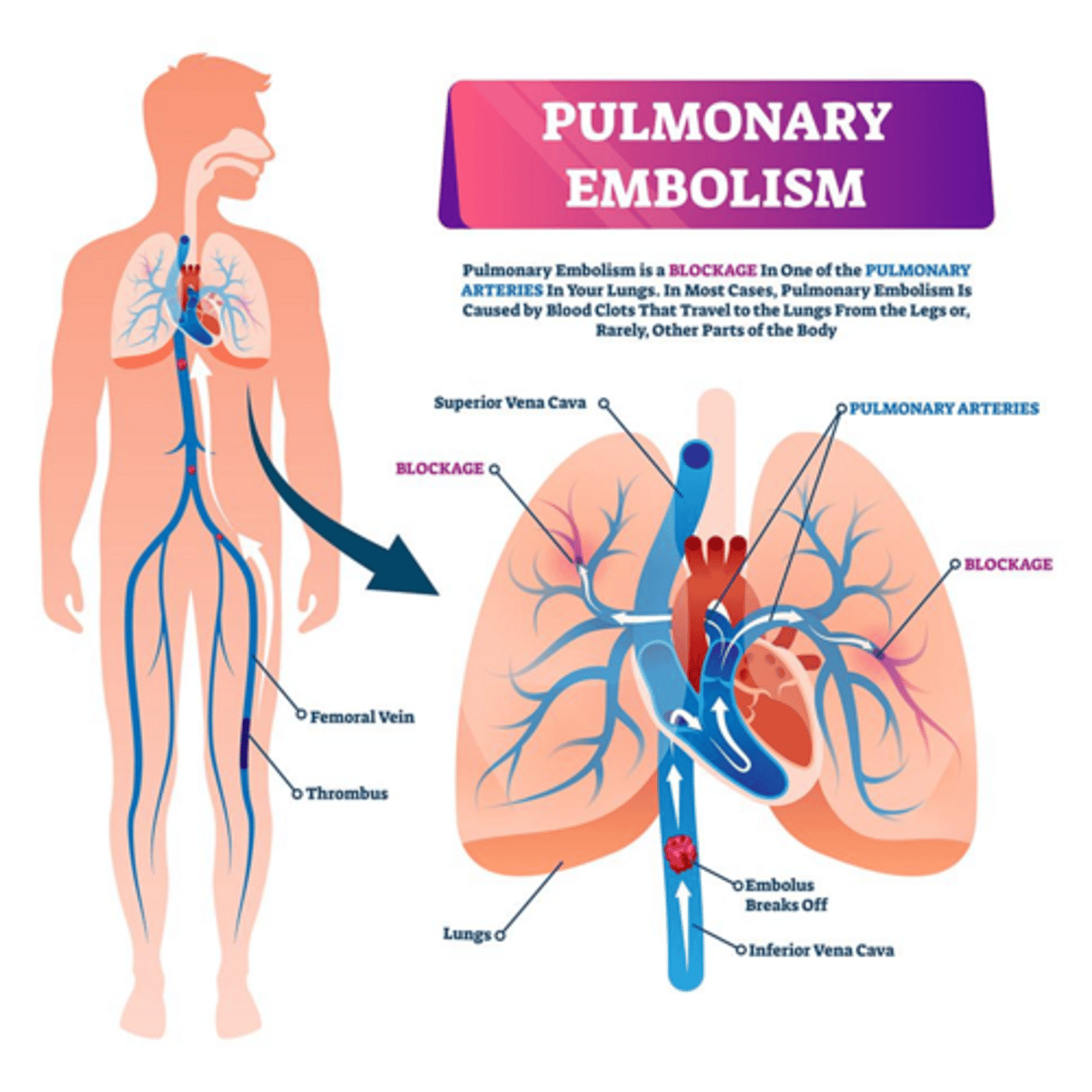
What is the primary symptom of PE?
Dyspnea, chest pain, tachycardia, syncope, hypoxia
What diagnostic tests are used for PE?
CT pulmonary angiography (CTPA) and V/Q scan
What does D-dimer indicate?
It detects fibrin clot degradation products and is sensitive but not specific for VTE.
What is Virchow's Triad?
A framework for understanding the risk factors for VTE: blood stasis, endothelial injury, and hypercoagulability.
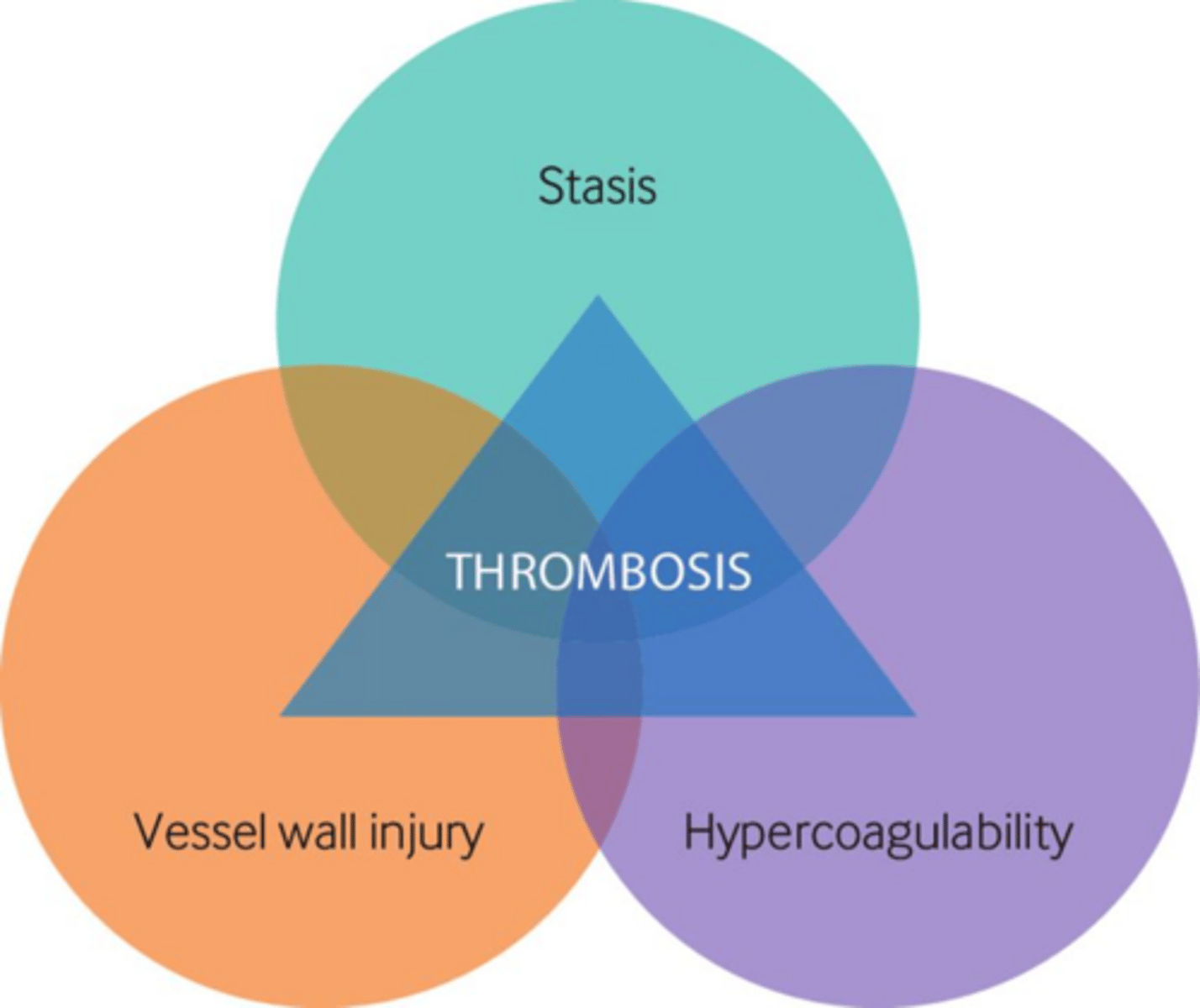
What are some causes of blood stasis?
Immobility, hospitalization, paralysis, long-haul travel, obesity.
What are some causes of endothelial injury?
Surgery, trauma, indwelling venous catheter, inflammatory bowel disease, infection.
What are some causes of hypercoagulability?
Cancer, antiphospholipid syndrome, factor V Leiden, pregnancy, estrogen use, polycythemia vera.
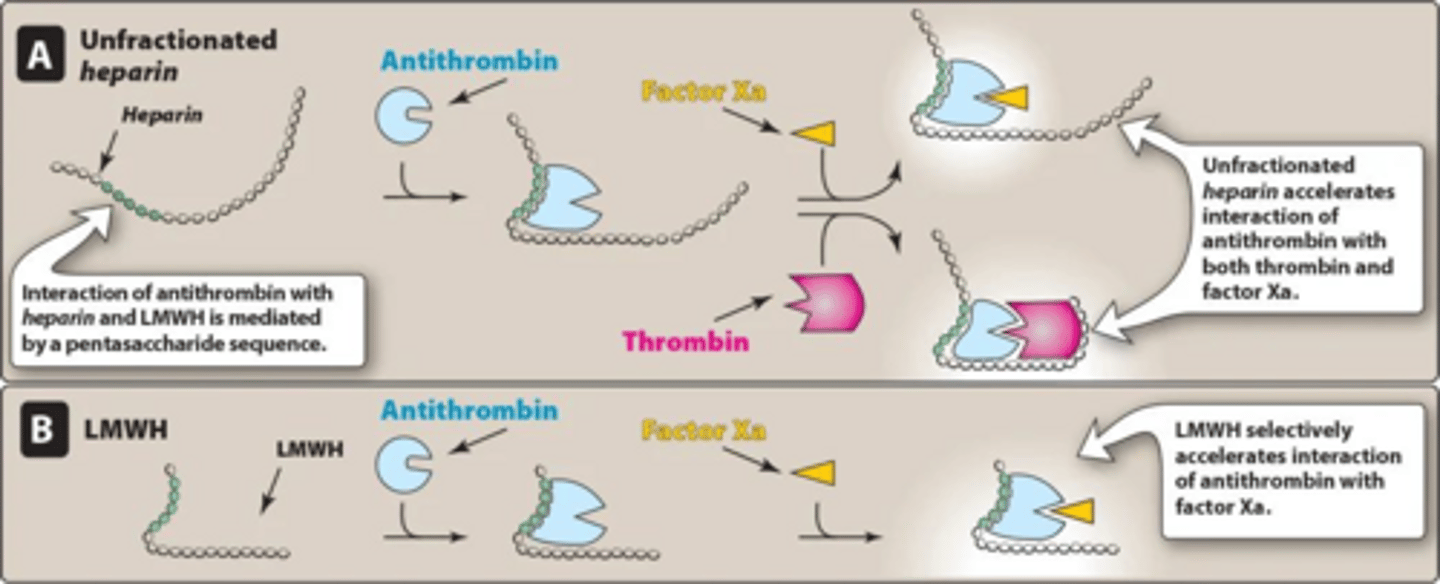
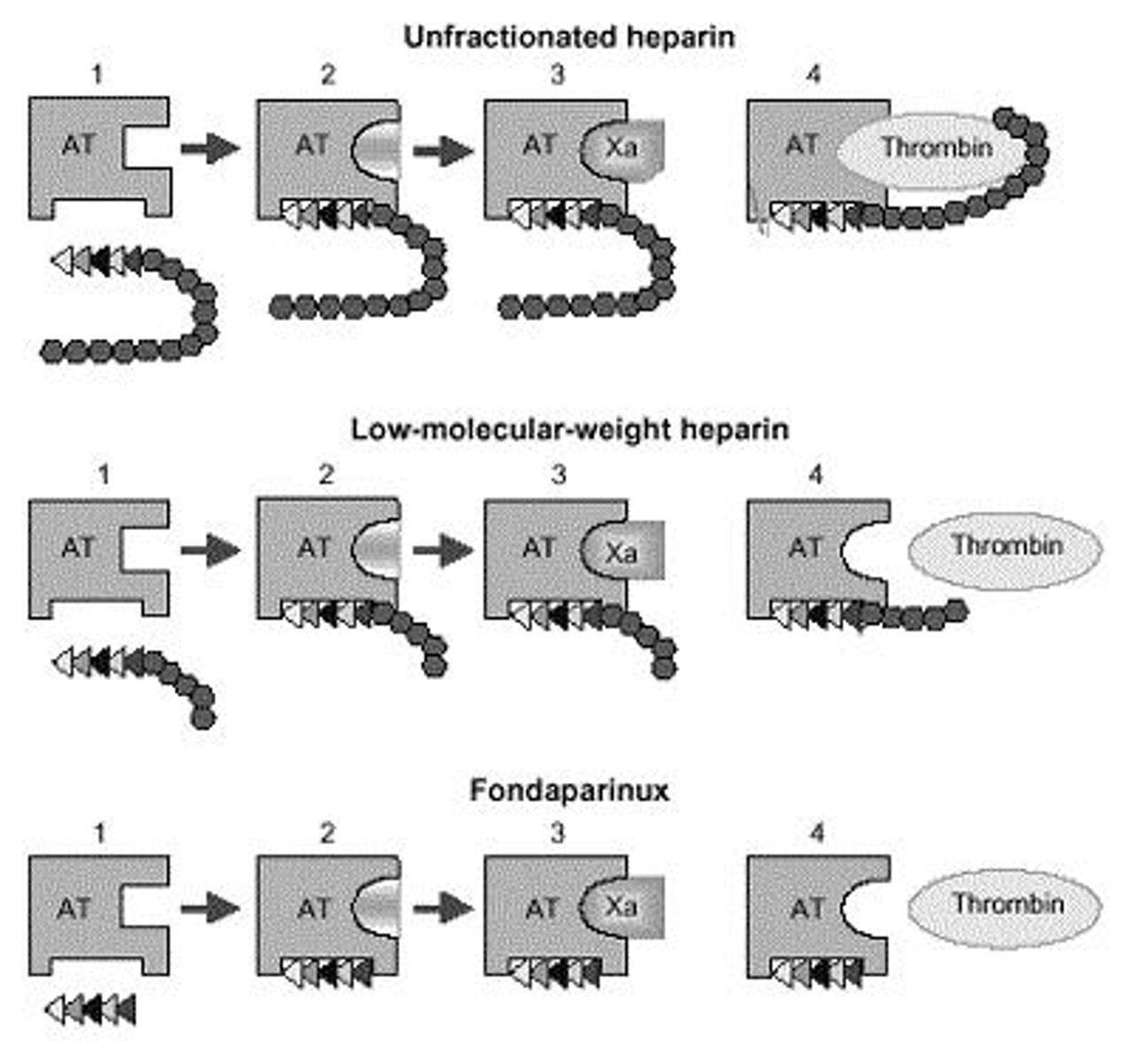
What is the mechanism of action of unfractionated heparin (UFH)?
Binds antithrombin to inactivate thrombin (IIa) and factor Xa.
What is the preferred anticoagulant for patients with renal failure?
Unfractionated heparin (UFH)
What is the dosing protocol for UFH in prophylaxis?
5,000 units SubQ every 8-12 hours.
What is the mechanism of action of low molecular weight heparin (LMWH)?
Binds antithrombin to primarily inhibit factor Xa with minimal inhibition of thrombin (IIa).
What is the dosing for enoxaparin (Lovenox) in treatment?
1 mg/kg SubQ every 12 hours or 1.5 mg/kg every 24 hours.
What anticoagulant is contraindicated in patients with a history of heparin-induced thrombocytopenia (HIT)?
Both unfractionated heparin (UFH) and low molecular weight heparin (LMWH).
What is the mechanism of action of direct oral anticoagulants (DOACs)?
They directly inhibit factor Xa or thrombin (IIa).
Name a direct thrombin inhibitor.
Dabigatran (Pradaxa)
What is the role of aspirin in VTE management?
It irreversibly inhibits COX-1 and COX-2, inhibiting platelet aggregation.
What are the key monitoring parameters for anticoagulants?
INR, renal function, anti-Xa levels, and complete blood count (CBC).
What is the role of thrombolytic therapy (tPA) in PE?
It is appropriate in massive PE with hemodynamic instability.
What is the primary treatment for acute DVT?
Anticoagulants such as UFH, LMWH, DOACs, or warfarin.
What is the difference between provoked and unprovoked VTE?
Provoked VTE occurs due to identifiable risk factors, while unprovoked VTE occurs without any identifiable cause.
What is the recommended duration of anticoagulation for unprovoked VTE?
Indefinite therapy is often recommended after initial treatment.
What are intermittent pneumatic compression (IPC) devices used for?
They are non-pharmacologic interventions to prevent VTE in at-risk patients.
What is the role of lifestyle modifications in VTE prevention?
They can reduce risk factors associated with VTE, such as obesity and immobility.
What factor does Enoxaparin (Lovenox) inhibit?
Factor Xa and Factor IIa (thrombin)
What factor does Fondaparinux (Arixtra) inhibit?
Factor Xa
True or False: Aspirin is a primary treatment option for VTE.
False
Which anticoagulant can be used in hemodialysis patients?
Dabigatran (Pradaxa)
Which anticoagulant can be used in renal impaired patients?
Apixaban (Eliquis)
What is the mechanism of action of Dabigatran (Pradaxa)?
Directly inhibits Factor IIa (thrombin)
What is the dosing regimen for Dabigatran prophylaxis after knee/hip surgery?
110 mg after surgery, then 220 mg PO daily for 10-35 days
What are common adverse effects of Dabigatran?
Bleeding, dyspepsia, GI bleeds
What is the required lead-in for Dabigatran treatment?
Requires ≥5-day parenteral anticoagulation lead-in
What is the dosing frequency for Apixaban (Eliquis)?
BID (twice daily)
What is the dosing frequency for Rivaroxaban (Xarelto)?
BID for 7 days, then daily
What is the dosing regimen for Edoxaban (Savaysa) in VTE treatment?
15 mg BID for 21 days, then 20 mg once daily
What is the target INR for VTE treatment with Warfarin?
2-3
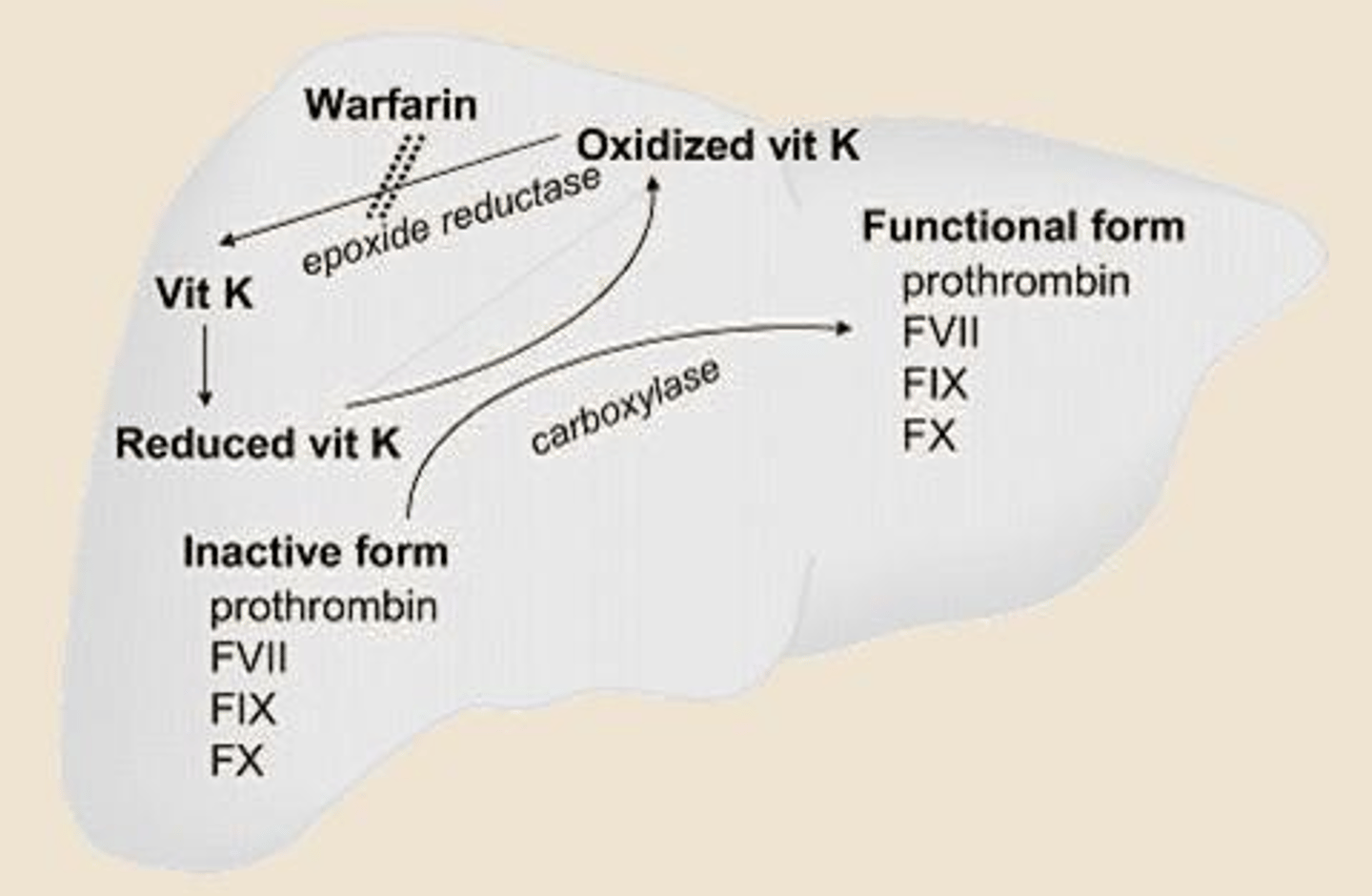
What is the mechanism of action of Warfarin?
Inhibits vitamin K epoxide reductase, blocking synthesis of vitamin K-dependent clotting factors
What should be monitored when a patient is on Warfarin?
INR (International Normalized Ratio)
What is a significant concern when using Warfarin?
Narrow therapeutic index and numerous drug interactions
What is the effect of increased vitamin K intake on INR?
Decreases INR
What is the effect of CYP3A4 inhibitors on Apixaban?
Increases bleeding risk
What is the preferred anticoagulant for patients with antiphospholipid syndrome?
Warfarin
What should be done if a patient on Warfarin increases vitamin K intake?
Adjust Warfarin dose upward by 10-20% of total weekly dose
What is the clinical scenario for Mr. D with confirmed DVT?
Choose Rivaroxaban for initial management
What is the clinical scenario for Mrs. R with antiphospholipid syndrome?
Increase Warfarin dose due to decreased INR from increased vitamin K intake
What is the dosing regimen for Apixaban in long-term VTE prophylaxis?
2.5 mg PO BID after at least 6 months of treatment
What is the dosing regimen for Edoxaban in long-term VTE prophylaxis?
10 mg daily after 6 months of treatment
What is the risk associated with spinal/epidural hematoma in anticoagulant therapy?
Increased risk of bleeding and complications
What is the effect of renal impairment on the use of Rivaroxaban?
Avoid if CrCl < 15
What is the effect of renal impairment on the use of Edoxaban?
Avoid if CrCl < 15 or > 95
What is the mechanism of action of Alteplase (tPA)?
Converts plasminogen to plasmin, leading to fibrinolysis.
What is the approved dosage of Alteplase for pulmonary embolism?
100 mg IV over 2 hours.
When is anticoagulant therapy preferred over thrombolytics in pulmonary embolism?
In acute hemodynamically stable patients who are not hypotensive (SBP ≥ 90).
What are the absolute contraindications for using Alteplase?
Active internal bleeding, prior intracranial hemorrhage, ischemic CVA <3 months, recent intracranial/spinal surgery, brain cancer, severe uncontrolled hypertension.
What are the major adverse effects of thrombolytic therapy?
Intracranial hemorrhage, cerebrovascular accident (CVA), major gastrointestinal bleed.
What is the scoring system used to assess the probability of Heparin-Induced Thrombocytopenia (HIT)?
4 Ts scoring system.
What does a score of 6-8 on the 4 Ts indicate?
High probability of HIT.
What is the primary complication associated with HIT?
Thrombosis, not just low platelet counts.
What should be done if HIT is suspected?
Stop heparin and start non-heparin anticoagulation.
Which anticoagulant is preferred for patients with renal dysfunction?
Argatroban IV (direct thrombin inhibitor).
What is the recommended duration of anticoagulation for a patient with a provoked VTE?
Minimum of 3 months.
When should a thrombolytic be used for venous thromboembolism (VTE)?
In cases of unstable pulmonary embolism (hypotension).
What is the first-line treatment for DVT and PE according to recent guidelines?
Direct Oral Anticoagulants (DOACs) are generally preferred over warfarin.
What is the typical management for a patient with unprovoked VTE?
Indefinite anticoagulation is recommended due to high recurrence risk.
What are the preferred anticoagulants for pregnant patients?
Unfractionated heparin (UFH) or low molecular weight heparin (LMWH).
What is the recommended approach for switching from warfarin to a DOAC?
Check INR before switching; start DOAC when INR is below the threshold (varies by DOAC).
What is the role of catheter-directed thrombolysis?
Used for submassive pulmonary embolism with lower doses to reduce systemic bleeding risk.
What is the treatment duration for recurrent VTE?
Indefinite anticoagulation is recommended.
What should be monitored in patients on warfarin?
INR levels and signs of bleeding.
What is the significance of the 4 Ts in HIT diagnosis?
It assesses thrombocytopenia, timing, thrombosis, and other causes.
What is the preferred treatment for cancer-associated VTE?
LMWH is historically first-line, but DOACs are now preferred.
What is the main concern regarding anticoagulation reversal?
Intracranial hemorrhage (ICH).
What is the recommended duration of non-heparin anticoagulation for VTE?
At least 3 months.
What should be done for patients with HIT and active bleeding?
Anticoagulation should be reversed and non-heparin alternatives should be used.
What is the role of pneumatic compression stockings in VTE prevention?
Non-pharmacological method for high thrombosis risk patients.
What is the significance of the Serotonin Release Assay (SRA) in HIT?
It confirms the diagnosis of HIT.
What is the risk of reversing anticoagulation?
It can cause thrombosis.
What is the half-life of Dabigatran?
12 to 14 hours.
How long does it take for 5 half-lives of Dabigatran to elapse?
Day 2.5 to 3.
What percentage of Dabigatran is cleared by the kidney?
80 to 85%.
What is the reversal agent for Dabigatran?
Idarucizumab (Praxbind).
What is the half-life of Apixaban?
Approximately 12 hours (range, 8 to 15).
How long does it take for 5 half-lives of Apixaban to elapse?
Day 1.5 to 3.
What percentage of Apixaban is cleared by the kidney?
27%.
What is the half-life of Edoxaban?
10 to 14 hours.
What is the half-life of Rivaroxaban?
11 to 13 hours.
What is the reversal agent for Rivaroxaban?
4-factor prothrombin complex concentrate (4F-PCC; Kcentra).
What is the dosing for vitamin K in major bleeding with Warfarin?
10 mg IV with Kcentra.
What is the mechanism of action of vitamin K?
Promotes liver synthesis of factors II, VII, IX, and X.
What is the reversal agent for Heparin?
Protamine.
What is the dosing for Protamine in Heparin reversal?
1 mg IV protamine per 100 units of heparin received in the last 2-3 hours.
What is the preferred anticoagulant for a patient with CrCl 28?
Apixaban.
What is the initial dose of Apixaban for a patient with CrCl 28?
10 mg BID for 7 days, then 5 mg BID.
What interaction does fluconazole have with Apixaban?
Fluconazole is a strong CYP3A4 and CYP2C9 inhibitor, increasing Apixaban levels.
What is the management for a stable PE?
Start anticoagulation; thrombolytics are not indicated.
What is the indication for an IVC filter?
Only when anticoagulation is absolutely contraindicated.