Physical Dysfunction topics given for final
1/333
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
334 Terms
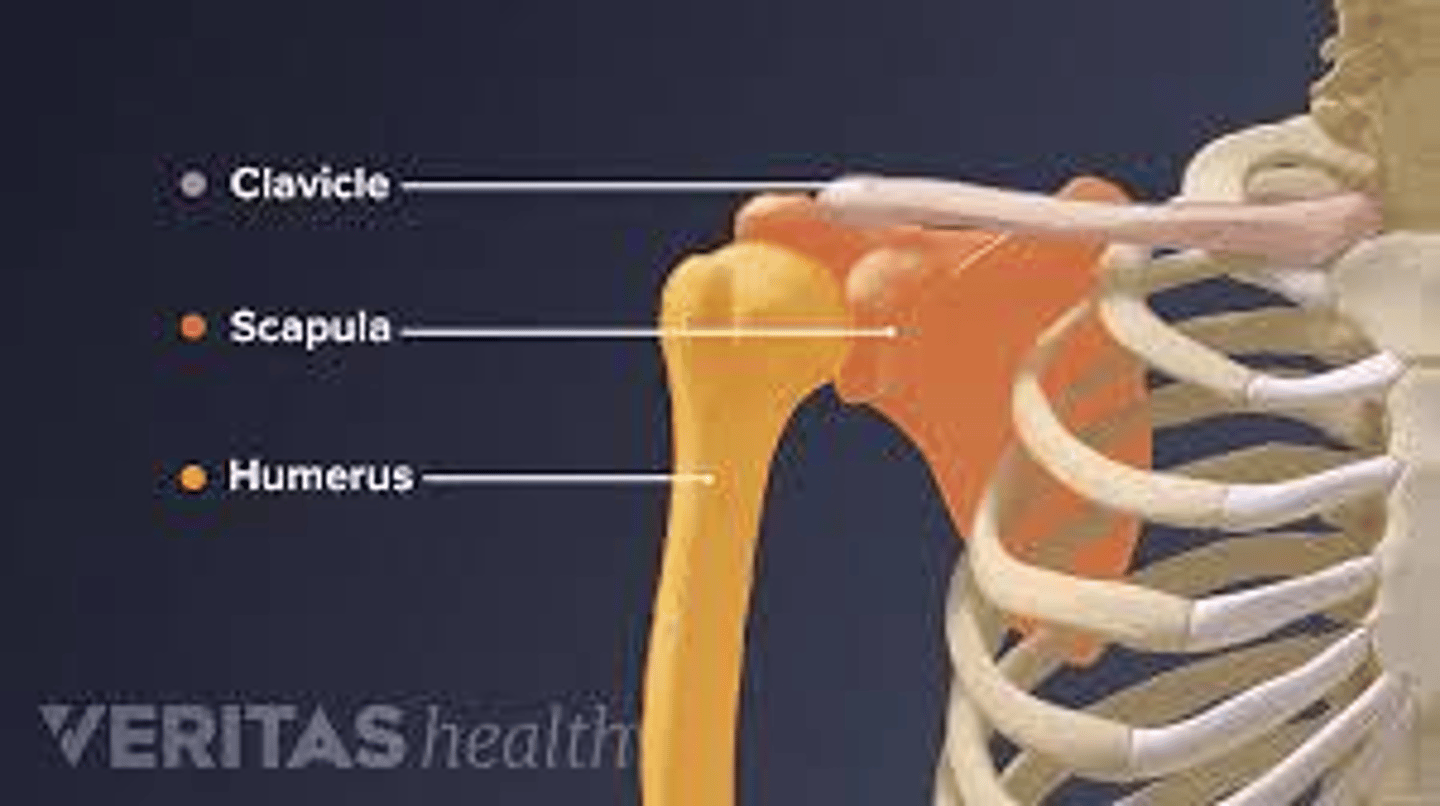
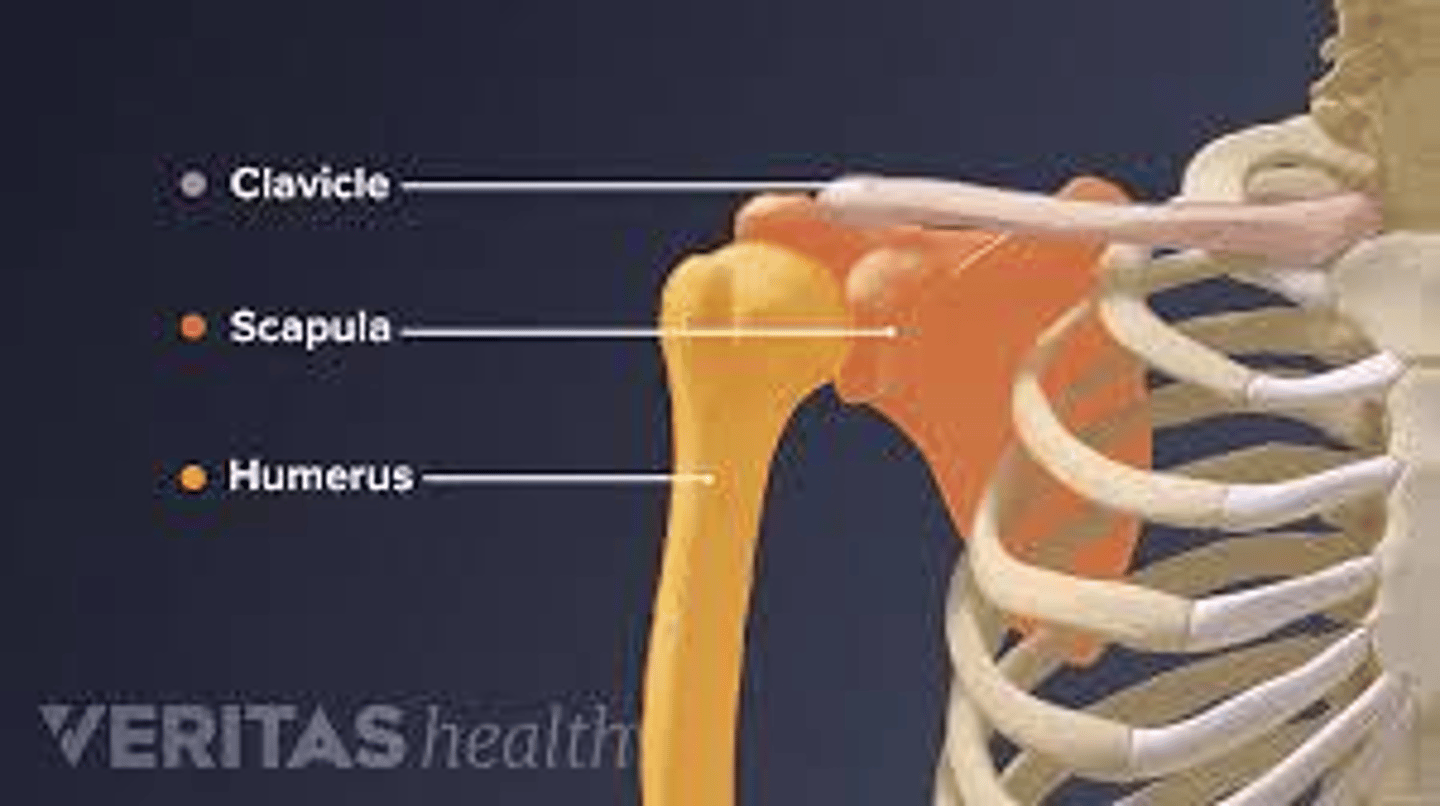
What are the three articulations of the scapula?
The clavicle, the humerus, and the posterior ribs.
List the six movements of the scapula.
Elevation, depression, protraction, retraction, upward rotation, and downward rotation.
Which muscles are considered the primary scapular stabilizers?
Trapezius, serratus anterior, levator scapulae, rhomboids (major/minor), and pectoralis minor.
Which muscles are responsible for scapular elevation?
Upper trapezius and levator scapulae.
Which muscles are responsible for scapular protraction?
Serratus anterior and pectoralis minor.
What scapular movements occur during humeral abduction?
Upward rotation, posterior tilting, and external rotation.
What scapular movement is coupled with humeral internal rotation?
Scapular protraction (abduction).
What does the acronym SICK stand for in the context of scapular dyskinesia?
Scapular malposition, Inferior medial border prominence, Coracoid pain, and Kinesis abnormalities.
Which nerve injury is associated with a winging scapula?
The long thoracic nerve.
What is Snapping Scapula syndrome?
An audible or palpable clicking/grinding caused by the scapula rubbing against the rib cage.
Where is the inferior angle of the scapula typically located?
Close to the level of the T7 vertebra.
How do you locate the coracoid process during palpation?
1-2 finger breadths inferior to the lateral third of the clavicle, feeling for a hard, rounded, tender knob.
What is the purpose of scapular protraction/retraction manual techniques?
To improve reaching, pulling, and pushing activities, provide postural support, reduce guarding, and build trust.
What is the purpose of the Scapular Distraction manual technique?
To improve upward rotation of the scapula to facilitate better flexion/abduction of the shoulder.
In the side-lying position for scapular mobilization, where should the stabilizing hand be placed?
On the superior border or spine of the scapula.
What are the four PNF patterns for the scapula?
Anterior elevation, posterior elevation, anterior depression, and posterior depression.
Which muscle is associated with a soft tissue restriction in anterior elevation?
Latissimus dorsi.
Which muscles are associated with soft tissue restrictions in posterior depression?
Upper trapezius and levator scapulae.
What is the goal of active assisted upward rotation treatment?
To improve general mobility, proprioception, and positional tolerances of the scapula to improve shoulder AROM.
What is the correct patient positioning for scapular mobilization techniques?
Side-lying with neutral head, hips flexed, and ear aligned with the acromion and trochanter.
What is the progression for manual therapy scapular exercises?
Passive to active assistive to active to resisted.
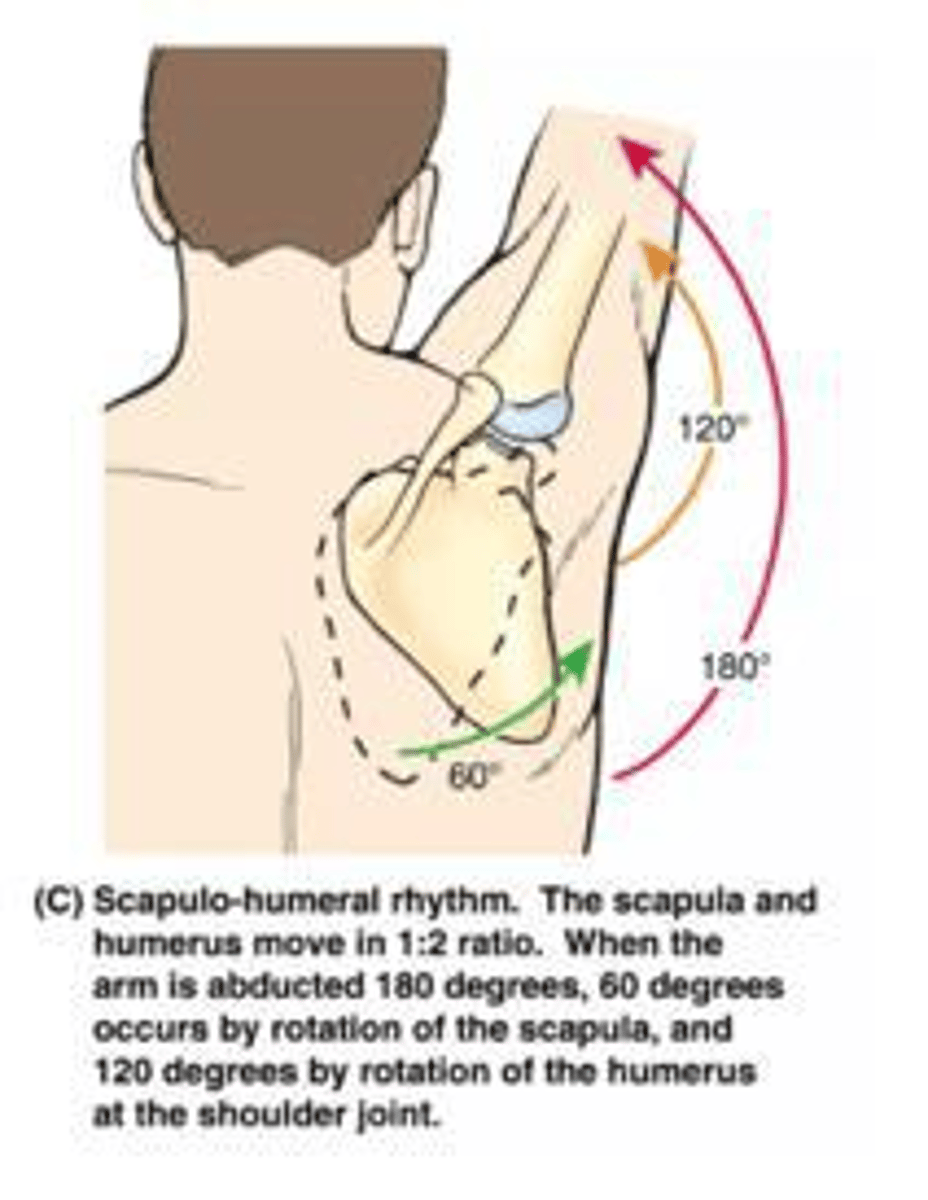
What is the clinical significance of scapular humeral rhythm?
It allows for maximum motion of the upper extremity and provides shoulder stability.
What should be considered when addressing the scapula in exercise intervention?
Incorporating the core.
What are the three articulations of the scapula?
The clavicle, the humerus, and the posterior ribs.
What is the generally accepted ratio for scapulohumeral rhythm?
1:2.
List the six movements of the scapula.
Elevation, depression, protraction, retraction, upward rotation, and downward rotation.
Which muscles are considered the primary scapular stabilizers?
Trapezius, serratus anterior, levator scapulae, rhomboids (major/minor), and pectoralis minor.
Which muscles are responsible for scapular elevation?
Upper trapezius and levator scapulae.
Which muscles are responsible for scapular protraction?
Serratus anterior and pectoralis minor.
What scapular movements occur during humeral abduction?
Upward rotation, posterior tilting, and external rotation.
What scapular movement is coupled with humeral internal rotation?
Scapular protraction (abduction).
What does the acronym SICK stand for in the context of scapular dyskinesia?
Scapular malposition, Inferior medial border prominence, Coracoid pain, and Kinesis abnormalities.
Which nerve injury is associated with a winging scapula?
The long thoracic nerve.
What is Snapping Scapula syndrome?
An audible or palpable clicking/grinding caused by the scapula rubbing against the rib cage.
Where is the inferior angle of the scapula typically located?
Close to the level of the T7 vertebra.
How do you locate the coracoid process during palpation?
1-2 finger breadths inferior to the lateral third of the clavicle, feeling for a hard, rounded, tender knob.
What is the purpose of scapular protraction/retraction manual techniques?
To improve reaching, pulling, and pushing activities, provide postural support, reduce guarding, and build trust.
What is the purpose of the Scapular Distraction manual technique?
To improve upward rotation of the scapula to facilitate better flexion/abduction of the shoulder.
In the side-lying position for scapular mobilization, where should the stabilizing hand be placed?
On the superior border or spine of the scapula.
What are the four PNF patterns for the scapula?
Anterior elevation, posterior elevation, anterior depression, and posterior depression.
Which muscle is associated with a soft tissue restriction in anterior elevation?
Latissimus dorsi.
Which muscles are associated with soft tissue restrictions in posterior depression?
Upper trapezius and levator scapulae.
What is the goal of active assisted upward rotation treatment?
To improve general mobility, proprioception, and positional tolerances of the scapula to improve shoulder AROM.
What is the correct patient positioning for scapular mobilization techniques?
Side-lying with neutral head, hips flexed, and ear aligned with the acromion and trochanter.
What is the progression for manual therapy scapular exercises?
Passive to active assistive to active to resisted.
What is the clinical significance of scapular humeral rhythm?
It allows for maximum motion of the upper extremity and provides shoulder stability.
What should be considered when addressing the scapula in exercise intervention?
Incorporating the core.
How many people in the US have some type of amputation or limb loss?
An estimated 2 million people.
What is the most common cause of limb loss in the upper extremity (UE)?
Trauma.
What is the most common cause of limb loss in the lower extremity (LE)?
Vascular disease.
What percentage of clients with amputations may require a second amputation within 2-3 years?
Over half.
What are the most common types of amputation secondary to cancers?
Osteosarcoma and Ewing's Sarcoma.
What psychosocial impacts can result from limb loss?
Alterations in self-awareness, performance skills, and social interaction skills.
What are the stages of grief progression after an amputation?
Shock, disbelief, denial, anger, guilt, bargaining, yearning, and acceptance.
What is phantom limb sensation/pain?
Sensations experienced in the area where the limb was amputated, including pulling, tingling, or pain.
What percentage of clients experience phantom limb sensations after amputations?
50-85%.
What is a socket in the context of prostheses?
The piece of the prosthesis that fits around the residual limb to attach the prosthesis.
What is the difference between a passive and a prehensile terminal device?
Passive TD is static and cosmetic; prehensile TD provides active grasp.
What is a voluntary opening (VO) device?
A device where the terminal device is held closed by a rubber band or spring and opens when a cable is pulled.
What is the cost range for a simple cosmetic prosthesis?
$5,000.
What is the cost of an advanced myoelectric prosthesis?
Around $100,000.
What is the purpose of a silicone liner in early management after amputation?
To provide constant pressure on the site to prevent hypertrophic scar tissue.
What is desensitization in the context of amputations?
A process that decreases sensitivity to stimuli to normalize the body's response.
What is myosite testing used for?
To determine clear signals for the use of a myoelectric prosthesis.
What is the goal of phase three in prosthetic training?
To incorporate prosthetic use into activities of daily living (ADLs).
What is mirror therapy?
A technique that decreases phantom limb pain by creating an illusion of two intact limbs.
What is targeted muscle reinnervation (TMR)?
A surgical procedure that enhances the use of myoelectric signals for intuitive control of a prosthesis.
What should be monitored to avoid skin irritation in prosthetic users?
Skin irritation, sweating, and moisture on the skin.
What is the importance of client education in the context of amputations?
It is critical for managing expectations and promoting adaptation to limb loss.
What is the role of prosthetic socks?
To fill the space between the socket and the residual limb.
What is the significance of performing regular skin checks for prosthetic users?
To prevent shearing irritation and maintain skin integrity.
What is the purpose of limb wrapping techniques?
To shape the residual limb and promote healing.
What is the recommended frequency for desensitization techniques?
Three times a day for 20-30 minutes if tolerated.
What is the function of a terminal device in a prosthesis?
It acts as the hand for grasping and manipulation.
What is the benefit of using fragrance-free lotion on the residual limb?
To prevent dryness and maintain skin integrity once the wound has healed.
What does grading mean in therapeutic treatment?
Grading is adjusting the difficulty of an activity while maintaining the same therapeutic goal.
What is the purpose of grading activities?
To match activity to client ability, promote success and challenge, and support progress toward independence.
Give an example of grading an activity.
Buttoning a shirt may be graded easier or harder.
What does upgrading an activity involve?
Making the activity more challenging.
Why might a therapist upgrade an activity?
Because the client is improving, to increase strength/endurance, or to improve coordination or cognition.
List some examples of upgrading an activity.
Increase resistance, add dual-tasking, reduce assistance, increase speed or repetitions, or increase task complexity.
Provide an example of upgrading an activity.
Stacking blocks while standing on a foam surface.
What does downgrading an activity mean?
Making the activity easier.
When might a therapist downgrade an activity?
Due to client fatigue, pain, safety concerns, or early recovery.
List some examples of downgrading an activity.
Provide physical assistance, simplify instructions, reduce repetitions or task demands, use larger or easier materials, or provide additional support or stabilization.
Provide an example of downgrading an activity.
Using larger buttons for buttoning a shirt.
What does adapting an activity involve?
Changing the method, tool, or environment to complete the task.
List some examples of adapting an activity.
Use adaptive equipment, modify the environment, or change the way the task is performed.
Provide an example of adapting an activity.
Using a button hook to button a shirt.
What are some ways to grade activities?
Physical, environmental, assistance, and cognitive.
What factors can be adjusted in physical grading?
Resistance, weight, distance, and repetitions.
What environmental factors can be graded?
Distractions, lighting, and surface stability.
What cognitive factors can be graded?
Level of cueing, physical assistance, number of steps, memory demands, and problem solving.
What should guide grading decisions in therapy?
Clinical reasoning based on the client's needs and abilities.
How can you downgrade an activity for a client recovering from a stroke who struggles to grasp objects?
By providing physical assistance or simplifying the task.
Why adaptive equipment is needed
Maintain independence with ADLs, follow post-surgical precautions, reduce pain and strain on joints, prevent falls or injury.
Common diagnoses for adaptive equipment
Total hip replacement, total knee replacement, arthritis, limited ROM.
Hip precautions (posterior)
Avoid hip flexion > 90°, hip adduction past midline, hip internal rotation.
Why equipment helps with hip precautions
Prevent bending, maintain joint alignment, support safe transfers.
Common lower extremity adaptive equipment
Reacher, sock aid, long-handled shoehorn, long-handled sponge, dressing stick, elastic shoelaces.