kale pancreatitis
1/43
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
44 Terms
endocrine pancreatic fxns
1. release insulin (glucose uptake and glycogen deposition)
2. release glucagon (converts glycogen to glucose)
somatostatin== inhibits glucagon and insulin, reduces pancreatic secretions
which pancreatic cells secrete water, electrolytes, and digestive enzymes
acinar cells
how is pancreatic secretion regulated
1. cephalic phase= sight/smell via vagus nerve (VIP and GRP)
2. intestinal phase
3. hormones== secretin, cholecystokinin
presence of acid in duodenum triggers release of ________
_______ causes release of bicarb
presence of fats in duodenum triggers release of _________
________ triggers release of enzymes
presence of acid in duodenum triggers release of __secretin__
_secretin__ causes release of bicarb
presence of fats in duodenum triggers release of __cholecystokinin___
__cholecystokinin___ triggers release of enzymes
why arent proenzymes automatically activated in pancreas? how do they get activated?
-pancreatic juices have a low level of trypsin inhibitor that stops early activation
- need ENTEROKINASE to activate TRYPSINOGEN which activates enzymes
_______________ activates ___________ which activates pancreatic enzymes
enterokinase; trypsinogen
which drugs are associated with acute pancreatitis
corticosteroids, ACE inhibitors, estrogen, furosemide, codeine, sulfasalazine, Bactrim, sulindac, carbamazepine, isoniazid
incretin based= liraglutide, exenatide, sitagliptan
+ others
gold standard dx of pancreatitis
surgical examination of pancreas
lab parameters of pancreatitis
-leukocytosis (necrosis-> infection-> WBCs)
- hyperglycemia (less insulin)
- increased BUN/Cr
- PT prolongation
- hyperbilirubinemia
- hypocalcemia
- thrombocytopenia
- increased Hbg/Hct
- hypoalbunemia
describe what happens to serum amylase during acute pancreatitis
increases within 24hrs of sx onset, return to normal over 3-4 days
t/f: amylase levels dont correlate to pancreatitis severity and are not specific to the pancreas
true
[compare to lipase which is specific and 7-10 days]
which serum enzyme is specific to pancreatitis and persists longer
serum lipase= specific to pancreas and persists 7-10 days
what dx technique is indicated for pts with suspected biliary involvement
ultrasound
what dx technique is useful in classifying pancreatitis severity and provides an estimate of risk for systemic complications
contract enhanced computer tomography (CECT)
t/f: there is greater mortality with first attacks of pancreatitis than with recurrent
true
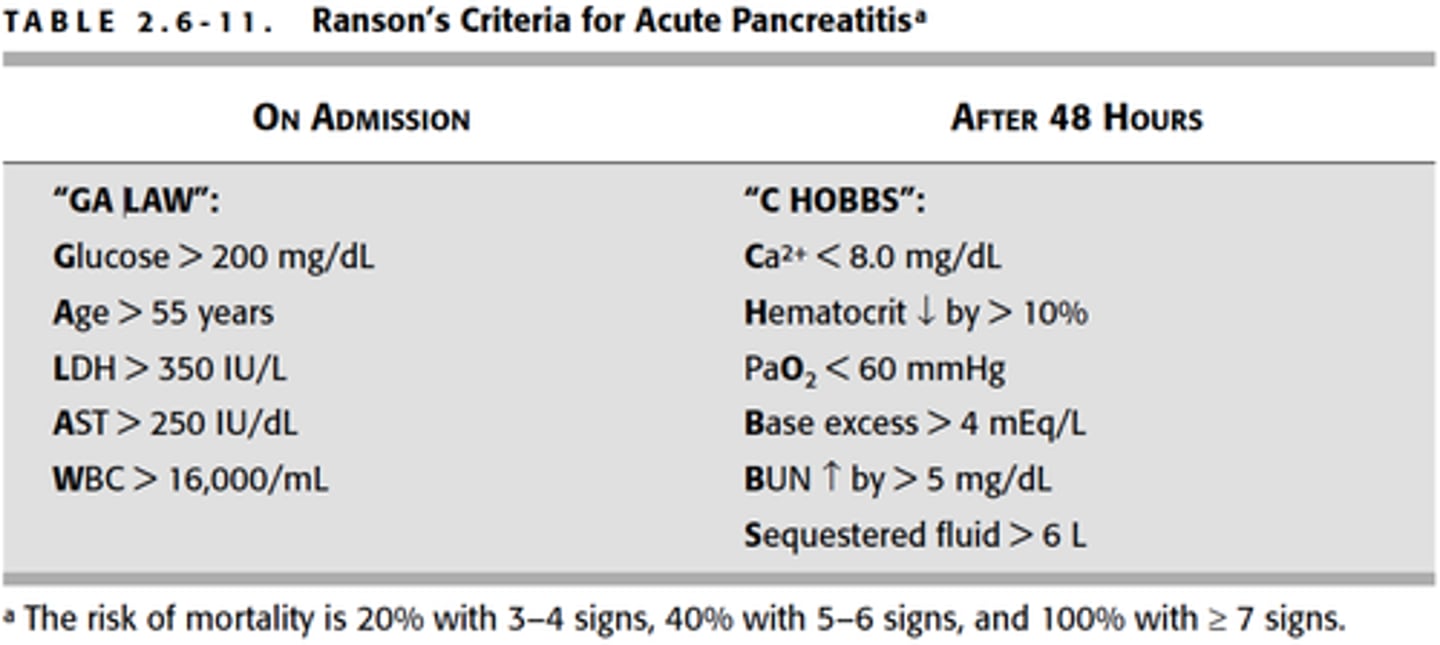
severity and mortality of pancreatitis pts is predicted by
Ranson's criteria
ex: age over 55, WBC, glucose, LDH, etc
phlegmon
mass of inflamed pancreas with patchy areas of necrosis
pseudocyst
cysts with no epithelial lining and most common chronic complication
-> fluid collections of necrotic debris, blood, and pancreatic enzymes
[must be drained]
manifestations of acute pancreatitis include
-hypotension/shock (main cause of death)
-HYPOcalcemia (think of using up Ca to activate enzymes)
-HYPERglycemia
- renal failure
- pulmonary edemas
- coagulopathy
what kind of route is indicated for pancreatitis tx
1. stop ingesting food/liquid [to stop stimulating pancreas]
2. En preferred==NG tube
- TPN INDICATED IF ON BOWEL REST FOR 1 WEEK
3. replace fluid/electrolyte losses
what kind of analgesics are indicated for acute pancreatitis
IV PREFERRED FOR ACUTE ATTACK
1. meperidine 50-100mg IV q4hrs and prn
-CI in renal failure, not rlly used bc seizures
2. morphine
3. hydromorphone (especially in renal insufficiency)
abx and acute pancreatitis tx
- NO benefit as prophylaxis in ethanol induces pancreatitis
- can use abx for pancreatic duct obstruction or abscess/necrotizing
which abx are recommended for secondary infections
1. imipenem 500mg IV q8hrs (covers gram neg and penetrates pancreas)
- NOT FOR PCN ALLERGY (beta lactam)
2. Cipro 400mgIV q12hrs + metro 500mg IV q 8hrs
t/f: H2RAs are the most effective in decreasing GI secretions in pancreatitis
false. not more effective than NG suction
acute pancreatitis tx summary
analgesics
- morphine or hydromorphone
- less preferred: meperidine 50-100mg IV q4hrs/prn
abx
- not needed as prophylaxis in alcohol induced
- can be used in pancreatic duct obstruction/ abscess/ necrotizing
1. imipenem 500mg IV q8hrs (covers gram neg and penetrates pancreas)
- NOT FOR PCN ALLERGY (beta lactam)
2. Cipro 400mg IV q12hrs + metro 500mg IV q 8hrs
t/f: chronic pancreatitis results in functional and structural damage to the pancreas and is irreversible
true
etiologies of chronic pancreatitis
alcohol
hyperparathyroidism (Ca activating all the proenzymes)
PCM (not enough protein)
heredity
trauma
duct obstruction
chronic pancreatitis clinical presentation
1. dull constant pain, epigastric and radiating through back
may be accompanied by N/V and weight loss
2. malabsorption= >7g of fat in feces-> steatorrhea and azotorrhea
- B12 malabsorption
-> diabetes, weight loss, jaundice
clinical triad of chronic pancreatitis dx
Chronic Disease Suck
calcification, steatorrhea, diabetes (10-20yrs of alcohol use)
t/f: serum amylase and lipase not useful in diagnosing chronic pancreatitis
true. lipase useful in acute only. amylase not rlly useful
gold standard diagnosing technique for chronic pancreatitis
ERCP (endoscopic retrograde cholangiopancreatography)
diet tx for chronic pancreatitis
- abstain from EtOH
- eat small and frequent meals (6/day)
- restrict fat (80-100g/day)
analgesics for chronic pancreatitis
- aspirin or tylenol before meals
- use around the clock!!
- opiates for severe pain (oral before parenteral)
celiac plexus block
Pain management technique for chronic pancreatitis
- injection of alcohol into celiac ganglion (3-6 month relief)
summary of chronic pancreatitis tx
1. diet= stop alcohol, eat small frequent meals with low fat
2. use aspirin or tylenol around the clock
- try opioids if rlly needed
3. enzyme replacement
4. celiac plexus block
how should lipase enzyme supplement be given/ what should be considered
lipase is irreversible inactivated at pH<4, can give H2RA/PPI to not degrade the exogenous enzyme
max delivery of lipase after a meal
140k IU for 4hrs
malabsorption is minimized if the concentration of lipase delivered to duodenum is at least __% of normal max
this means you need _______IU of lipase and ______IU of trypsin during 4hrs after meal
5%
30k IU lipase every meal and 10k IU trypsin
which brand of enzymes are not EC and must be taken with a PPI
Viokase
(others that are EC: pancreaze, creon, zenpep, pertzye, ultresa)
ADEs of supplemental enzymes? monitoring?
hyperuricosuria
hyperuricemia
kideny stones
folic acid deficiency
===monitor uric acid and folic acid levels!
to treat steatorrhea:
begin with pancreatic enzyme supplement: ______units/meal
if dose increase needed: ____ units/meal
if no improvement?
25k-50k/ meal
increase to max of 90k units/meal
add H2RA or PPI and reduce dietary fat
max dose of enzymes
90k units per meal
opioids for chronic pancreatitis
tramadol 50-100mg q4-6hrs
codeine, hydrocodone, morphine sulfate, oxycodone, methadone, hydromorphone
monitoring parameters for pancreaze and counseling
30,000 IU q4 hrs
may cause kidney stones
monitor: folic acid and uric acid levels