Lab Med Final
1/51
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
52 Terms
urine analysis
dip stick and microscopy(presence of five bacteria per high power field means there is an infection and you have to get a culture)
can be used to detect infection, urolithiasis, malignancy, or metabolic disease
also get urine culture and susceptibility
-Complicated UTI
-High-Risk Populations: symptomatic males, pregnancy, females 65+ years old
-Immunocompromised
-Recurrent Infections
-Treatment Failure or Resistance
-Preparation for endoscopic urologic procedures
types of urine specimens
For urine culture and sensitivity: must use clean catch- midstream, sterile container, cleanse urinary meatus with antiseptic. And area cleansed beforehand
random urine specimen: choice for drug screen does not require clean catch or any prep and can be obtained any time of the day
24hr urine: large container that is quantitative study for hormone, glucose, and proteins (nephrotic syndrome for Cr clearance
first morning viod: they viod before bed and then collect the first pee of the day - best for STI testing
urine analysis
includes a urine dip stick and a microscopic exam
drip stick: pH, specific gravity, glucose, bilirubin, nitrates, protein, ketones, acult blood, more affordable (absences of nitrate does not eliminate need for culture bur presence means there an infection)
microscopy- small volume to identify cells - bacteria, crystal, cast present, quantitative(not just yes and no)
both needed: urine having intact RBC and hemoglobin will both be detected by dip stick and microscopy would confirm true hematuria (RBC in urine)
color and transparency
normal- clear to deep yellow
red- bleeding
dark yellow/orange- bilirubinemia
cloudy- pus, RBC, bacteria
specific gravity
high means more concentration could mean dehydration or glucose in urine
low = dilated urine
indication of hydration
pH
high protein diet = lower pH -affected by diet
can indicate kidney stone
shows excretion of acid by metbolic acitivity
blood
detects the presence of hemoglobin and myoglobin, UTI, cancer, nephrolithiasis- false + in myoglobinuria (rhabdo and muscle disorder)
detect peroxidase activity of urinary tract
glucose
is + if blood glucose is above 180 mg/dL as in diabetes
ketones
increase fat metabolism due to low carbs, starvation, vomiting, diabetic ketoacidosis
nitrites
due to bacteria converting nitrates to nitrites (gram -) but not all bacteria does that conversion so does not r/o UTO. E.coli need four hours to convert so if pt is frequently peeing may be false neg
leukocyte esterase
produced by WBC breakdown sign of use UTI
•False positive due to vaginal discharge or menstrual blood, some medications (ex: doxycycline), systemic infections
•False negative due to dilute urine, high level proteinuria or glucosuria, expired test strips
used with nitrites (nitrites is more specific while esterase is more sensitive )
bilirubin
present with liver diseasep
proteins
will not pick all protein but very sensitive to albumin and a sign of renal disease can also be with exercise, seizure, pre-eclampsia
urobilinogen
•present in very low amounts
•Increased with hemolysis, intestinal bacteria
produced from break down of bilirubin in intestine
Combining diagnostic value
•Ruling In: The presence of blood on a dipstick, especially when combined with positive nitrites, has a high predictive value for UTI.
•Ruling Out: While individual negative results are not definitive, the combination of negative LE, negative nitrites, and negative blood is highly effective for eliminating a UTI from the differential diagnosis
leukocyte enterase is produced by
neutrophiles
urine microscopy quantitatively of
cells
cast
crystal
bacteria or yest
if drip stick shows blood cound RBC
if shows nitrites check WBC
crystal
form when mineral in urine precipitate dependent on urine pH and concentration
indicate renal stone
helpful in gout- uric acid crystals
cast
form in renal tubules
•Clumps of material or cells that form in the renal tubules; take on shape of tubules
•Ex: WBC cast in Pyelonephritis
•Ex: RBC casts in glomerulonephritis
urine microalbumin
test for albumin- Prescence nephropathy detectable before GFR goes down
also use to monitor kidney and dietetic monitoring
an increase in microalbumin in diabetics have a higher risk of cardiovascular event, renal disease, retinopathy - should be monitor yearly with diabetics and hypertension
even for non diabetics elevated urine microalbumin correlates to lower life expectancy due to CVD
spot urine albumin/creatine ratio
quantifies the amount of albumin in urine- measures extend of glumonlar damage - therefore the development of kidney disease
1+ or greater= injury to glomeruli
urine electrolytes
•Quantitative measure of electrolyte content of urine (Calcium, Sodium, Potassium)
•Variable clinical utility (ex: Urine sodium aids in diagnostic eval of hyponatremia)
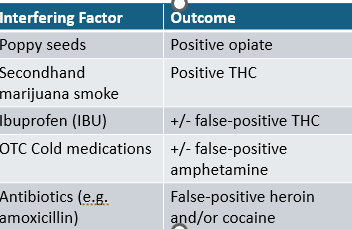
urine drug test
qualitative:•Amphetamines
•Barbiturates
•Cocaine
•Marijuana (THC)
•MDMA
•Methadone
•Opiates
•Oxycodone
where is lect 17
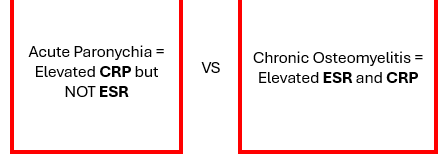
acute phase reactants
proteins whose plasma concentration increase/ decrease 25%during inflammatory stress
levels reflect the Prescence and intensity of the inflammatory process
IL-6 inducer of most APR other IF Y, TNF, IL1 - negative APR like albumin and ferratin
most common are ESR/ CRP
Eythrocyte sedimentation rate ESR
EBC suspended in plasma fall when place in a vertical tube good at measuring fibrinogen non specific can also be impacted in changes in RBC size, shape, number and tequnical factors
•infection, inflammation, advanced neoplasm, tissue necrosis, or infarction with these condition: RBC have more fibrinogen and will fall faster '
helpful: monitoring disease courses for autoimmune
ESR limination
very nonspecific influence by many factors any tissue injury, increase protein levels, anemia , smoking/ obesity, pregnancy, specimen handling, age (increase with age),
C- reactive protein (CRP)
an acute phase reaction - better than ESR levels rise and fall faster
nonspecific for infection, inflammation, and tissue necrosis
preferred for detecting early inflammatory responses
protein produced by the liver during an acute inflammatory process
good for cardiovascular and connective tissue disorders
more sensitive for rapidly responding indicator of inflammation- measuring only one protein while ERS is an accumulation
good parker for future cardiovascular event (plaque have inflammation markers)
4-6 hrs when it rise
could mean bacterial, MI, inflammatory response- mainly reserved for cardiovascular screening than general inflammatory
limitations of a CRP/ ESR
can have false positive so only use when there is clinical susception
ANA
•ANA = type of autoantibody that targets substances inside the nucleus of cells (nuclear antigens).
•Most commonly used to screen for autoimmune diseases; especially connective tissue disease
•Sensitivity variable depending on disease
•Specificity= low
•Clinical Context is KEY– pretest probability is important
•Higher pretest probability of autoimmune disease, the more value ANA has
-high sensitivity or lupus (good for r/o) also present in viral infection hismatoos, scleroderma,
order when high test probability
reported as a titer and pattern (lower titers are often insignificant with no sx of signs of autoimmune diease)
ANA and RF
both antibody test
ANA-lupus
RF- RA
RA
inflammation joint destruction and deformities
RA the antibody that is created against the synovial joints
symmetric polyarthritis, morning stiffness, extraarticular manifestation
abnormal antigenic IgG antibodies, antibodies against Fc portion of antigen IgG produced
RF and ACPA (Anti-citrullinated peptide antibodies (ACPA or anti-ccp) confirm RA diagnosis
RF has lower sensitivity but higher specificity
higher levels of RA= greater likelihood the pt had true rheumatic disease and can correspond to worse prognosis and poor drug responsiveness
serum uric acid
gout testing (hyperuricemia) - monosodium urate crystals that cause joint point
crystal formed from so oversaturation of serum acid
shellfish, anchovies, alc increase uric acid
uric acid levels in gout
can be high, low, or normal during acute flare
how long does it take for resolution of gout flare
2 weeks to completely normalize
what is the goal for urate lowering meds
less than 6mg/dL want to make sure you have the right titration of medications
make sure to wait 2 weeks out from a flare to get serum and make alteration to medications
does a normal serum uric acid level mean you can r/o a flare
no can be in normal range during acute flare
clot byproductions
fibrinogen and d-dimer
D dimer used to identify
intravascular clotting so like a DVT, PE, and disseminated intravascular coagulation (DIC- accelerated clotting, increase platelets, and uncontrollable bleeding)
highly sensitive but no specific good for r/o is high needs imagining for confirmation
advanced age = above 50 age x 10= threshold positive
is there is a high pretest probability for PE or something like that
skip the D-dimer and go directly to imaging
MUST consider the pre-test probability prior to ordering
using the modified well criteria and PERC rule = but do not have to know the criteria
When to not order a D-dimer
when there is a very low risk patient
or
extremely high risk patients that have a high pre test probability they go straight to imaging
all pregnancy test based
on detection of hCG
hCG double every 3 days for the first 6 weeks - then declines after the first trimester
urine HCG
known as point of care
qualitative not quantitative
false neg- testing before levels are detectable
false +
serum HcG
qualitative and quantitative ability to trend the levels
-ensure complete evacuation of products of miscarriage
-serial monitoring demonstrating abnormal low or slowly can suggest ectopic or miscarriage
abnormal high hCG
molar pregnancy
LH from and what it does, why would we check
anterior pituitary gland
acts on either ovaries and testes that stimulates hormone release -used when checking for primary hypogonadism (LH will be high but the hormone will be low)
Leydig cell
Klinefelter syndrome
boys
turner syndrome
increase in FSH/ LH
menopose
FSH will be high cause there is no negative feedback of estrogen
testosterone
best time to take 7
DHEA- testosterone in peripherical fat and some produced in the adrenal and ovaries ?
finish last three
slides
test twice for hypogonsism
HPV
starting at 21 regardless of sexual activity with pap (cytology) every 3 years and after 30 HPV testing every five years
HPV testing is via vaginal swab and does not e