Ch 12: Motivation & Regulation of Internal States
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
Motivation
= factors that initiate, sustain & direct behaviours
behaviour thats NOT explained solely by outside stimuli, bc our internal states are driving it
→ NO theory fits it perfectly
Instinct
= behaviour thats automatic, unlearned & unmodifiable, occurring in everyone in a species (innate)
ex. animal migration & parental behaviour
NOT used to discuss humans → use drive theory instead
Incentive & Arousal Theories
Incentive Theory = ppl are motivated by external stimuli, not just internal needs
ex. full → eat more dessert
ex. hungry → still dieting
ex. starting drugs to look “cool”
Arousal Theory = ppl act in ways to maintain a PREFERRED level of stimulation
thus, they seek out stimulation, not just bc of external stimuli or needs
they like being outside of homeostasis
ex. adrenalin junky
Drive Theory (use for humans)
= body drives return to homeostasis (balance)
Drive = aroused condition
ex. hungry → body drives u to eat
→ CANT explain why we leave homeostasis (ex. eating too much)
Drive Theory: 1. Temperature
→ use drive theory to maintain ideal (set point) body temp
Set point = point of homeostasis the body returns to (can change)
women have a higher set point, thus need more warmth & perceive bigger differences in temp
Temperature Regulation:
ECTOthermic animals = need external heat to regulate internal heat
ENDOthermic animals = have internal heat regulation
via: Preoptic area = contains warmth-sensitive & cold-sensitive cells in hypothalamus of mammals
→ activates something to return to homeostasis (ex. shiver when too cold, or sweat when too hot)
Drive Theory: 2. Thirst
thirst = dry mouth & throat drive when to drink, NOT how much to drink
detected in: brain, heart & kidneys
Types:
Hypovolemic thirst = when blood volume drops from loss of extracellular water ] blood needs water
Osmotic thirst = when cells need water
→ can experience both types of thirst at the SAME time (ex. sweat a lot), or have ONLY osmotic thirst (ex. after salty meals)
Drive Theory: 2. Thirst - Brain Structure Involved
via brain/heart signals:
Subfornical organ (SFO) + Organum Vasculosum lamina terminalis (OVLT) = sense & regulate internal water balance TOGETHER
contain receptors that detect the amount of water in the 3rd ventricles cerebral fluid → tell MnPO
Circumventricular organs = outside blood-brain barrier w direct access to blood circulation → THUS, talk to blood & ventricle using astrocytes
Osmoreceptors = fire more as ventricle’s volume decreases (like it plump)
Median preoptic nucleus (MnPO) = integrates signals from SFO & OVLT
also receives signals from baroreceptors in heart arteries: increased pressure in arteries from liquid → signal MnPO
or
via kidney signals:
Angiotensin II = hormone released by kidneys → stimulates SFO & OVLT receptors in brain via cerebral fluid to notify a drop in blood volume
takes 10-20 min for brain to realize the deficit is gone & to stop sending stimulatory signals → may over drink
note: act of drinking tells brain we’re satisfying the need FASTER than an injection
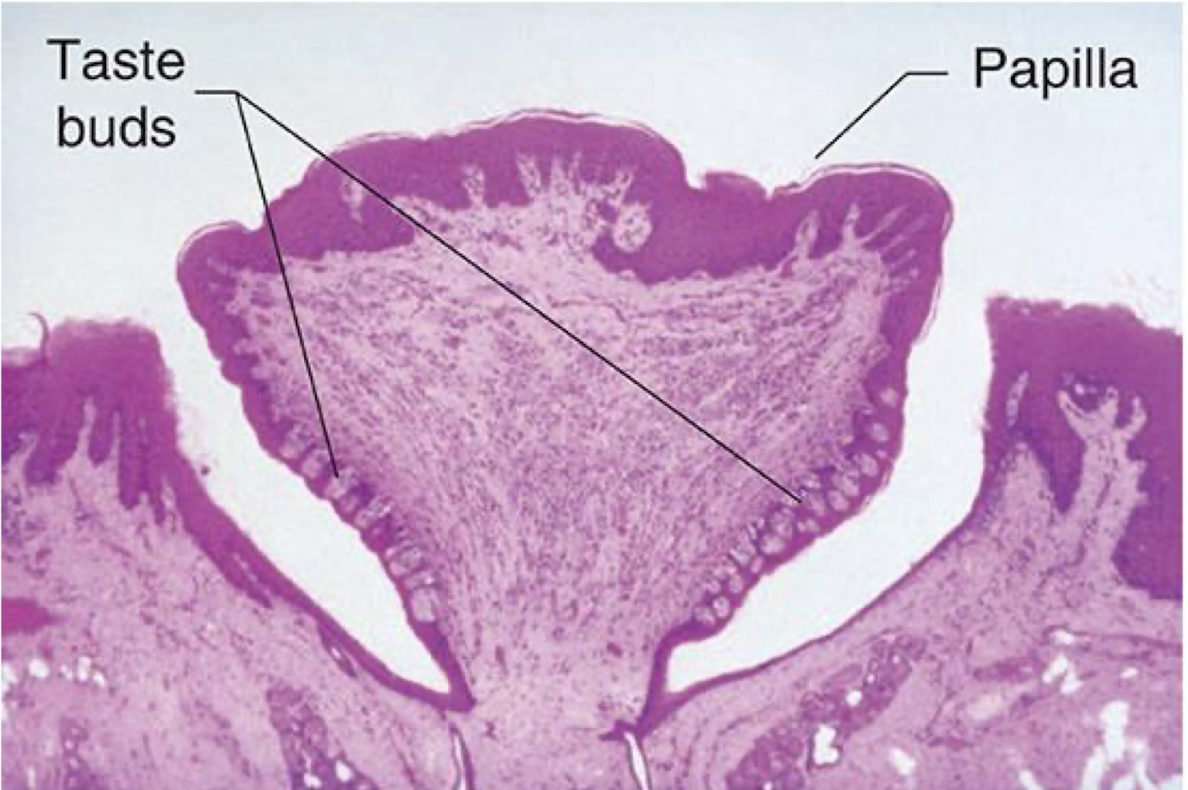
Drive Theory: 3. Hunger - role of taste
food selection varies depending on digestive tracts (ex. humans are omnivores)
taste primaries: sour, sweet, bitter, salty, umami
→ taste is used to detect what type of nutrients are in the good
balanced meals activate all 5 taste receptors (on sides of papilla)
diff taste cells have diff receptors
diff neurons in brain are specialized for diff tastes + they’re in multiple areas
Drive Theory: 3. Hunger - sensory-specific satiety
Sensory-specific satiety = the more u eat a food item, the less appealing it becomes
innate
BUT, if well balanced, this is less likely to occur
Learned taste aversion = avoid foods associated with illness or poor nutrition
not innate (based on experience & familiarity)
Learned taste preference = preference for flavour of food, instead of the nutrients in it
not innate (based on experience & familiarity)
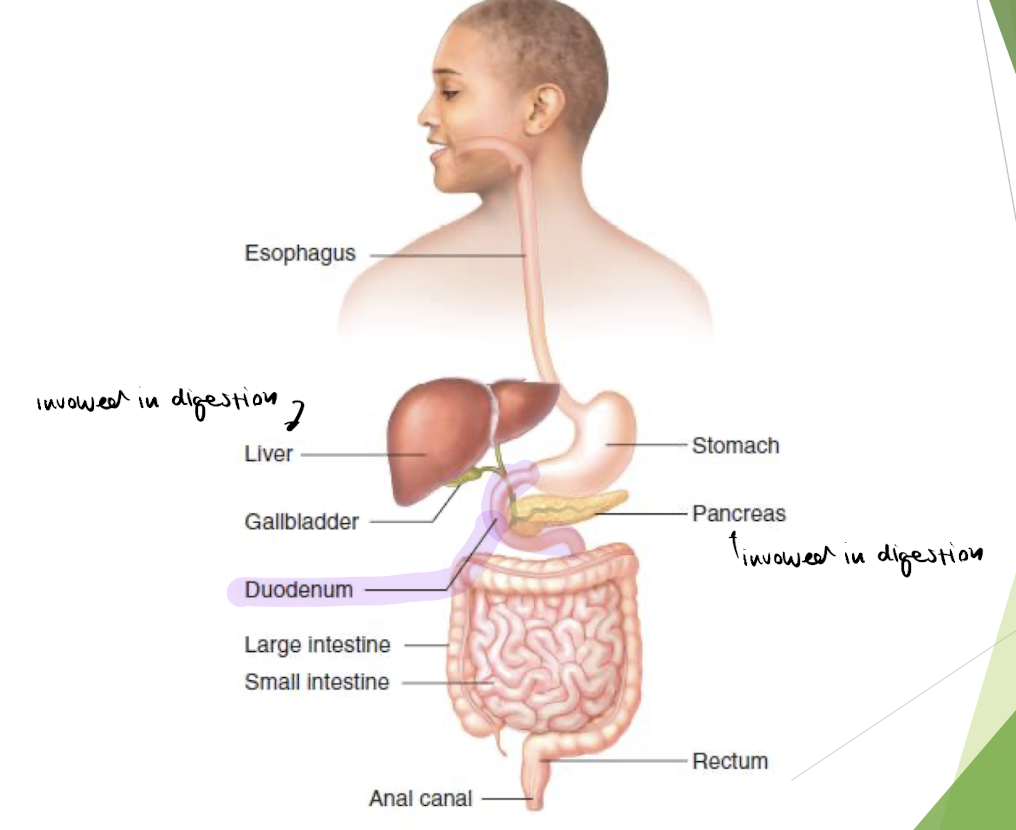
Drive Theory: 3. Hunger - digestive process (basics)
Area postrema = region in brain (outside the blood-brain barrier to detect directly) that induces vomiting if activated by toxins
ex. throw up bad shrimp
Duodenum = small intestine where most digestion & absorption occurs
Drive Theory: 3. Hunger - digestive process
glucose: from carb digestion → for energy
AA: from protein digestion
fatty acids: from fat digestion in intestine
glycerol: from fat digestion in liver
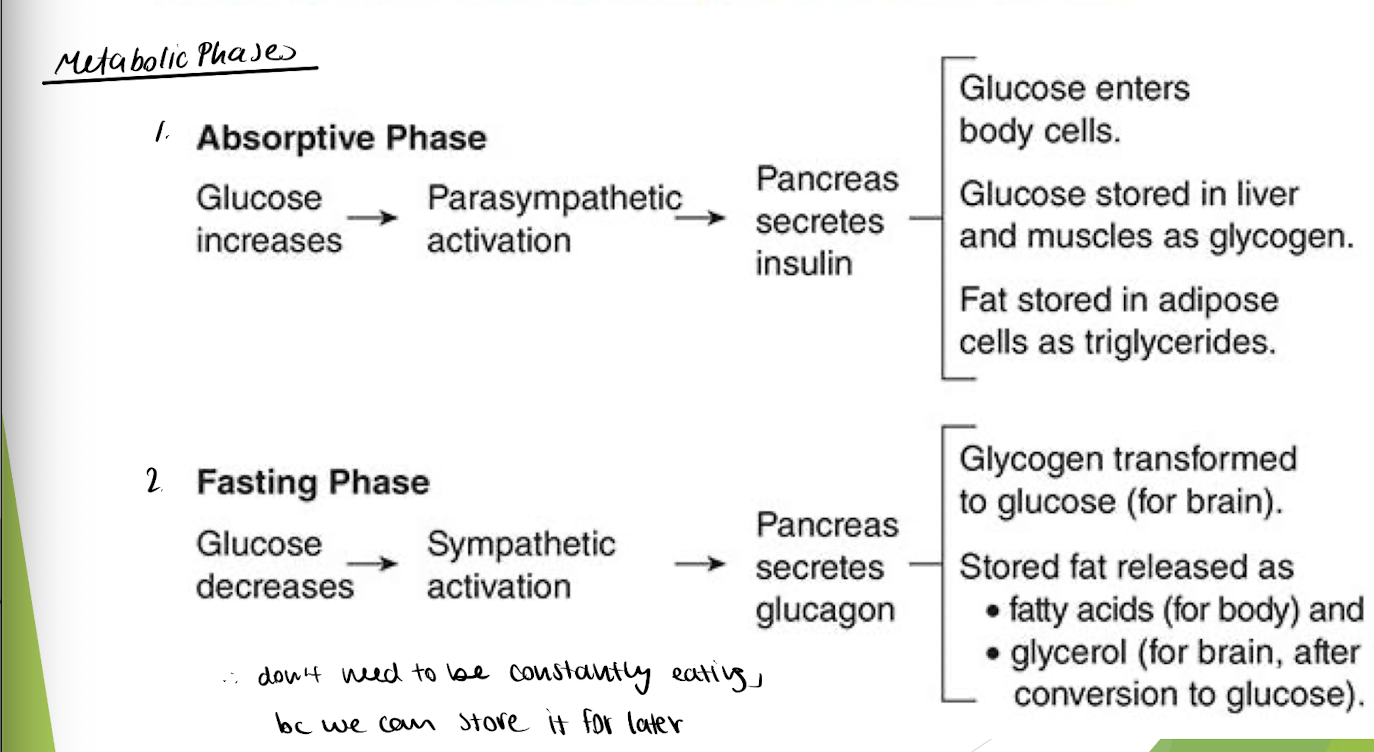
→ digestive process is controlled by autonomic NS (2 metabolic phases)
Absorptive Phase = few hrs after meal + living off nutrients arriving from digestion
Fasting Phase = drop in blood glucose → body lives off energy stores
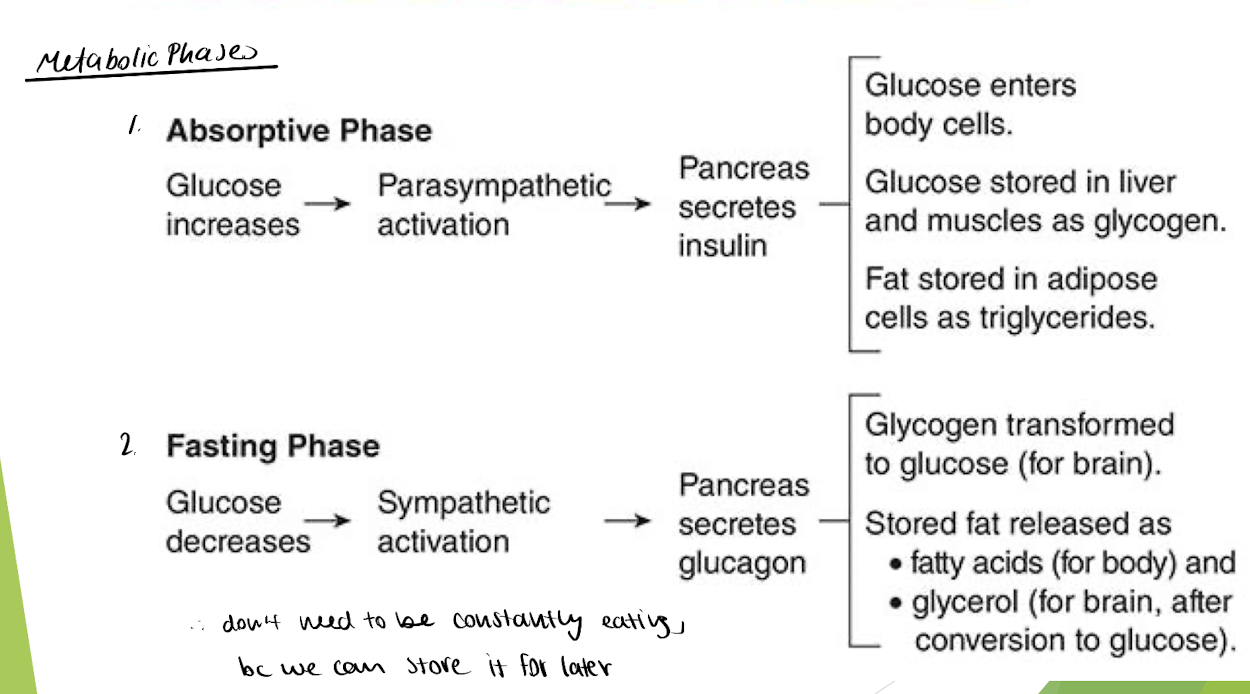
Drive Theory: 3. Hunger - Absorptive Phase
absorptive phase = few hrs after meal + live off of nutrients from digestion
focus on glucose
→ insulin allows body cells to take up glucose from blood + store glucose in muscle/fat cells
during parasympathetic activation (to digest)

affected by: Diabetes
Type 1 = pancreas cant produce enough insulin (WBCs killed the beta islet cells)
Type 2 = tissues are relatively unresponsive to insulin (not enough insulin receptors) → dont take in glucose
→ thus, glucose remains in blood & cells dont get enough sugar
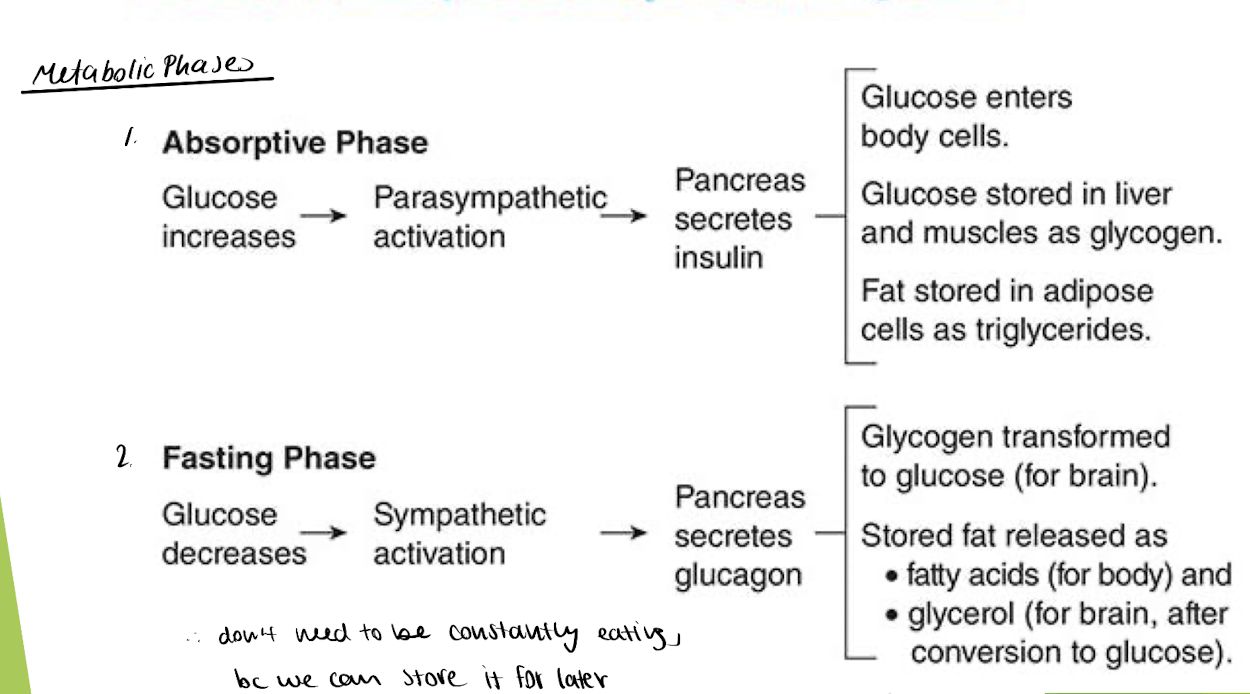
Drive Theory: 3. Hunger - Fasting Phase
fasting phase = glucose levels drop in blood → body uses energy stores
why we don’t need to be constantly eating
→ pancreas secretes glucagon → causes muscle/fat cells to turn glycogen into glucose
during sympathetic activation (need energy)

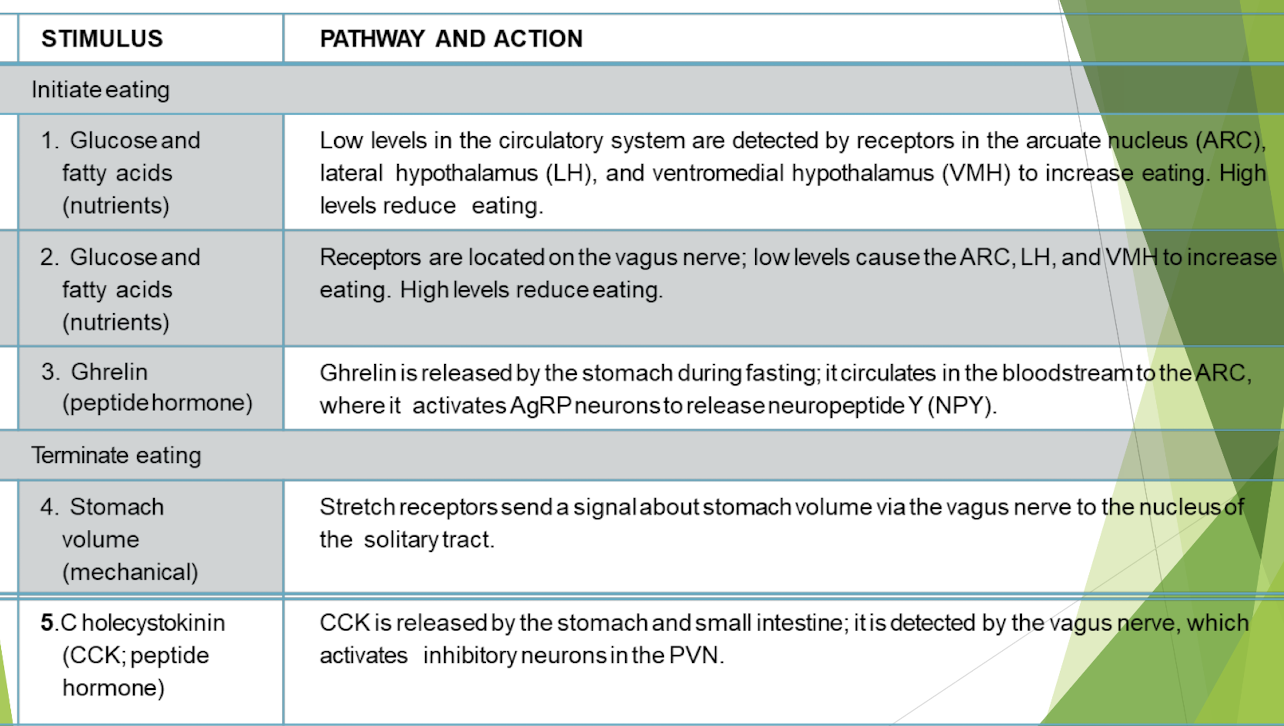
Drive Theory: 3. Hunger - Regulating Hunger
Ghrelin = orexigenic peptide hormone that increases eating by signalling orexin to activate ARC (via AgRP neurons)
synthesized & released from stomach when it has room, NOT just when hungry
released fast
Orexin = neuropeptide that increases eating & wakefulness when starving
→ excites ARC
Arcuate Nucleus (ARC) = hypothalamic center for food intake control
NPY/AgRP neurons : increase hunger by activating ARC
POMC neurons : decrease hunger by deactivating ARC
→ sends signals to lateral hypothalamus
Paraventricular nucleus (PVN) = regulates amount of eating & metabolic processes (body temp…)
signalled by ARC neurons
Lateral Hypothalamus = initiates eating + controls feeding behaviour & metabolic responses (controls chewing, swallowing, insulin production, amount of gastric juices)
Ventromedial hypothalamus (VMH) = produces satiety & increases metabolism
POMC neurons (decrease hunger) deactivate ARC → increases VMH activity → stop eating
Cholecystokinin (CCK) = hormone that signals satiety when food passes thru duodenum
limits meal size + aids digestion ] provides satiation after a snack
higher CCK DOESNT help w weight loss, bc they just eat more small meals
note: smaller meals allow us to absorb more nutrients
![<p><strong>Ghrelin </strong>= orexigenic peptide hormone that <span style="color: rgb(151, 236, 226);">increases eating by signalling orexin to activate ARC </span>(via AgRP neurons)</p><ul><li><p><em>synthesized & released from stomach when it has room, NOT just when hungry</em></p><ul><li><p><em>released fast</em></p></li></ul></li></ul><p></p><p><strong>Orexin</strong> = neuropeptide that<span style="color: rgb(171, 236, 226);"> increases eating & wakefulness when starving</span></p><p>→ excites ARC</p><p></p><p>Arcuate Nucleus (<strong>ARC</strong>) = hypothalamic center for<span style="color: rgb(152, 242, 241);"> food intake control</span></p><ul><li><p>NPY/AgRP neurons :<span style="color: rgb(162, 239, 234);"> increase hunger</span> by activating ARC</p></li><li><p>POMC neurons : <span style="color: rgb(173, 239, 234);">decrease hunger </span>by deactivating ARC</p></li></ul><p>→ sends signals to lateral hypothalamus</p><p></p><p>Paraventricular nucleus (<strong>PVN</strong>) = <span style="color: rgb(181, 241, 221);">regulates amount of eati</span><span style="color: rgb(184, 243, 223);">ng</span> & metabolic processes (body temp…)</p><ul><li><p>signalled by ARC neurons</p></li></ul><p></p><p><strong>Lateral Hypothalamus</strong> =<span style="color: rgb(175, 239, 231);"> initiates eating + controls feeding behaviou</span>r & metabolic responses <em>(controls chewing, swallowing, insulin production, amount of gastric juices)</em></p><p></p><p>Ventromedial hypothalamus (<strong>VMH</strong>) = <span style="color: rgb(165, 239, 219);">produces satiety & increases metabolism</span></p><ul><li><p>POMC neurons (decrease hunger) deactivate ARC → increases VMH activity → stop eating</p></li></ul><p></p><p>Cholecystokinin (<strong>CCK</strong>) = hormone that signals satiety when food passes thru duodenum</p><ul><li><p>limits meal size + aids digestion ] <span style="color: rgb(150, 238, 230);">provides satiation after a snack</span></p><ul><li><p>higher CCK DOESNT help w weight loss, bc they just eat more small meals</p></li></ul></li></ul><p></p><p><em>note: smaller meals allow us to absorb more nutrients</em></p><p></p>](https://assets.knowt.com/user-attachments/b8e96f15-3a82-452e-8a8f-14cb37dbc47a.png)
Drive Theory: 3. Hunger - Long-term Regulation of Hunger
PYY = hormone released by intestines → suppresses appetite for LONG period (inhibits NPY release)
long-term satiation, BUT DOESNT decrease the total amount of food u eat
Leptin = hormone secreted by fat cells already full of fat → INHIBITS NPY release → STOPS eating
reduces meal size & total daily intake !!
opposite of ghrelin
→ sent to deactivate ARC via POMC neurons
Drive Theory: 3. Hunger - Summary
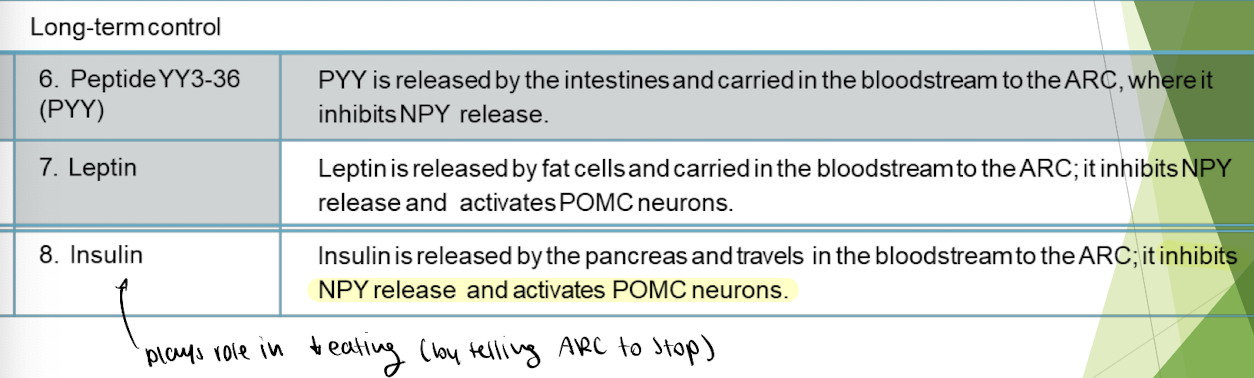
role of insulin
allows uptake of glucose into cells from bloodstream
activates POMC neurons → deactivate ARC → INHIBITS NPY release → decreases eating
Obesity
malnourished DOESNT equal underfed, it means NOT enough nutrients
use: BMI = weight in kg / height in meters
a qualifier of obesity or leanness
info:
a global epidemic bc obese ppl exceed the # not overweight
increased health risks (correlated)
ex. increased risk of Alzheimers
CANT be characterized by lack of impulse control, inability to delay gratification, or maladaptive eating style
no obesity or diabetes gene in humans
found in mice tho (db - chromosome 4) & (ob - chromosome 6)
has multiple genetic factors
epigenetic factors like methylation have been LINKED to obesity
cause: smoking, pollution, stress
ex. Holland kids were methylated by environmental stressor → became fat
Obesity & dieting
Basal metabolism = energy required (set point) for body survival
metab will increase/decrease to defend a set point weight
increase quicker after gaining weight
accounts for 75% of body energy usage - remainder is split b/w digestion & physical activity
→ dieting eats less than basal metabolism
10% weight reduction is more practical + less risk of chronic disease
standard treatment: dietary restriction
serotonin could play a role in weight control:
eating carbs raises serotonin, but for those that crave carbs, serotonin inhibits ur desire for carbs → THUS, SSRIs lower carb eating
psych therapeutic approaches: treat out-of-control eating as addictive behaviour
surgery: gastric bypass (limits meal size by removing stomach cells that release ghrelin) → cant eat as much + feel less hungry
Anorexia Nervosa
= restrict food intake to maintain unhealthy weight
equal prevalence b/w sexes
most recover (1/3 in 9yrs, 1/3 in 22yrs )
body dysmorphia
types:
restrictor : reduce food intake
binge purgor : restrict food intake & PURGE
results:
changes in brain structure
dysfunction in areas for reward system & body image
decreased grey matter - only partially recovers
loss of ovulation, decrease muscle mass
HIGHEST mortality rate of ALL psych disorders
Bulimia Nervosa
= binging & purging to control weight
can have no weight loss or increase in weight
have higher ghrelin levels b/w meals (tells them they’re hungry)
lower PYY levels → less long-term satiation
higher relapses than anorexia
body dysmophria
Binge-eating disorder
= recently eat large amounts of food in short period
feels uncontrollable
feel disgust/shame after → try to hide it
Anorexia, Bulimia, Binge Eating
bulimia is more heritable than anorexia
anorexia & bulimia may have social environmental causes + genetic links
decreased reward system
eating disorders are usually comorbid w other psych disorders (depression, anxiety, OCD)
serotonin may play a role