Physiology and Therapeutics of Calcium Balance
1/134
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
135 Terms
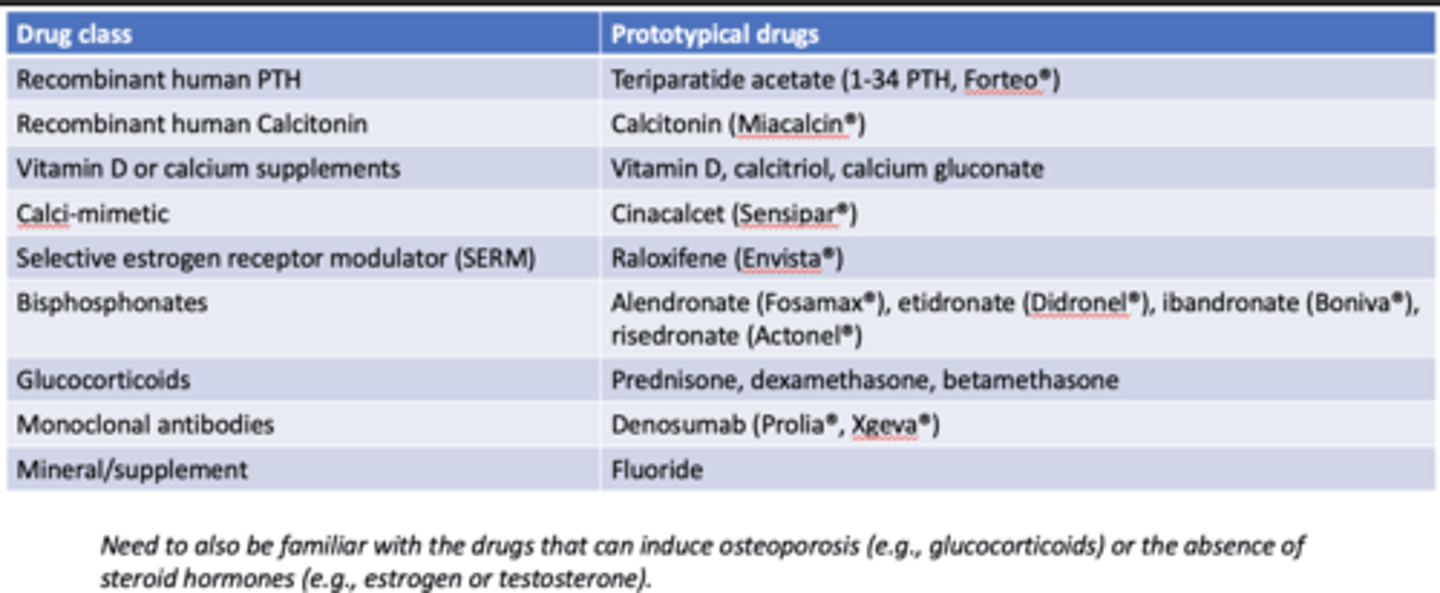
something that acts as an agonist at certain tissues and as an antagonist at other tissues
What is a modulator?
drug list:
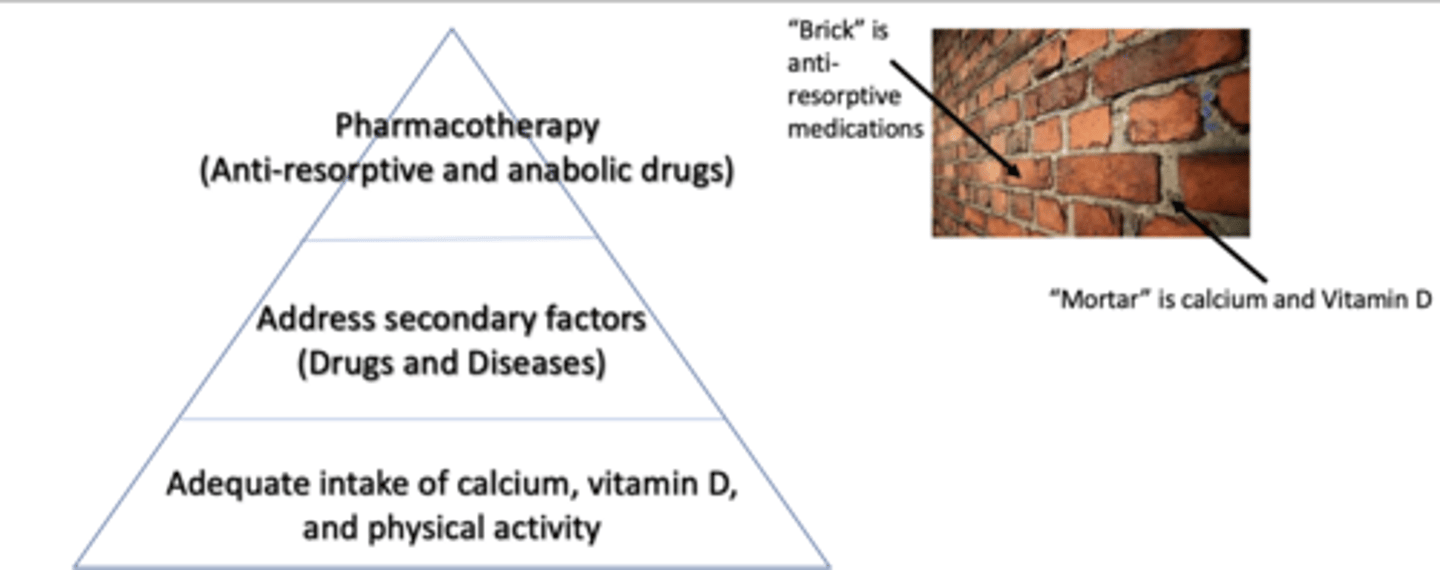
ensure there is adequate intake of Ca2+, vitamin D, and physical activity
When considering therapeutics for Ca2+ balance, what should be considered 1st?
address secondary factors (drugs and diseases)
When considering therapeutics for Ca2+ balance, what should be considered 2nd?
pharmacotherapy (anti-resorptive and anabolic drugs)
When considering therapeutics for Ca2+ balance, what should be considered 3rd?
steps for addressing considerations of therapeutics for Ca2+ balance:
-primary osteoporosis
-secondary osteoporosis
What are the 2 main types of osteoporosis?
*post-menopausal osteoporosis (type I)
*senile osteoporosis (type II)
What are the 2 main types of primary osteoporosis?
bone loss accelerates due to loss of estrogen sex hormones
What is the basis of post-menopausal osteoporosis (type I)?
metabolic processes and the ability to build bone decrease throughout aging
What is the basis of senile osteoporosis (type II)?
*excessive or high thyroid replacement therapy
*glucocorticoid drugs
*anticoagulants
*chronic lithium therapy
*chemotherapy (breast cancer or lymphoma)
*gonadotropin-releasing hormone agonists or antagonists
*anticonvulsants
*chronic phosphate-binding antacid use
*extended tetracycline use (chelation of Ca2+)
*diuretics producing calciuria (Ca2+ excretion)
*phenothiazine derivatives
*cyclosporin A, tacrolimus, methotrexate
What are 12 examples of secondary osteoporosis or drugs that are associated with osteoporotic syndromes?
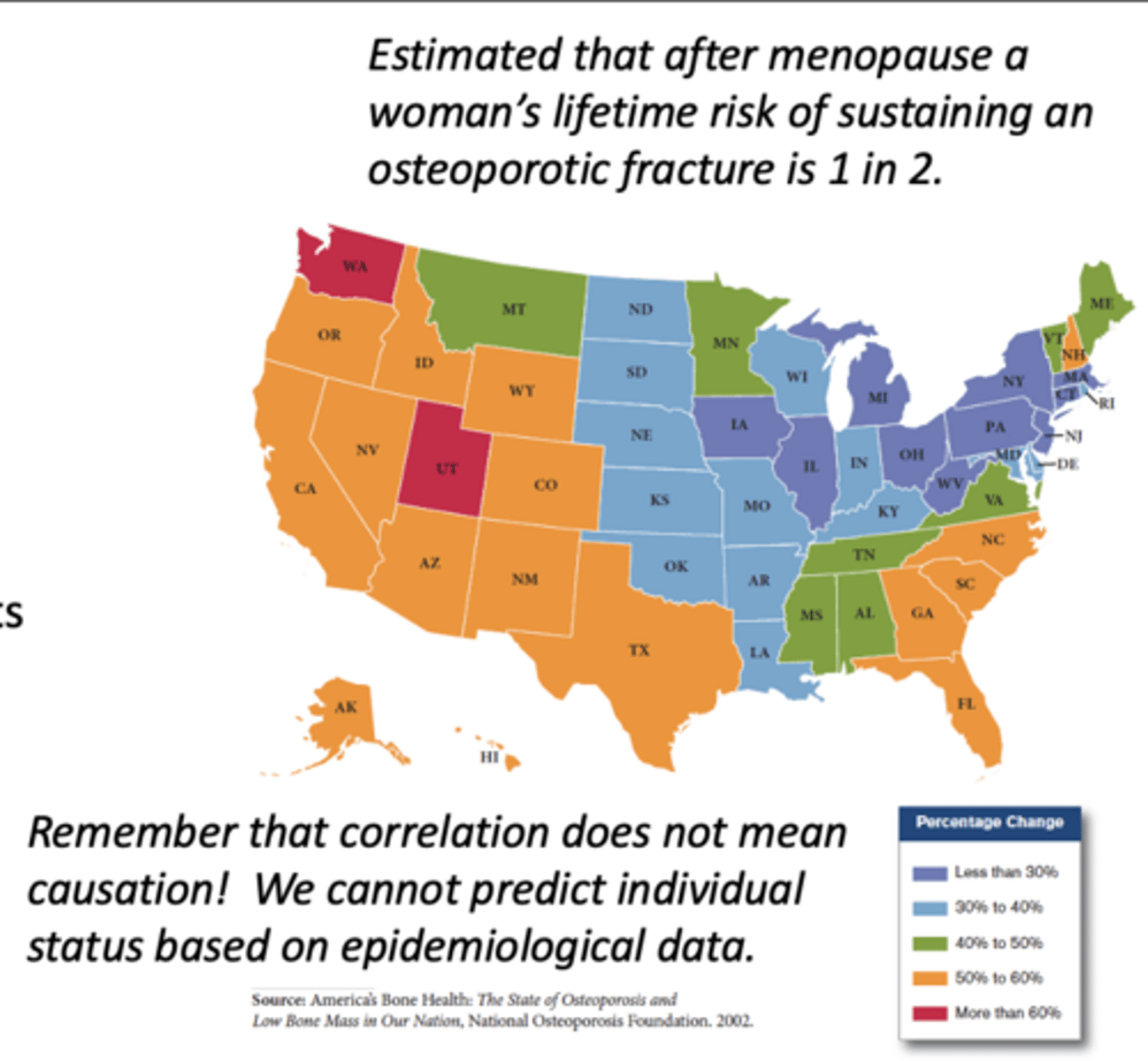
prevalence of osteoporosis:
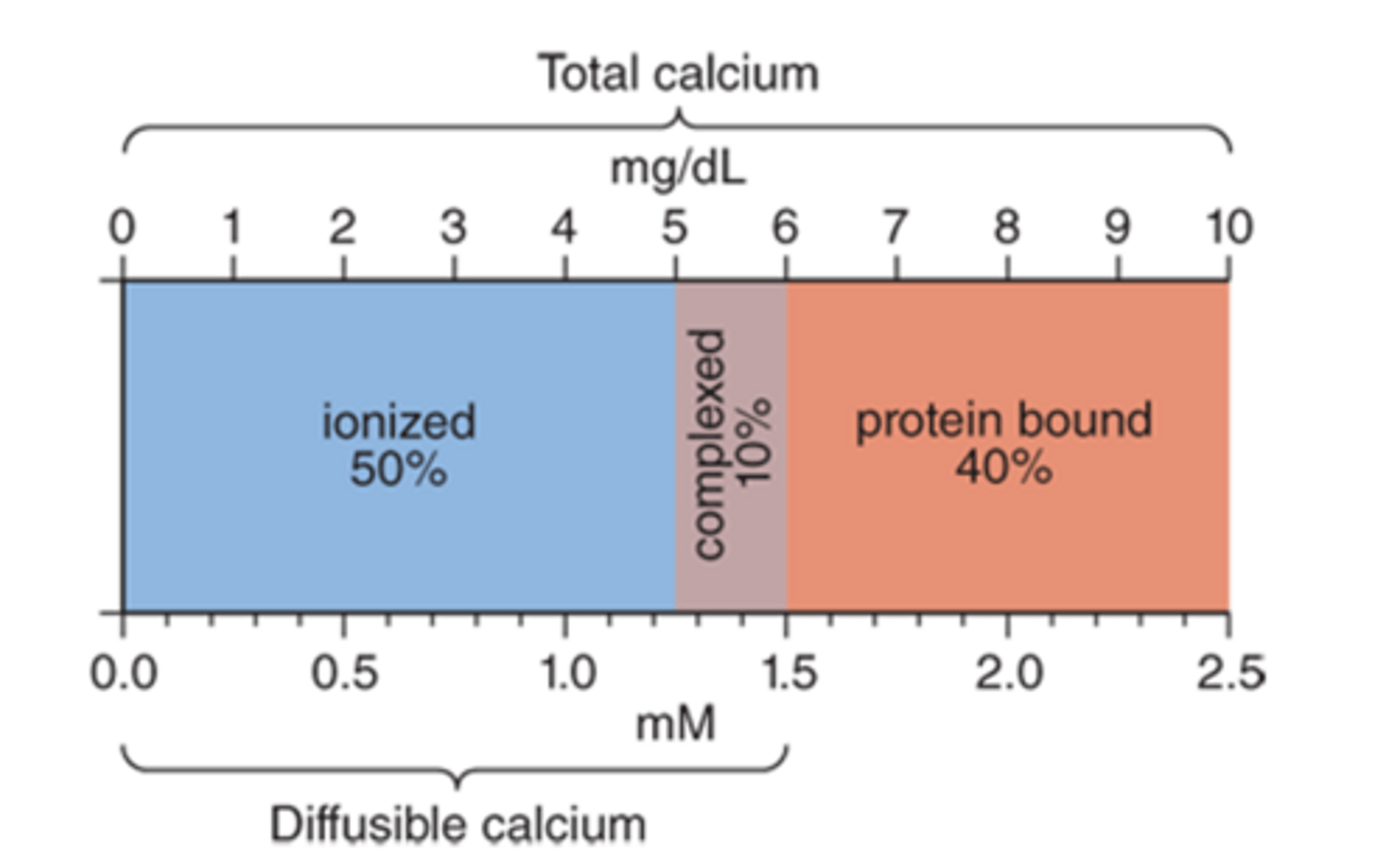
divided into 3 pools;
*ionized form (Ca2+) (largest amount)
*protein-bound (albumin-bound)
*complexed with anions, such as phosphate and citrate (smallest amount)
How is the total calcium level divided in the body, and explain?
body pH and concentrations of calcium and anions
What does the degree of complexed calcium depend on?
an intracellular Ca2+-binding protein that assists with cell signaling
What is calmodulin?
the quantity of phosphorus in the diet is similar to that of calcium
How does the quantity of phosphorus in the diet compare to that of calcium?
balances intestinal absorption
What does renal excretion of calcium and phosphate do to intestinal absorption in the steady state?
disruption of bone mineral homeostasis
What can dysfunction of the intestine or kidney lead to?
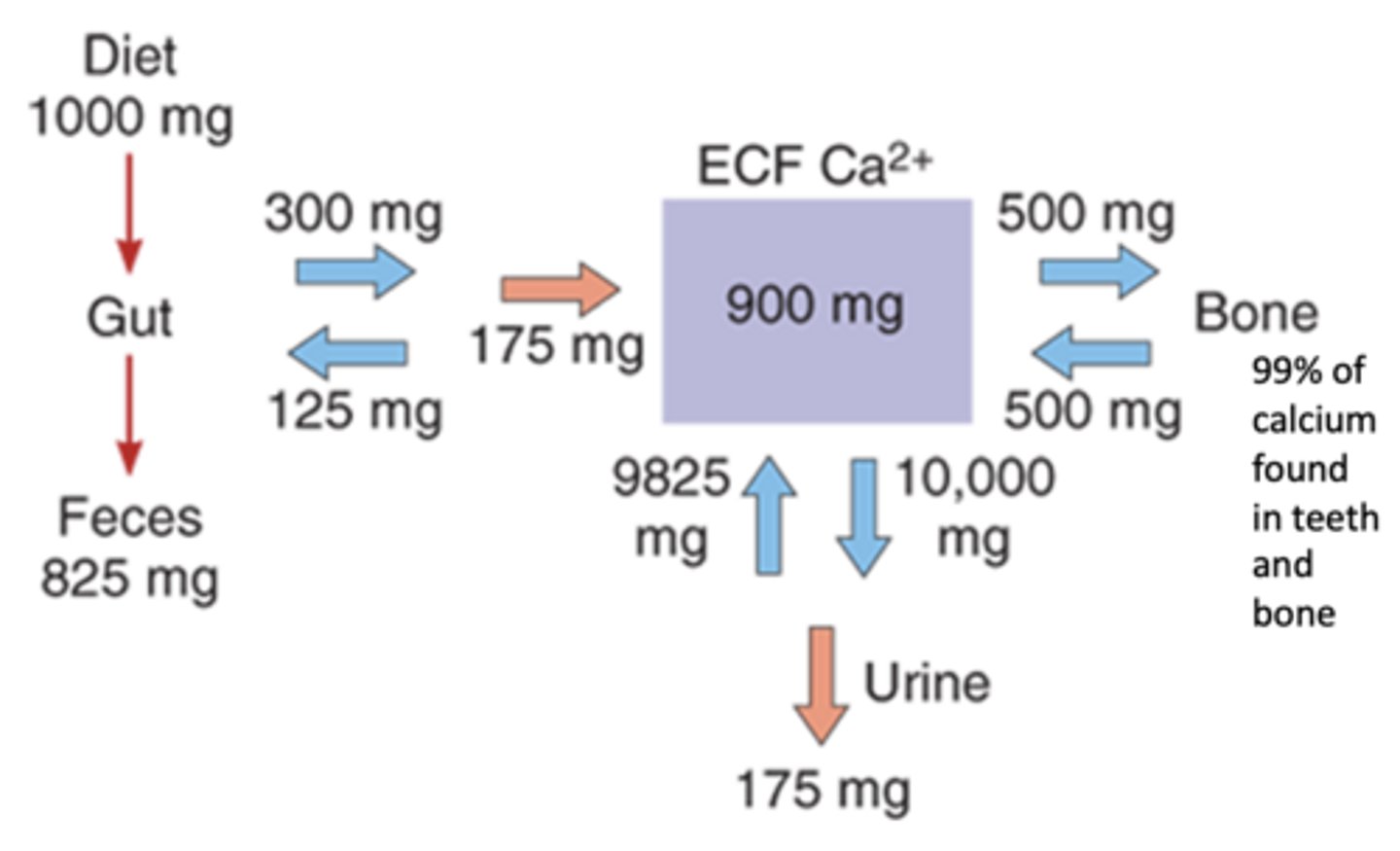
intestines (feces)
Is more Ca2+ lost via the kidneys (urine) or intestines (feces)?
note the 99% of Ca2+ found in teeth and bone:
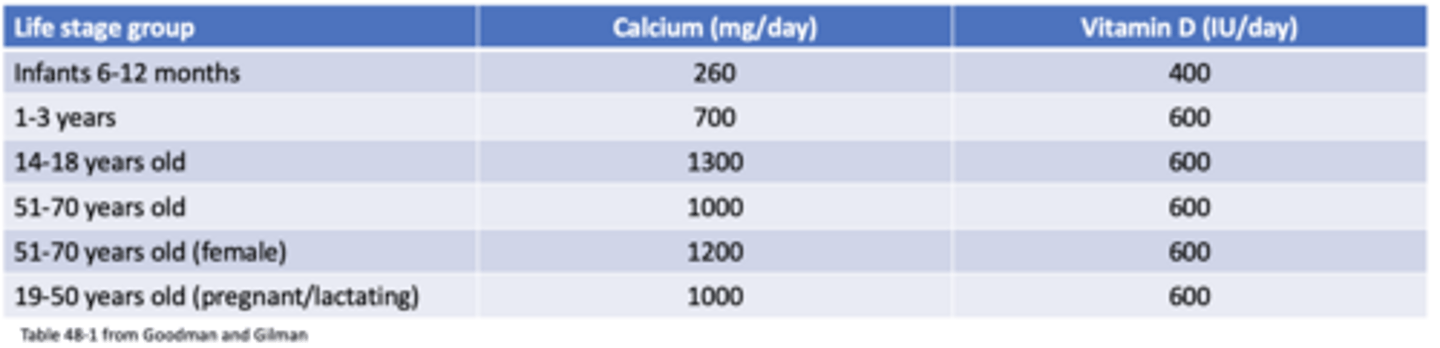
requirements change depending on a person's age, pregnancy, and lactation status
What is the recommended daily allowance of calcium and Vitamin D like?
-cheese
-yogurt
-milk
-sardines
-dark leafy greens (spinach, kale)
-soybeans
What are examples of foods with high calcium?
-fish (tuna, salmon)
-beef liver
-cheese
-egg yolks
What are examples of foods with high vitamin D?
recommended daily allowance of calcium and Vitamin D:
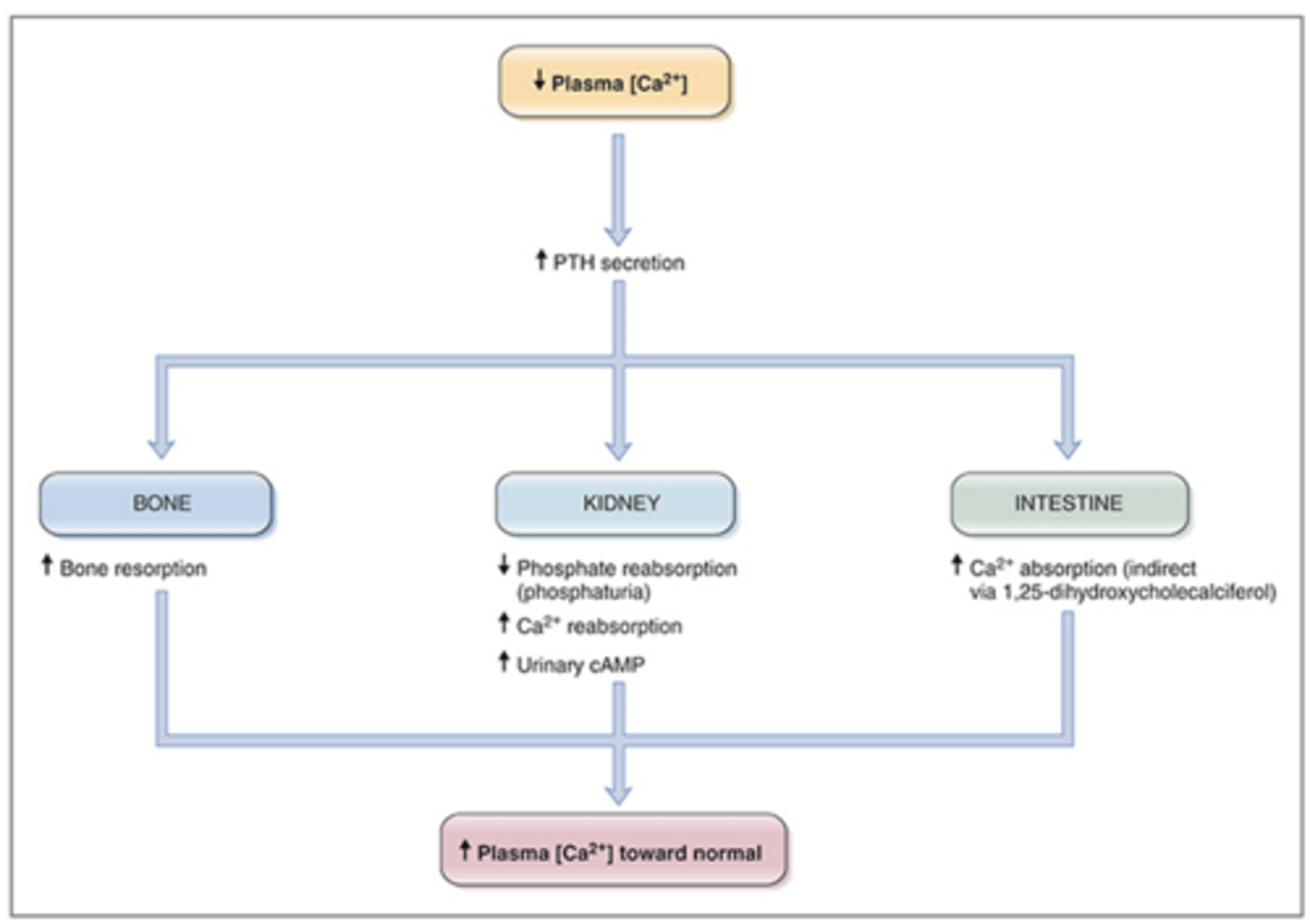
a polypeptide that increases serum calcium levels -> through bone resorption, decreased renal calcium excretion, and increased calcitriol synthesis
What is parathyroid hormone (PTH), and explain?
T1/2 = 4 minutes -> is primarily cleared by the liver and kidney
What is the half-life and clearance of PTH like?
PTH maintains constant concentration of calcium and phosphate in extracellular fluid.
PTH maintains constant concentration of ______ and ______ in extracellular fluid.
intermittent or pulsatile
What type of PTH exposure can promote bone formation?
when plasma Ca2+ levels fall below normal, PTH is released to increase plasma Ca2+ -> an example of a negative feedback pathway:
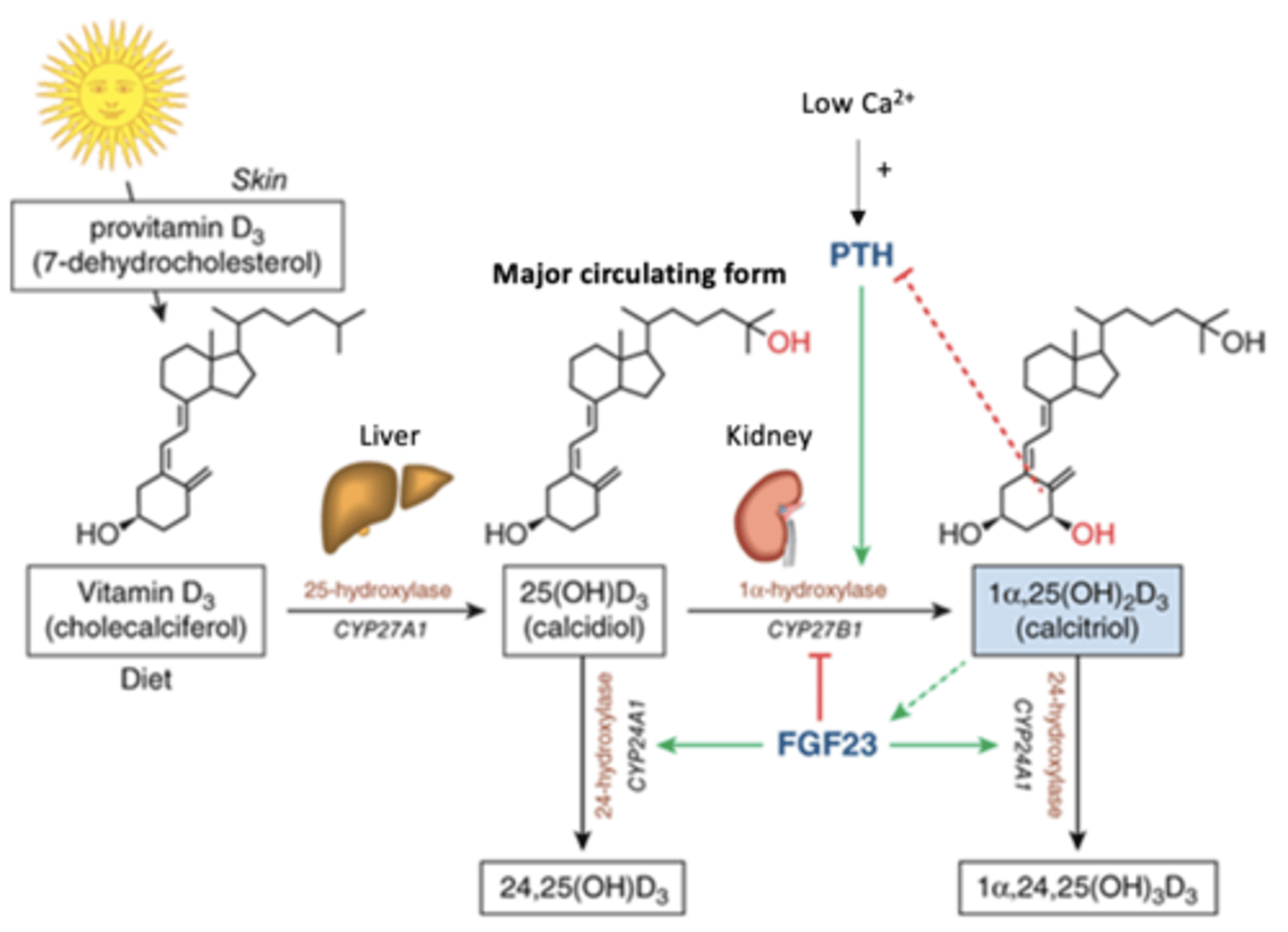
multiple enzymatic steps in the skin, liver, and kidneys
Generally, what is required for the production of 1,25-dihydroxy vitamin D3 (calcitriol)?
cholesterol
What is the precursor to 1,25-dihydroxy vitamin D3 (calcitriol)?
requires two successive hydroxylation (-OH) reactions
What must happen to the cholesterol precursor to form 1,25-dihydroxy vitamin D3 (calcitriol)?
-stimulates bone formation
-increases Ca2+ and PO4 absorption in the small intestine
-decreases excretion of Ca2+ and PO4
What are 3 main physiological effects of calcitriol?
by vitamin D-binding globulin
How is calcitriol carried in the body?
1⍺-hydroxylase in the kidney -> to promote calcitriol formation
What will be stimulated by a dietary deficiency of vitamin D, Ca2+, or PO4, and explain?
calcitriol will be deactivated through 24-hydroxylase
What will happen to calcitriol if Ca2+ levels are high?
can increase calcitriol synthesis in the renal proximal cells
How can parathyroid hormone (PTH), low phosphate levels, and low calcium affect calcitriol?
produced in response to PTH, it blocks the formation of 1⍺-hydroxylase in the kidney and promotes the formation of 24-hydroxylase to block absorption of PO4 and increase its secretion
What is the function of FGF23?
production of 1,25-dihydroxy vitamin D3 (calcitriol) requires multiple enzymatic steps in the skin, liver, and kidneys:
can lead to significant bone loss called renal osteodystrophy
How can chronic kidney disease (CKD) affect the bones?
-vitamin D deficiency
-hyperparathyroidism
What are 2 effects of renal failure or CKD that lead to the development of renal osteodystrophy?
must be careful with the administration of drugs to these patients -> due to renal deficiency
What should clinicians be careful of when it comes to treating patients with renal osteodystrophy due to CKD, and explain?
-vitamin D analog (Calcitriol, Eldecalcitol)
-cinacalcet
-denosumab
What are the 3 main treatments for renal osteodystrophy due to CKD?
eldecalcitol has 2.7-fold greater affinity than calcitriol, but eldecalcitol weakly inhibits PTH in comparison to calcitriol
How do calcitriol and eldecalcitol vitamin D analogs compare?
-secondary hyperparathyroidism
-hypocalcemia in patients undergoing chronic renal dialysis
-CKD
-osteoporosis (both primary and secondary)
-vitamin D deficiency or insufficiency (genetic or diet-related, ex: lipid malabsorption bc cholesterol-derived hormone)
What are the 5 main pharmacotherapeutic uses of calcitriol (eldecalcitol, given in Japan)?
topical form to treat mild to moderate plaque psoriasis
What is a unique administration form and use of calcitriol?
oral or IV; rapid absorption (because it's a lipid)
How can calcitriol be administered, besides topically, and what is its absorption like?
it can enter fetal circulation
What is important to note about the use of calcitriol in pregnant patients?
it is bound extensively to alpha-globulin vitamin D binding protein (>99%)
What happens to administered calcitriol in the blood?
metabolized by 24-hydroxylase (minor) and 23- and 26-hydroxylase activity in the kidneys (major)
What is the metabolism of calcitriol like?
calcitriol undergo enterohepatic recycling on bile salts (t1/2 = 5-8 hours) which increases the half-life
What is the significance of the liver to calcitriol?
-ectopic calcification
-cardiac arrhythmias
-HTN
-hypercalcemia (skeletal muscle fatigue)
What are the 4 main adverse effects of calcitriol?
a calci-mimetic
What type of drug is Cinalcet?
suppresses PTH secretion
What is the function of Cinacalcet, a calci-mimetic?
-for treatment of secondary hyperparathyroidism in patients with CKD who are on hemodialysis or peritoneal dialysis
-hypercalcemia in patients with parathyroid carcinoma (ex: desensitization)
What are the 2 main pharmacotherapeutic uses of Cinacalcet?
increases sensitivity of Ca2+-sensing receptors on thyroid follicular cells to activation by extracellular Ca2+, which will inhibit PTH secretion
What is the MOA of Cinacalcet?
rapid absorption
What is the absorption of Cinacalcet like?
binds largely to plasma proteins (93-97%)
What happens to Cinacalcet in the blood?
metabolized by CYP3A4, CYP2D6, and CYP1A2
What is the metabolism of Cinacalcet like?
patients with liver impairment (insufficiency/failure), due to its role in the metabolism of the drug
In what patients should Cinacalcet not be used, and explain?
-upset stomach
-vomiting
-weakness
-chest pain
What are the 4 main side effects of Cinacalcet?
suppresses bone resorption in patients with metastatic bone cancer
What does Denosumab (Prolia) do?
*post-menopausal women or men with a high risk of fracture
*women receiving adjuvant aromatase inhibitor therapy for breast cancer
*men receiving androgen deprivation therapy for nonmetastatic prostate cancer
What are the 3 main pharmacotherapeutic uses of Denosumab (Prolia)?
an IgG2 monoclonal antibody
What type of drug is Denosumab (Prolia)?
blocks RANKL from activating its receptor RANK on surface of osteoclasts, which blocks bone resorption and helps to increase bone mass and strength
What is the MOA of Denosumab (Prolia)?
given SubQ (injected!) -> half-life of 25-30 days
What is the route of administration of and half-life of Denosumab (Prolia) like?
-musculoskeletal pain
-hypercholesterolemia
-cystitis
-possible increased risk of infection
-hypersensitivity reactions
-pancreatitis has been reported in clinical trials
What are the 5 main adverse effects associated with Denosumab (Prolia)?
summary on calcitriol, cincalcet, and denosumab:
-bisphosphonates (MOSTLY!)
-calcitonin
-estrogen or testosterone
What are 3 treatments utilized to block osteoclast activity, such as in osteoporosis?
less likely -> because given in perimenopausal range, there is a risk of malignancy
What is the likelihood of using estrogen or testosterone to block osteoclast activity, such as in osteoporosis, and explain?
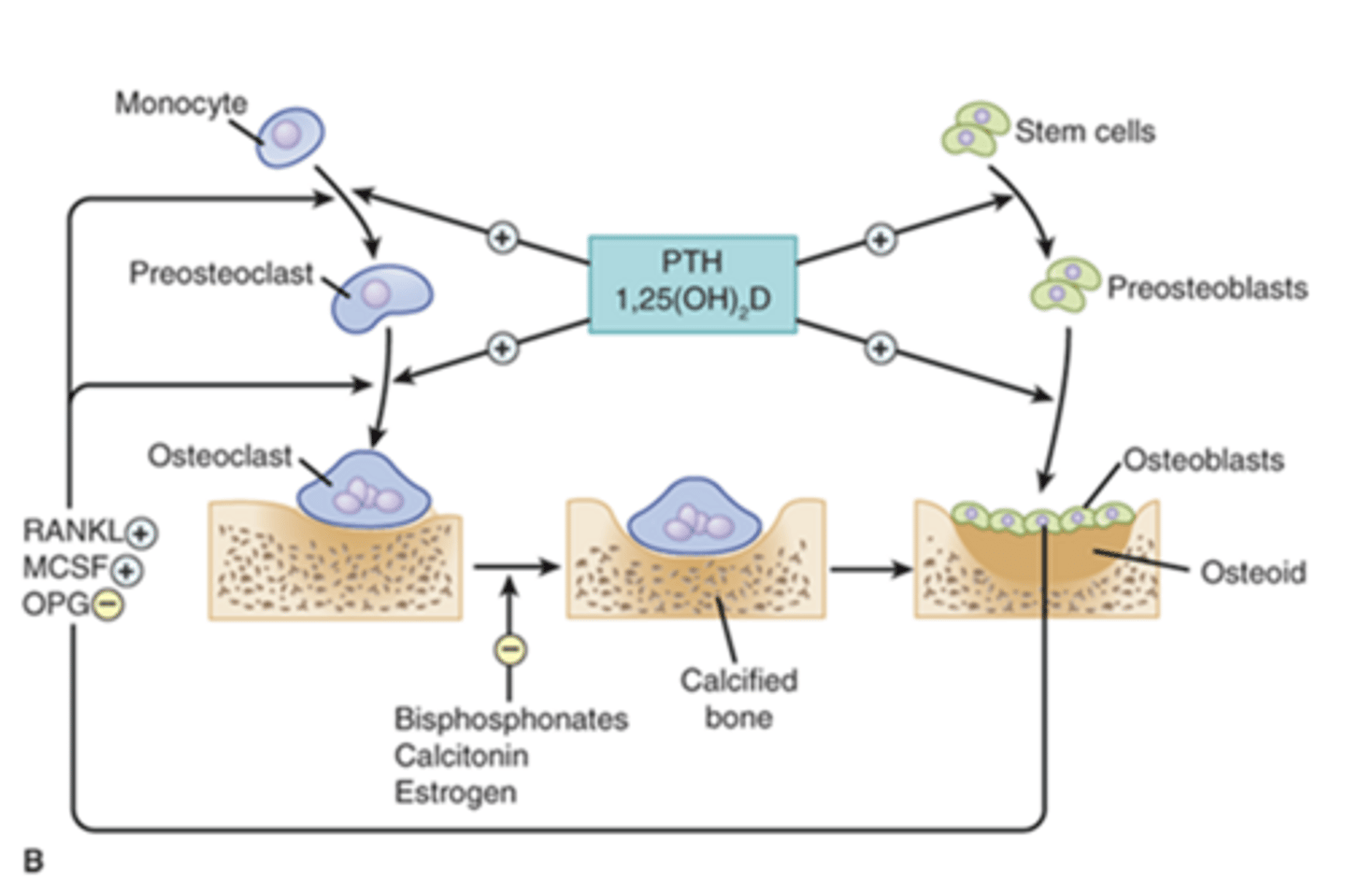
treatments utilized to block osteoclast activity:
glucocorticoid-induced osteoporosis
What is the most common form of secondary osteoporosis?
chronic use of glucocorticoids (ex: prednisone); can lead to osteoporosis and aseptic necrosis of the hip
What is the basis of glucocorticoid-induced osteoporosis, and explain?
dosages as small as 2.5 mg per day can significantly enhance osteoporosis
How does the dose of glucocorticoids used affect development of glucocorticoid-induced osteoporosis?
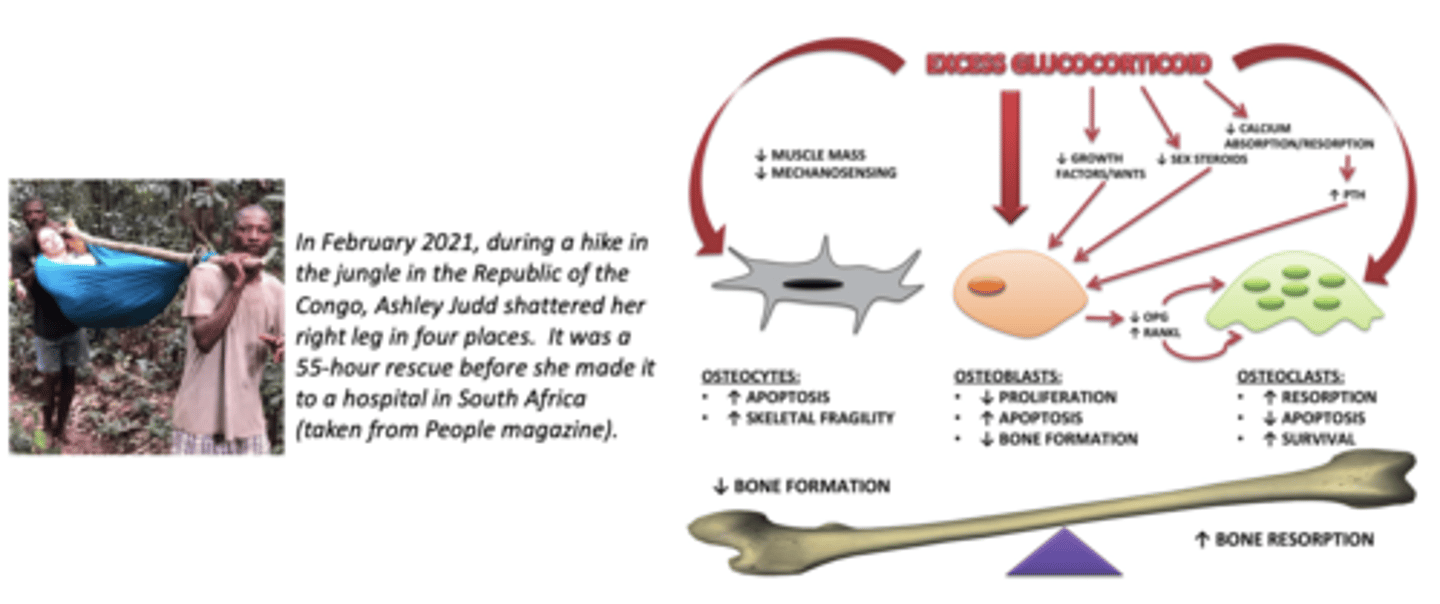
glucocorticoid-induced osteoporosis, note that Ashley Judd had a combo of chronic glucocorticoid use AND post-menopausal low estrogen = higher risk of osteoporosis, and need for regular bone mineral density monitoring:
affects 2-3% of population (>60 yo)
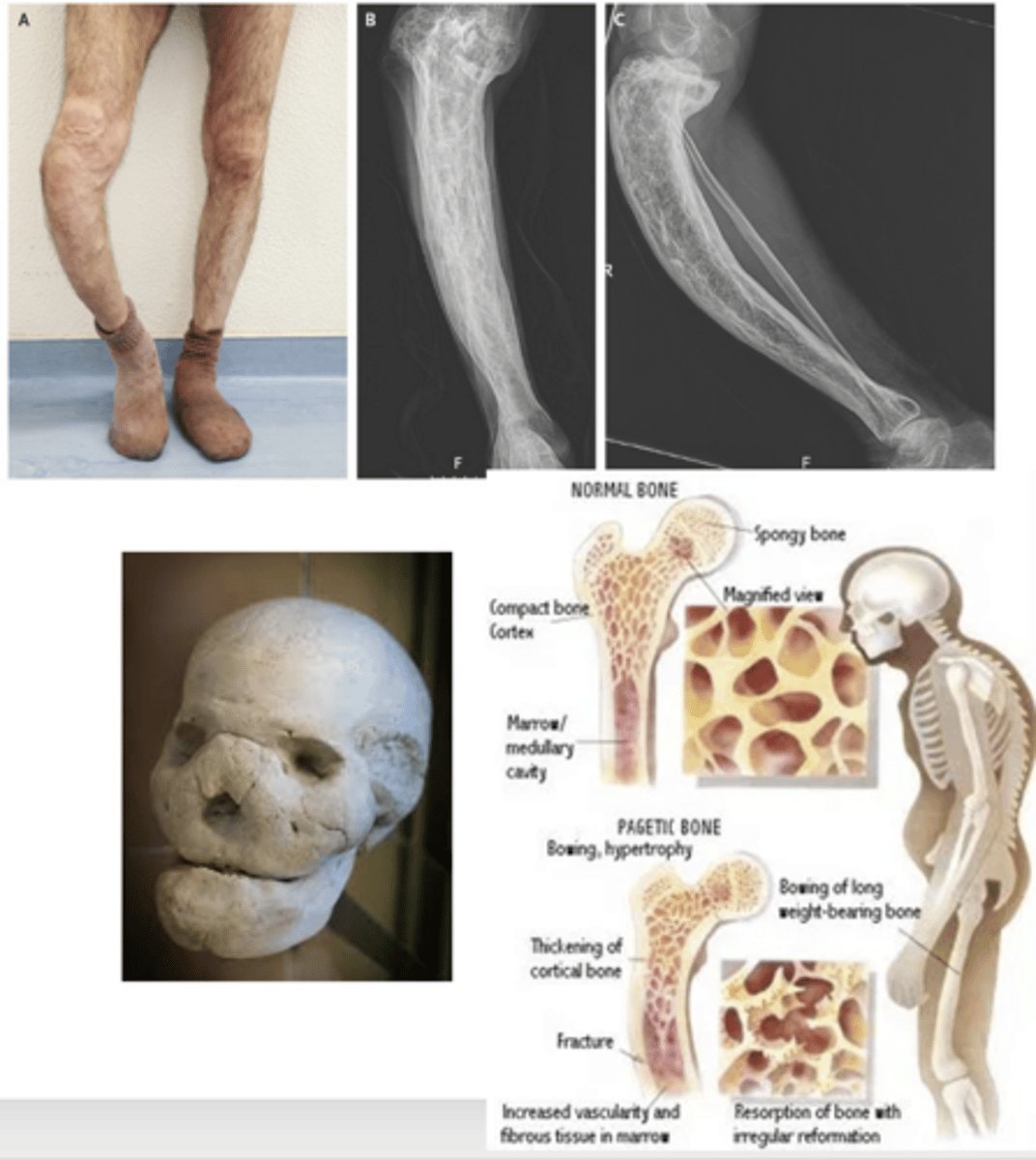
(first described by Sir James Paget in 1877)
What is the prevalence of Paget's disease (osteitis deformans)?
-genetic component (mostly!)
-environmental component
What are the 2 main components that lead to the development of Paget's disease (osteitis deformans)?
those diagnosed with Paget's disease should have relative screened
What precaution should be taken due to Paget's disease (osteitis deformans) having a genetic component?
increased bone resorption followed by exuberant/irregular bone formation -> leads to bone bowing, stress fractures, and arthritis of joints
What are the physiological changes that occur due to Paget's disease (osteitis deformans), and explain?
*deafness
*spinal cord compression
*nerve damage to the spinal nerves
*high-output cardiac failure
*pain
*headaches
*facial droop
*loose teeth
What are 8 secondary problems associated with Paget's disease (osteitis deformans)?
bisphosphonates or calcitonin, and NSAIDs are used for pain
What is the treatment for Paget's disease (osteitis deformans)?
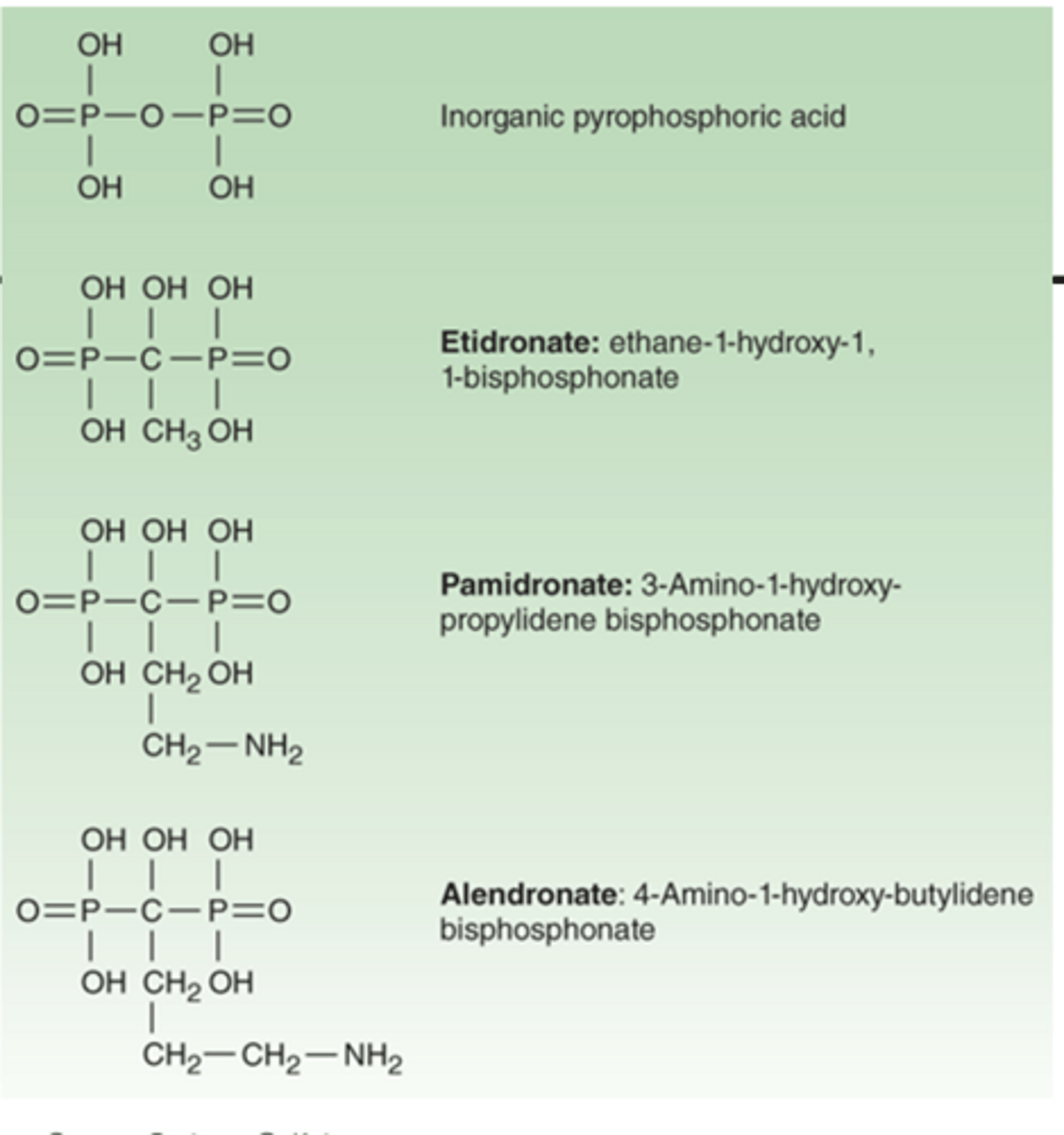
analogs of pyrophosphate in which P-O-P bond has been replaced by P-C-P bond
What are bisphosphonates?
P-O-P is the pyrophosphate bond normally found in bone, while P-C-P bond is harder to hydrolyze/break and can cause osteoclast death
What is the significance of the P-O-P bond being replaced by a P-C-P bond in bisphosphonates?
binds to hydroxyapatite crystals and reduces dissolution
How do bisphosphonates function?
-etidronate-
-alendronate
-ibandronate
-risedronate sodium or risedronic acid
-zoledronic acid
What are 5 common types of bisphosphonates?
osteomalacia -> by impairing new bone formation
What can etidronate lead to, and explain?
bisphosphonates:
a third-generation bisphosphonate
What is risedronic acid?
*osteoporosis in men and post-menopausal women
*Paget's disease
*glucocorticoid-induced osteoporosis
What are the 3 main pharmacotherapeutic uses of risedronic acid?
binds to bone hydroxyapatite and, when taken into osteoclasts, can cause the release of risedronic acid to induce apoptosis through inhibition of farnesyl pyrophosphate synthase
What is the MOA of risedronic acid?
resistant to chemical and enzymatic hydrolysis due to P-C-P linkage
What is the main pharmacokinetic feature of risedronic acid?
1x/year as an injection (long DOA) or orally 1x/day
How is risedronic acid administered?
-back pain
-arthralgia
-abdominal pain
-dyspepsia
-can increase esophagitis
What are the 5 main adverse effects of risedronic acid?
bisphosphonates should be taken on an empty stomach with a full glass of water and patient should remain upright for at least 30 minutes after taking a bisphosphonate
How can the increased risk of esophagitis from risedronic acid, and other bisphosphonates, be avoided?
may cause decrease in serum Ca2+ and PO4 -> milk or antacids can bind the drug and reduce its absorption
What may overdosing on risedronic acid cause, and explain?
"tones" down Ca2+ levels in the blood and opposes the function of PTH
What is the function of calcitonin?
in the parafollicular C cells of the thyroid gland
Where is calcitonin produced?
helps to protect the skeleton from "calcium stress"
What is the purpose of calcitonin decreasing levels of Ca2+ in the blood?
circulating levels are 10-15 pg/mL -> abnormally elevated levels of calcitonin are found in medullary thyroid carcinoma and C cell hyperplasia
What are the circulating levels of calcitonin like, and how does this change in disease?
can have tissue specific splice variants, katacalcin and calcitonin-gene related peptide (CGRP)
What is the basis of medullary thyroid carcinoma and C-cell hyperplasia like?