CM II Week 6 (Altered LOC/Syncope)
1/55
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
56 Terms
consciousness includes
–Arousal (wakefulness; brainstem reticular activating system)
–Awareness (content of consciousness; cerebral cortex)
confusion
disorientation, impaired attention, fluctuating awareness
lethargy
Drowsiness
Decreased alertness; arousable to voice
syncope
Transient loss of consciousness due to reduced blood flow to both cerebral hemispheres or the brainstem
stupor
Arousable only to vigorous or painful stimuli
coma
a sleep-like state with no purposeful response to internal or external stimuli, from which the patient cannot be aroused.
States of Consciousness
• normal consciousness
• confusion "clouding of the sensorium"
• drowsiness and stupor
• coma
Etiological Categories Of Altered LOC
•Structural
•Metabolic
•Toxicologic (drugs)
•Infectious (meningitis)
•Hypoxic/Ischemic
•Endocrine (hyper/hypoglycemic)
major causes of altered mental status (AEIOU TIPS)
•A --> Alcohol, Acidosis
•E --> Epilepsy, Electrolytes (Na**, K, Ca, Mg)
•I --> Insulin (hyperglycemia / hypoglycemic**)
•O --> Overdose, Opiates
•U --> Uremia
•T --> Trauma, Temperature
•I --> Infection
•P --> Psychiatric, Poisoning
•S --> Stroke, Seizures
Initial approach to Altered LOC... Primary Survey
•#1 ABCs!!
•Check glucose immediately
•Pulse ox
•IV access
•Cardiac monitoring
Altered LOC... Focused History
•Onset and progression
•Witness account
•Medications/Toxins (any SI?)
•Seizure Activity
•Trauma or fall
•Past neurologic history
Altered LOC... PE
•Vitals (fever, hypotension, low O2 sat, increased RR)
•Neuro Exam (esp. pupils, gaze deviation, motor asymmetry)
•Signs of trauma
•Signs of infection
Altered LOC... Diagnostic Studies
•Fingerstick glucose
•CBC with diff, CMP, ABG, Tox screen
•Non-contrast CT of head (check for hemorrhage)
•ECG
•EEG if seizure suspected
•+/- Lumbar Puncture if CNS infection suspected
Altered LOC... Management
•Secure airway if GCS < 8
•Give O2 if hypoxic (unless end stage COPD)
•Correct any metabolic conditions
•Treat infection if present
•Reverse toxins
•Consider Naloxone if opioid suspected
•Manage ICP
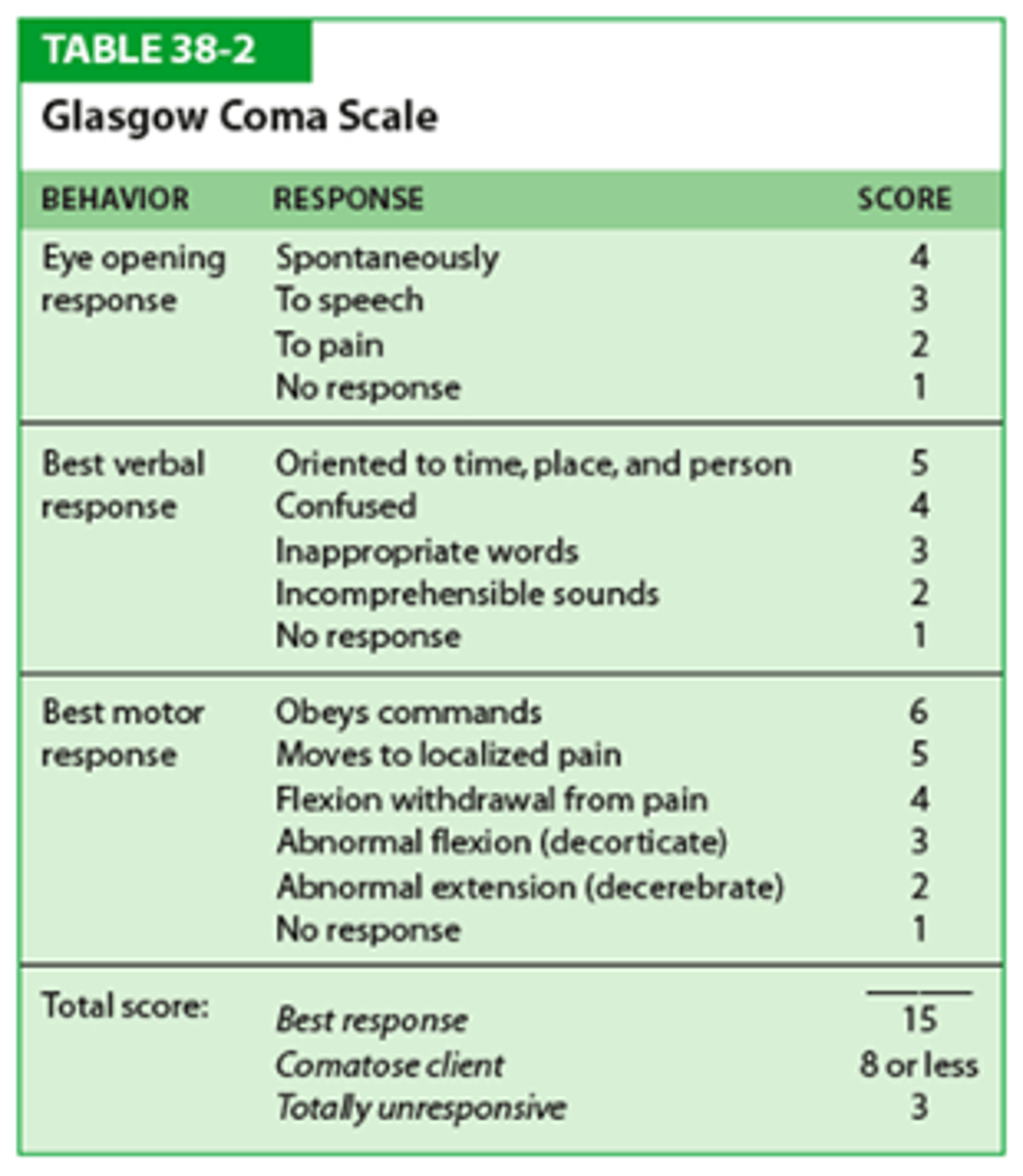
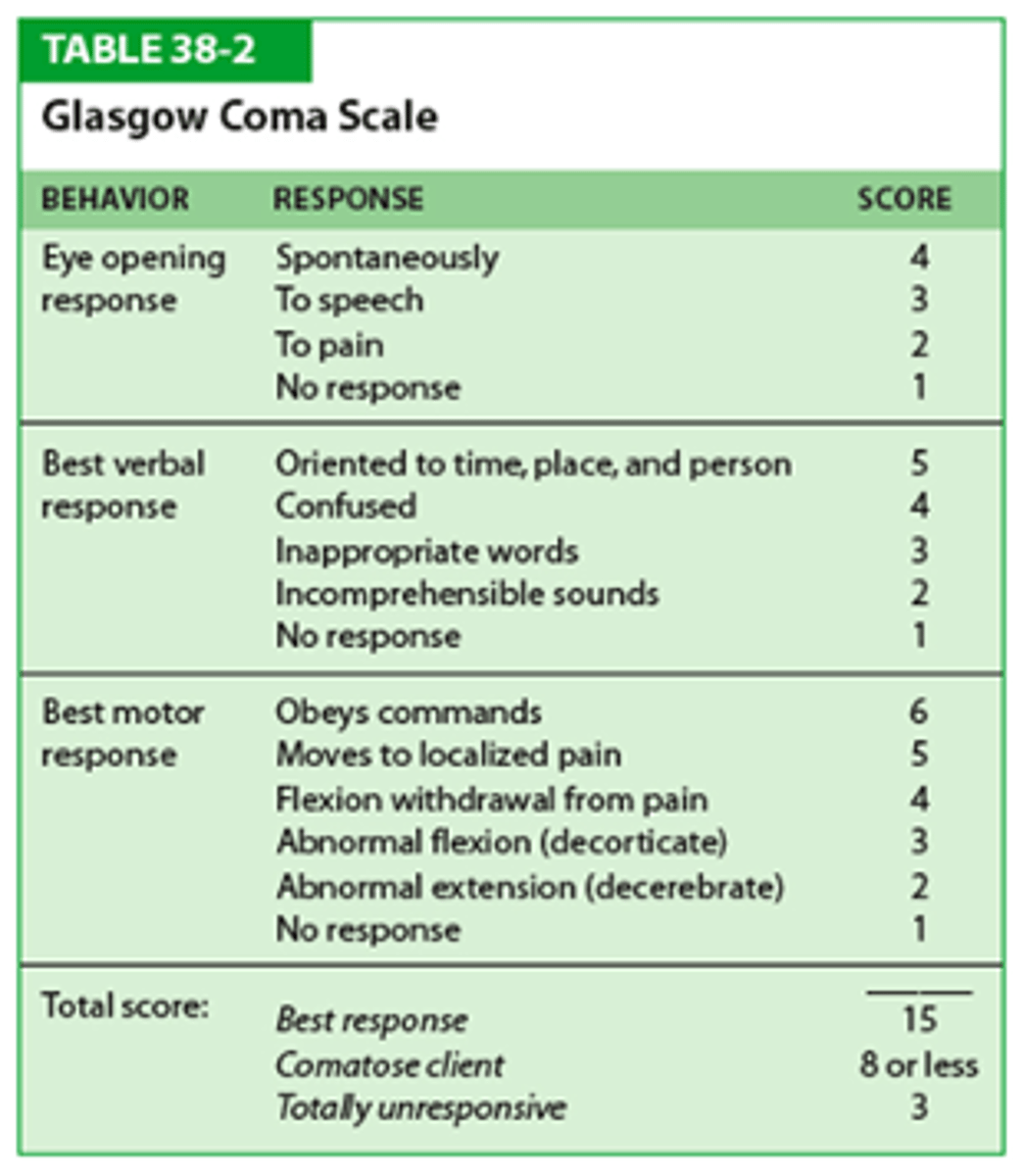
Glasgow Coma Scale
used to assess LOC in patients with acute brain injury, trauma, stroke, or altered mental status.
It scores eye opening, verbal response, and motor response. The total score ranges from 3 to 15.
Total Score and Severity: GCS
Document each component E+V+M
13-15: Mild brain injury
9-12: Moderate brain injury
≤8 Severe brain injury (secure airway)
coma caused by
caused by lesions that affect both cerebral hemispheres OR the brainstem reticular activating system.
1. Supratentorial causes
2. Brainstem lesions (infratentorial)
3. Diffuse encephalopathies
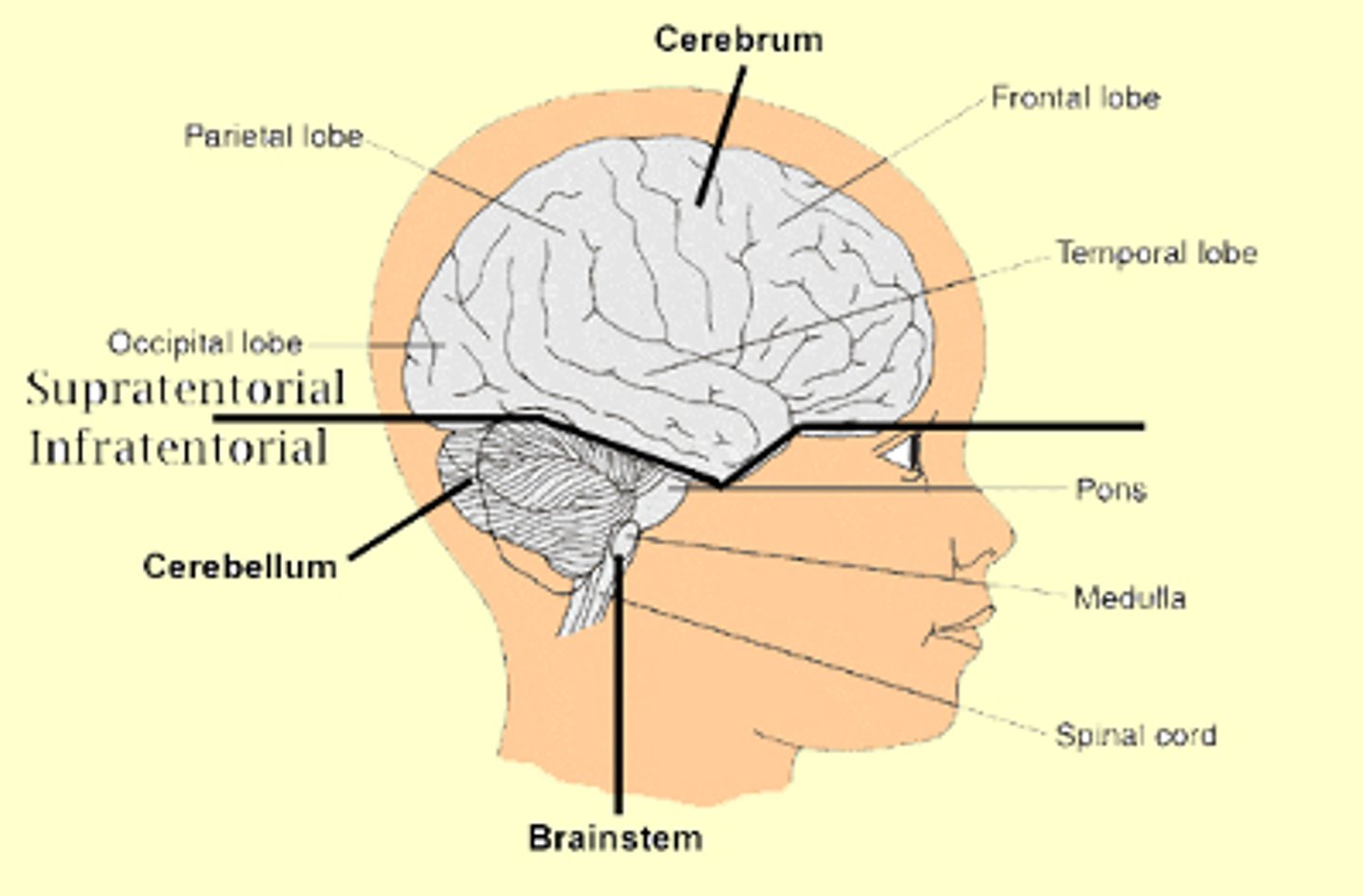
supratentorial causes of coma characteristics
usually progress in an orderly manner and cause coma by eventually compressing the midbrain and upper brainstem
brainstem lesions may cause coma _______
may cause coma abruptly
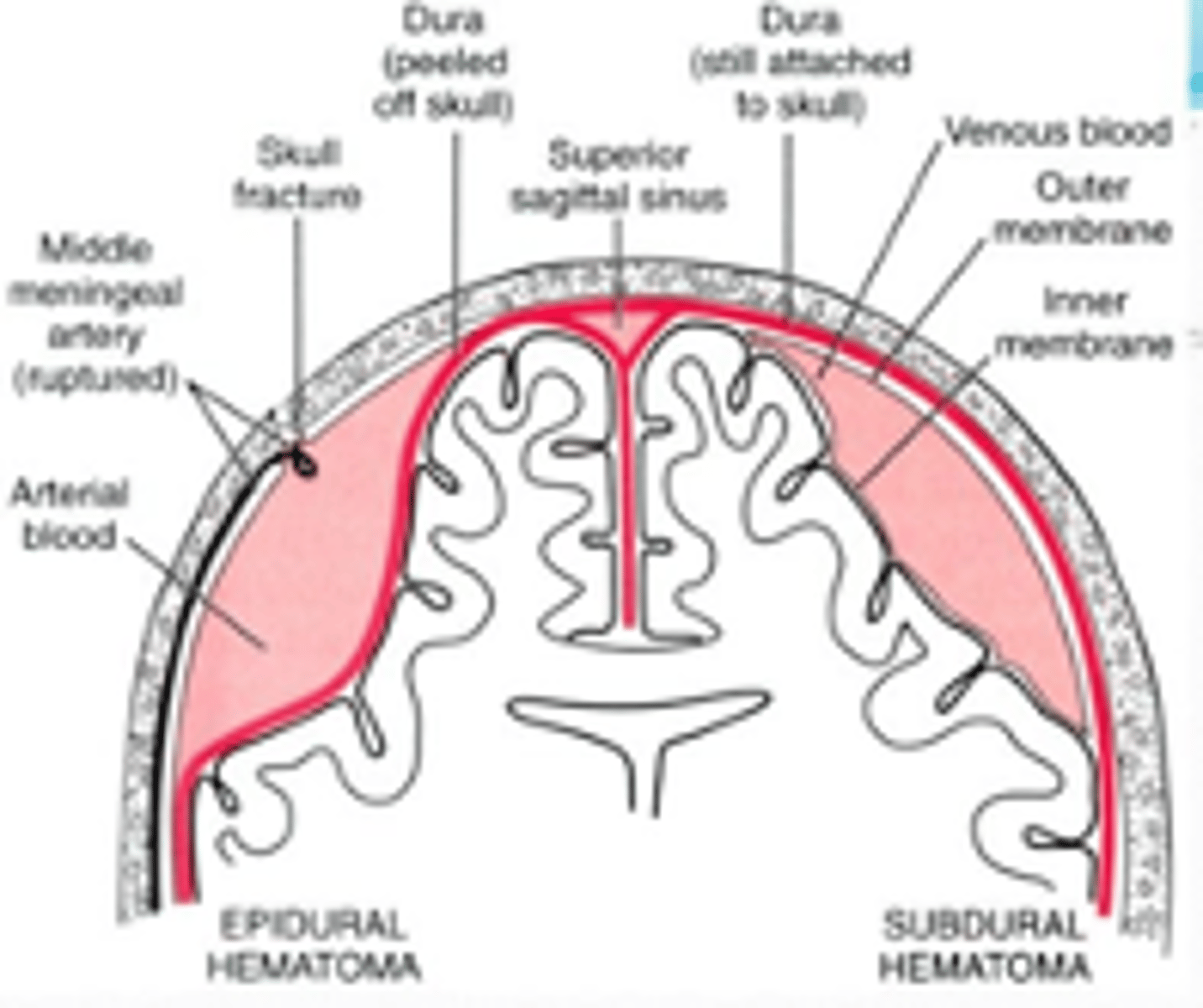
Coma: Supratentorial Causes
•Subdural hematoma
•Epidural hematoma
•Cerebral contusion
•Intracerebral hemorrage
•Brain abcess (rare)
•Cerebral infarction (stroke)
•Brain tumor
Coma: Infratentorial Causes
•Basilar artery thrombosis
•Pontine hemorrhage
•Cerebellar hemorrhage or infarction
Coma: Diffuse Encephalopathies Causes
•Meningitis & encephalitis
•Subarachnoid hemorrhage
•Hypoglycemia
•Global cerebral ischemia
•Drug intoxication
•Hepatic encephalopathy
•Hyperosmolar states
•Hyponatremia
•Hypothermia
•Hyperthermia
•Seizure*
Approach to the Comatose Patient
1. ABCs
2. Priority labs
3.I V: dextrose, thiamine, naloxone
4. Treat seizures
5. Full history (family) & neuro exam
6. Head CT if indicated
7. Consider: LP, EEG, MRI
priority labs for comatose pt
-Glucose
-Electrolytes
-ABG
-Liver, thyroid fn
-CBC
-Tox screen
-PT,PTT
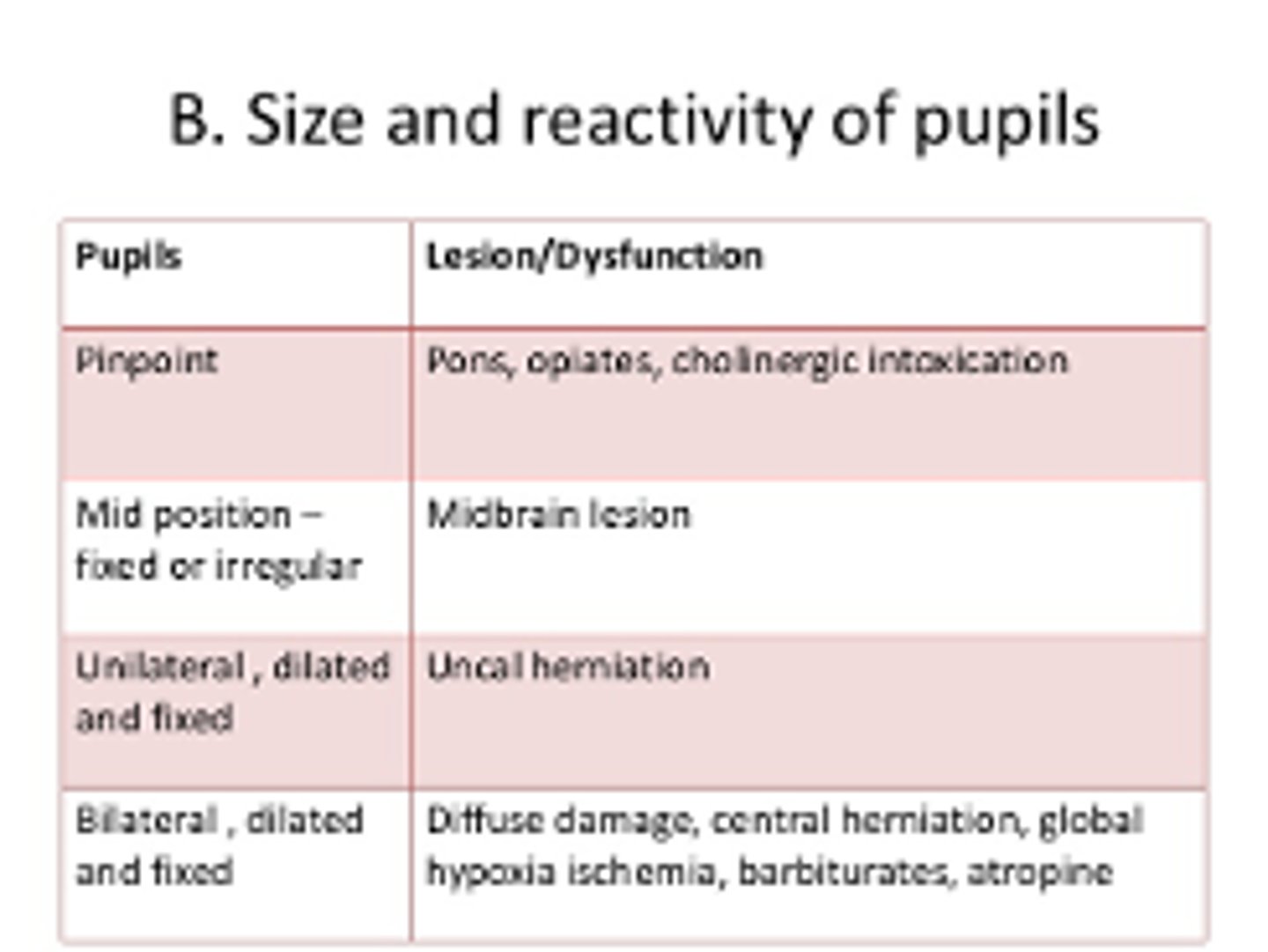
Coma PE: eyes
-Funduscopic
-Pupils
-Oculocephalic reflex (doll's eyes)
-Oculovestibular reflex (cold calorics)
-Corneal reflex
Oculocephalic reflex
doll's eyes movement assessing brainstem functioning
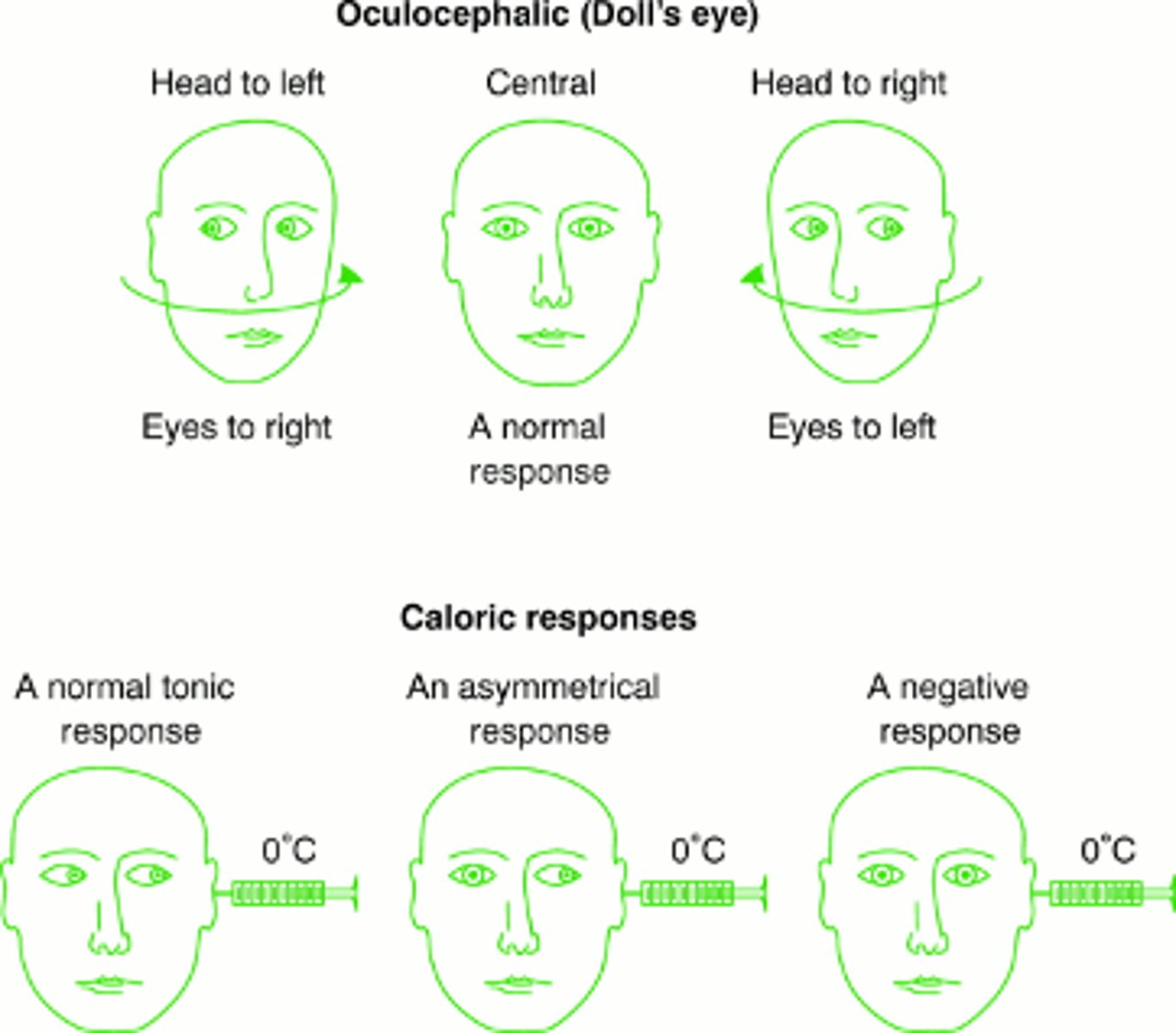
brainstem function and oculovestibular reflex
The reflex is independent of the cerebral cortex
Presence of OVR indicates intact brainstem
Oculovestibular reflex (cold calorics)
Used in comatose patients or neurologic exams: Cold water irrigation of the ear → Eyes deviate toward the irrigated ear
(No fast corrective phase in coma)
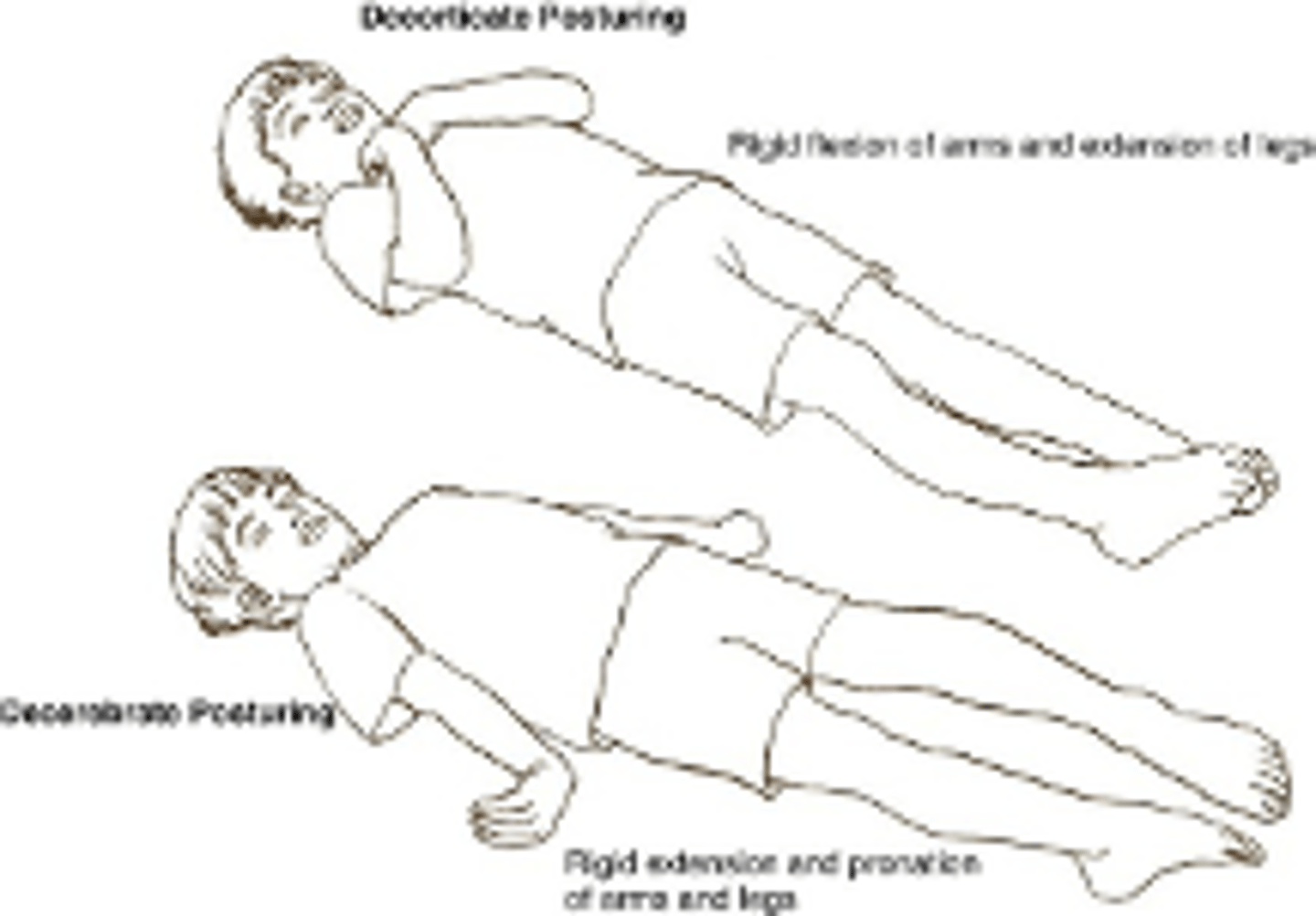
Coma PE: Posturing and responses to pain, Breathing patterns
Posturing and responses to pain:
–Decorticate
–Decerebrate
–Flaccidity
Breathing patterns
Decorticate posturing
arms flexed toward chest, wrists and fingers flexed, legs extended and internally rotated
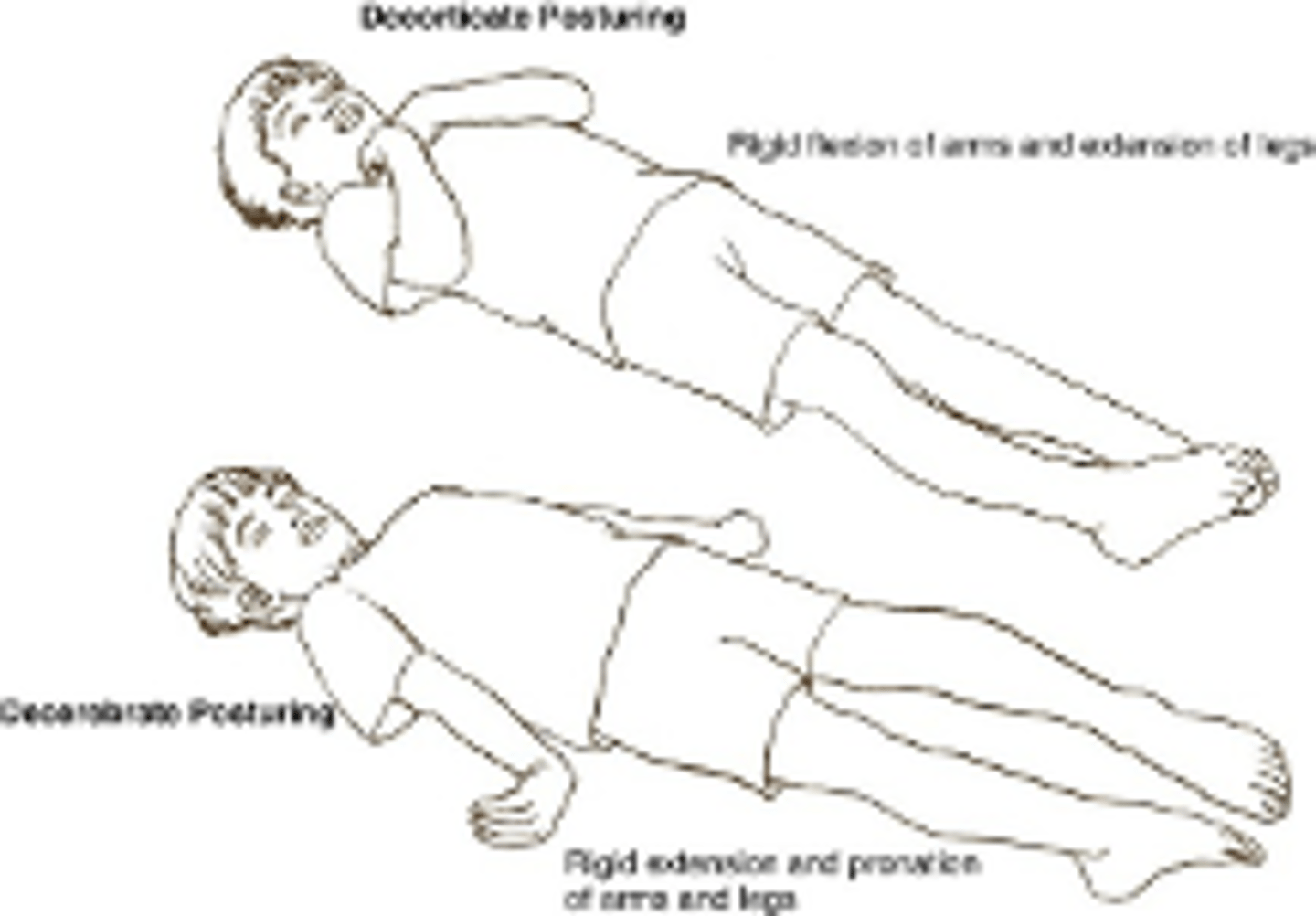
Decerebrate posturing
extensor posturing arms extended, adducted and internally rotated, wrists pronated, legs extended and plantar flexed, neck extended
Flaccidity
reduced or absent muscle tone, often seen in certain neurological conditions (e.g., damage to motor nerves, spinal cord injury, or some forms of paralysis)
Flaccid muscles feel limp and offer little resistance to movement.
Syncope
The transient loss of consciousness with spontaneous recovery that results from an acute global reduction in cerebral blood flow.
Syncope is a symptom; the goal is to determine the cause.
3 major types of syncope
orthostatic
cardiac
neurocardiogenic
Differential Diagnoses
•Seizures
•TIA
•Substance use
•Sleep disturbances/Narcolepsy
•Head trauma
•Somatoform disorders
Syncope Causes - Orthostatic
Hypovolemia, vasodilator medications autonomic neuropathies (DM, Parkinson's), pheochromocytoma
Syncope Causes - Cardiac
Arrhythmias, bradycardia, tachycardia, reduced cardiac output, left ventricular flow obstruction (aortic stenosis, hypertrophic cardiomyopathy),PE, pulmonary hypertension, MI, cardiac tamponade, sick sinus syndrome, AV block, V tach or V fib, Mitral stenosis, Long QT syndrome, pacemaker dysfunction
Syncope Causes - Neurocardiogenic
vasovagal, situational (acute hemorrhage, cough, sneeze, anxiety), Valsalva, POTS, hyperventilation
Vasovagal Syncope
ages? physiology?
•"Fainting"
•Common in all age groups
•Physiology: hypotension, vasodilatation & bradycardia due to withdrawal of sympathetic tone and increase in vagal tone
Vasovagal Syncope - Common precipitants
-Prolonged standing
-Warm environments
-Emotional distress
-Pain
Vasovagal Syncope - Pro Drome
-Diaphoresis
-Pallor
-Nausea
-Dim vision
-Salivation
-ringing ears
-Difficulty thinking
Other Reflex Syncope: Situational and Carotid Sinus Sensitivity
•Situational:
-Cough
-Micturition
-Defecation
•Carotid Sinus Sensitivity (overreaction of a "pressure sensor" in your neck like when shaving)
Orthostatic Hypotension causes
•Autonomic dysfunction -- ANS is not regulating BP. sympathetic "fight of flight" system overreacts; blood vessels constrict too much
•Massive hemorrhage
•Severe dehydration
Cardiac Causes of Syncope - Bradyarrhythmias
- Sinus node dysfunction
- 2nd and 3rd degree AV block
- Drugs (beta blockers, Ca channel blockers, digoxin...)
- Pacemaker malfunction
Cardiac Causes of Syncope - Tachyarrhythmias
SVTs more likely to cause pre-syncope & palpitations
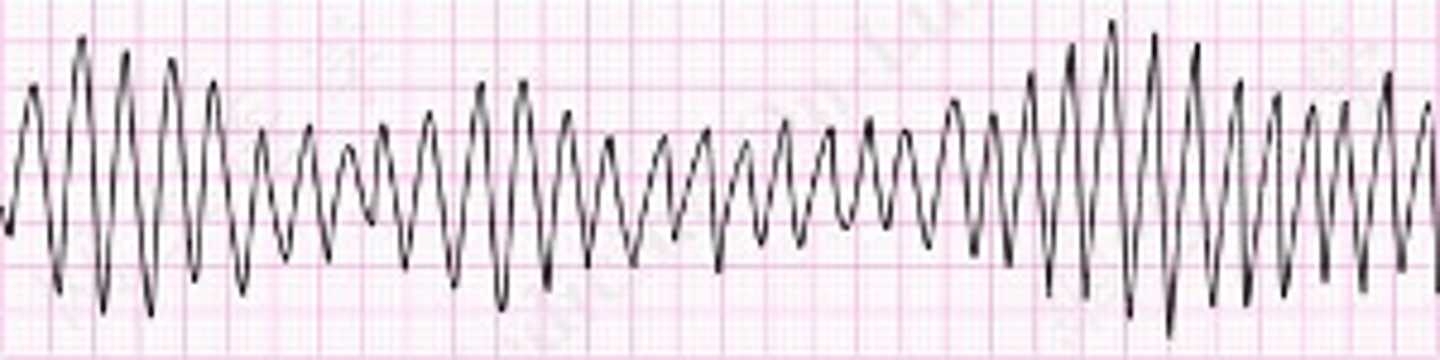
Ventricular arrhythmias:
•Ventr. Tachycardia
•Torsades de pointes
•Ventr. Fibrillation
•Long Q-T syndrome
•Brugada syndrome
Cardiac Causes of Syncope - Outflow obstructions
exertional symptoms are common
-Aortic stenosis
-Hypertrophic cardiomyopathy
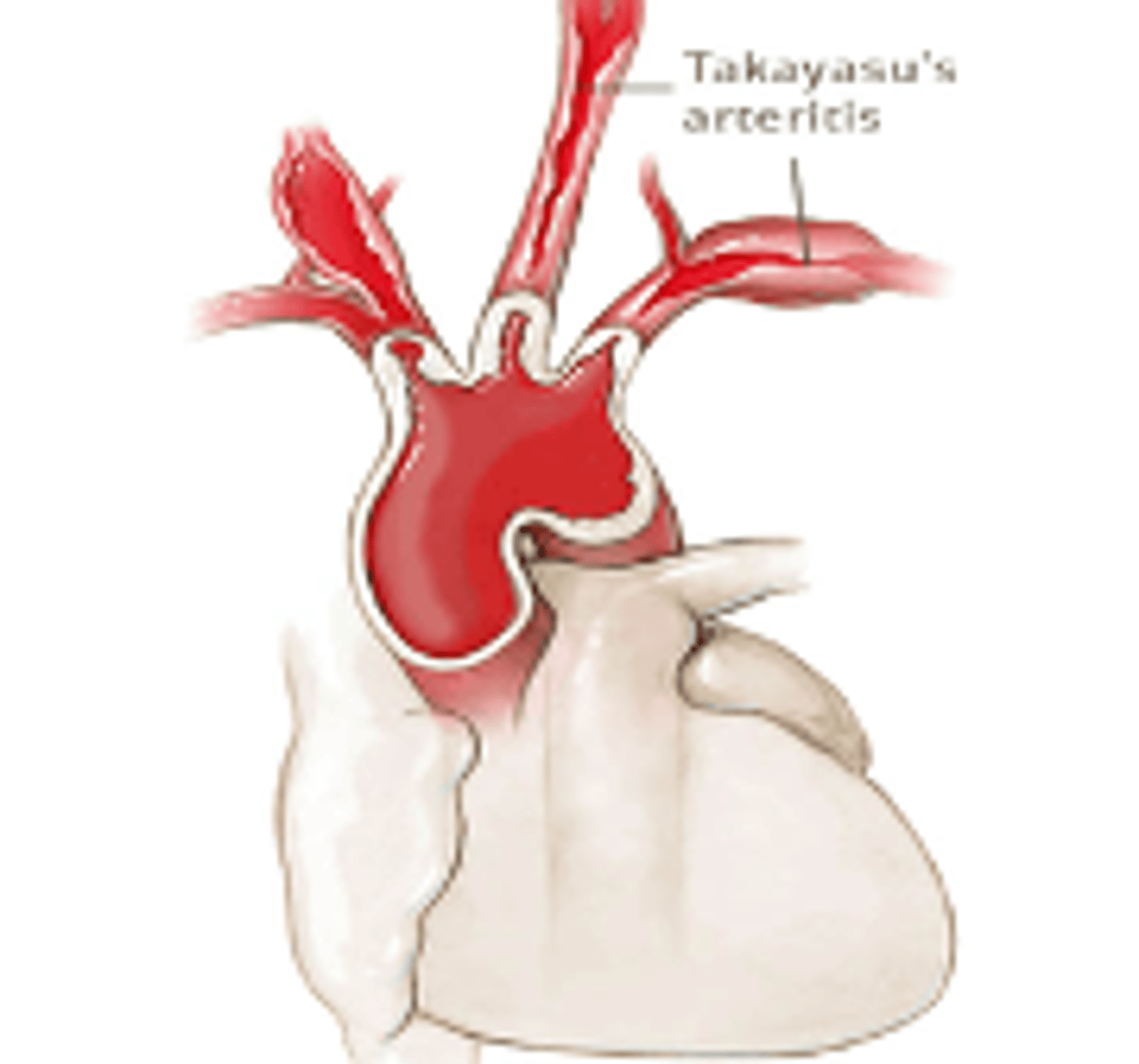
Cerebrovascular Causes of Syncope (uncommon)
•Takayasu's disease
•Vertebrobasilar insufficiency
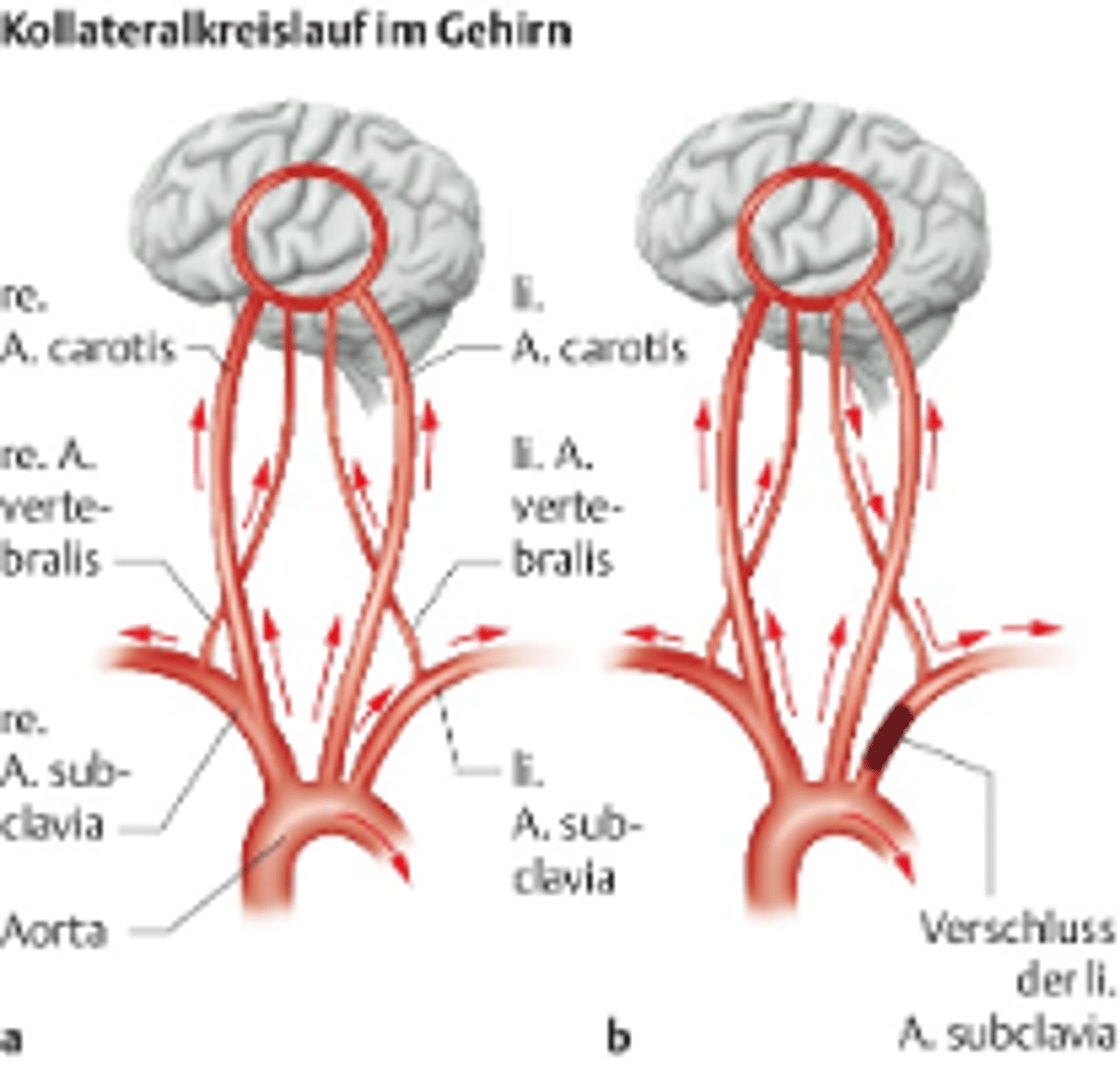
•Subclavian steal syndrome
•Subarachnoid hemorrhage
Takayasu disease
stress cardiomyopathy: preceded by an intense emotional, physical or psychologic stress causing ballooning of the left ventricle. Can be caused by excessive coronary vasoconstriction or increase catecholamine release.
Subclavian steal syndrome
occlusion or severe stenosis of the proximal subclavian artery leading to decreased flow of the ipsilateral vertebral artery
Syncope: Diagnosis
History is essential
-Past Medical History
-Prodrome
-Duration/description of event
-After the event
Physical Exam: incl HEENT, CV, pulm, abd, neuro
Tests
Syncope: Physical Exam... signs
1. Vitals
2. General Appearance
3. Skin
4. HEENT
5. Cardiac/vascular
6. Pulmonary
7. Abdominal
8. Neuro
VS: hypotension ox sats, temp
GA: LOC, signs of trauma, signs of intoxication or withdraw
Skin: skin abrasions or ecchymosis turgor, edema, cap refill, (think volume status/dehydration)
HEENT: any signs of trauma, conjunctiva, pupils, mucus membranes
Cardiac: JVD, displaced PMI (think tamponade, HF, cardiomyopathy) murmurs, rhythm, extra heart sounds,
Vascular: peripheral pulses, carotids
Pulm: crackles, breath sounds (unequal: pneumothorax)
Abd: tenderness, pulsatile mass, signs of GI bleed
Neuro: Mental status, cranial nerves, motor strength and tone, sensation, reflexes, signs of focal deficits
Syncope: Diagnostic Tests
-ECG
-Echocardiogram
-Holter (or other) monitors-inpatient cardiac monitoring for some.
-Tilt table testing
vasovagal syncope treatment overview
-Education
-Maneuvers
-Meds (beta blockers, midodrine)
cardiac syncope
-Varied, depends on the etiology.
- Referral to Cardiology
A patient has the following GCS components:
Eye opening to voice, Inappropriate words, Localizes to pain. What is the total GCS score?
A.9
B.10
C.11
D.12
3
5
5
= 11 (moderate)
Which of the following statements best defines syncope?
A.Loss of consciousness caused by seizure activity
B.Sudden LOC lasting > 30 minutes
C.LOC with persistent neurologic deficits
D.Transient LOC due to global cerebral hypoperfusion
D. Transient LOC due to global cerebral hypoperfusion