Metabolic dz / T2DM
1/91
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
92 Terms
What is metabolic syndrome?
A cluster of metabolic abnormalities associated with insulin resistance, visceral adiposity, increased CV risk, progression to T2DM
What are the common components of metabolic syndrome?
central obesity, hypertension, dyslipidemia, hyperglycemia, and insulin resistance
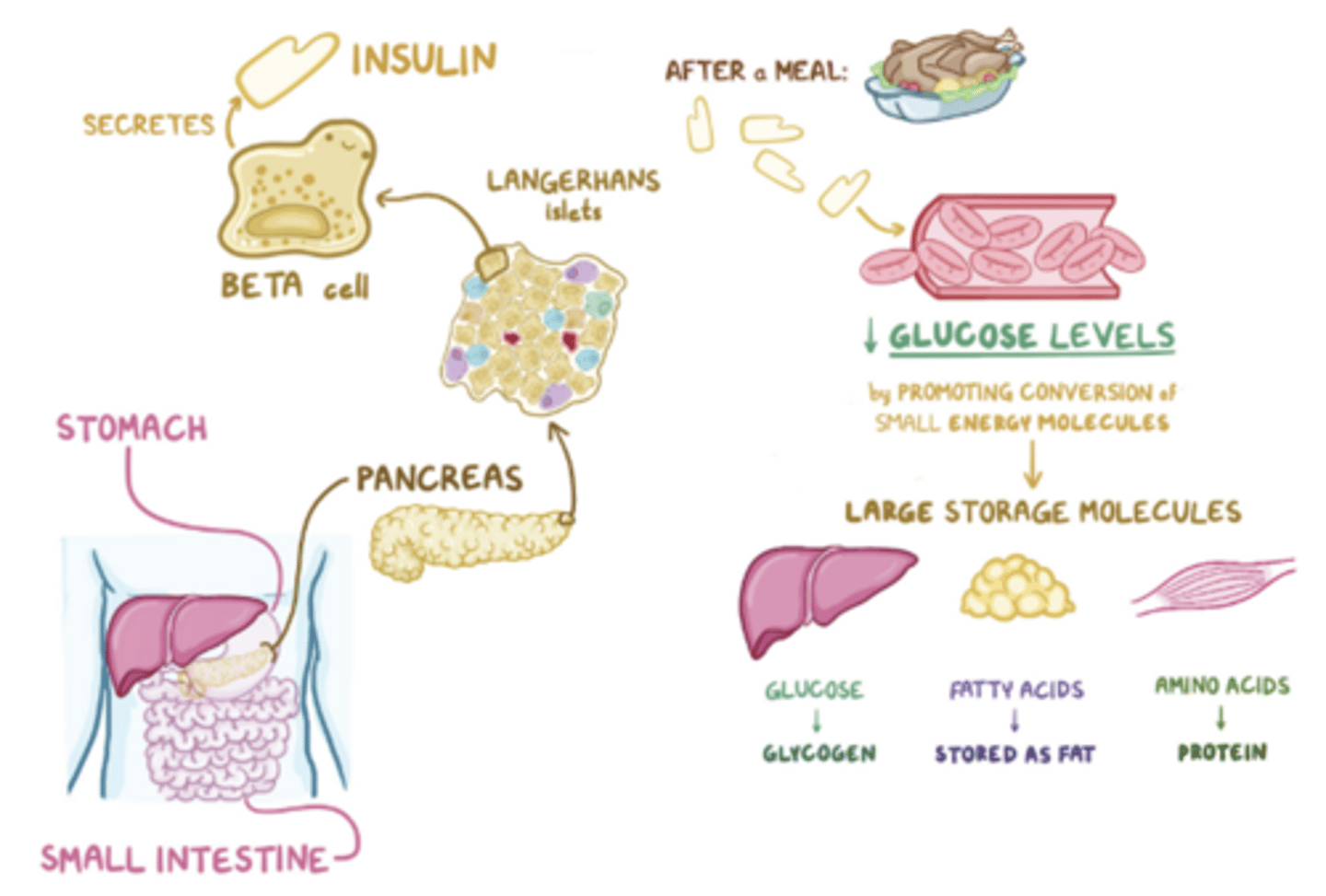
What occurs when insulin is released from pancreatic beta cells after food ingestion?
increased muscle and adipose glucose uptake and decreased liver production/ release of glucose to lower blood sugar
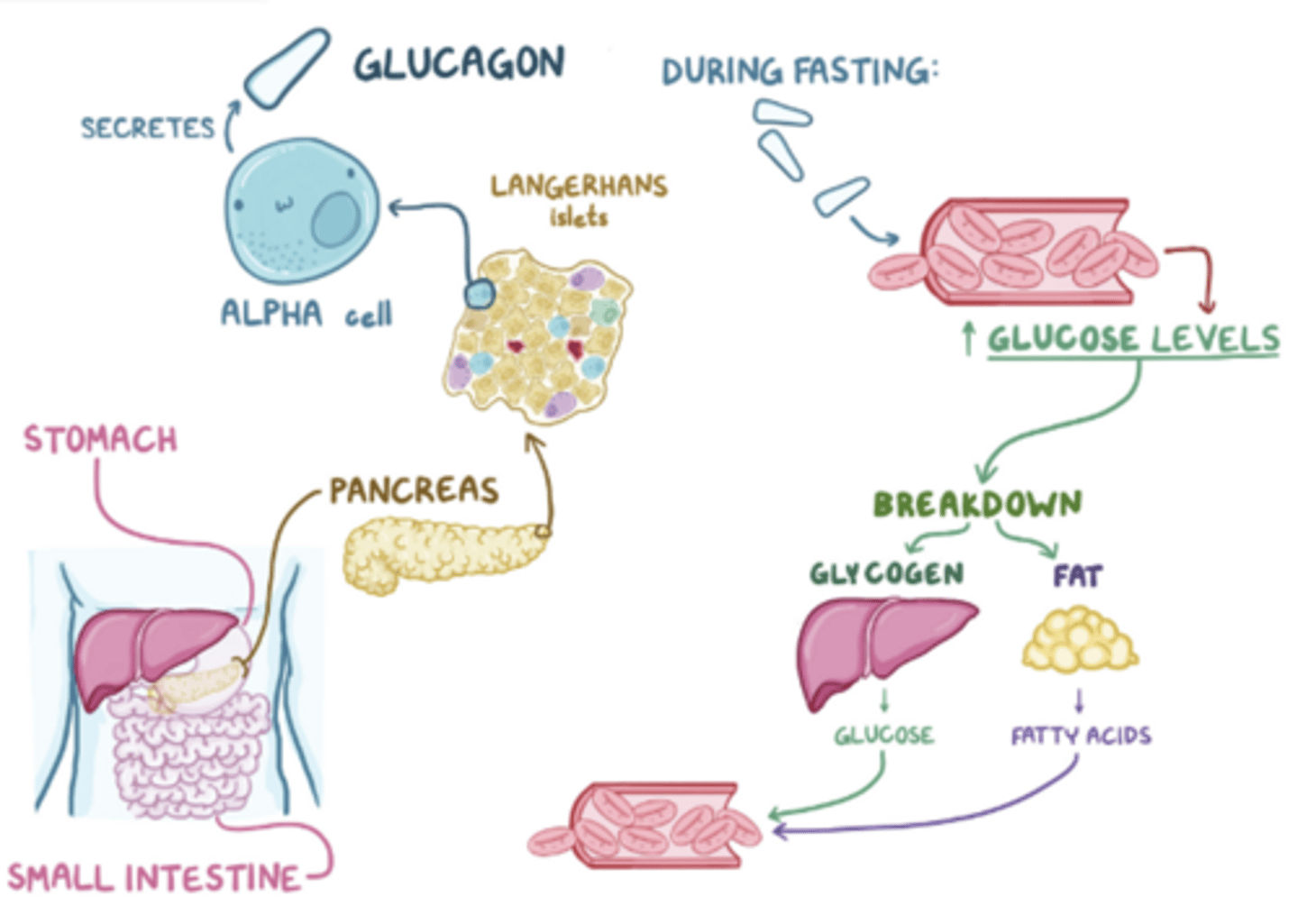
What occurs during the fasting state, between meals, during excercise, or stress?
glucose lowers and glucagon is released causing increased liver glycogenolysis and gluconeogenesis to elevate blood sugar
What is the role of incretins (GLP-1 and GIPs) in glucose metabolism?
amplify glucose-stimulated insulin secretion and suppress glucagon secretion
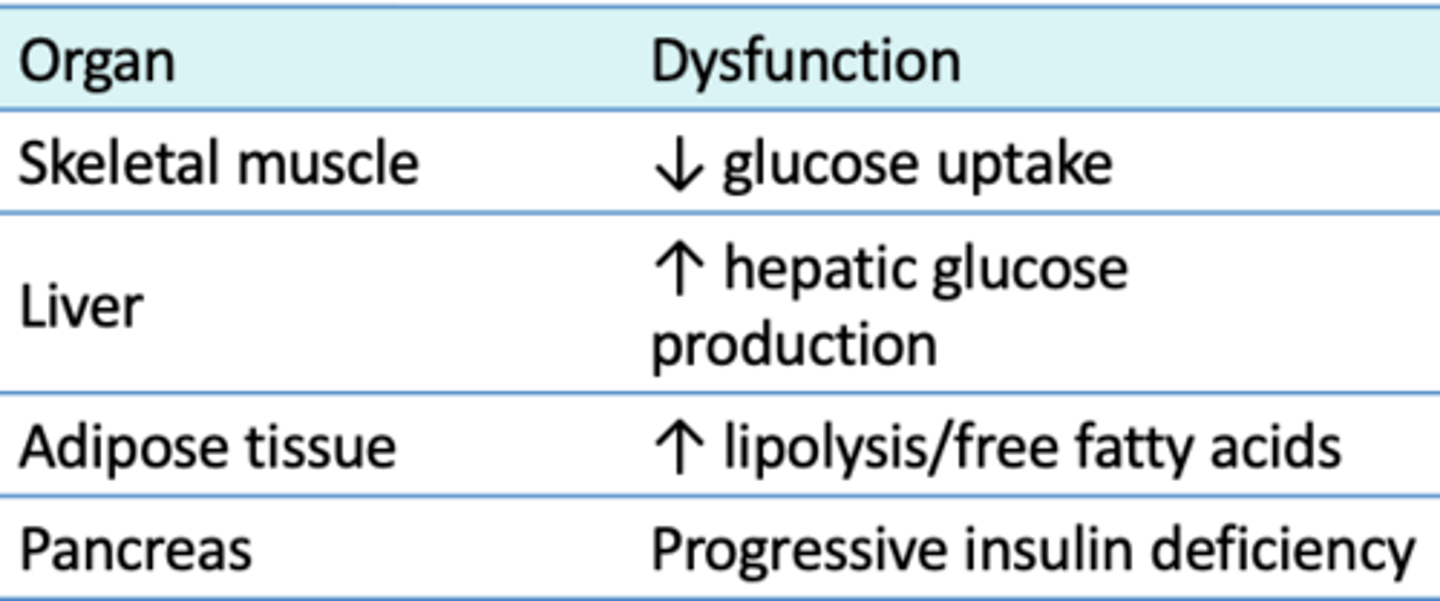
What is the pathophysiology of insulin resistance?
Muscle, adipose, and liver cells no longer “listen” to insulin making it unable to produce its normal effects and cause hyperglycemia
What are the consequences of chronic hyperglycemia?
beta cell failure and the inability to produce adequate levels of endogenous insulin
What is the central mechanism of insulin resistance?
visceral adiposity → increased inflammatory cytokines → insulin resistance → compensatory hyperinsulinemia → metabolic abnormalities
What is the diagnostic criteria for metabolic syndrome?
Any 3 of the following:
Waist circumference M >40 F > 35in
Triglycerides ≥150 mg/dL
HDL M <40 F <50 mg/dL
BP ≥130/85 mmHg
Fasting glucose ≥100 mg/dL
What are the common history findings in patients with Metabolic Syndrome?
Weight gain, sedentary lifestyle, fatigue, poor sleep, family history of T2DM, and snoring/sleep apnea symptoms.
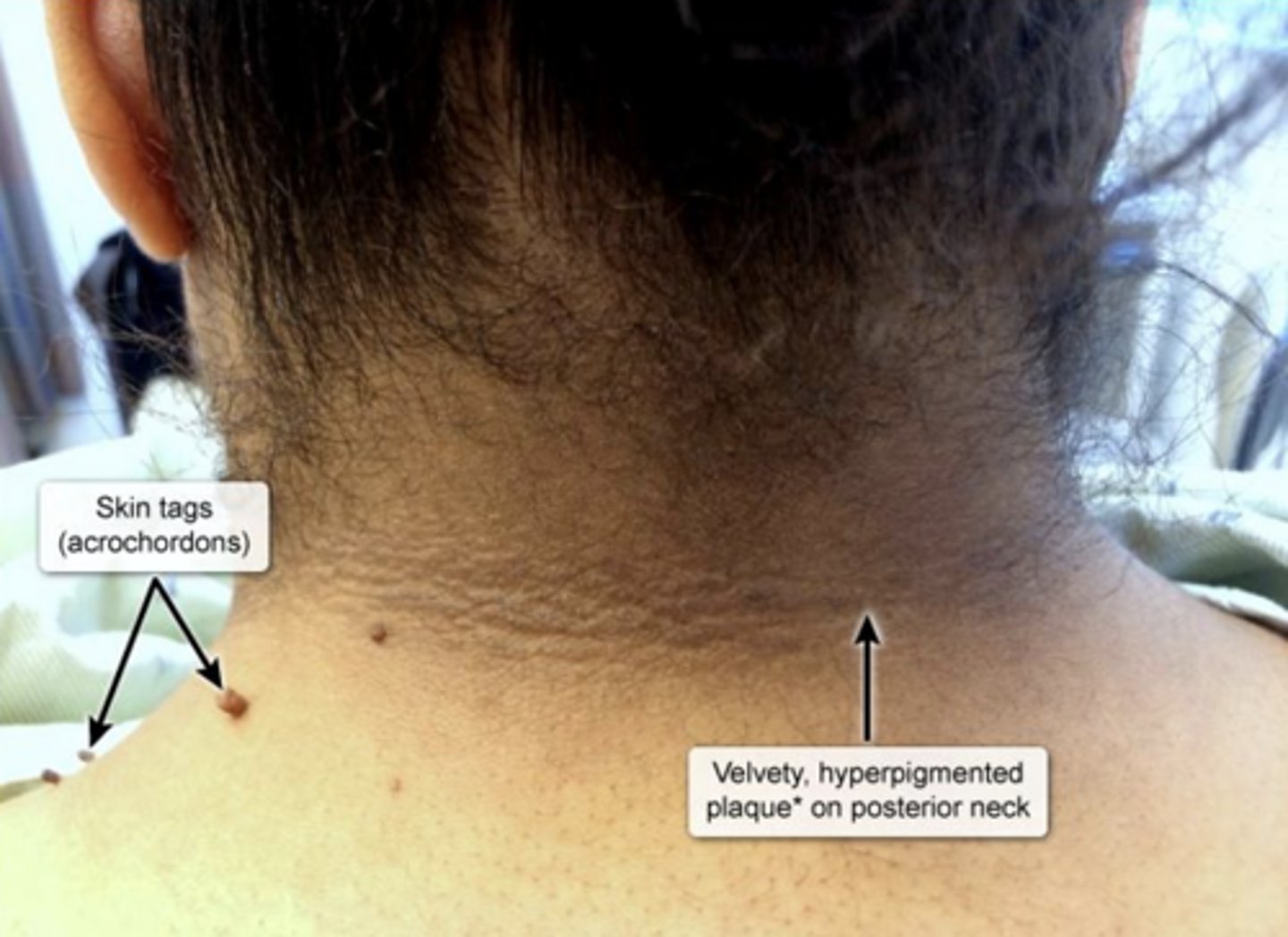
What are the physical exam findings in patients with Metabolic Syndrome?
central obesity, hypertension, acanthosis nigricans and skin tags
What are the risk factors of metabolic syndrome?
Diabetes mellitus type 2, Cardiovascular disease, and Non-alcoholic/ metabolic-dysfunction associated fatty liver disease
What is the first line treatment for metabolic syndrome?
aggressive lifestyle modification
What is prediabetes?
blood sugar levels are higher than normal, but not quite high enough to be diagnostic of diabetes mellitus
What are the USPSTF screening recommendations for prediabetes?
screening starting at age 35 in adults who are overweight or obese
How often should screening for prediabetes be repeated if the initial result is normal?
Every 3 years.
What is the clinical presentation of prediabetes?
often asymptomatic
What are the Hemoglobin A1C test results indicating prediabetes?
5.7-6.4%.
What Fasting Plasma Glucose (FPG) level indicates prediabetes?
100-125 mg/dL.
What Oral Glucose Tolerance Test (OGTT) result indicates prediabetes?
140-199 mg/dL.
What lifestyle changes can help manage prediabetes?
Increased physical activity, weight management, and dietary changes.
What is the recommended physical activity goal for reducing the risk of Type 2 Diabetes Mellitus (T2DM)?
150 active minutes per week and a 5-7% body weight reduction.
What medication is commonly used off-label to prevent the onset of T2DM?
Metformin
What are the indications for metformin use in prediabetes?
< 60 years old, BMI of 35+, history of gestational diabetes, implemented lifestyle changes but did not see improvement
How is prediabetes typically monitored?
Using HbA1C, with recommendations to recheck at least every year.
What are the two major defects in Type 2 Diabetes Mellitus (T2DM)?
Insulin resistance and B cell Dysfunction from chronic hyperglycemia
What are the pathophysiologic causes of T2DM?
impaired incretin, increased appetite, altered microbiota, decreased GLP-1 secretion, immune dysregulation, increased glucose absorption, upregulation of SGLT2 transporter
What are the risk factors for T2DM?
Overweight/obesity, >45, Family Hx, and Physical inactivity
What medications may be linked to T2DM?
Glucocorticoids, Thiazides, Antiretrovirals, and Atypical antipsychotics
What are common symptoms of hyperglycemia?
Fatigue, polyuria, polydipsia, polyphagia, blurred vision, numbness or tingling in hands/feet, recurrent infections, and slow wound healing.
What types of recurrent infections may occur in T2DM?
Vulvovaginal candidiasis, Skin infections, and UTIs
What are the physical exam findings of T2DM?
Obesity, HTN, Acanthosis nigricans, peripheral neuropathy findings
What diagnostic criteria indicate T2DM based on Fasting Plasma Glucose?
≥126 mg/dL.
What A1C level indicates T2DM?
≥6.5%.
What 2-hour OGTT level indicates T2DM?
≥200 mg/dL
What random glucose level indicates T2DM?
≥200 mg/dL
How often should A1c be monitored in T2DM?
Every 3 months if uncontrolled and every 6 months if stable
What is the general A1c goal?
< 7%
What may cause A1c to be unreliable?
anemia, hemoglobinopathies, CKD, and recent transfusion
What should be monitored for in T2DM?
vascular disease, kidney injury, neuropathy and treatment complications
What are the core goals of T2DM managment?
improve glycemic control, reduce cardiovascular risk, prevent complications, amd improve quality of life
What psychological interventions should be assessed in T2DM education?
Diabetes distress, depression, anxiety, disordered eating, and cognitive capacity.
What are the dietary recommendations for T2DM?
Minimize carbohydrates, increase fibers, involve healthy fats, limit alcohol (F <1 M <2), sodium <2300, avoid non-nutritive sweeteners
What are the weight reduction goals for T2DM?
Achieve & maintain ≥ 5% weight loss; consider medication if BMI ≥ 27 (semaglutide/tirzepatide) or surgery if BMI ≥ 40
What exemptions permit a A1c goal <8%?
history of severe hypoglycemia, limited life expectancy, older adults, and comorbid conditions
When should blood glucose be self-monitored?
fasting, 90-120 minutes after meals and before bedtime
What are the fingerstick blood glucose goals for diabetes?
Fasting: 80-130 mg/dL
Post-prandial: <180 mg/dL
Whos is continuous glucose monitoring reccomended for?
all individuals with T2DM, regardless of insulin use
When is Metformin (Biguanide) indicated for T2DM?
As initial therapy; does not cause hypoglycemia but has potential for lactic acidosis
What is the starting dose of metformin?
ER 500mg-1000mg daily with food (titrate to target dose of 1000mg BID with meals)
When is metformin contraindicated?
eGFR <30mL/min.
When are sulfonylureas (glipizide, glimepride) reccomended for T2DM?
In combination with metformin, especially if cost is a factor; may cause hypoglycemia and weight gain
When are meglitinides (repaglinide, nateglinide) or Amylin analogs (pramlintide) reccomended for T2DM?
Historically given with meals to reduce post-prandial hyperglycemia; may cause hypoglycemia and weight gain
When are SGLT2-I (canagliflozin, empagliflozin) recommended for T2DM?
Preferred therapy in patients with established heart failure and CKD to reduces mortality
What are the starting doses of canagliflozin and empagliflozin?
Empagliflozin 10mg PO daily (increase to max 25mg)
Canagliflozin 100mg PO daily
(can increase to max 300mg)
When are GLP-1 (dulaglutide, liraglutide, semaglutide) reccomended for T2DM?
Treatment of choice in obesity; can be used as initial or combination therapy in patients with established ASCVD or CKD
What are some starting doses of GLP-1's?
- Dulaglutide 0.75mg SQ once weekly, titrated to max dose of 4.5mg SQ weekly
- Liraglutide 0.6mg SQ once daily, titrated to max dose of 1.8mg SQ once daily
- Semaglutide 0.25mg SQ once weekly, titrated to max dose of 2mg SQ weekly
When is insulin reccomended for T2DM treatment?
If A1c is >10% or blood sugar is >300mg
What are the types of short-acting insulin and how are they given?
Lispro, Aspartate, and Glulisine used with meals (prandial) for quick action
What is a type of intermediate-acting insulin and how is it given?
NPH that can be mixed with short acting in specific ratios (50:50, 70:30)
What are the types of long-acting insulin and how are they given?
Detemir (Levemir), Glargine (Lantus), Degludec (Tresiba) that can be dispensed in pre-filled syringes
What is the systematic delivery of insulin for T2DM?
1) Add basal insulin
2) Titrate dose by 2 units every 3 days to reach FPG goal without causing hypoglycemia
3) If still not at goal, add prandial insulin with largest meal of the day
4) If still not at goal, refer to endocrinology
What is the starting dose for basal insulin?
10U SQ daily (alternative: 0.1-0.2 units/kg/day)
What is the starting dose for prandial insulin?
4U SQ daily with largest meal (alternative: 10% of basal dose); Increase by 1-2 units every 3-4 days and track blood sugar response
What is the follow up timeline after making adjustments to insulin?
every 2 weeks
What should be done if patients experience hypoglycemic episodes with insulin use?
lower the total daily insulin dose by 10-20% and monitor for improvement
What are the first-line medication classes for hypertension in diabetes?
ACE inhibitors, ARBs, thiazide diuretics, and calcium channel blockers.
What is the blood pressure goal for adults with diabetes?
<130/80 mmHg if safely achieved
What are the respective statin use recommendations for patients with diabetes?
40-75 y/o with DM: Mod intensity
DM + ASCVD: High intensity
DM + multiple ASCVD risk factors: High intensity
What are the LDL-C goals for patients with diabetes?
High Risk: <70 mg/dL
Very High: <55 mg/dL
What are the microvascular changes in diabetes?
Retinopathy, Nephropathy, and Neuropathy
What are the macrovascular changes in diabetes?
CAD, Stroke, and PAD
What are the clinical findings of diabetic retinopathy?
cotton wool spots, "dot blot" hemorrhages, hard exudates, neovascularization, and vitreous hemorrhage

What is the recommended frequency for dilated eye exams in diabetic patients?
Immediately after diagnosis then every 1-2 years
What is the treatment for proliferative retinopathy?
Laser photocoagulation and IVEGF
What is the leading cause of end-stage renal disease?
Diabetes
What are the signs of diabetic kidney disease?
Albuminuria, progressive CKD, and hypertension
What screening tool is used for diabetic kidney disease?
Estimated glomerular filtration rate (eGFR) and Urine albumin/creatinine ratio (spot UACR)
What Urine albumin/creatinine ratio (spot UACR) is concerning?
Macroalbuninuria of >300 mg/dL
How often should diabetic kidney disease screened for?
If initial screening test is abnormal, repeat testing x 2 over a span of 3-6 months.
What medications are reccomended for diabetic kidney disease?
SGLT2 inhibitor and ACE-I/ARBs for proteinuria
What is diabetic neuropathy?
A complication of diabetes that includes peripheral and autonomic neuropathy.
What is the pathology of diabetic peripheral neuropathy?
Excess blood sugar reacts with proteins and fats inside nerve cells, impairing normal nerve function.
What are the symptoms of diabetic neuropathy?
Burning pain, numbness, and loss of vibration, proprioception, and protective sensation
What is included in a comprehensive foot exam of diabetic peripheral neuropathy?
skin exam, circulation (pulses), pinprick and vibratory sensation, temperature, achilles reflexes, and monofilament exam at every visit
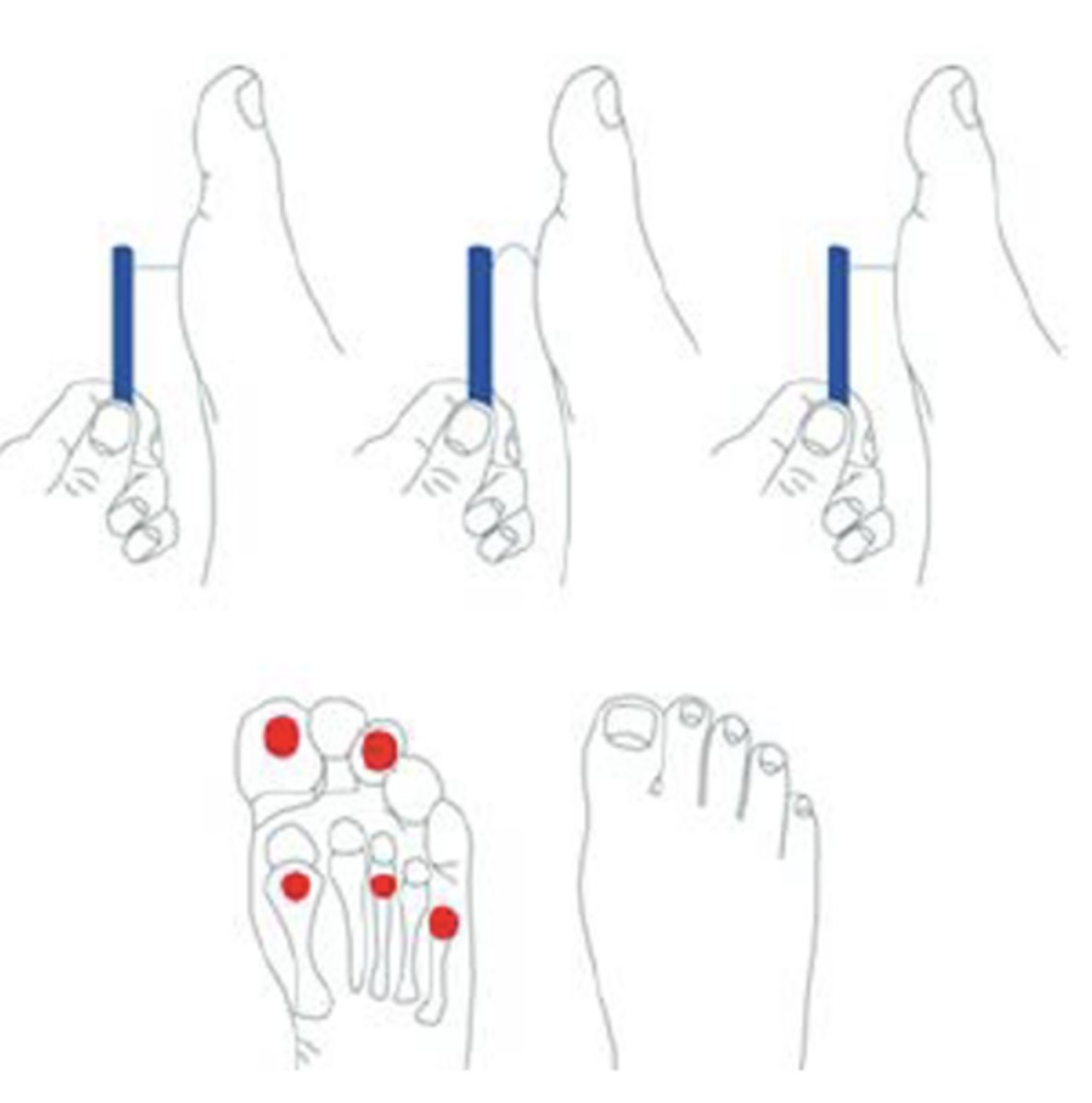
What are the 5 sites that should be tested during the monofilament tests?
- plantar surface of the hallux and 3rd toe
- 1st, 3rd, and 5th metatarsal heads
What monofilament test result indicates neuropathy?
A score of 8 or less
What are two manifestations for diabetic autonomic neuropathy?
Gastroparesis and Erectile Dysfunction
What is the leading cause of death in Type 2 Diabetes Mellitus?
Cardiovascular disease.
When is an ABI indicated to screen for PAD?
Decreased pulses, non-healing wounds, claudication, smoking, hypertension, and hyperlipidemia
What medication can be used for claudication?
Cilostazol
What vaccines are reccomended in patients with T2DM?
Influenza, Pneumococcal, Hepatitis B, and COVID-19