Understanding Shock: Types, Causes, and Management
1/44
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
45 Terms
Shock
A physiologic state characterized by systemic reduction in tissue perfusion, resulting in decreased tissue oxygen delivery.
Inadequate tissue perfusion
A condition in which circulation fails to meet the metabolic need of the tissue and fails to remove metabolic waste products.
Anaerobic metabolism
A metabolic process that occurs when there is insufficient oxygen delivery to tissues.
Effects on Heart during Shock
Decreased cardiac output (CO), hypotension, and presence of myocardial depressants.
Effects on Lung during Shock
Decreased gas exchange, tachypnoea, and pulmonary edema.
Effects on Endocrine during Shock
Increased reabsorption of water due to ADH release.
Effects on CNS during Shock
Decreased perfusion leading to drowsiness.
Effects on Blood during Shock
Coagulation abnormalities, including disseminated intravascular coagulation (DIC).
Effects on Renal during Shock
Decreased glomerular filtration rate (GFR) and decreased urine output.
Effects on GIT during Shock
Mucosal ischemia leading to bleeding and increased enzyme levels in the liver.
Hypovolaemic Etiology
Caused by blood loss, plasma/body water loss, electrolyte imbalance, vomiting, diarrhea, or dehydration.
Cardiogenic Etiology
Caused by valvular heart disease, myocardial infarction, cardiac arrhythmias, or cardiomyopathy.
Obstructive Etiology
Caused by cardiac tamponade, pulmonary embolism, tension pneumothorax, or air embolism.
Neurogenic Etiology
Caused by paraplegia, quadriplegia, trauma to the spinal cord, or spinal anesthesia.
Anaphylactic Etiology
Caused by injections (e.g., penicillin, anesthetics), stings, or shellfish.
Septic Etiology
Caused by Gram-positive, Gram-negative bacteria, fungi, viruses, or protozoa.
Endocrine Etiology
Caused by hypo- and hyperthyroidism or adrenal insufficiency.
Clinical Features of Shock
Depend on the degree of volume loss and duration of shock.
Types of Shock
Mild shock, moderate shock, and severe shock.
Mild Shock Features
Collapse of subcutaneous veins, pale and cool extremities, normal urine output, normal pulse rate, normal blood pressure, and patient feels thirsty and cold.
Moderate Shock Features
Mild shock features plus drowsiness and confusion, oliguria, pulse rate increased usually less than 100/min, and blood pressure normal initially then falls in later stage.
Severe Shock Features
Unconsciousness, gasping respiration, anuria, rapid pulse, and profound hypotension.
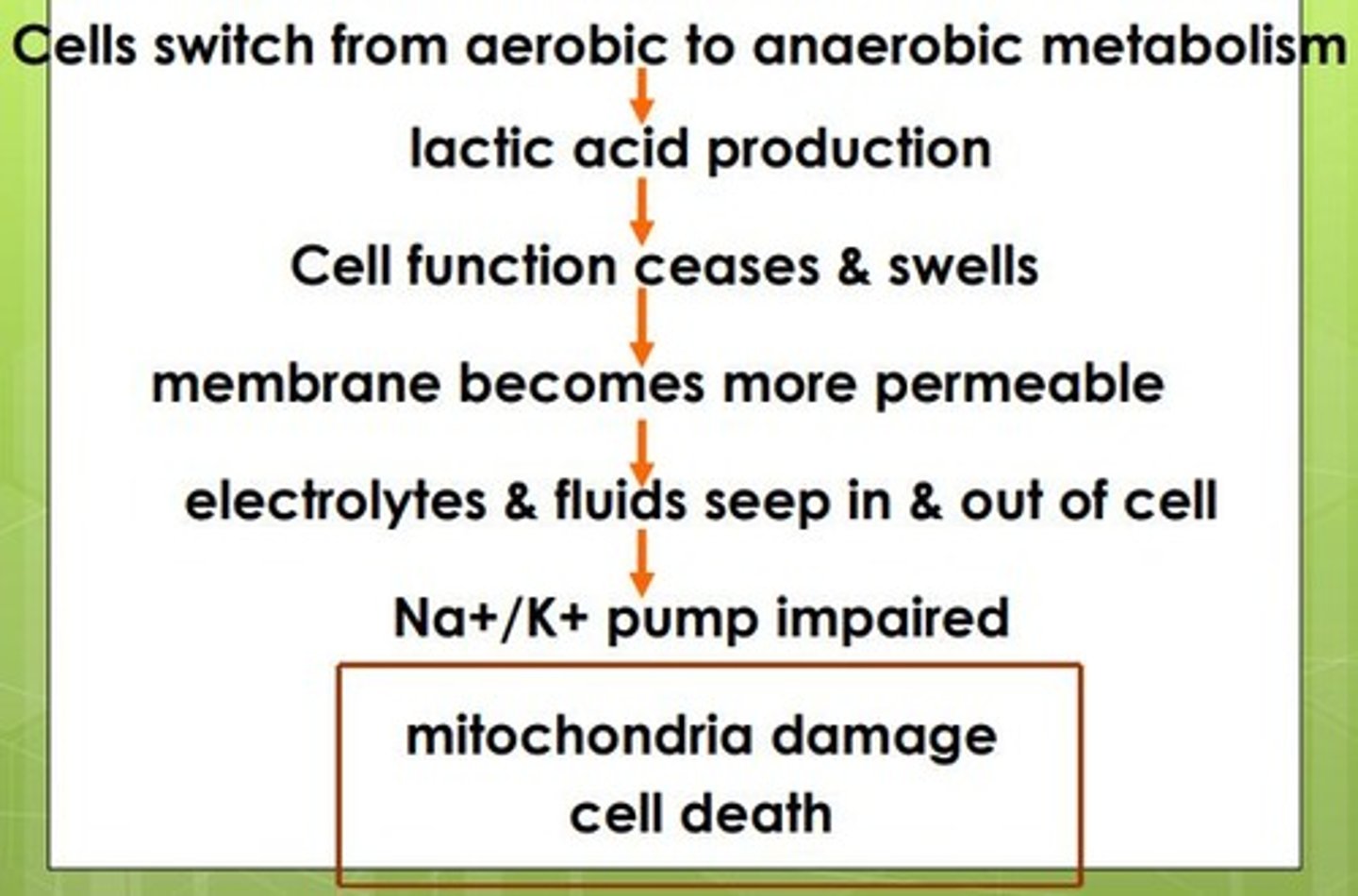
Stages of Shock
Initial stage: cells become leaky and switch to anaerobic metabolism; Non-progressive stage: attempt to correct metabolic upset; Progressive stage: compensation begins to fail; Refractory stage: organs fail and shock can no longer be reversed.
Monitoring
Blood pressure, Heart rate, Respiratory rate, Urine output, Blood CBC, Pulse-oximetry, ECG, U/S, CT, X-ray
Central venous pressure
Normal; 5-10cmH2O, If CVP<5cmH2O - Inadequacy of blood volume, CVP>12cmH2O - Cardiac dysfunction
Cardiac output
Measurement of the volume of blood the heart pumps per minute.
Pulmonary catheter
A catheter placed in the pulmonary artery to measure pressures.
Doppler ultrasound
A method used to assess blood flow and cardiac output.
Pulse waveform analysis
A technique to analyze the shape of the pulse wave to assess cardiovascular function.
Urine output & LOC
Clinical indicators of systemic and organ perfusion.
Sr. Lactate estimation & Base deficit
Tests used to evaluate metabolic status and perfusion.
Blood gas analysis
Measurement of PO2, PCO2, and pH levels in the blood.
Mixed venous O2 saturation
Normal range is 50-70% indicating the balance of oxygen delivery and consumption.
Dynamic Fluid Response
Infusing 250-500ml of Fluid rapidly in 5-10 minutes. Responders show improvement, transient responders revert back, non-responders do not improve.
Vasopressors
Medications like Phenylephrine and Norepinephrine used in distributive shock states.
Inotropic Drugs
Medications like Dobutamine used to increase cardiac output in cardiogenic shock.
Fluid Therapy in Shock
Includes Crystalloid Solutions (Normal saline, Ringers Lactate solution, Hartmann's solution) and Colloid Solutions (Blood transfusion).
Oxygen Carrying Capacity
Only RBC contribute to oxygen carrying capacity (hemoglobin); other solutions support volume but do not provide additional oxygen carrying capacity.
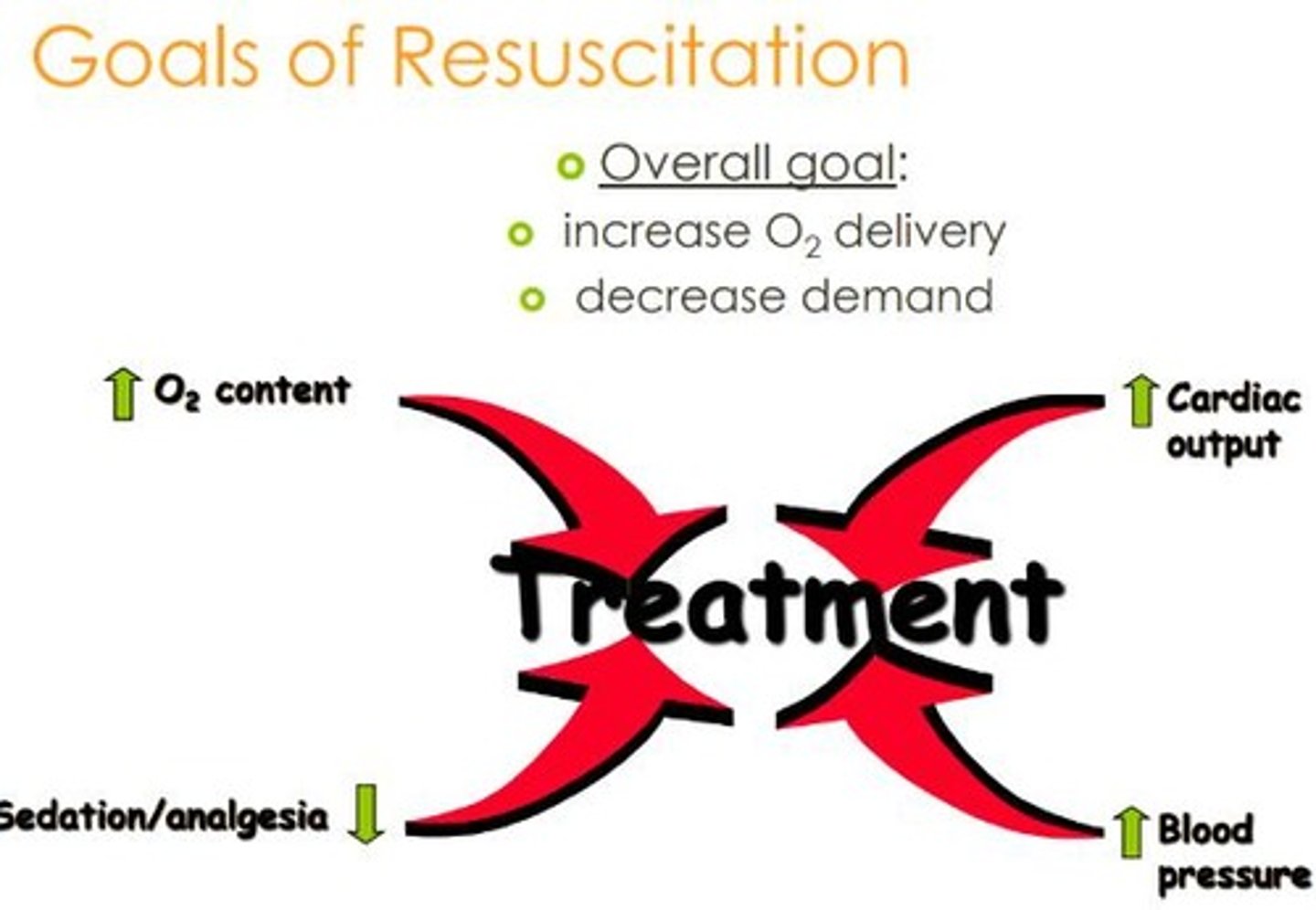
End Points of Resuscitation
Classic/Traditional: Restoration of blood pressure, normalization of heart rate and urine output, appropriate mental status. Improved/Global: All of the above plus normalization of serum lactate levels, resolution of base deficit, adequate mixed venous saturation.
Goal directed approach
Urine output > 0.5 mL/kg/hr, CVP 5-10 cm H2O, MAP 65 to 90 mmHg, Central venous oxygen concentration > 70%.
Obstructive shock
Causes include cardiac tamponade, air embolism, and pulmonary embolism; cardiac arrhythmias are primarily associated with cardiogenic shock.
Agent of choice in Severe septic shock
Norepinephrine is the first-line agent, but vasopressin is often used as an adjunct.
Type of shock from abdominal injury
The clinical picture suggests hemorrhage leading to hypovolemic shock.
Newer methods for monitoring tissue perfusion
Include muscle tissue O2 probes, infrared spectroscopy, and sublingual capnometry; Doppler ultrasound is not considered a newer method.
Last signs of shock
Profound hypotension is one of the last signs, indicating severe circulatory failure.