Human Physiology Final
1/75
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
76 Terms
The Endocrine System
Hormones
Chemical messengers
Distant targets
Travel in the blood → diffuses into blood and travels through body in low concentrations
Low concentrations
Endocrine cells/glands
Cells which release hormones
Target tissue (cell)
Tissues (cells) which contain receptors for that particular hormone
Types of Hormones
Peptide
made of chains of amino acids
most diverse group
ANP, insulin
Steroid
derived from cholesterol
smaller group
“-sterone” suffix
Aldosterone, progesterone, testosterone, etc
Amines
derived from tyrosine or tryptophan (single amino acids)
subgroup: catecholamine → dopamine
subgroup: thyroid hormone → T3 and T4
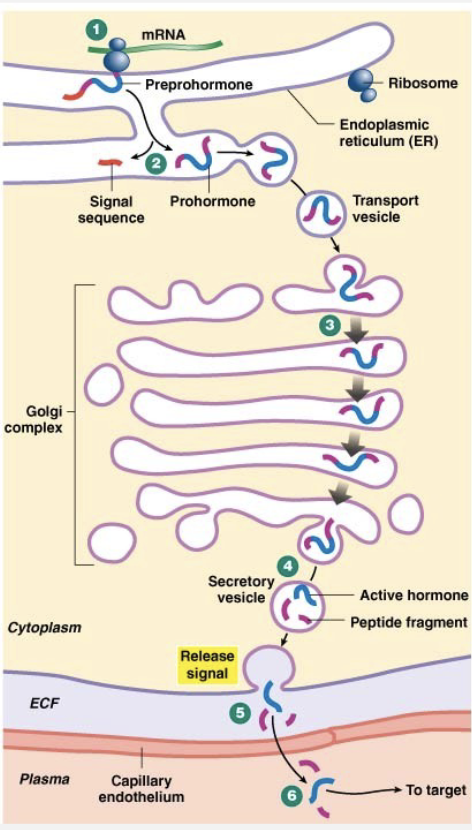
Peptide Hormones
Made of peptides
Preprohormones
Cleaved to activate
Hydrophilic
Fast acting, short duration
Membrane receptors
2nd messenger systems, ion channels
Half life = few minutes
Half life = time until half of the hormone degrades
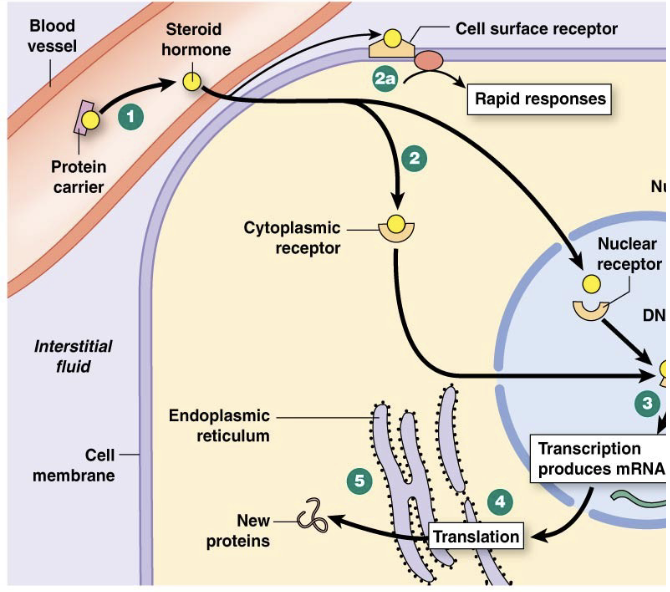
Steroid Hormones
Lipophilic
Made when needed, if made in advance, will diffuse out bc permeable
Slow acting, long duration
Intracellular receptors
Activate gene transcription
Half-life = minutes to hours
Use protein carriers in the blood to move through the body
protein carriers protect the hormone from being taken into the wrong cell and metabolized.
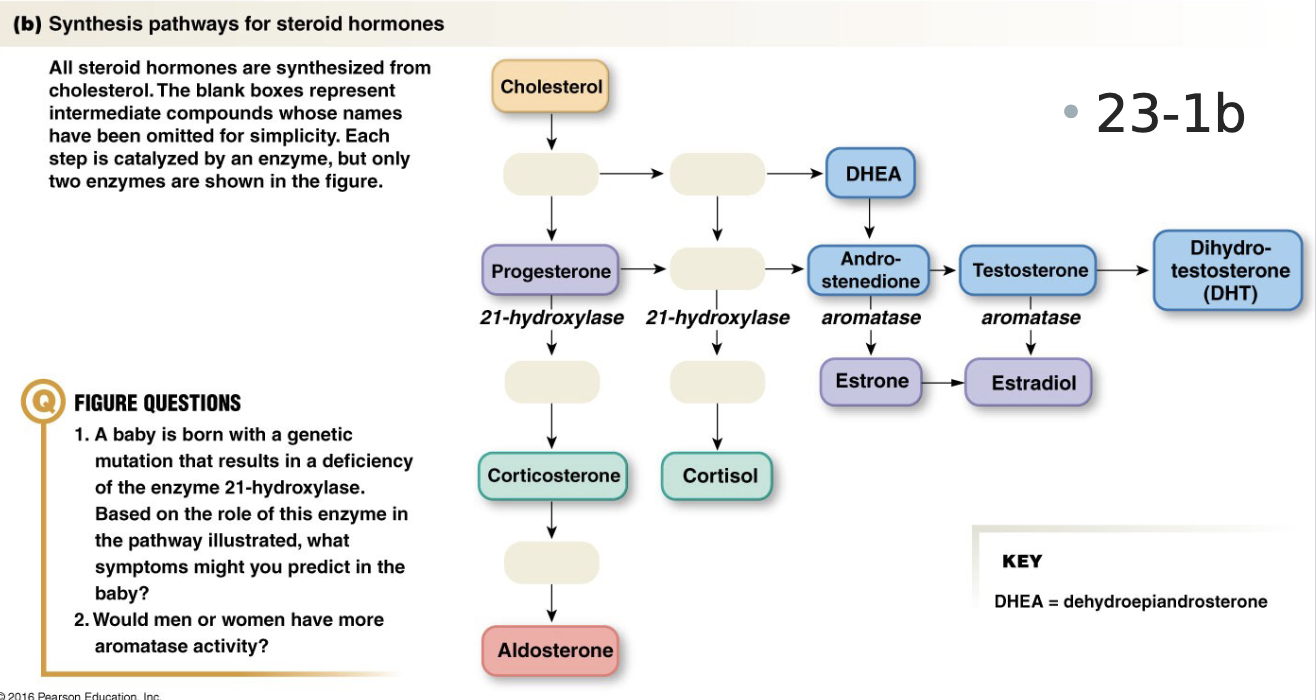
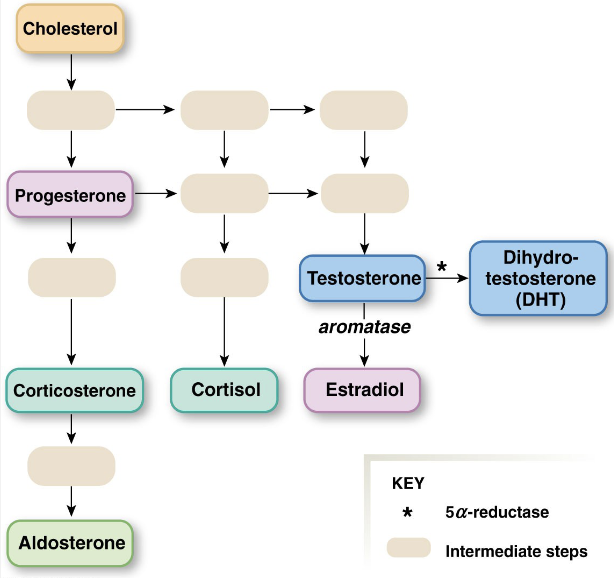
Synthetic Pathway of Steroids
generally: cholesterol → progesterone → corticosterone → aldosterone
testosterone → estradiol
Amine Hormones
Catecholamines
epinephrine, norepinephrine
hydrophilic
membrane receptors
Thyroid
T3 and T4
Hydrophobic
Intracellular receptors
regulate metabolism
Hormone Release
Feedback loops
Mostly negative
Some positive
Simple (classic)
Endocrine cell senses and releases hormone which effects another cell
Multiple stimuli/input: as a result of feedback loops
Complex pathways
two or more hormones
Hormone A affects Hormone B affects C…
Hypothalamic pituitary axis
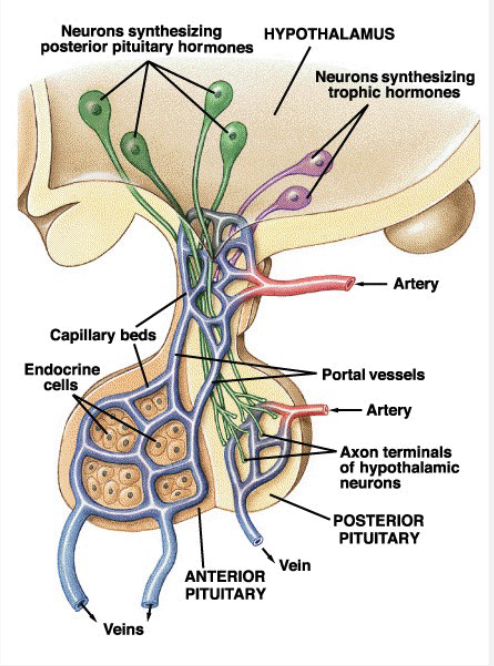
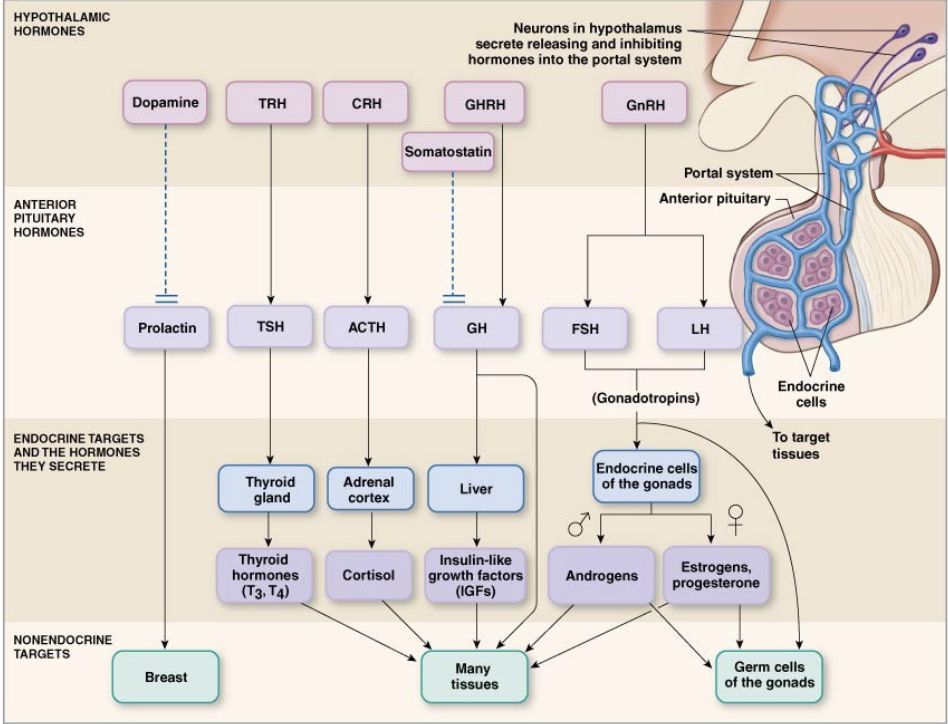
Hypothalamic Pituitary Axis
Hypothalamus
Neurocrines- produced by neurons, released into blood
Hormones
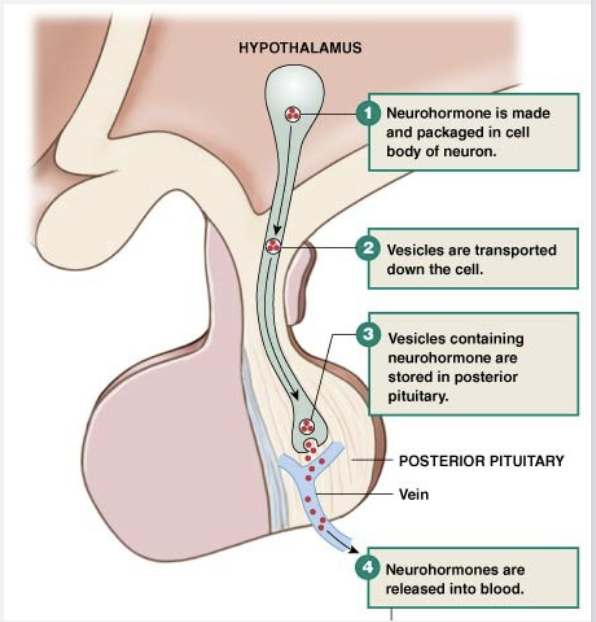
Posterior Pituitary
Releases hypothalamic neurocrines
not a true endocrine gland because it does not produce a hormone, but it’s still treated like an endocrine gland
Anterior Pituitary
Responds to trophic hormones from hypothalamus
true endocrine gland because it produces and responds to hormones
Hypothalamic Anterior Pituitary
“-RH” = releasing hormone
“-IH” = inhibiting hormone
dopamine = prolactin inhibiting
somatostatin = growth hormone inhibitor
“-RH” and “-IH” = hormones released by the hypothalamus
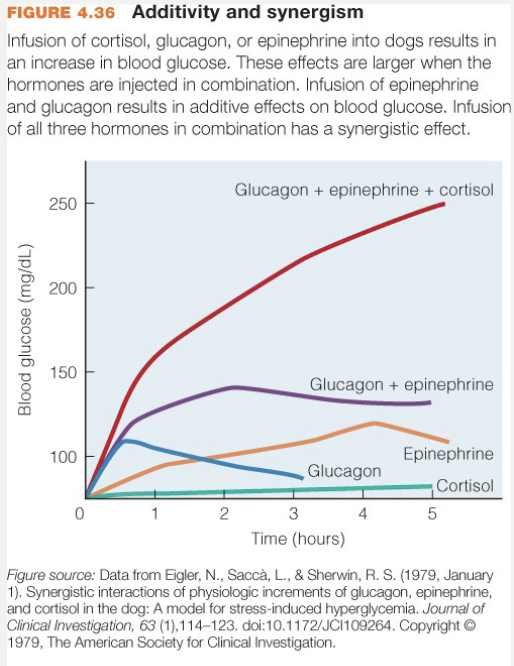
Hormone Interactions
Synergistic (Moyes 3rd ed)
Two+ hormones affect target
Results in greater than additive response (not just added)
Permissiveness
Hormone allows another to be fully active
Antagonistic
One hormone blocks effects of another
Hormone Pathologies
Secretion
Hypo-secretion: less/below
Hyper-secretion: more/above
Receptors
Up-regulation (more sensitive; hyper-responsiveness)
Down-regulation (less sensitive; hypo-responsiveness)
Metabolism
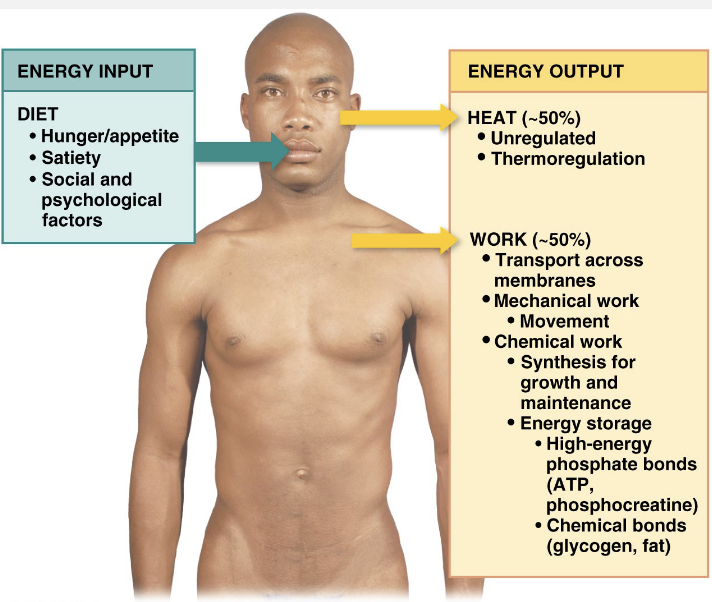
Metabolism – all chemical reactions in body
Input (food) = Output (work + heat
Input > Output
Weight gain
Glycogen, Fat → long-term energy store, takes longer to release. Short-term energy store, rapidly available
Input < Output
Weight loss
Energy Balance
Input
appetite → tells us when hungry
satiety → tells us when full/satisfied
Output
transport work → across membranes
chemical work → synthesis for growth/maintenance
mechanical work → movement
heat
Social and psychological factors tend to override satiety. why people eat more when they are already full.
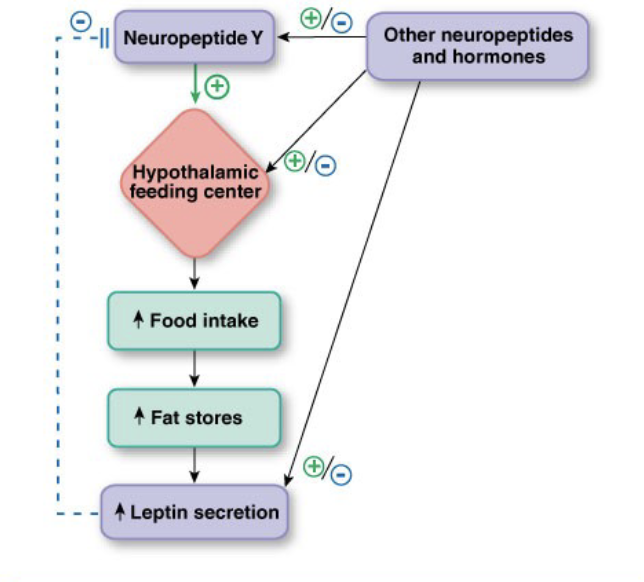
Energy Balance and Neural Factors
Neural Factors
Feeding Center
- Satiety Center
Hormonal Input
CCK → released by digestive tract in response to proteins and lipids
Insulin → released by pancreas in response to high glucose. insulin = carbohydrate
Leptin → released by adipose tissue
Energy Balance and Theories
Glucostatic Theory: Short-term, meal-by-meal
Low glucose
Stimulate feeding center
Inhibit satiety center
Satiety center needs insulin
Relationship to diabetes I: Not enough insulin. Symptom is polyphagia→ eating all the time bc insulin is too low to stimulate satiety center
Lipostatic Theory: long-term, weeks/months
Low fat stores
Stimulate feeding center: eat a little extra at each meal → increase lipid stores and increase leptin = stimulate satiety center
Inhibit satiety center
Measuring Energy Use
Direct Calorimetry
Why don’t we use this?
because psychological factors and bigger organisms cause bigger leaks.
people panic about small spaces → feel like they’re put in a box
O2 consumption
LO2/hour x kcal/LO2
assumes all rxns are aerobic
assumes you’re using all O2 right now for current needs, and none is stored
Respiratory Quotient
gives estimate of calories an individual is burning
CO2/O2
Carbohydrates = 1
Proteins = 0.8
Fats = 0.7
Metabolic Rate Factors
Basal Metabolic Rate
Taken while resting/fasting. must be awake.
Age (younger): 5 year old has a higher rate than a 60 year old bc lower body mass and lots of energy is being used for growing
Gender (males): males generally have higher rates than females
Lean Muscle Mass (more): more lean muscle = higher metabolic rate
Hormones
Resting Metabolic Rate
taken when awake and not fasting
Metabolism
Activity level (more): high rate
Diet induced thermogenesis (proteins): creating heat = high metabolism. proteins take more energy to digest
Temperature Homeostasis
Temperature increase
Exercise
Diet induced
thermogenesis
Circadian rhythms
Hormonal cycles
Environment
Temperature decrease
Environment
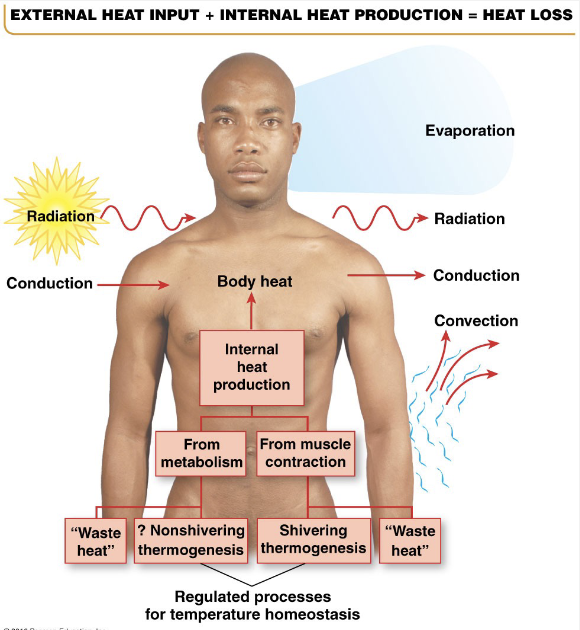
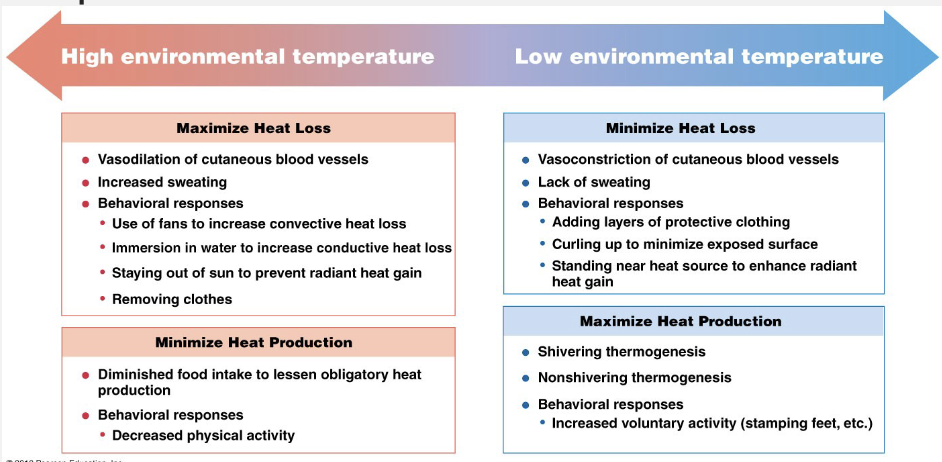
Regulation of Temperature
Increase or decrease
Blood flow
Behavioral adaptations
Decrease
Sweating
Increase
Shivering
Regulation and Set Point
Set Points
Increase → fever
Decrease → hot flash
Imbalances → no longer in set point range
Too hot
Heat exhaustion → sweating increases, red skin, lightheadedness/fainting, barely above setpoint
Heat stroke → no longer sweating, temp rapidly increases, delirious
Malignant Hyperthermia → can’t signal correctly to maintain homeostasis
Too cold
Hypothermia: can start at 70 degrees
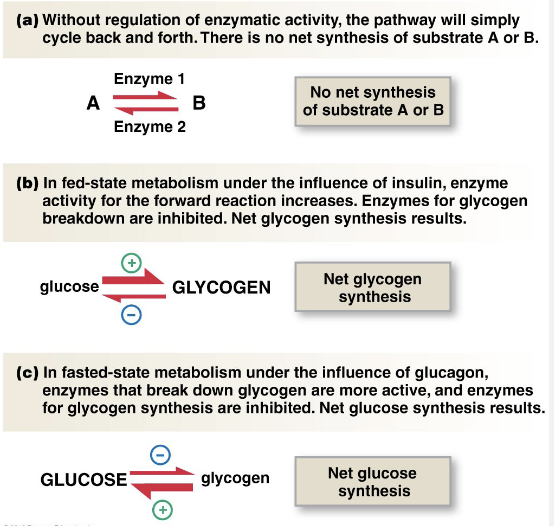
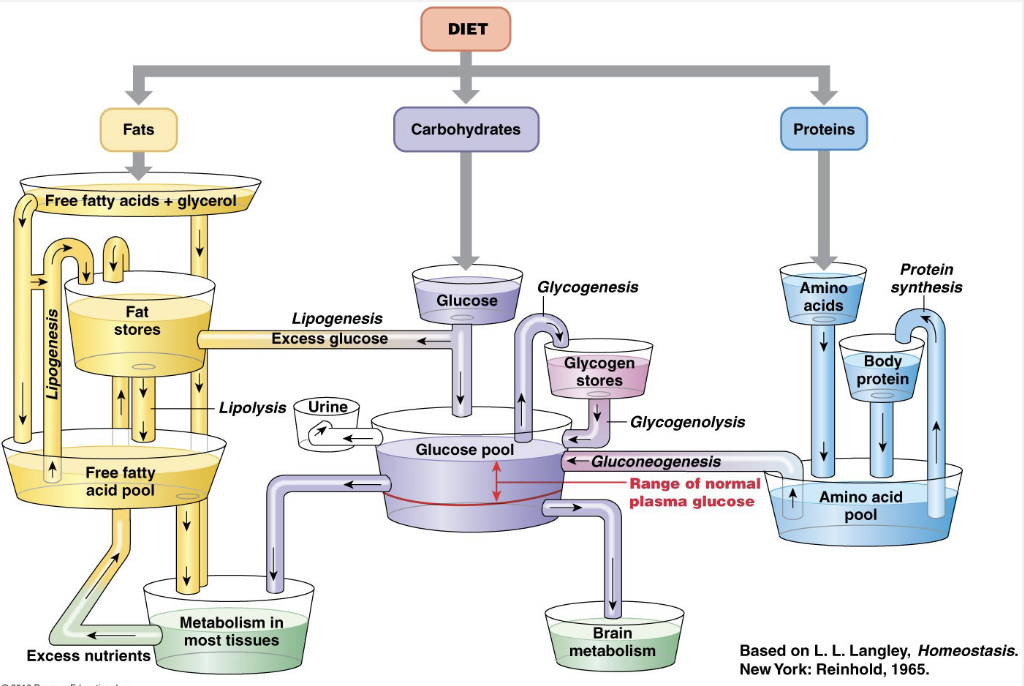
Metabolism: Fed/Absorptive State
Energy: (carbohydrates)
Synthesis (proteins) → repair, rebuilding, synthesis
Storage (fats and carbohydrates) → excess carbs go to storage
Storage = glycogenesis: glucose → glycogen
Synthesis: glycogenolysis: glycogen → glucose
Metabolism: Fasted/Post-Absorptive State
Catabolic Reactions: breaking down
which rxns release energy?
glycogenolysis: glycogen → glucose
lipolysis
protein degradation → only occurs during prolonged fasting
Anabolic reactions
Gluconeogenesis: production of new glucose
breaking down lipids and proteins to make glucose
mostly used by brain
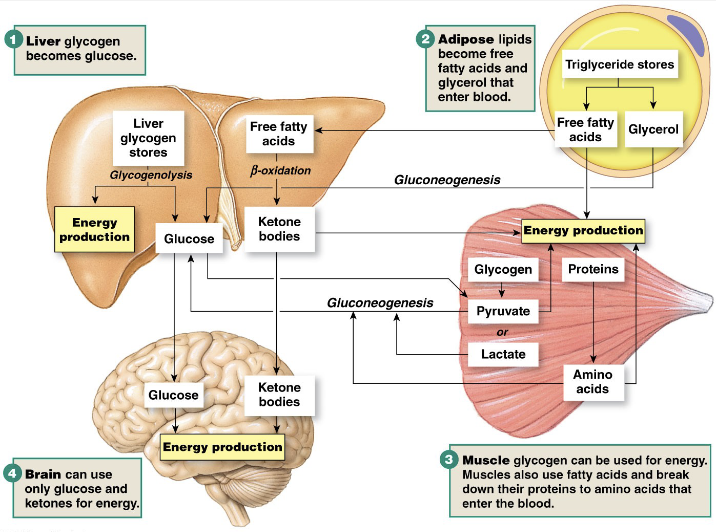
Metabolism Overview (Image)
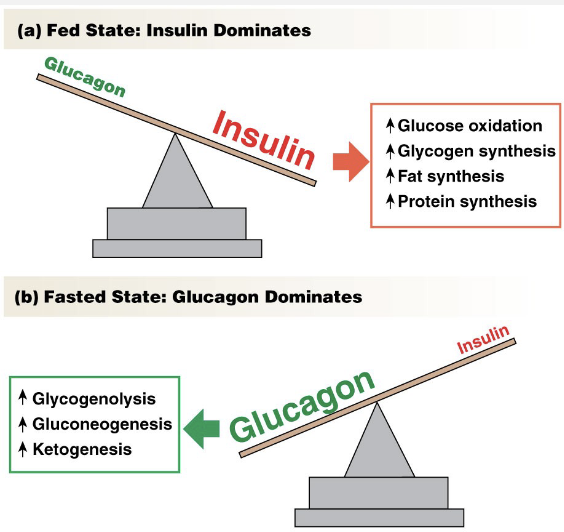
Control of Metabolism: Hormones
Pancreatic Hormones
Insulin → released in fed state
Decreases glucose levels
Promotes anabolic reactions → synthesis/building
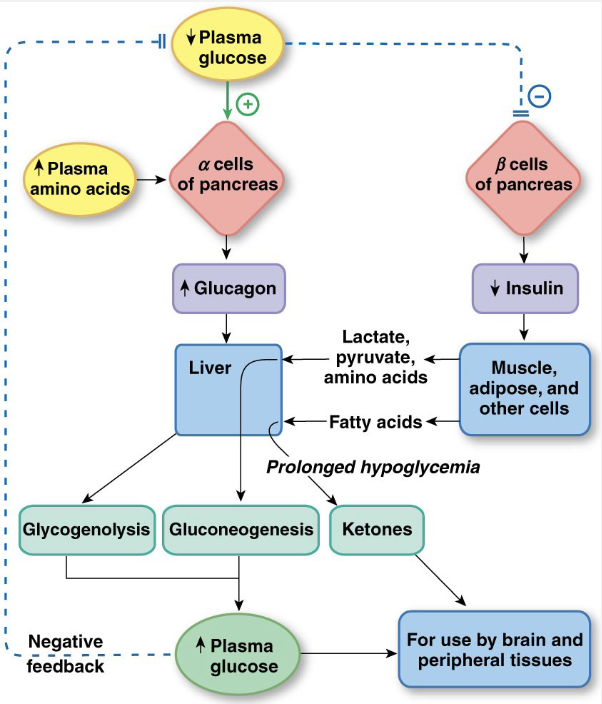
Glucagon → released in hungry state
Increases glucose levels
Promotes catabolic reactions
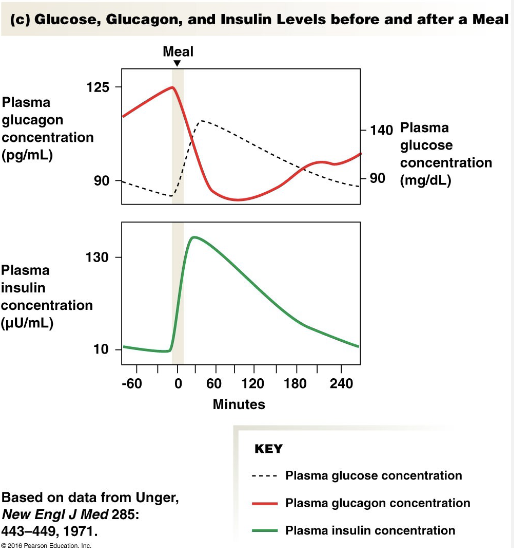
Insulin Stimuli
Increased Glucose Concentrations
Increased Amino Acid Concentrations
GIP Secretion: Glucose-dependent Insulinotropic Peptide
Parasympathetic Stimulation → Sympathetic Division inhibits
Glucagon-like Peptide 1 (GLP-1) Secretion
released by small intestine when glucose is in GI tract
if glucose is in intestine, it will be a short time before it’s in the blood.
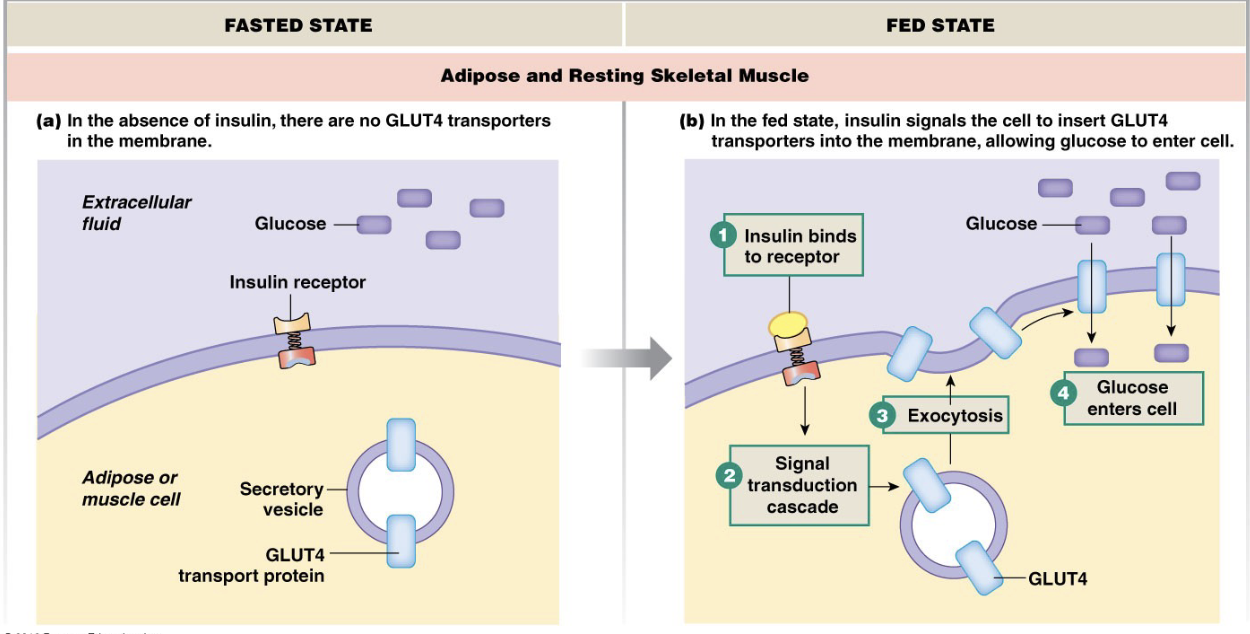
Mechanism of Insulin’s Effects
The brain (with exception of satiety center) doesn’t require insulin to take up glucose
if exercising, it causes skeletal muscle to insert glucose transporters
Glucagon
Antagonist to insulin
Increases glucose
Glycogenolysis
Lipolysis
these two release stored energy
Gluconeogenesis: uses breakdown products of lipids and proteins to make glucose
under starvation conditions, breaks down proteins
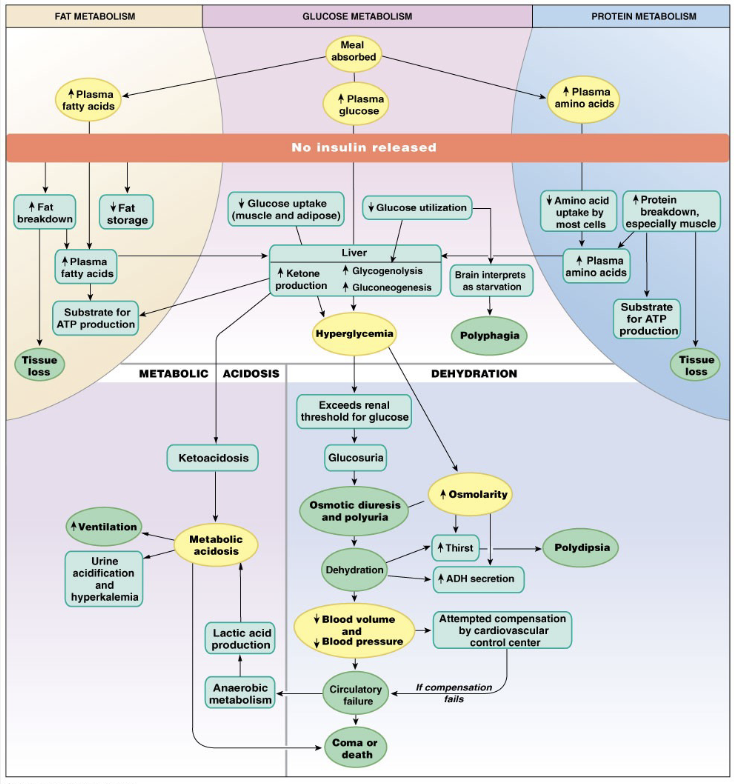
Type I Diabetes Mellitus
not enough insulin production
polyphagia: always hungry bc no stimulus going to satiety center
polyuria: frequent urination → glucose pulls water out of urine, increasing blood osmolarity
polydipsia: always thirsty → increasing blood osmolarity bc increased blood sugar and decreased volume due to frequent urination.
decreased blood pressure and blood volume causes decreased circulation = coma or death
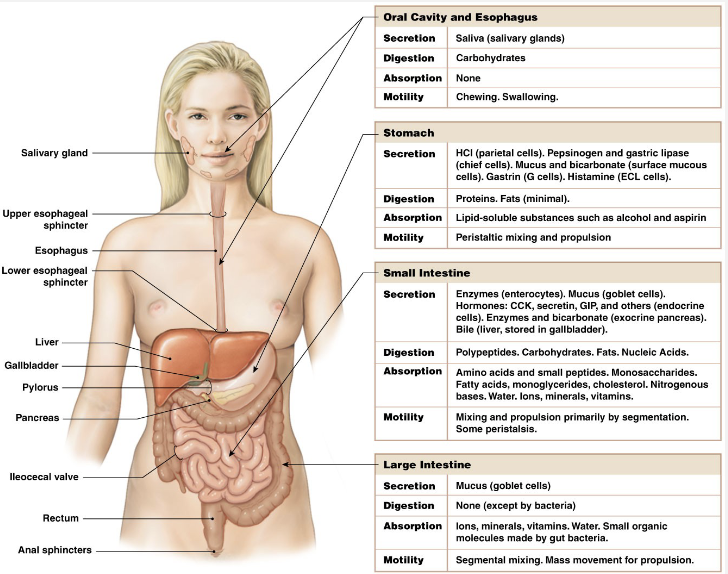
Phases of Digestion
focus on hormone productions in each phase
Cephalic
It’s all in the head
Gastric
Food in stomach
Intestinal
Food in intestines
Motility, secretion, digestion, and absorption for each phase
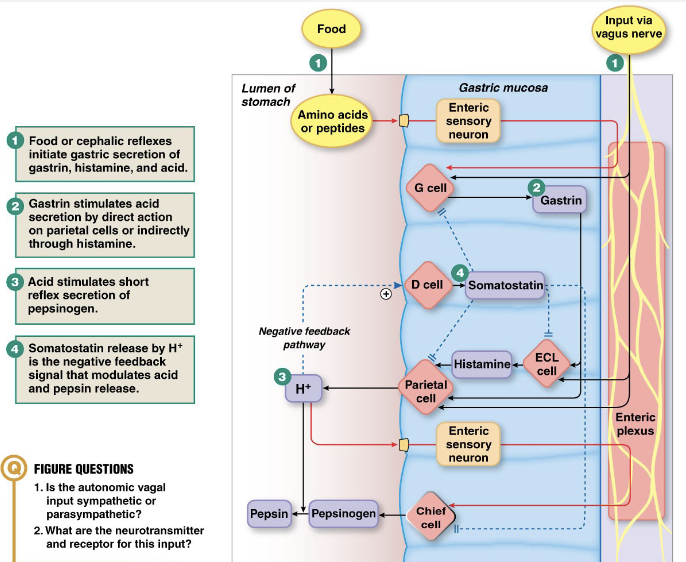
Gastric Phase: Stimuli and Effects
Stimuli
Peptides or amino acids in stomach, stretch, signals from CNS (cephalic phase)
Effects
Increased motility
Increased secretion of enzymes and hormones
Gastric Phase: Motility and Secretions
Motility:
Peristalsis and movement of food to intestines
Pyloric valve /sphincter
Secretions
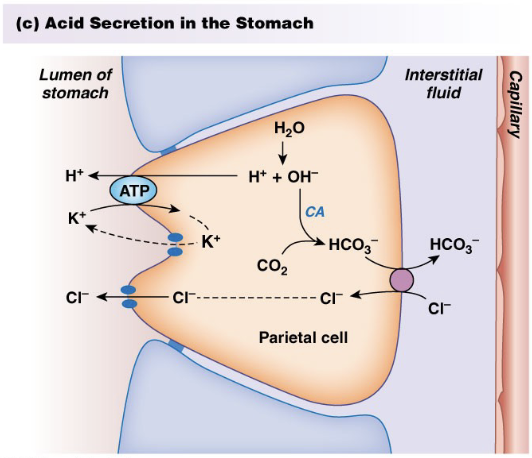
Acid, intrinsic factor
Pepsinogen (proteins), gastric lipase (fats) ← enzymes
Somatostatin (hormone: inhibits acid secretion)
Gastrin (hormone: stimulates acid secretion) → causes protein degradation making them easier to digest
mucus and bicarbonate: protects stomach from acid (buffer
Gastric Phase: Digestion and Absorption
Digestion
Proteins (acid, pepsin)
Fats (gastric lipase)
Absorption
Alcohol, Lipophilic drugs (aspirin): rate of alcohol consumption and % alcohol affect absorption because they create a concentration gradient
Very small amounts of water
Intestinal Phase: Stimuli and Effects
Stimuli
Fats, amino acids, carbohydrates, or acid in intestine
Effects
Increased motility
Increased secretion of enzymes and hormones
Intestinal Phase: Secretion and Enzymes
Secretion
from intestinal wall, pancreas, and liver
Enzymes
Intestine (brush border enzymes):
peptidases
disaccharidases
enteropeptidase
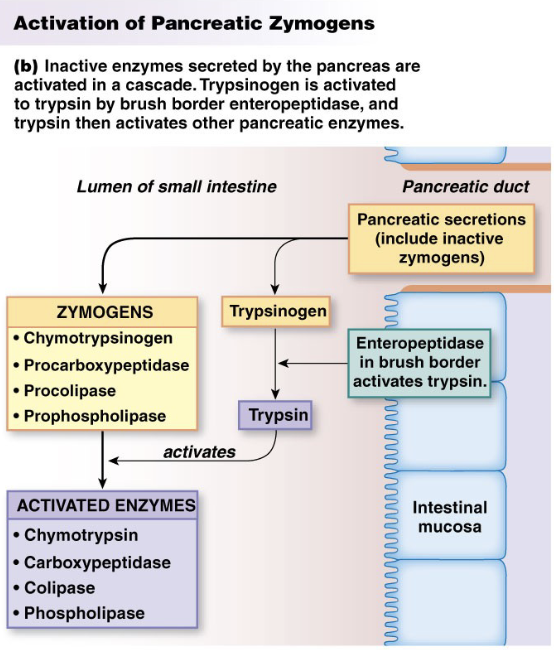
Pancreas:
pancreatic amylase
lipase
proteases
carboxypeptidase and aminopeptidase
Other Digestive Secretions
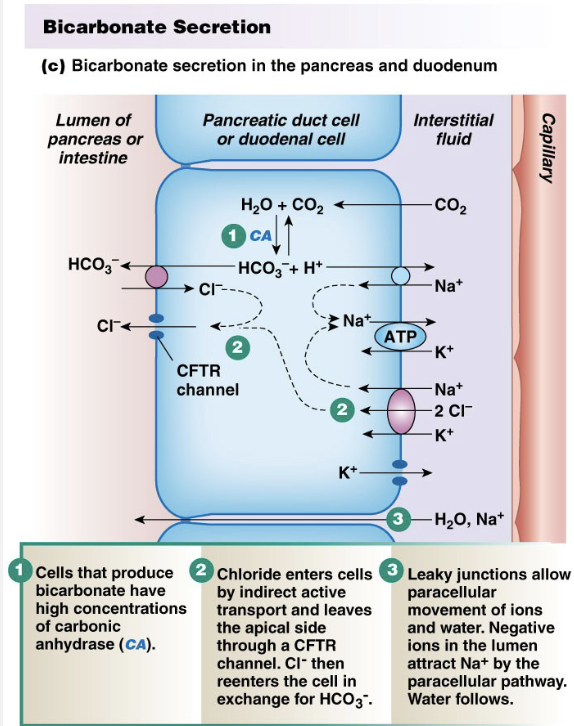
Intestine: mucus, bicarbonate
Pancreas: bicarbonate
Liver: bile (stored in gallbladder as well)
Intestinal Phase: Secretions
Intestinal Hormones
need to know hormone: stimulus: effect
Cholecystokinin (CCK): fatty and amino acids; stimulates pancreatic enzyme release, contractions of gall bladder.
digests fats/proteins and gallbladder releases bile to help digest fats
Secretin: acid in intestine; stimulates bicarbonate release, inhibits gastrin
Glucose-dependent insulinotropic peptide (GIP): glucose, fatty and amino acids; stimulates insulin release, may inhibit acid release
Motilin: fasting; stimulates migrating motor complex
Intestinal Phase; Digestion and Absorption
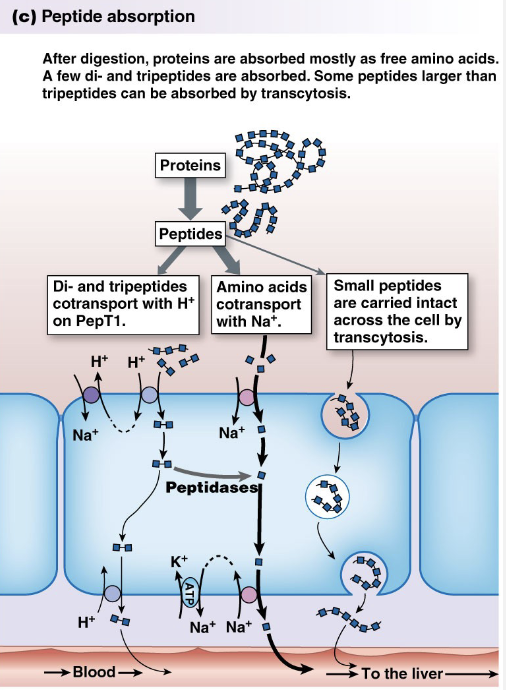
Proteins
Proteases: Trypsin, Chymotrypsin, and peptidases
Amino acids, di and tri-peptides
Transporters absorb larger 3 aa peptides whole via transcytosis after binding to membrane receptors on luminal surface of intestine
Link to newborns and food allergies + immunity bc peptides may act as Ag. If parents delay feeding their infant allergy-inducing peptides, gut has chance to mature, reducing chance of allergy.
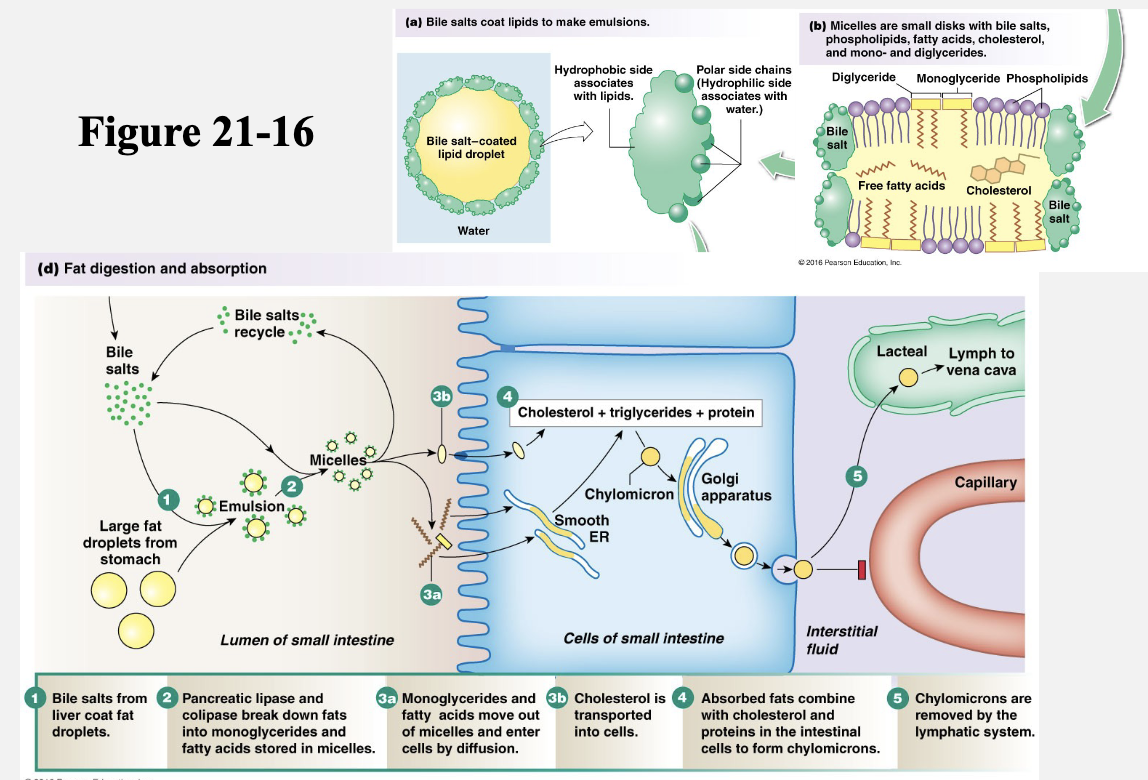
Fats/Lipids → 2nd image
Bile: amphipathic → hydrophobic portion interacts with the surface of lipids and polar side chains interact with water to create water-soluble droplets
Lipase: breaks down triglycerides into a monoglyceride and 2 fatty acid chains
Colipase: lipase can’t penetrate bile salt. Colipase is secreted by the pancreas and acts as a cofactor that displaces bile salts, allowing lipase access to fats inside the bile salt coating.
Free fatty acids and monoglycerides → absorbed via simple diffusion
Multiple stages for digestion
Absorbed by diffusion
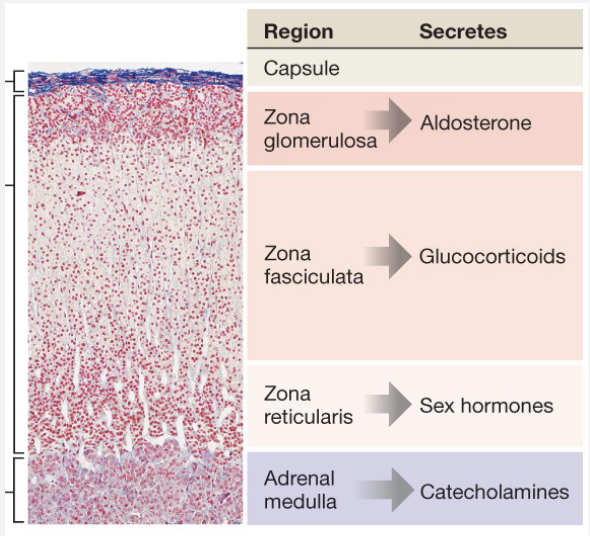
Adrenal Glands
Adrenal Cortex
Outer – aldosterone
Middle – glucocorticoids
Inner – sex hormones
Adrenal Medulla
Catecholamines
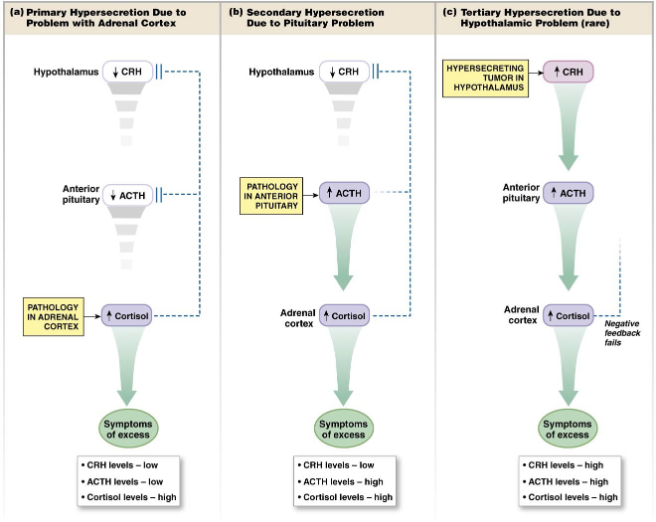
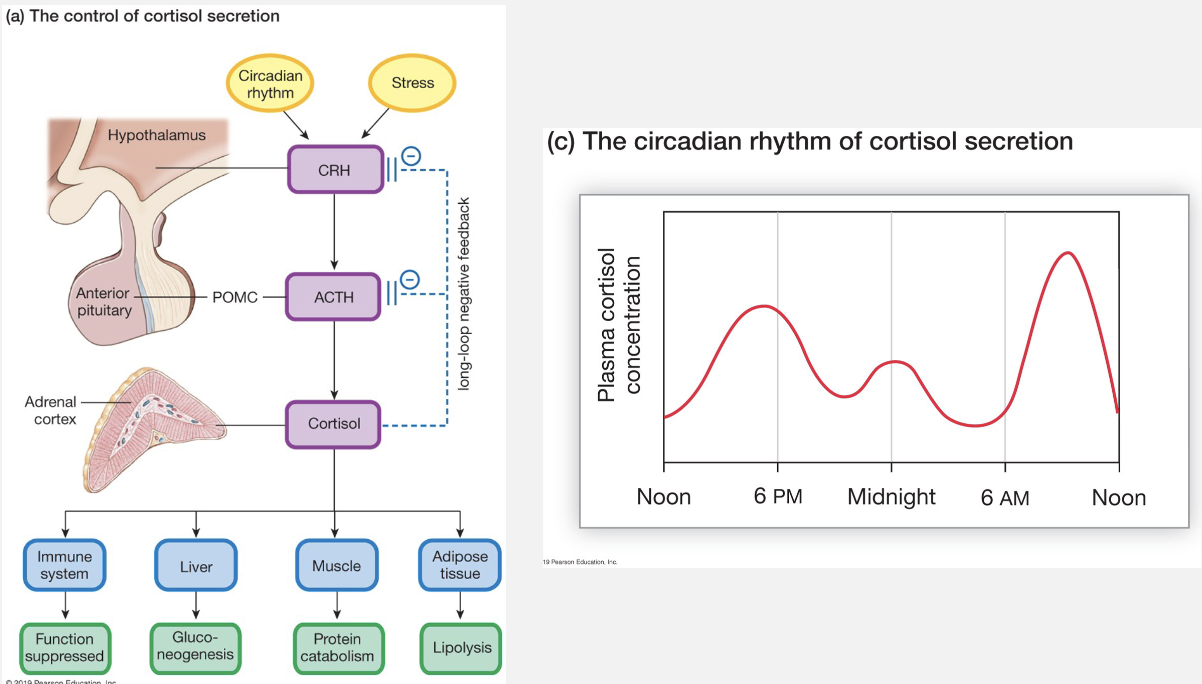
Cortisol
Hypothalamus: secretes CRH (corticotropin-releasing hormone), which is transported to A. Pituitary.
A. Pituitary: secretes ACTH (adrenocorticotropin hormone), stimulates adrenal cortex to synthesize and release cortisol
Adrenal Cortex: produces Cortisol, which acts in a negative feedback loop to inhibit CRH and ACTH
Effects of Cortisol
Gluconeogenesis: in liver. Some glucose produced in liver is released into the blood and the rest is stored as glycogen → prevents hypoglycemia
Catabolism of skeletal muscle: breaks down skeletal muscle proteins to provide substrate for gluconeogenesis
Lipolysis: enhances lipolysis so fatty acids are available to peripheral tissues for energy. Glycerol from the fatty acids is used for gluconeogenesis
Suppress immune system: inhibits release of cytokines and blocks Ab production by wbc’s. Decreases inflammatory response by inhibiting leukocyte mobility. Immunosuppressant → treats inflammation from bee stings, poison ivy, etc, and is effecting in preventing transplant rejection
Catabolism of bones: decreases intestinal Ca2+ absorption, increases renal Ca2+ excretion = net Ca2+ loss. Cortisol causes net breakdown of calcified bone matrix. People who take therapeutic cortisol for long periods have higher frequency of broken bones
Permissive for glucagon and epinephrine: because it’s required for full glucagon/catecholamine activity.
What happens if you take cortisol blockers?
can treat Cushing Syndrome (hypersecretion of cortisol)
reduced gluconeogenesis → hypoglycemia
decreased vasoconstriction → low bp
increased inflammation and autoimmune flare-ups due to reversed immunosuppression
disrupt sleep
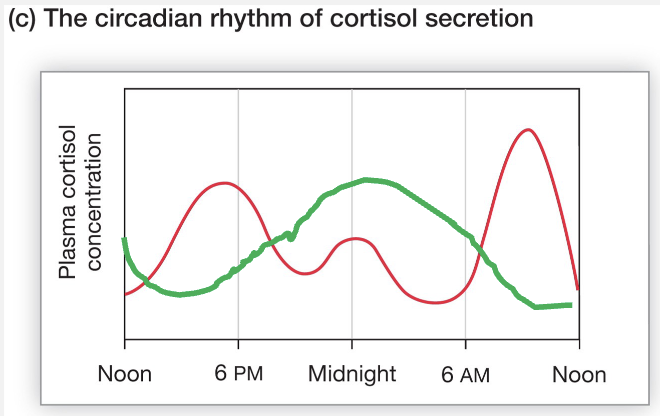
Cortisol Loop and Circadian Rhythm
Cortisol follows a strict 24-hour circadian rhythm, peaking roughly 30–45 minutes after waking (the Cortisol Awakening Response, or CAR) to promote alertness and hitting its lowest point around midnight.
Effects of T3 and T4 (Thyroid Hormones)
In Fetus and early childhood
Full expression of GH
Normal growth
Development of neural system
Affect metabolic rates (all ages)
Increases metabolism and heart rate
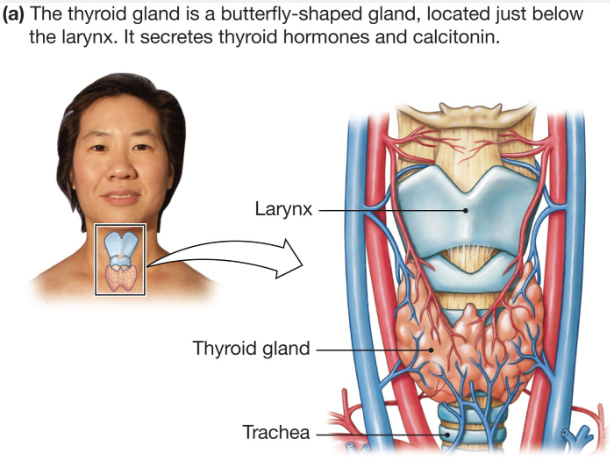
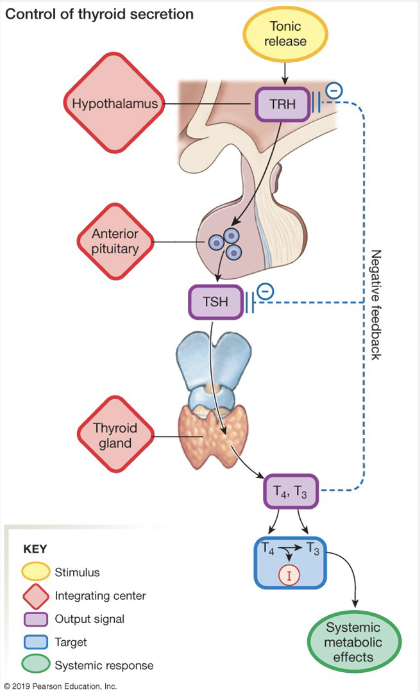
Thyroid Hormone Loop
Hypothalamus: TRH → thyrotropin releasing hormone. controls release of A. Pituitary hormone thyrotropin or TSH
A. Pituitary: TSH → Thyroid-stimulating hormone. acts on thyroid gland to promote synthesis of T3 and T4
Thyroid Gland – T3 and T4 → act as negative feedback and inhibit TRH and TSH to prevent hyper-secretion
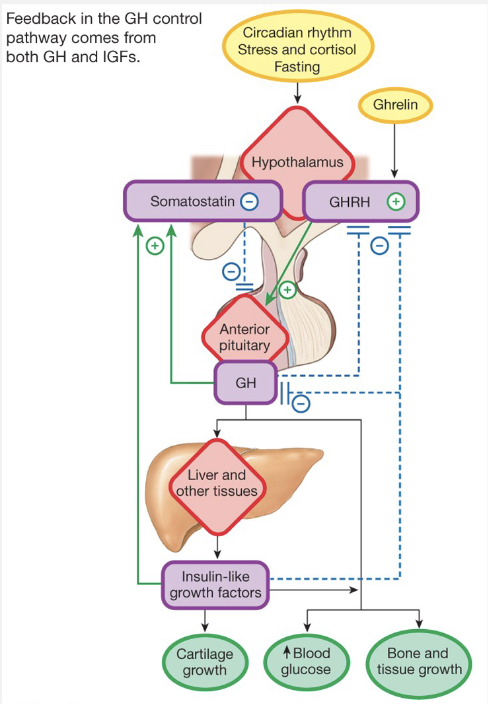
Growth Hormone Loop
Hypothalamus – GHRH, SS (GHIH)
A. Pituitary – GH
Affects growth of tissues, bones
Causes release of insulin-like growth factors
Cortisol – catabolic reactions releasing energy
Growth Hormone – anabolic reactions (building and repairing)
Growth Hormone Pathophysiologies
Dwarfism: Severe growth hormone deficiency in childhood, resulting from problem with GH synthesis or defective GH receptors
Giantism: over-secretion of growth hormone in children. Bone growth stops in late adolescence, but GH can still act on cartilage and soft tissues
Acromegaly: adults with excessive GH secretion causing lengthening of jaw, coarsening of facial features, and growth of hands and feet.
Hormonal Regulation
Anti-diuretic hormone / Vasopressin
Water balance
Aldosterone
Na+, K+ Balance (and water)
Atrial Natriuretic Peptide (ANP)
Na+ Balance (and water)
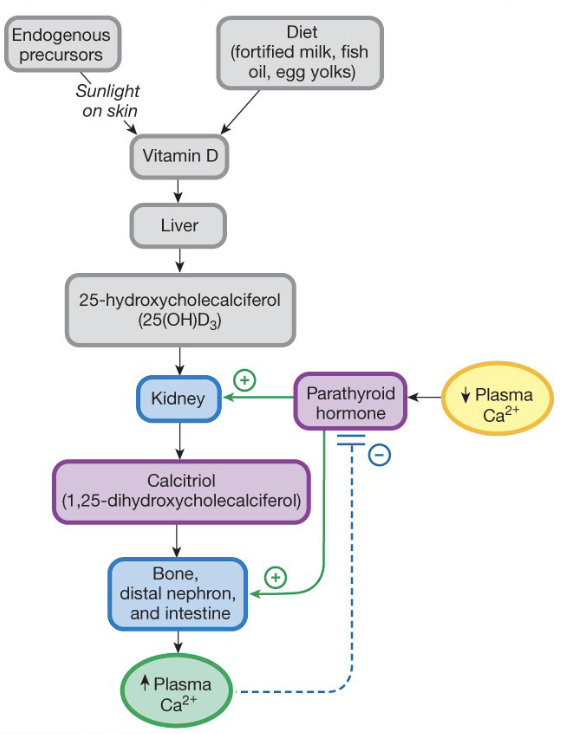
Parathyroid Hormone (PTH) and Calcitriol (D)
Ca2+ Balance
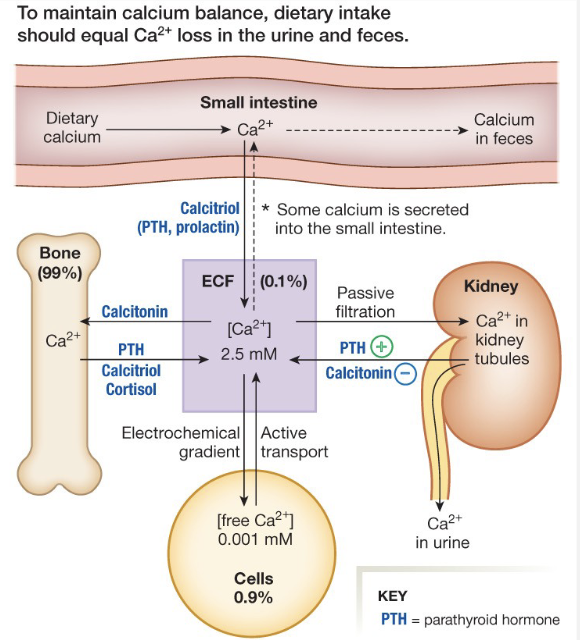
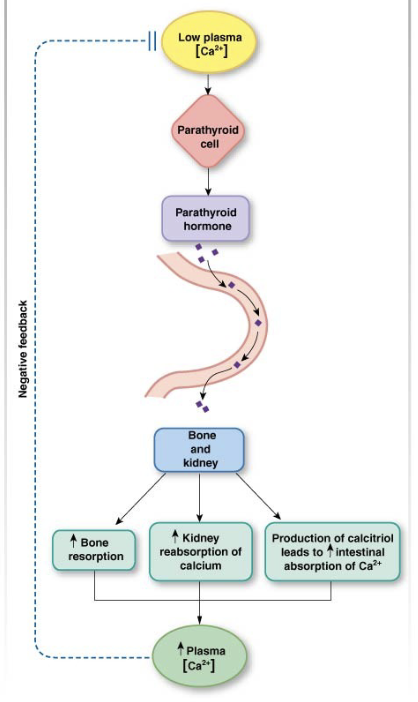
Calcium Balance and Loop
Parathyroid Hormone
Increases Calcium levels
Bone, Kidney, Intestine
Calcitriol (vitamin D)
Reinforces PTH effects
Calcitonin
Decreases Calcium Levels
Bone, Kidney
Reproduction
Sex Determination
• 22 matched pairs of chromosomes
• 1 pair sex chromosomes
• XX- female
• XY- male
• X is required for survival
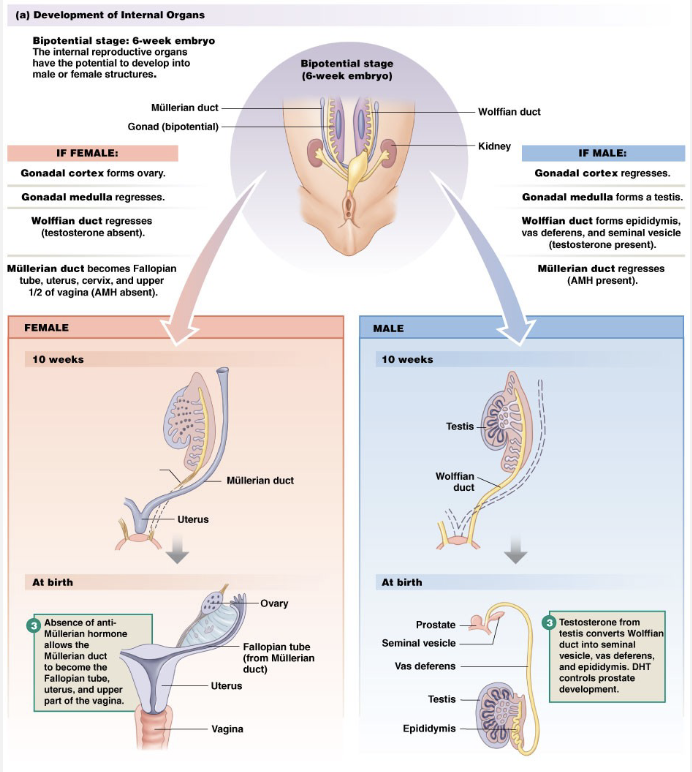
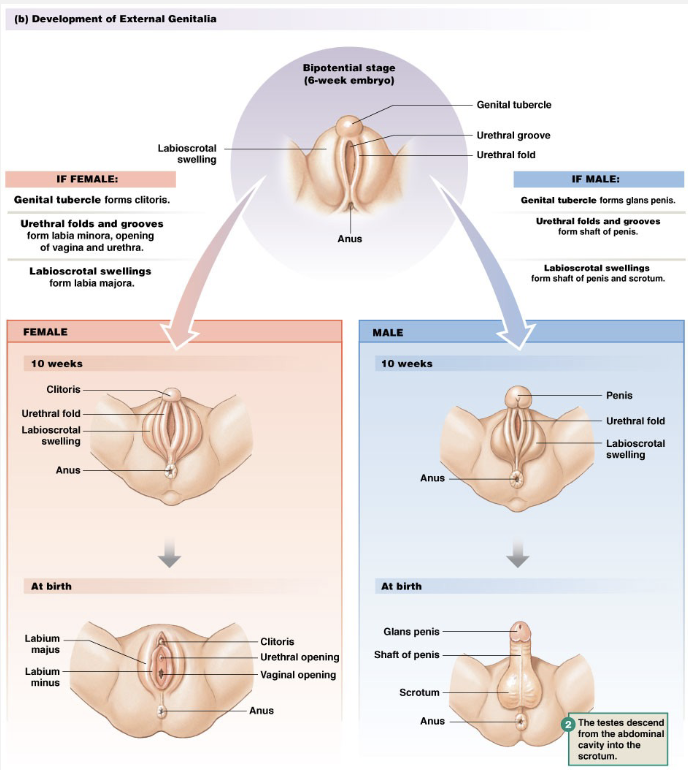
Sexual Differentiation
Male
SRY gene present
Encodes testes determining factor
Testes secrete:
• Mullerian inhibiting substance
• Testosterone and DHTWolffian (mesonephric) ducts converted
Female
No SRY gene
Mullerian (Paramesonephric) ducts form vagina, uterus, fallopian tubes
External genitalia become female
Gametogenesis
Males- sperm
Females – oocytes
Mitosis occurs in embryo for both
Mitosis = 2 identical cells → builds population of cells for division
Each gamete contains one sex chromosome
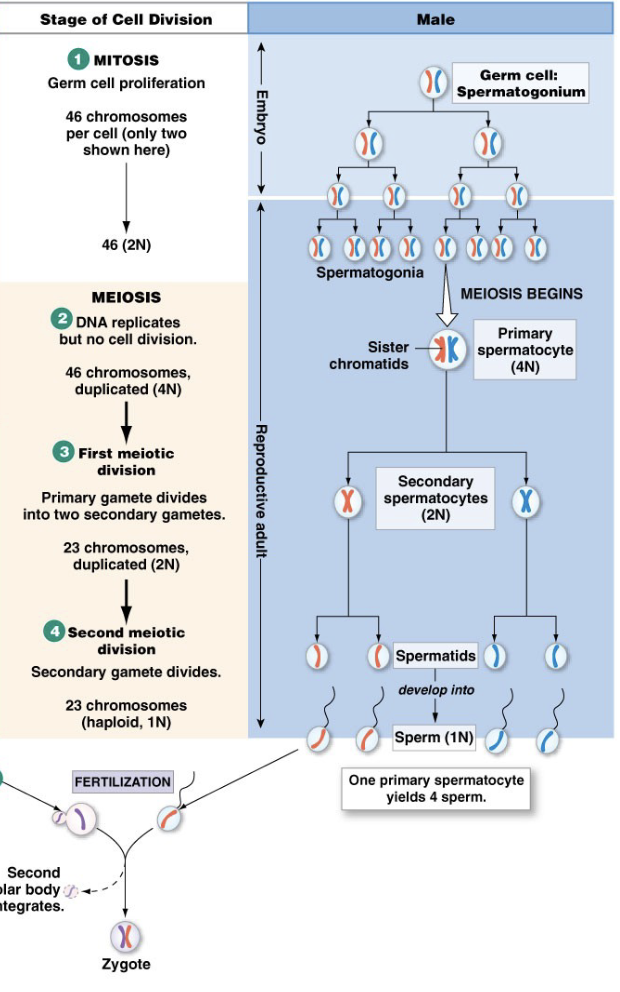
Gametogenesis: Male
Mitotic division starts again at puberty to ensure there are enough primary spermatocytes to produce 100 mil sperm/day as adult
All stages of meiosis occur as adult
Reproductive adult
Takes about 2 months
100 million sperm/day → part of reason for high metabolism in males, lots of energy is dedicated to sexual reproduction
one primary spermatocyte produces 4 sperm
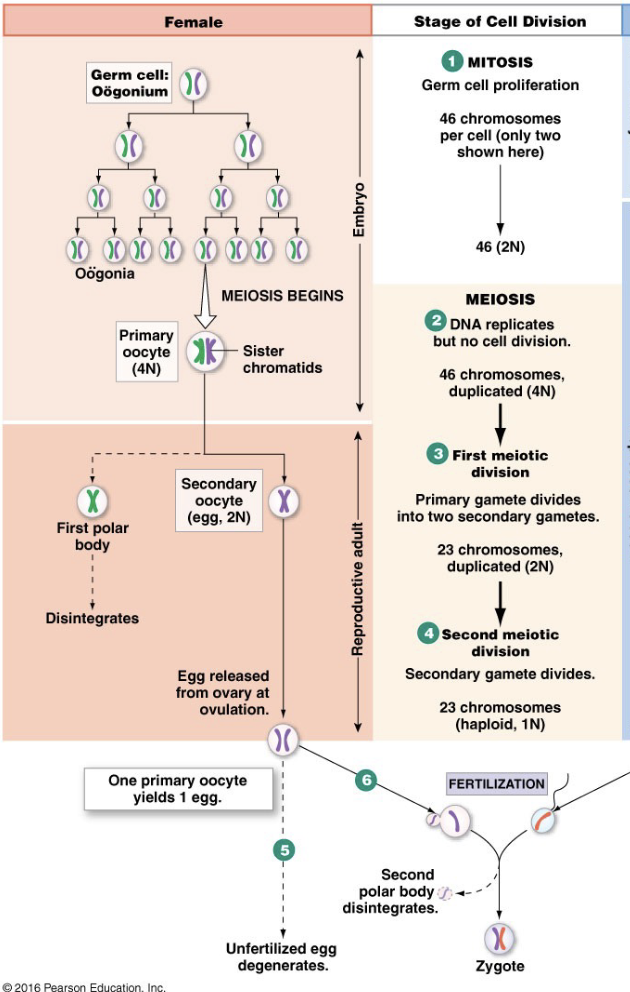
Gametogenesis: Female
Embryo
Mitosis
Meiosis I started (prophase I pause)
when females are born, they will have all of the primary oocytes they will need for the rest of their lives
Reproductive Adult
Meiosis I finishes (1 per month
Secondary oocyte released
Meiosis II starts (pauses in metaphase)
Fertilization
Meiosis II finishes
primary oocyte produces 1 egg and polar bodies
polar bodies = very small cells with half DNA, only purpose of polar body is to take ½ DNA from egg
the egg produced is very large bc it needs to have all resources for development
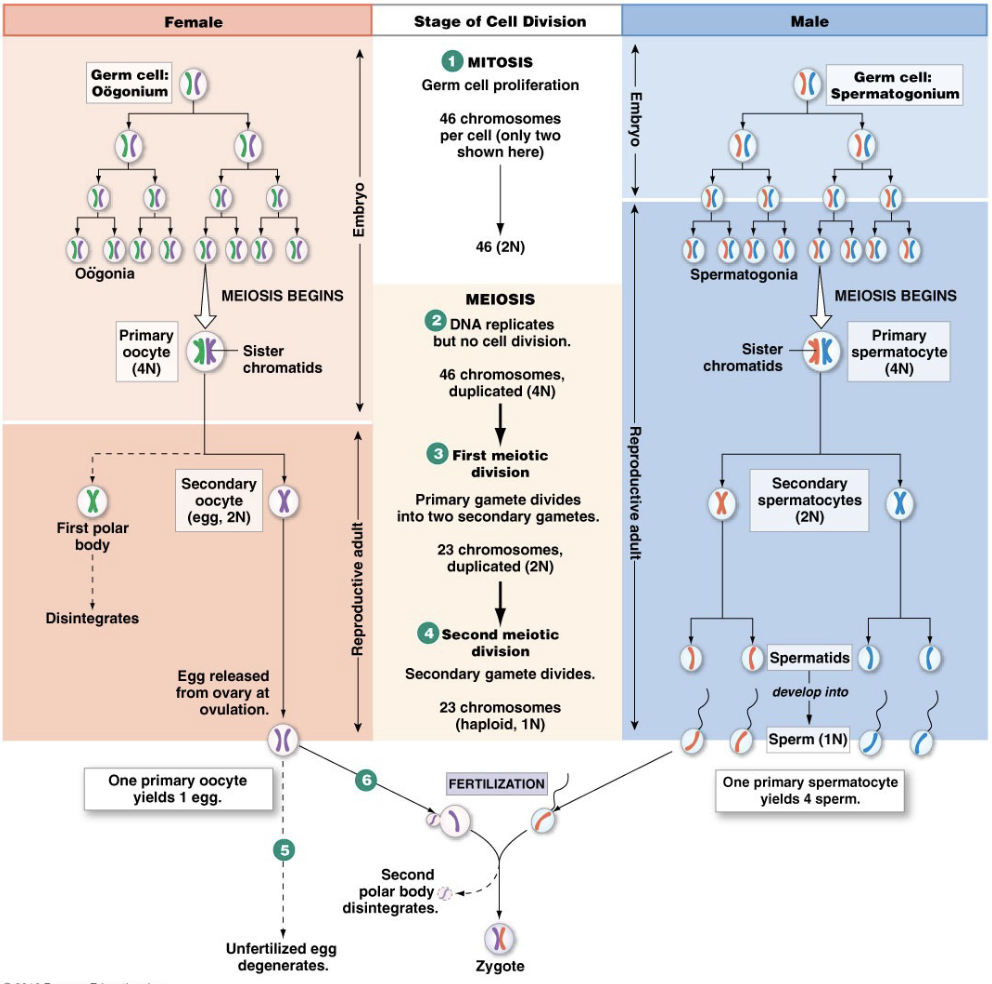
Gametogenesis Differences Between Males and Females
Males
Mitosis in embryo and adult
Meiosis continuous in adult
100-200 million/day
4 sperm/primary gamete
34-35°C → below body temperature, which is why testes descend to be on outside of the body to allow enzymes to function at the cooler temperature for spermatogenesis
Females
Mitosis in embryo only
Finishes only with fertilization
1/month
1 oocyte + 2 (3) polar bodies/gamete
37°C
Hormone Control Loop (Image)
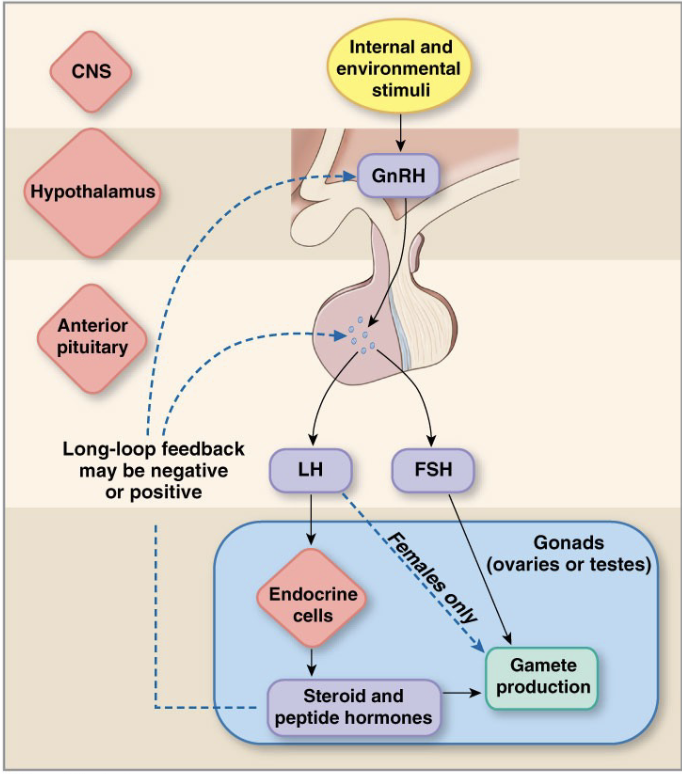
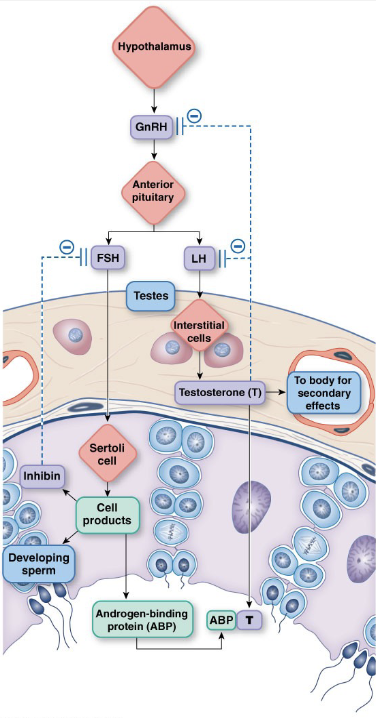
Male Control Loops
GnRH – stimulates FSH and LH
LH → Stimulates Leydig (interstitial) cells to produce testosterone (inhibits GnRH and LH)
FSH → Stimulates Sertoli (nurse, sustentacular) cells to produce sperm and Inhibin
Hormones released in pulses
Circadian Rhythms
Testosterone
Secondary sex characteristics
forms small amounts of estrogen
Why do synthetic androgens cause sterility? Because high testosterone inhibits GnRH and LH, preventing spermatogenesis
What would excess secretion (hyersecretion) of TSH result in?
increased secretion of T3 and T4
decreased secretion of TRH
increased metabolic rates
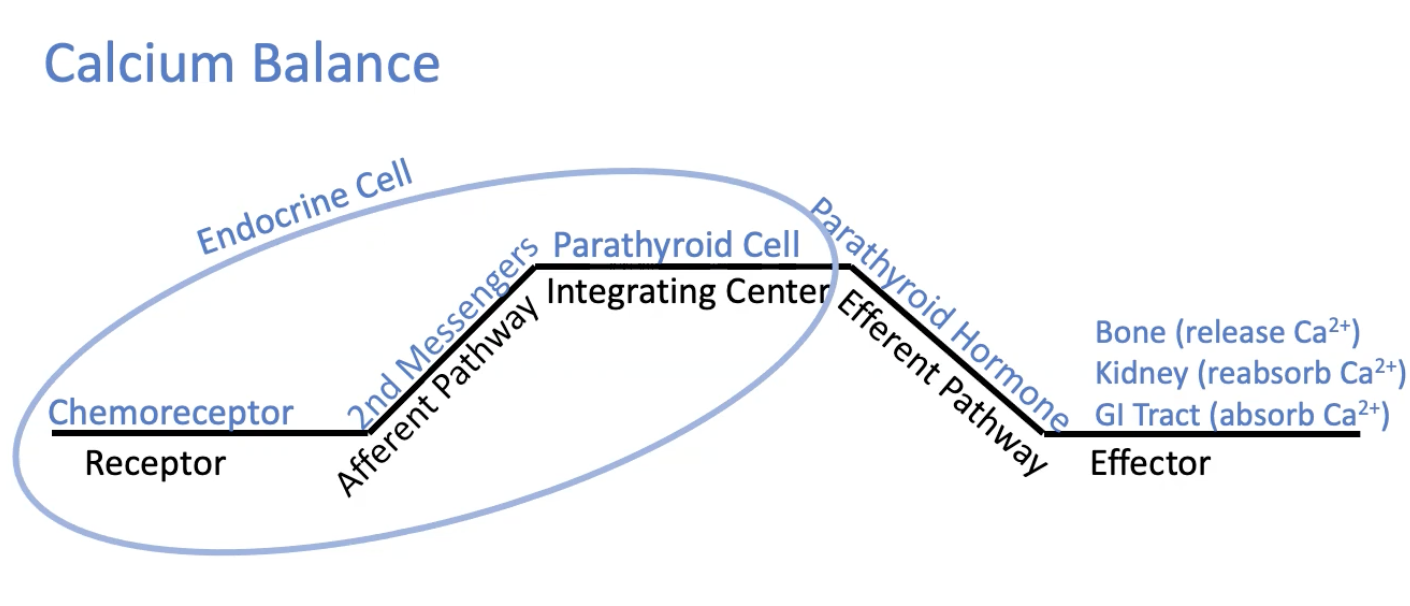
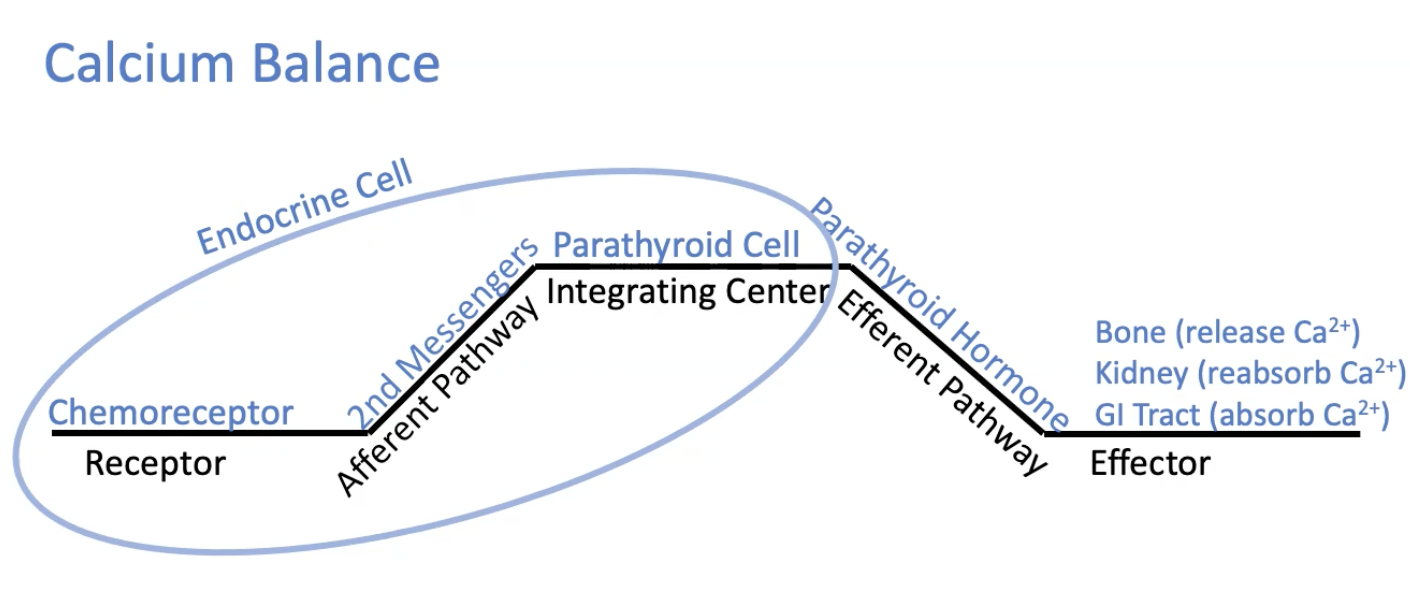
Calcium Balance Feedback loop
The receptor (chemoreceptor), afferent pathway (2nd messengers), and integrating center (parathyroid cell) are all located within the endocrine cell
the efferent pathway = parathyroid hormone
effector = bone (release Ca2+), kidney (reabsorb Ca2+), and GI tract (absorb Ca2+)
What are two characteristics that are true for an endocrine feedback loop but NOT a neural loop?
multiple effectors can be stimulated by a single signal
the first three parts of the feedback loop are contained in a single cell
Why is the posterior pituitary gland not a true endocrine organ?
it does not produce a hormone
Hormones which have long half-lives, utilize intracellular receptors, and are slow-acting may belong to the group known as:
Steroid hormones (e.g., cortisol, aldosterone, sex hormones) are lipid-soluble, so they:
Diffuse across cell membranes
Bind intracellular (cytoplasmic or nuclear) receptors
Directly influence gene transcription
This leads to:
Slow onset of action (requires protein synthesis)
Long half-lives (circulate bound to carrier proteins, reducing degradation)
How do insulin and cortisol act as an antagonistic pair?
Insulin lowers blood glucose by promoting uptake and storage (glycogenesis, lipogenesis).
Cortisol raises blood glucose by promoting gluconeogenesis and reducing glucose uptake in tissues.
→ These effects directly oppose each other.
What could an increase in ACTH cause?
Gluconeogenesis
ACTH (adrenocorticotropic hormone) stimulates the adrenal cortex to release cortisol.
Cortisol is a catabolic hormone that:
Increases gluconeogenesis in the liver
Promotes protein breakdown (not synthesis)
Promotes lipolysis rather than lipogenesis
What could cause low levels of Calcium?
Hypersecretion of calcitonin
Calcitonin lowers blood calcium by:
Inhibiting osteoclast activity (less bone resorption)
Increasing calcium deposition in bone
→ Excess calcitonin can decrease blood Ca²⁺ levels
What makes an endocrine loop simple?
The use of only one hormone
In a simple endocrine reflex, a single endocrine gland both senses the stimulus and secretes the hormone.
There’s no hypothalamus–pituitary cascade involved.
What is the order of events for the male hormone feedback loop?
Release of GnRH
Secretion of LH increases
Gonads increase secretion of testosterone/estrogen/progesterone
Elevated levels of T/E/P create feedback
GnRH and LH levels decrease
What hormone inhibits FSH?
inhibin, produced by the sertoli cells
What is the relationship between estrogen levels, receptors, and responses
higher levels of estrogen are able to bind to receptors with lower affinity for estrogen, stimulating the release of more GnRH and LH
What are the order of events for the female hormone loop?
elevated levels of estrogen stimulate GnRH and LH
LH surge causes ovulation of the oocyte
LH causes the remainder of the follicle to form the corpus lutetium
Corpus luteum releases progesterone, inhibin, and estrogen
Progesterone, inhibin, and estrogen inhibit GnRH, LH, and FSH while waiting to see if pregnancy occurs
When is chorionic gonadotropin released? What does it do?
after implantation occurs and the placenta forms → placenta releases chorionic gonadotropin
human chorionic gonadotropin causes growth of the corpus luteum
Female Control Loops: GnRH, LH, FSH
GnRH- stimulates FSH and LH
LH
Stimulates thecal cells
Forms corpus luteum (along with granulosa)
Peak – ovulation
FSH
Follicle development and granulosa (follicle) cells
Granulosa cells produce estrogen, inhibin
Female Control Loops: Estrogen/Estradiol
Estrogen (Estradiol)
Produced primarily by follicle and at lower amounts by the Corpus luteum
Builds endometrium → layer where implantation occurs
Inhibits GnRH at low levels
Stimulates GnRH at sustained high levels
Secondary sex characteristics (androgens help)
How can positive and negative feedback of GnRH occur with Estrogen?
the key is receptors → determine how cells and tissues respond to hormones
Female Control Loops: Progesterone
Progesterone
Produced primarily by corpus luteum and in lower amounts by follicle
Maintains endometrium with high levels
Inhibits GnRH
Inhibin – inhibits FSH
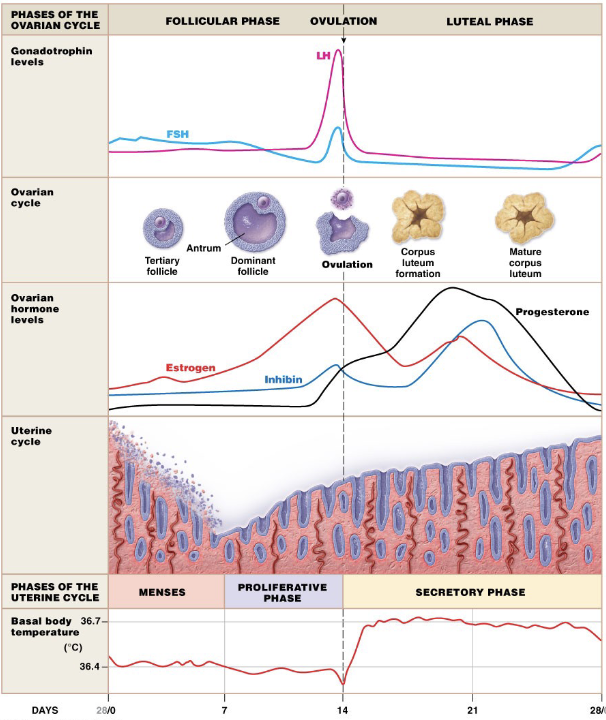
Female Control Loops: Hormonal Cycle
Menses
low progesterone causes shedding of lining
high FSH causes shedding of lining to start over and create a new follicle
Proliferative Phase
high estrogen level → pos. feedback to LH
surge in LH triggers ovulation
Secretory Phase
high progesterone → inhibits GnRH, FSH, and LH
high inhibin → inhibits GnRH, FSH, and LH
oocytes have 24 hours to be fertilized before th hormones drop and the corpus luteum dissolves
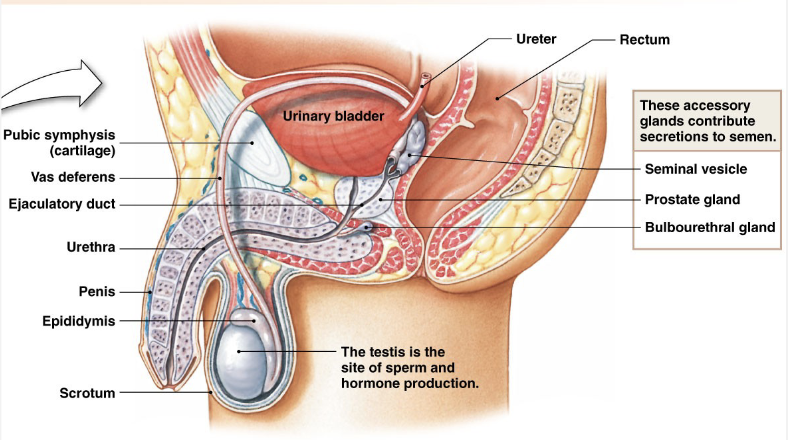
Procreation: Males
Pathway for Sperm
Seminiferous Tubules
Epididymis
Vas (Ductus) Deferens
Urethra
Prostate = joining point of urinary tract and sexual fluid
Composition of Semen
Sperm – gamete
Water – travel medium
Mucus – lubrication → holds sperm in clump
Bicarbonate – buffer → vagina is acidic, it slows the change in pH
Nutrients – cell survival, sperm live 5-6 days in a female
Prostaglandins → motility in the female tract
Glands: Seminal Vesicles, Prostate Gland, Bulbourethral Gland
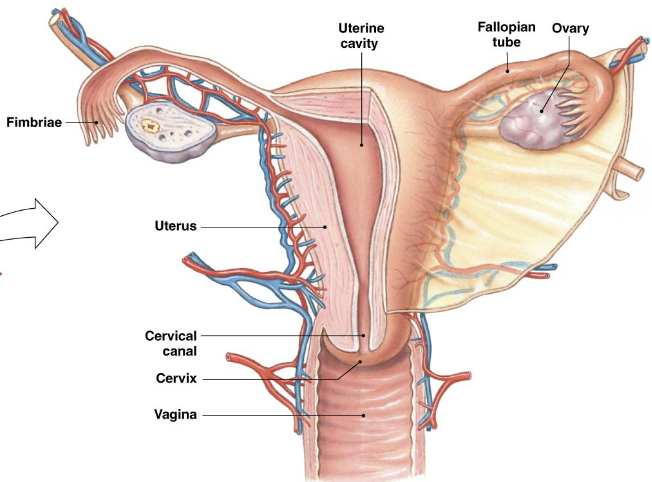
Procreation in females
Pathway for Ova/Eggs
Ovary
Fallopian (Uterine) Tubes/(Oviducts)
Fertilization
Uterus
Pregnancy
Implantation in uterus
Ectopic and Tubal → tubal is most common. Ectopic is any implantation outside the uterus