Final Major Revision
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
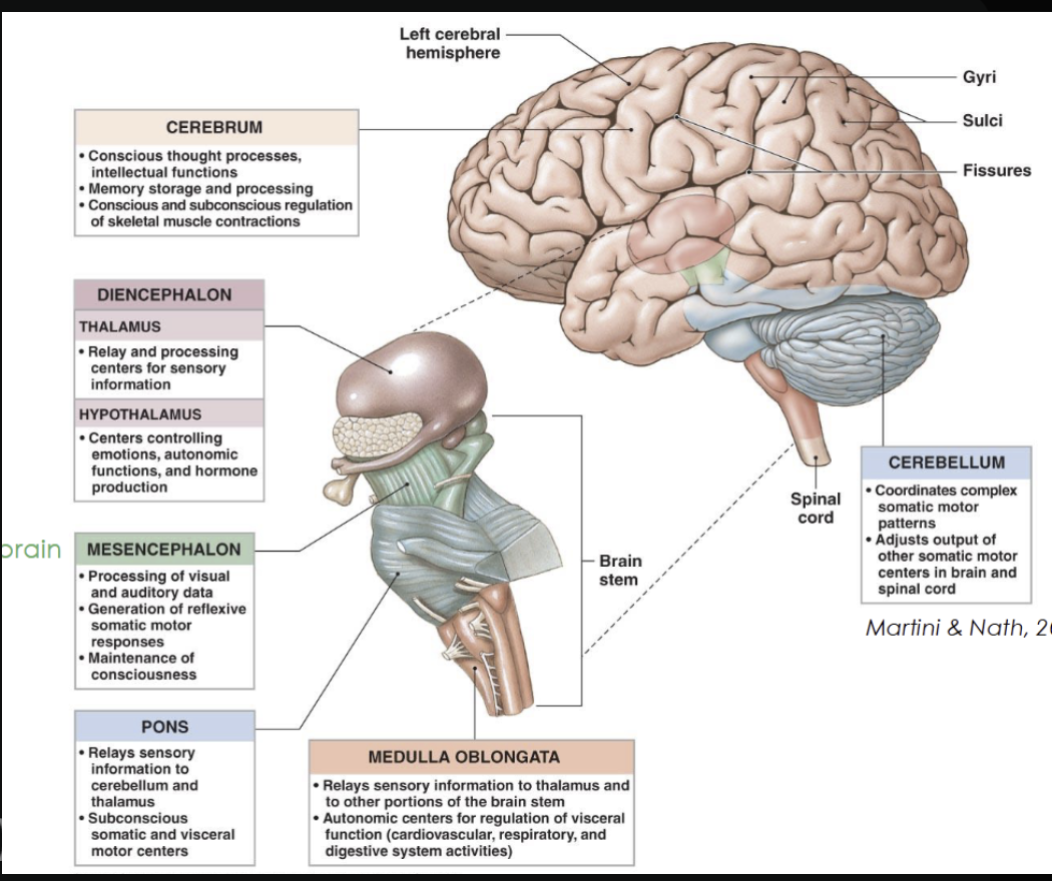
Name the various divisions/regions of the brain and their functions.
Diencephalon
Thalamus → relays sensory information to the cortex
Hypothalamus → maintains homeostasis, and regulates emotions
Epithalamus (pineal gland) → day and night cycles (melatonin produced in response to darkness)
Brainstem
Midbrain → visual and auditory reflexes
Pons → Relays signals between brain regions and regulates sleep and breathing
Medulla oblongata → Controls autonomic functions
Cerebellum
Coordinates movement, balance, and posture (works subconsciously)
Classifications of bones
Long bones
Longer than wide
Help with movement
Examples: femur, humerus
Short bones
Small and cube-shaped (equal length, width, and thickness)
Give stability
Examples: wrist (carpals), ankle (tarsals)
Flat bones
Thin, flat, and usually curved
Protect organs
Examples: skull, ribs, sternum
Irregular bones
Odd-shaped
Have special jobs (support/protection)
Examples: vertebrae, pelvis
Sesamoid bones
Small bones in tendons
Help reduce friction
Example: kneecap (patella)
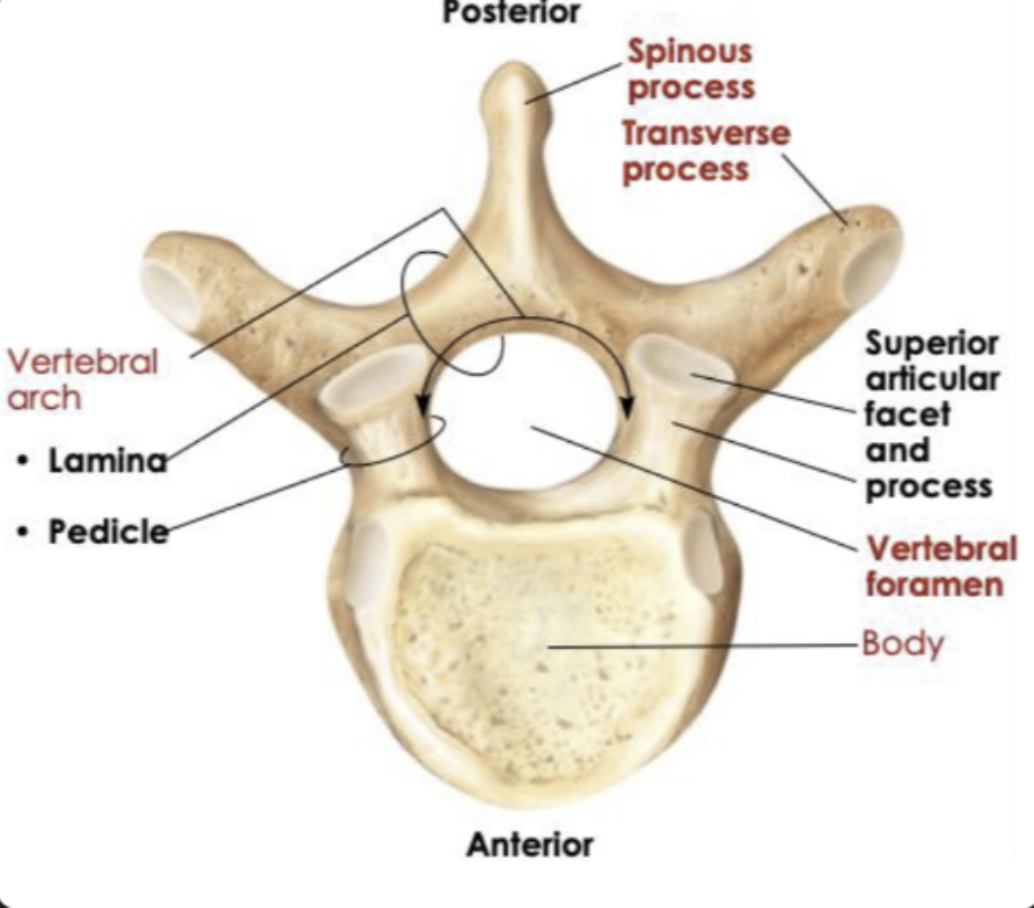
Common structure of all vertebrae
Cervical: Small oval body, large triangular vertebral foramen, small transverse process
Thoracic: Heart shaped body, smaller circular vertebral foramen, large transverse process
Lumbar: Very large, thick oval body, smaller triangular vertebral foramen but bigger than thoracic, short and flat transverse process
Understand changes to the skeleton during development, ageing, and disease.
Bone Development
Starts as cartilage → ossifies in embryo
Long bones: ossification ~8–25 weeks
Growth continues until ~25 years
Age-Related Changes
Children: formation > resorption → growth
Young adults: formation = resorption → stable
Adults: resorption > formation → bone loss
Osteoporosis
Resorption > formation → low bone mass
Common in elderly (especially women)
Prevention: weight-bearing exercise
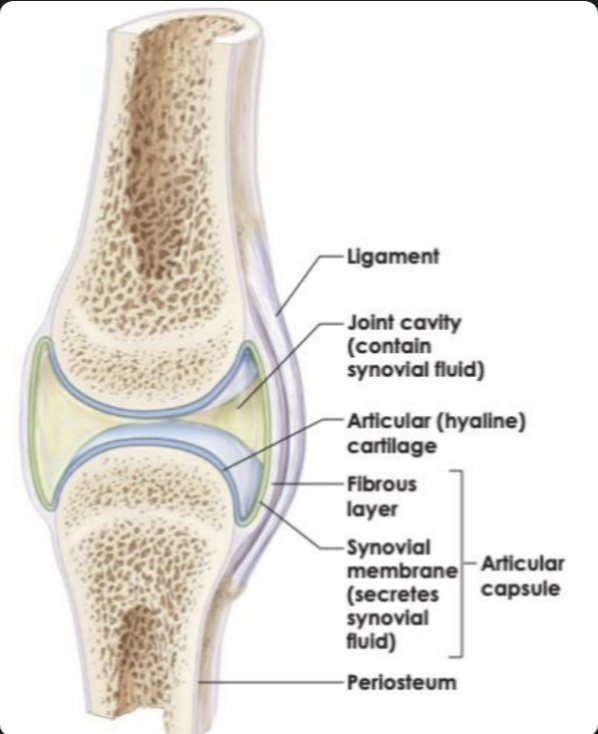
Synovial joint structure
Articular cartilage → reduces friction
Joint cavity → allows movement
Synovial fluid → lubrication
Joint capsule → encloses the joint
Fascicle architecture linked to function
Pennate muscles have fascicles arranged at an angle which produces a reduced range of motion, due to shorter fibre lengths. Whereas, parallel muscles have fibres running parallel to the line of pull with longer fascicles, allowing for a larger range of motion through its longer muscle fascicles.
This results in the Pennate muscles to pack a higher volume of muscle fibres, allowing for higher power (higher PCSA), but less range of motion. With the parallel muscles, its longer muscles makes it where there is less volume of it, reducing its power (lower PCSA), giving it a higher range of motion.
Physiological Cross-Sectional Area - PCSA
Structure that makes up the wall of blood vessels
1. Tunica intima (inner layer)
Endothelium (smooth epithelial lining)
Thin connective tissue layer
Function: smooth blood flow, reduces friction
2. Tunica media (middle layer)
Smooth muscle + elastic fibres
Function: controls vessel diameter (vasoconstriction/vasodilation) and blood pressureThickest in arteries
3. Tunica externa (outer layer)
Connective tissue (collagen + elastin)
May contain small blood vessels (vasa vasorum)
Function: support and anchoring
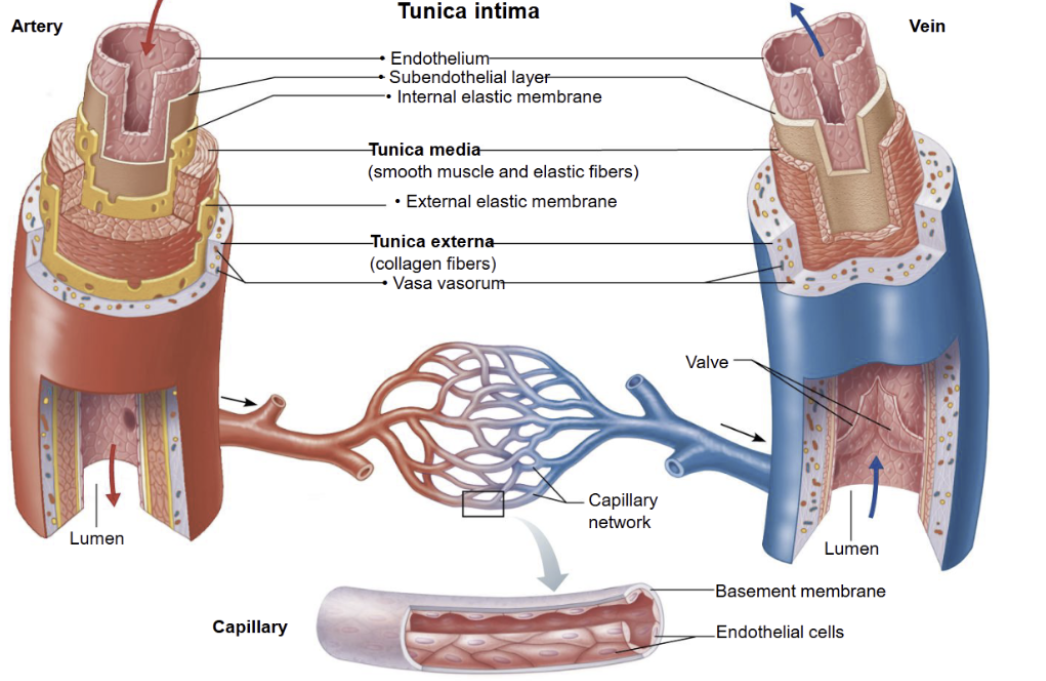
Compare arteries, veins and capillaries
It should be noted:
The pressure is high in arteries as it needs to be pumped throughout the whole body.
Wall thickness is important in arteries as it needs to withstand all that pressure, whereas in veins its doesn’t face such pressure and in capillaries it needs to be thin to allow diffusion.
Lumen affects flow speed, so in arteries it’s narrow to maintain high pressure whereas in veins its wide in order to carry large volumes of blood, and very narrow in capillaries, however due to being arranged in a large cross-sectional area it slows blood down to giving it time for exchange.
The reason valves are present in veins is to prevent backflow.
And as for function, in capillaries especially its is used to exchange gases, nutrients and wastes

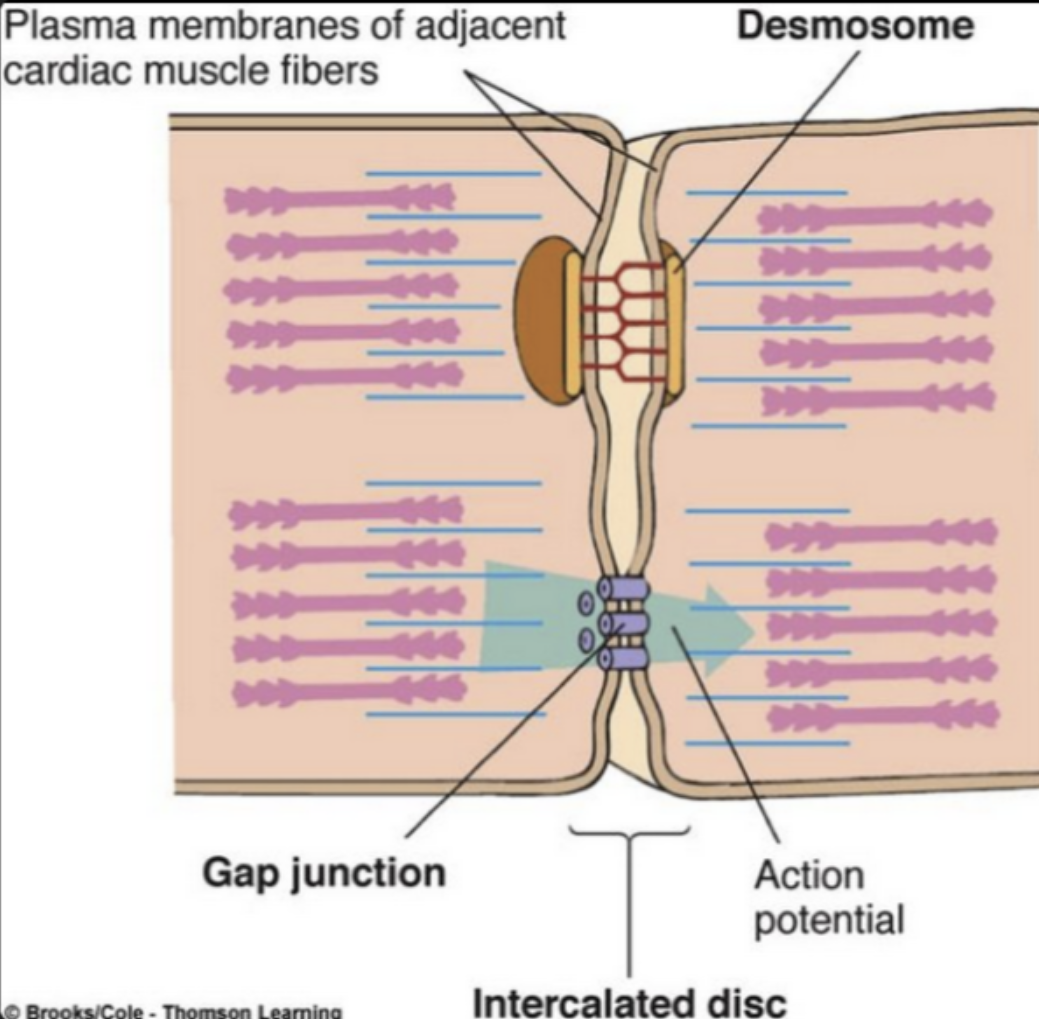
Structure of cardiac muscle its relationship to its function
Structure
Striated cells → contain proteins that cause contractions
Short, branched cells → form a connected network
Intercalated discs (join cells):
Desmosomes → hold the myocytes together
Gap junctions → allow ions & electrical signals to pass through the membrane
Cardiac cells can contract simultaneously due to rapid flow of action potentials between the cardiac myocytes
Relationship to Function
Striations → strong contractions to pump blood
Branching network → rapid spread of contraction
Desmosomes → prevent cells pulling apart during forceful beats
Gap junctions → fast electrical communication, so cells contract together
Important: Cardiac myocyte = cardiac muscle cells
Baroreceptor reflex and the autonomic nervous systems role
Detects changes in blood pressure via stretching of blood vessel walls
Sends signals to the medulla
↑ Blood pressure
↑ firing (too much pressure) → ↑ parasympathetic, ↓ sympathetic
Leads to, ↓ heart rate, vasodilation → BP decreases
↓ Blood pressure
↓ firing (not enough pressure) → ↑ sympathetic, ↓ parasympathetic
Leads to, ↑ heart rate, vasoconstriction → BP increases
The autonomic nervous system adjusts heart rate and vessel diameter to keep blood pressure stable.
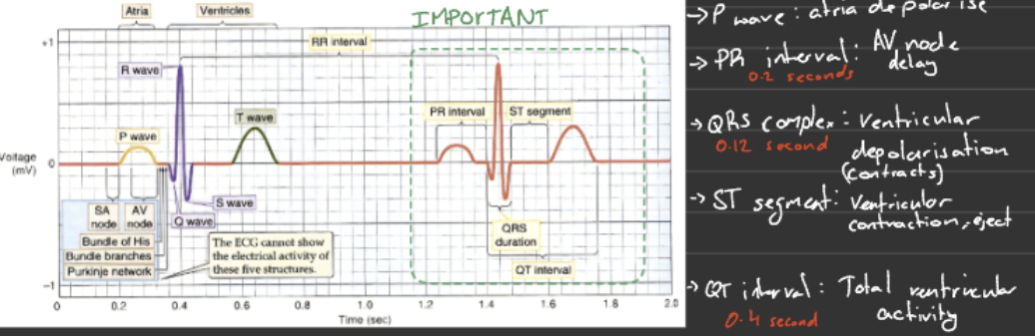
Describe how the ECG correlates with the cardiac cycle
P wave → atria depolarise → atria contract (atrial systole)
PR interval → delay at AV node → ventricles fill with blood
QRS complex → ventricles depolarise → ventricles contract (ventricular systole) - AV valves close
ST segment → ventricular contraction → blood is ejected
T wave → ventricles repolarise → ventricles relax (diastole)
Explain the concept of the mean electrical axis (cardiac axis), what it measures, and how it changes with physiological and pathological factors
The cardiac axis (mean electrical axis) is the average direction of the heart’s ventricular electrical activity during contraction, shown as an angle on an electrocardiogram (ECG).
What it measures:
The net direction of the heart’s electrical activity during ventricular contraction
Represented as an angle in degrees
Key idea:
It summarises all ventricular electrical forces into one main vector
Why it matters:
Helps detect cardiac enlargement or hypertrophy
Identifies conduction defects and some cardiac pathologies
Describe some pathologies that can be detected by ECG
Extrasystoles and sinus arrhythmia → irregular heart rhythms
Supraventricular tachycardia (starts at the atria) and ventricular tachycardia (starts in the ventricles) → abnormally fast heart rates
Heart block → delayed or blocked electrical conduction
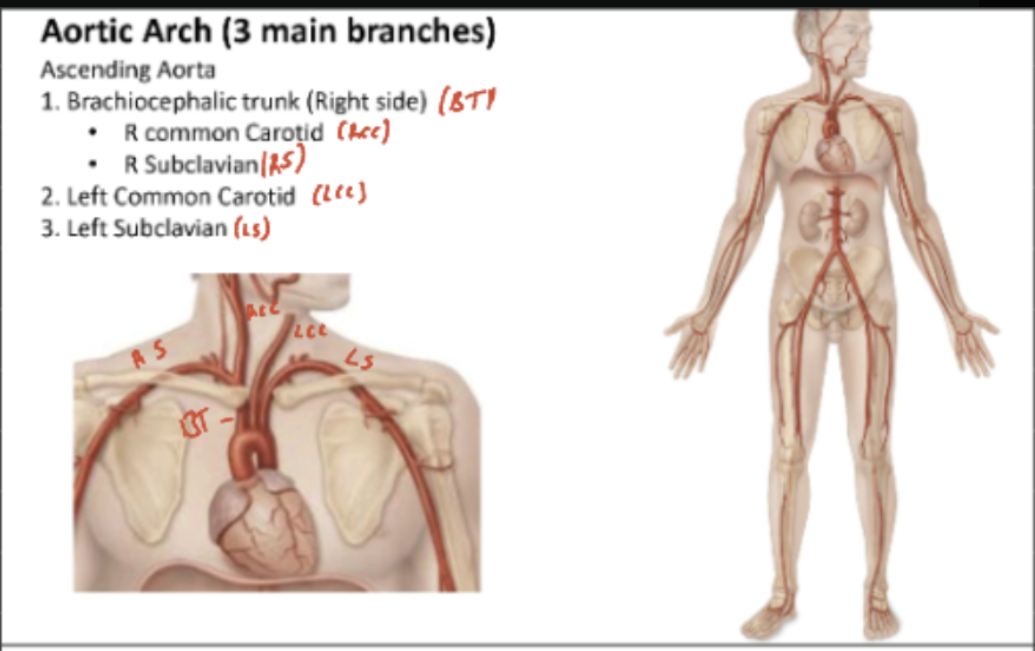
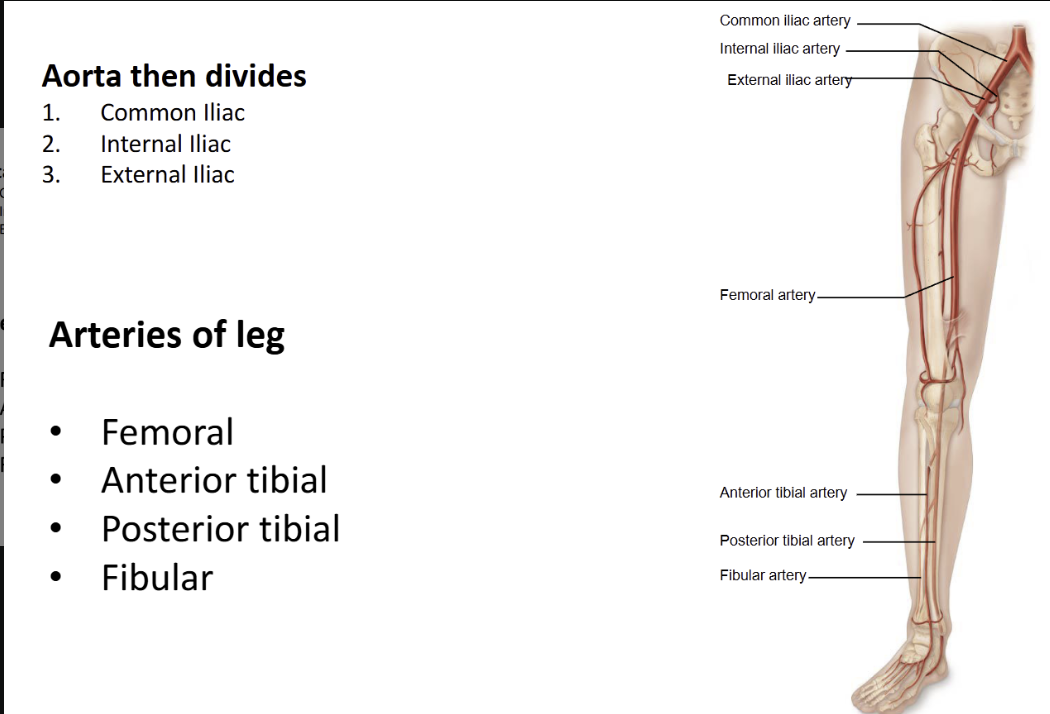
Name the arteries which branch off the Aorta to give rise to the arteries in different regions of the body
Aorta
Ascending Aorta
Descending Aorta
Aortic arch
Name the arteries of the legs
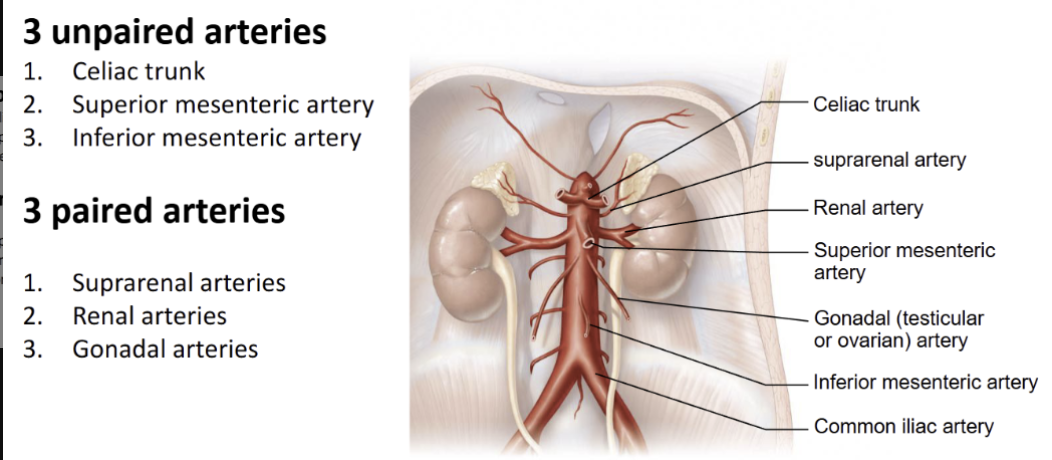
Name the arteries of the torso (paired and unpaired branches from Aorta)
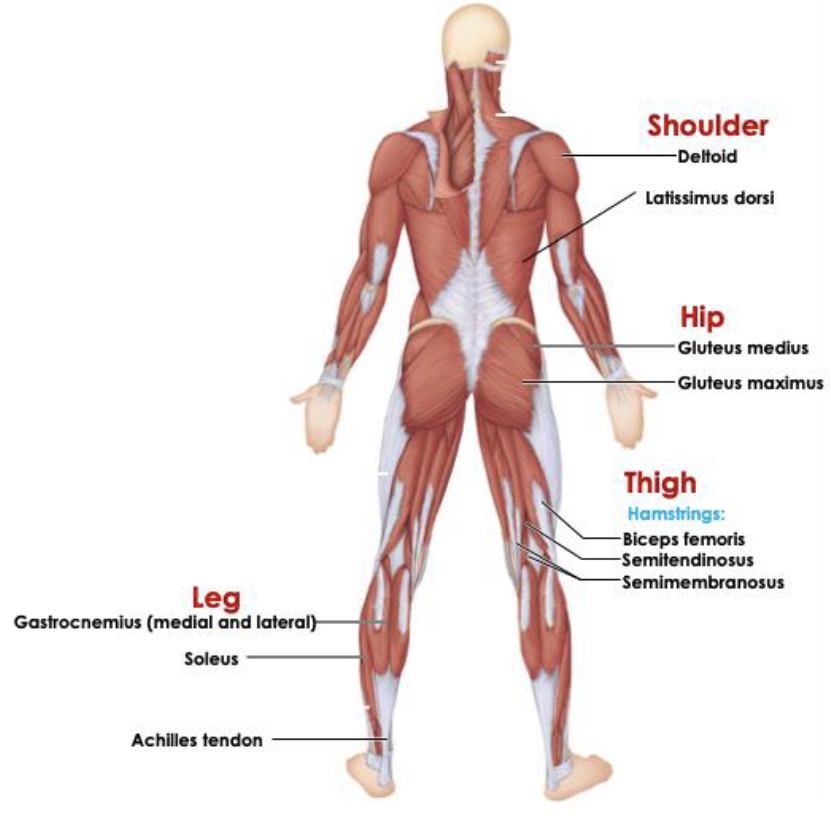
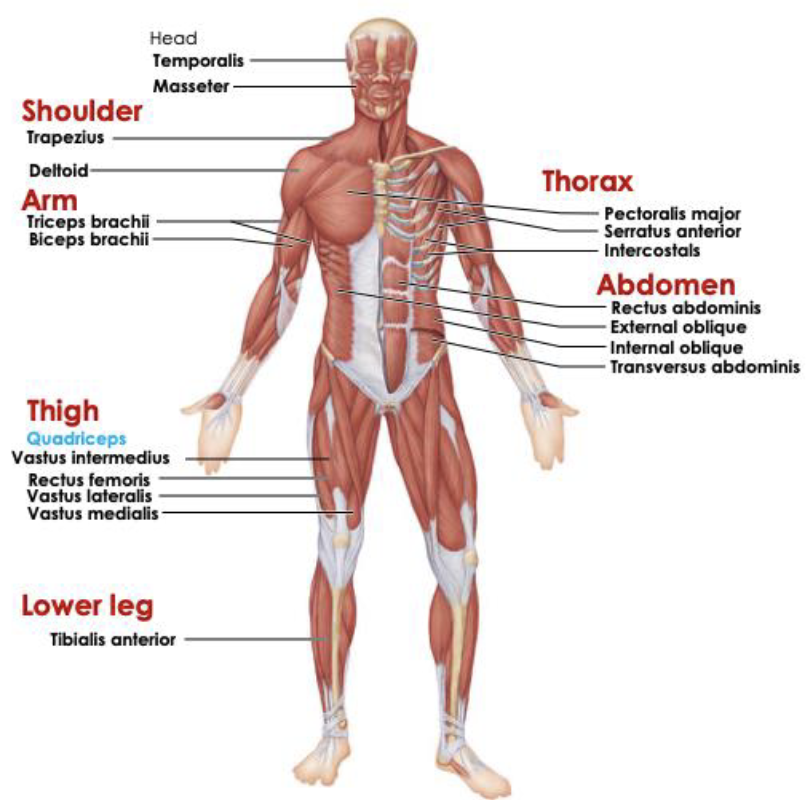
Anterior Muscles
Posterior Muscles