childhood + adolescent psychological problems
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
what are 4 difficulties associated with diagnosis psychological problems in childhood
children may struggle to communicate how they feel → may describe somatic symptoms rather than psychological, making accurate diagnosis challenging
children go through different developmental stages at different ages, and symptoms change with time → what constitutes as atypical behaviour may depend on child’s age
labelling theory → diagnosis may cause conformity to that label
cultural norms → differences in behavioural norms means that some societies will class behaviours as pathological, whether others would regard them as normal
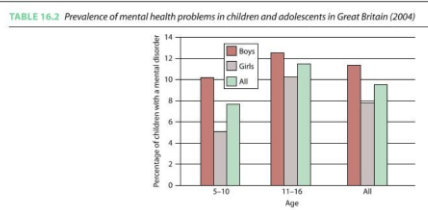
what is the incidence rate of mental health issues for children + adolescents (2004)
around 10% in 5-10 year olds
12.5% in 11-16 year olds, though this is reported as high as 20-25% in American studies
what are externalising disorders + what are 4 behavioural examples
disorders based on outward-directed behavioural problems → e.g. aggressiveness, hyperactivity, non-compliance or impulsivity
what are internalising disorders + what are 3 behavioural examples
disorders represented by more inward-looking + withdrawn behaviours → e.g. depression, anxiety + social withdrawal
what is the general consensus around ‘internalising’ + ‘externalising’ labels
these are relatively traditional terms that have been replaced by modern diagnostic categories, but they are still useful in regards to children specifically → difficulty articulating symptoms means that diagnosis = more behaviour focused
what are 2 examples of childhood anxiety
separation anxiety → much more common + specific to childhood
OCD → occurs similarly to adult OCD, but may present differently
what are features of diagnostic criteria of separation anxiety
excessive anxiety surrounding separation from attached figure → distress + aversion to being along
has to last for 4 weeks in children + 6 months in adulthood (criteria needs to be much more severe)
criteria includes somatic symptoms e.g. headaches/nausea
how can OCD in childhood differ from OCD in adulthood
some children can get compulsions without obsessions
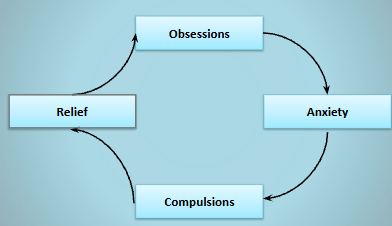
traditional cycle → disturbing intrusive thoughts cause anxiety + stress, which causes sufferer to engage in compulsions (repetitive/ritualised behavioural patterns), which causes relief (reinforcing obsessions)
childhood cycle → general stress + anxiety causes engagement in compulsions, which causes relief, reinforcing the anxiety + continuing the cycle
individual believes the compulsions will prevent a catastrophic event
what are 5 types of OCD compulsions
checking → flicking light switches, locking doors etc., seeking reassurance from otehrs
contamination → excessive cleaning/washing
symmetry + order
hoarding
symptoms must cause marked distress + difficulty performing daily functions due to being time-consuming/interfering with routine
how does childhood generalised anxiety disorder differ from adult form
functions similarly to adult anxiety, but more focus on pathological worry, e.g. about potential problems/threats
different childhood anxieties are typical to particular ages, e.g. 4-7 may be afraid of separation + imaginary creatures, whether 11-13 may be afraid of social threats
pathological worry tends to increase over time → e.g. 8 year olds have double the worry of 5 year olds
how common are specific phobias in childhood + when are they a concern
very common → specific phobias e.g. of water/heights are normal in early childhood + can appear/disappear quickly
there is difficulty diagnosing phobias due to developmental trajectories → they can lead to an actual phobic disorder later in development if it persists
social phobia is less common, but begins as fear of strangers → typical behaviour in early childhood unless it persists
how heritable is anxiety + what is 1 contributing genetic factor
anxiety is moderately heritable → 54%, though this changes from childhood to adulthood (due to it increasing)
certain target genes in GABA system may increase disposition
what are 3 environmental factors that may increase anxiety risk in childhood
trauma
modelling/exposure to information → parent responses to information given will influence the child’s reaction to that information in the future
parenting style → both overprotective/overbearing and neglectful styles can lead to anxiety
how does depression present differently + similarly in childhood to adulthood
diagnostic criteria is largely the same as adult with minor amendments:
difficult to recognise due to children struggling to describe symptoms, so focuses more on observable behaviour
more common ‘clingy’ behaviour, school refusal + exaggerated fears
increased somatic complaints e.g. stomach/headaches
what is the heritability rate of depression + how does this change from childhood to adulthood
moderate heritability estimated for depression → large range between 30-70%, but usually estimated as 40-50%
childhood heritability tends to be lower due to increased environmental influence → abuse/neglect are risk factors early in life
what are 6 domains of risk factors for adolescent depression
cognitive → negative cognitions/attributional styles
dispensational factors + psychopathologies → low self-esteem, internalising + externalising behaviour
stress → major life events
social + coping skills → interpersonal conflict with parents
physical → physical illness, reduced level of activities, tobacco use
academic → absenteeism + grade dissatisfaction
for what 2 main reasons is there an increased risk of depression in children of parents with depression
genetic component → may pass a short form of 5-HTT etc.
psychological components → behaviours affecting upbringing that may increase childhood risk
what are 3 potential psychological causes for children of depressed parents developing depression themselves
if parent is depressed due to current environment e.g. poverty, child may inherit it due to sharing the environment
potential childhood neglect due to not being able to respond to child’s emotions adequately → lack of support/interpersonal conflict
low mood or negative attributional styles may be learnt from parental interaction
what is the ambiguous scenarios test + what does it assess
a test of positive or negative attributional style → subtle method of testing childhood/adolescent depression or anxiety
given multiple scenarios e.g. ‘you give a speech + observe the audience’s reaction’ + patient has to finish the scenario based on what they envision
what are the 3 types of ADHD presentation
predominantly inattentive
predominantly hyperactive/impulsive
combined presentation
what are potential treatments for childhood/adolescent psychological problems
drug treatments → tend to be given the same treatments as adult but in lower doses
family interventions
CBT → may be less appropriate for young children, more appropriate for internalising disorders
play therapy → more appropriate for young children who don’t have appropriate communicative abilities
what are 3 potential issues with prescribing drug treatments in childhood in comparison to adulthood
drugs need to be consistently taken + may be less effective if inconsistent → child may require supervision
addiction → medication may be necessary in some situations (e.g. drug misuse is more common in untreated ADHD), but often causes drug dependence
intervening on a biological level may lead to neurochemical changes in a still-developing brain, which have long-term consequences
e.g. proscribing Prozac to adolescent mice produces more anxiety in adulthood
what are 3 types of family intervention
systematic family therapy → focuses on communication, structure + organisation between family members
parent management training → focuses on not rewarding antisocial/externalising behaviour
functional family therapy → strengthens relationships
what effect does making decisions on treatment/support in partnership with children have on their mental health
shared decision-making tends to increase the efficacy of interventions → creates mutual understanding between clinician + child, meaning child is better understood + receives the most effective treatment for them
what are the differences between oppositional defiant disorder (ODD), conduct disorder (CD) + antisocial personality disorder (APD)
all externalising disorders, but:
ODD = a milder form of CD
CD is either childhood CD (before age 10) or adolescent CD (after age 10)
CD can develop into APD in adulthood, but sometimes stays as CD
what are callous + unemotional (CU) traits + what 3 characteristics do children/adolescents with these often have
distinguished by a persistent pattern of behaviour that reflects a disregard for others, lack of empathy + generally deficient affect (associated with CD + APD). often observed with:
distinct problems in emotional + behavioural regulation that distinguish them from other antisocial youth; more similar to adult psychopathy
range of distinctive cognitive characteristics, e.g. less sensitive to punishment cues
positively related to verbal intellectual skills → not associated with low general mental ability
what is challenging behaviour defined as (Ogundele, 2018)
culturally abnormal behaviour of such an intensity, frequency or duration that the physical safety of the person or others is likely placed in serious jeopardy, or seriously limit access to use of ordinary community facilities
can include self-injury, physical/verbal aggression, non-compliance, disruption of environment + other stereotypies
what are 3 examples of disruptive behavioural problems (Ogundele, 2018)
ADHD
ODD
CD
what is disruptive mood regulation disorder (DMDD) (Ogundele, 2018)
a type of ‘emotional problem’ → characterised by pervasively irritable/angry mood, including frequent episodes of severe temper tantrums/aggression (more than 3 a week) + persistently negative mood
lasts more than 12 months in multiple settings
what are pervasive developmental disorders + what are 5 examples
characterised by pervasive qualitative abnormalities in reciprocal social interactions + patterns of communications, with restricted + stereotyped interests/activities. now called autism spectrum disorders. includes:
autism
Asperger syndrome (though considered out of date → autism spectrum)
childhood disintegrative disorder (CDD) → acute onset of autism symptoms
pervasive developmental disorder not otherwise specified (PDD-NOS)
Rett syndrome
what is the 6-month prevalence rate for any mental health disorder in young people up to 17 (WHO, 2001)
20.9%, 13% being anxiety disorders + 10% DBDs
what are 10 common risk factors for development of childhood emotional/behavioural disorders (Ogundele, 2018)
maternal psychopathology → e.g. low education, anxiety, antisocial behaviour
adverse perinatal factors → e.g. alcohol in gestation, early labour onset
poor child-parent relationships → poor supervision, harsh discipline
adverse family life → dysfunctional family due to substance abuse, violence etc.
household tobacco exposure
poverty/adverse socio-economic environment
early age of onset → more likely to experience more persistent + chronic trajectory
child’s temperament
developmental delay + intellectual disability
child’s gender → boys more likely to suffer from DBD, whether depression predominantly affects girls