Naplex 2026 - Anemia Ch 35
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Define anemia
A decrease in red blood cells (RBCs), hemoglobin (Hgb) and/or hematocrit (Hct)
Leads to reduced oxygen delivery.
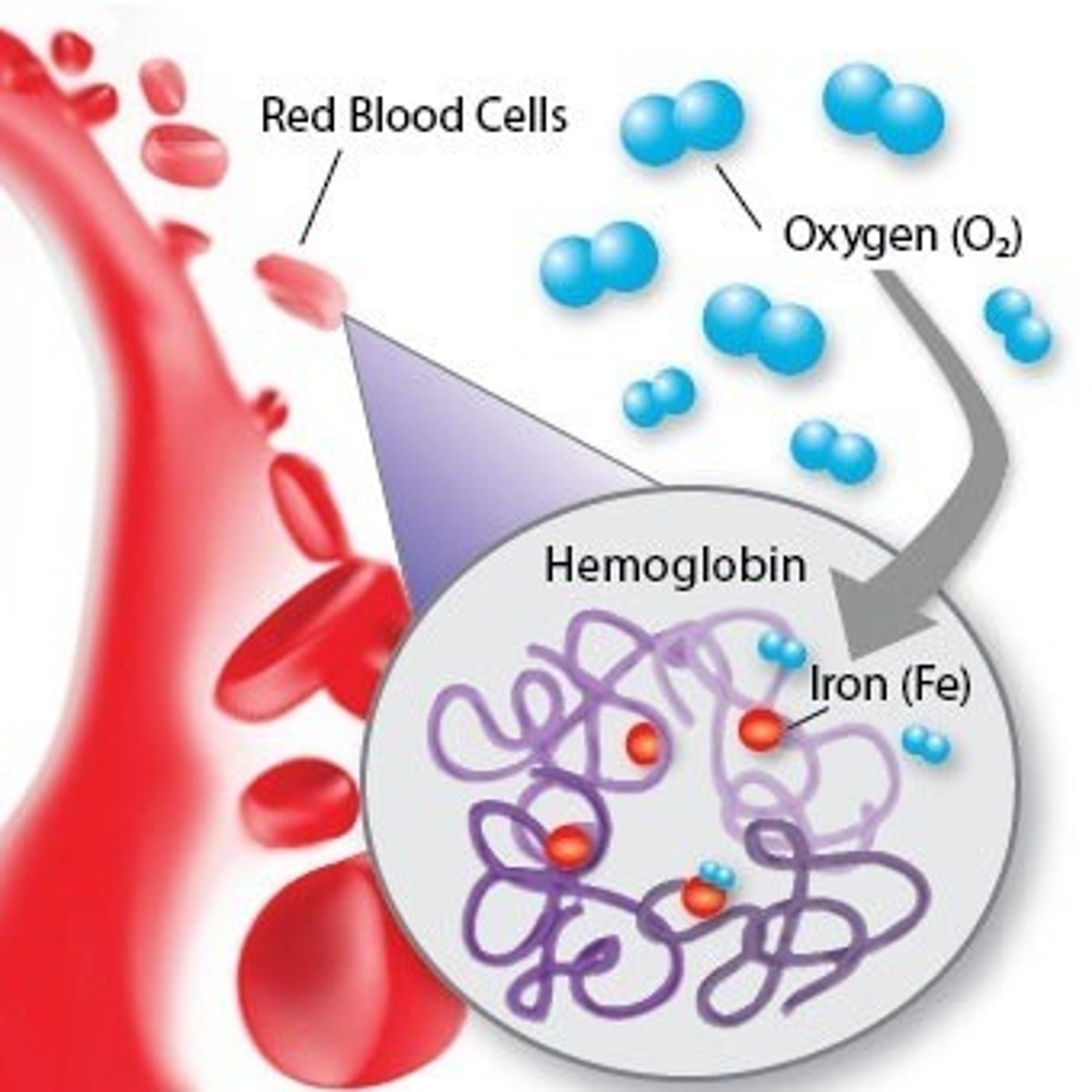
What is hemoglobin (Hgb)
Iron-rich protein found in RBCs that carries oxygen
What is hematocrit (Hct)
% of RBC volume compared to the total blood volume
What are reticulocytes
Immature RBCs, formed in the bone marrow
What are erythrocytes
Mature RBCs
What are some causes for anemia?
1) Impaired RBC or Hbg production
2) Increased RBC destruction: hemolysis
3) Nutritional deficiencies: iron, folate, vitamin B12
4) A complication from a disease such as CKD or cancer
What are the 3 main nutritional deficiencies that can lead to anemia
Iron
Folate
Vitamin B12
Sx from prolonged/severe anemia?
-Fatigue
-Weakness
-SOB
-Exercise intolerance
-HA
-Dizziness
-Pallor
Due to reduced oxygen delivery
What is Mean corpuscular volume (MCV)
The size or avg volume of RBCs
If a pt has low Hgb/Hct ± S/sx of anemia, then you check MCV:
If MCV is low (<80 fL) this is called ____ anemia
If MCV is high (>100 fL) this is called ____ anemia
If MCV is normal (80-100) this is called ____ anemia
If MCV is low (<80 fL) this is called microcytic anemia
If MCV is high (>100 fL) this is called macrocytic anemia
If MCV is normal (80-100) this is called normocytic anemia
A likely cause for microcytic anemia is ....
Iron deficiency
Some causes for macrocytic anemia include... (6)
1) Vitamin B12 deficiency (diet or autoimmune)
2) Folate deficiency (diet)
3) Alcohol use disorder
4) Decreased GI absorption due to Crohn's disease, celiac disease or gastric bypass
5) Pregnancy
6) Long-term use of metformin, H2RAs or PPIs
Likely causes for normocytic anemia includes (5)
1) Acute blood loss
2) Malignancy
3) CKD
4) Bone marrow failure (aplastic anemia)
5) Hemolysis
What is ferritin
Iron stores
What is the most common nutritional deficiency in the US?
Iron
What pt populations require an increase in iron?
1) Pregnancy
2) Lactation
3) Infants
List the common causes for iron deficiency (6)
1) Vegetarian or vegan diet
2) Heavy menses
3) PUD
4) High gastric pH (eg use of PPIs)
5) GI disorders: celiac disease and IBD
6) Gastric bypass
List the lab findings consistent with iron deficiency anemia (IDA) aka microcytic anemia
Decrease in (6) markers
Increase in (1) marker
Decrease in:
1) Hgb
2) MCV (< 80 fL)
3) Reticulocyte count
4) Serum iron
5) Ferritin
6) TSAT (transferrin saturation)
Increase in:
1) TIBC (Total iron binding capacity)
What is the treatment regimen + counseling tips for iron deficiency, using oral tablets
Take 1 tab PO daily or every other day.
Take on an empty stomach (1 hr before or 2 hr after meals) for best absorption.
Avoid H2RAs and PPis; separate admin from antacids.
Sustained-release or enteric-coated iron tablets cause less ___ ___ but are not recommended due to __ ___
Sustained-release or enteric-coated iron tablets cause less GI irritation but are not recommended due to poor absorption
What is the general lab goal after starting oral iron tx for IDA
An increase in Hgb after 1-2 weeks
How long to continue oral iron tx for IDA?
For 3-6 months or until iron stores return to normal.
What is the dose in ferrous sulfate tablets (mg? elemental iron?)
365 mg (65 mg elemental iron)
What is the boxed warning for iron tablets
Accidental overdose in children can cause fatal poisoning. In case of overdose, go to ER or call poison control immediately, even if asymptomatic.
What are common SE of taking iron tablets
Constipation (dose related)
Dark and tarry stools
What is the antidote for iron overdose? (generic and brand name)
Deferoxamine (Desferal)
Why do antacids need to be separated from iron administration?
And why do we have to avoid H2RAs and PPIs?
Increasing gastric pH will decrease iron absorption
What can be taken to help increase iron absorption?
Vitamin C aka ascorbic acid
Iron is a polyvalent cation that can DECREASE absorption of other drugs by binding/chelating with them in the GI tract.
Separate administration is needed with the following meds (5)
1) Quinolones
2) Tetracyclines
3) Bisphosphonates
4) Levothyroxine
5) INSTIs (Integrase strand transfer inhibitors)
T/F: There is no difference in efficacy among the oral iron tablets, or among the IV iron formulations.
T
Due to cost and the risk of more severe ADR, IV iron is restricted to the following pt populations (3)
1) CKD on hemodialysis
2) Receiving erythropoiesis stimulating agents (ESAs)
3) Unable to tolerate oral iron
Name two IV iron products and their brand names
1) Iron sucrose (Venofer)
2) Ferumoxytol (Feraheme)
What is the boxed warning for Iron dextran
Serious and sometimes fatal anaphylactic rxns. All pts should be given a test dose prior.
What is the boxed warning for Ferumoxytol
Serious and sometimes fatal anaphylactic rxns.
Warning for all IV iron products
Hypersensitivity rxns
What is pernicious anemia?
A common cause of vitamin B12 deficiency.
It's an autoimmune condition caused by antibodies to intrinsic factor, which is required for vitamin B12 absorption.
What is the tx and duration for pernicious anemia
Vitamin B12
Lifelong
Lab markers for macrocytic anemia
Decrease in:
Hgb
Reticuloctye count
Vitamin B12 and/or folate
Increase:
MCV
± Methylmalonic acid (deficiency in B12)
± Homocysteine metabolism (deficiency in folate and B12)
Vitamin B12 is required for the metabolism of .... in the body
Methylmalonic acid and homocysteine
Folate is required for the metabolism of ... in the body
Homocysteine
Vitamin B12 deficiency can result in ... if untreated
Neurologic dysfunction including cognitive impairment and peripheral neuropathy which can become IRREVERSIBLE if untreated
Folic acid deficiency causes what sx
Ulcerations of the tongue and oral mucosa
What is 1st line tx for severe vitamin B12 deficiency
Cyanocobalamin injections (B12)
What vitamin is folic acid
Vitamin B9
1st line tx for folate deficiency is usually
oral folic acid / folate / vitamin B9
What is Nascobal and how do you use it
Cyanocobalamin (B12) nasal spray
Use in one nostril once weekly
What is the route of admin for cyanocobalamin (B12) injection
IM or deep Subq
What is erythropoietin (EPO)
A hormone made by the kidneys that simulates bone marrow to produce RBCs
Anemia of chronic disease (CKD or cancer) is often due to a deficiency of ....
Erythropoietin (EPO)
What is 1st line tx for anemia of chronic disease (CKD or cancer)
1) IV iron (preferred over oral)
2) Erythropoiesis-stimulating agents (ESAs):
Epoetin alfa
Darbepoetin alfta
Name the Erythropoiesis-stimulating agents (ESAs) and their brand names
1) Epoetin alfa
=> Epogen, Procrit
2) Darbepoetin alfta
=> Aranesp
The ___ guidelines recommend iron in all pts with anemia of CKD.
KDIGO (Kidney Disease Improving Global Outcomes)
A pt with "anemia of chronic disease" has been on IV iron but their Hgb remains < ___ g/dL. A erythropoiesis-stimulating agent can be used.
Hgb < 10 and on iron
=> start ESA
If Hgb approaches or exceed __ g/dL, then the ESA dose needs to be decreased or interrupted
Hgb 11 g/dL
If Hgb approaches or exceed 11 g/dL, then the ESA dose needs to be .....
decreased or interrupted
What is required for ESAs to be effective in the body?
Adequate iron stores
Epoetin alfa (Epogen, Procrit) for anemia of CKD: what is the dosing regimen
3x / week
Boxed warnings for Epoetin and Darbepoetin (4)
1) Increased risk of death, MI, stroke, VTE and thrombosis
2) Use lowest effective dose
3) CKD: increased risk of death when Hgb lvl > 11 g/dL
4) Select cancers: do not use if anticipated outcome is cure from cancer (it can worsen tumors)
Epoetin and Darbepoetin can do what to BP?
Increase it
It can cause HTN
Side effect of ESAs
Arthralgia (joint pain)
Lab monitoring for ESAs (5)
1) Hgb
2) Hct
3) TSTAT
4) Serum ferritin
5) BP
(IV/oral) route of ESAs is recommended for pts on hemodialysis
IV
Epoetin and Darbepoetin storage/handling
Fridge; do not shake
Darbepoetin (Aranesp) regimen
Weekly
Half-life of Epoetin vs Darbepoetin
Darbepoetin has half-life 3x LONGER than Epoetin, that is why darbepoetin is dosed once weekly and epoetin is 3x/week
Two common mechanisms of drug-induced hemolytic anemia
1) Immune-mediated:
Drug binds to RBCs and triggers antibodies to destruction
2) Glucose-6-phosphate dehydrogenase (G6PD) deficiency
The MD suspects a pt developed immune-mediated hemolysis. How can this be confirmed?
With a positive direct Coombs test
It detects antibodies stuck to the surface of RBCs
What is the relationship of G6PD enzyme and blood?
What happens if a pt is G6PD deficient?
G6PD enzyme protects RBCs from oxidant injury.
If a pt is G6PD deficient, RBCs can hemolyze after exposure to oxidative stress from high-risk medications. Can cause drug-induced hemolytic anemia
List common drugs that can cause immune-mediated anemia
Use mneumonic
Quite Quick Positive Coombs Lab Reveals Immune Mediated Situation
Q = Quinine
Q = Quinidine
P = Penicillin
C = Cephalosporins
L - Levodopa
R = Rifampin
I = Isoniazid
M = Methyldopa
S = Situation
List common drugs that can cause hemolytic anemia with G6PD deficiency pts
Use mneumonic
Patients Not Making Sufficient RBC Please Don't Quit Quietly
P = Pegloticase
N = Nitrofurantoin
M = Methylene Blue
S = Sulfonamides
R = Rasburicase
P = Primaquine
D = Dapsone
Q = Quinidine
Q = Quinine
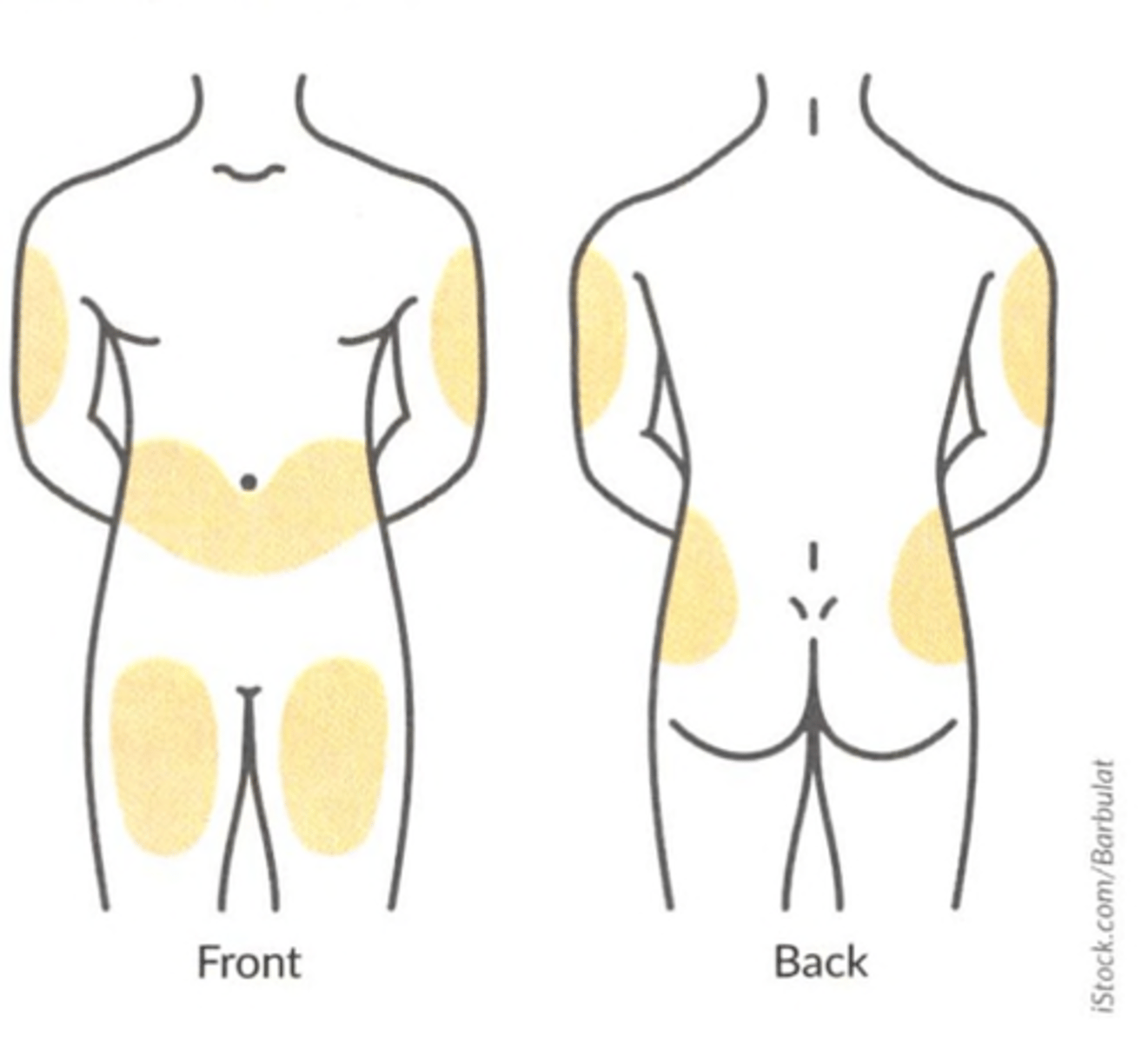
Where are the injection sites for ESAs?
Abdomen around belly button
Upper/outer arms
Thighs
Hips to the back