developmental anatomy of cardiovascular and respiratory system
1/26
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
27 Terms
heart
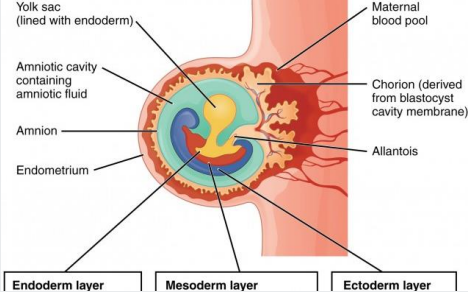
Soon after fertilisation, 3 germ layers form
Ectoderm (top)
Mesoderm (middle)
Endoderm (bottom)
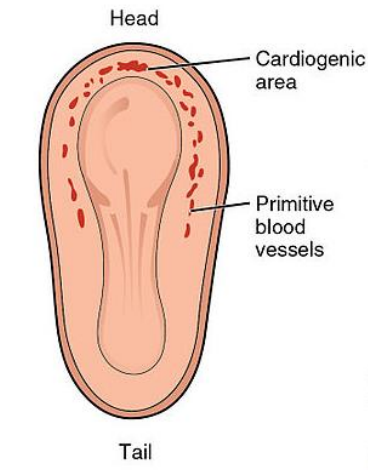
The heart forms from mesoderm around 18 to 19 days after fertilization
heart
Within mesoderm, a horseshoe-shaped area develops (the cardiogenic area or plate)
The cardiogenic plate moves ventral to the pharynx as the head process grows upward
Formed from cardiac myoblasts and blood islands (forerunners of blood cells and vessels)
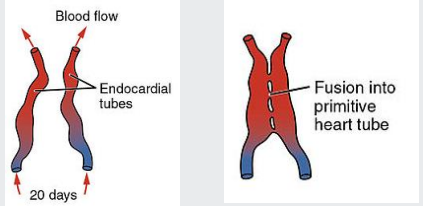
Within each side of the cardiogenic area, an endocardial tube forms (lined by endothelial cells)
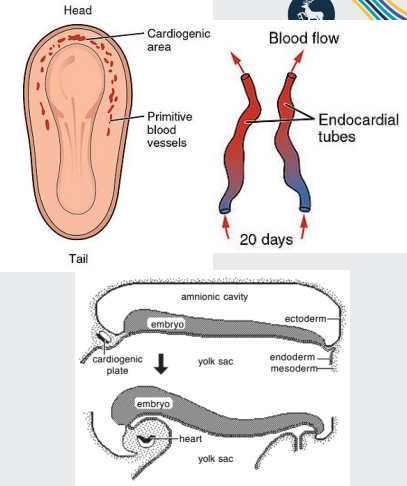
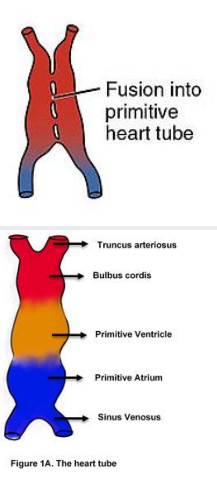
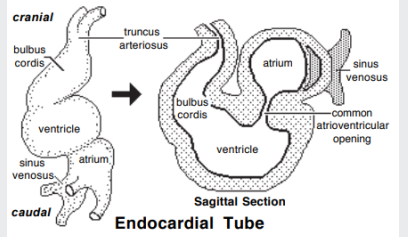
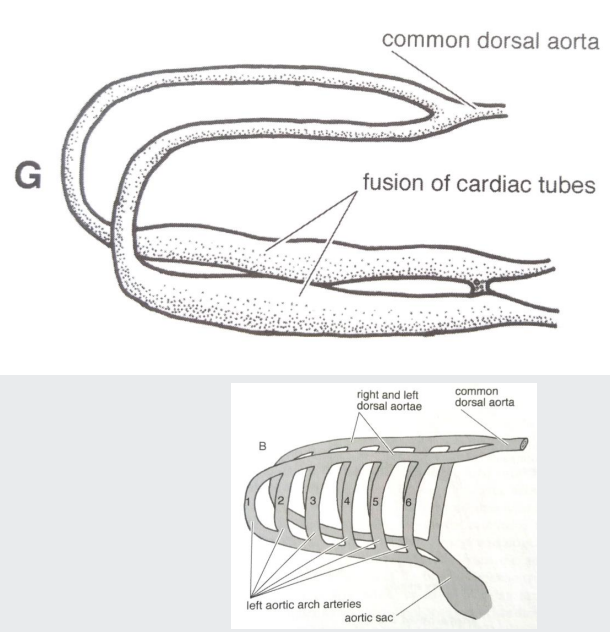
development of the heart
The endocardial tubes fuse midway along their length, forming the tubular heart or cardiac tube
A single tube is formed with an arterial and a venous end
The tubular heart undergoes differential growth and expansion
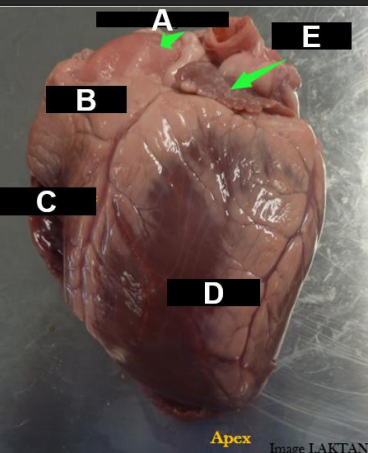
test your previous knowlefge
Two atria and two ventricles
Atria are the blood-receiving chambers
Ventricles are the blood-pumping chambers
The auricle is blind ear-shaped pouch of the atrium
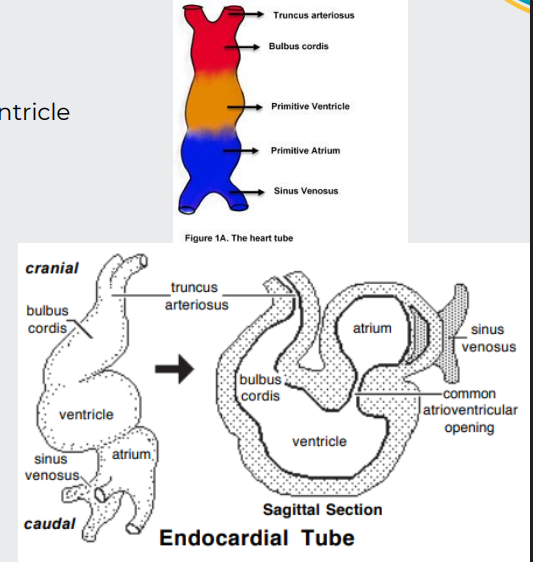
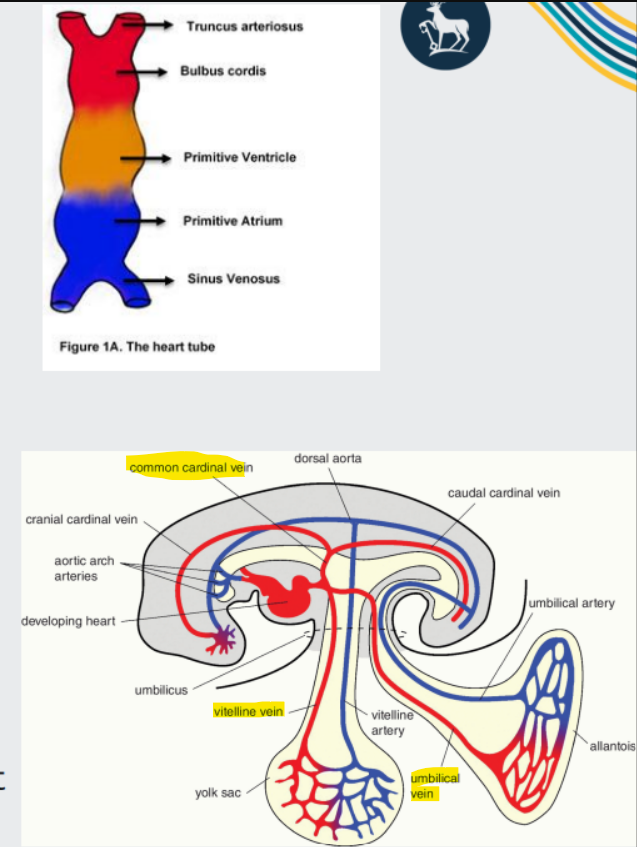
development of the heart
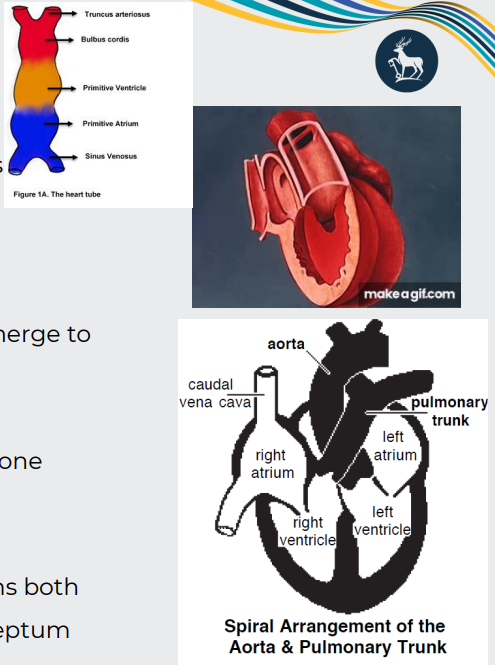
Truncus arteriosus (aorta and pulmonary trunk)
Bulbus cordis (right ventricle)
Primitive ventricle (left ventricle)
Primitive atrium (right and left auricles)
Sinus venosus (remains bifurcated, a paired area where veins drain
- The left sinus venosus becomes the coronary sinus;
- the right is incorporated into the wall of the right atrium
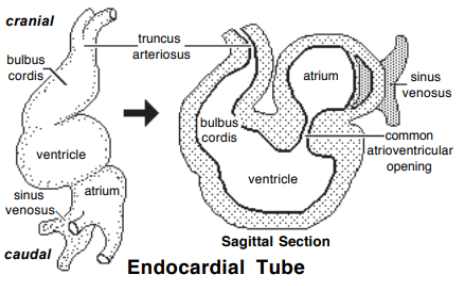
morphogenesis
Endocardial tube lengthens and loops on itself
This puts the bulbus cordis (right ventricle) beside the ventricle (left ventricle) and the atrium dorsal to the ventricle
Venous return is shifted to the right
The larger right sinus venosus becomes the right atrium (embryonic atrium becomes auricles)
The smaller left sinus venosus joins the future right atrium as the coronary sinus venosus
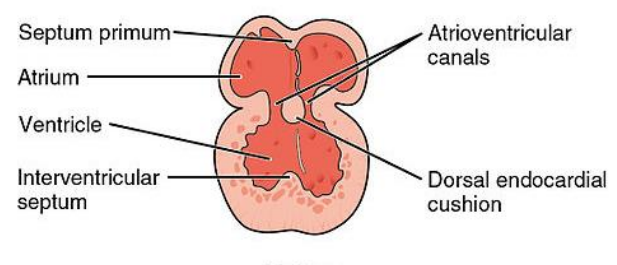
formation of cardiac chambers
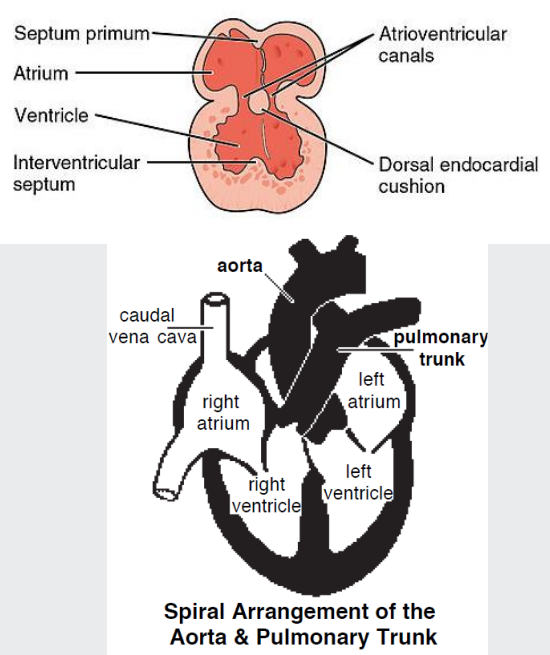
Partitions form a 4-chambered organ. The septa that form:
1. Divide atrium and ventricle (cardiac cushions → septum intermedium)
2. Divide the atrium (septum primum and secundum)
3. Divide the ventricle (interventricular septum)
4. Divide the outflow tracts (Aortico-pulmonary septum)
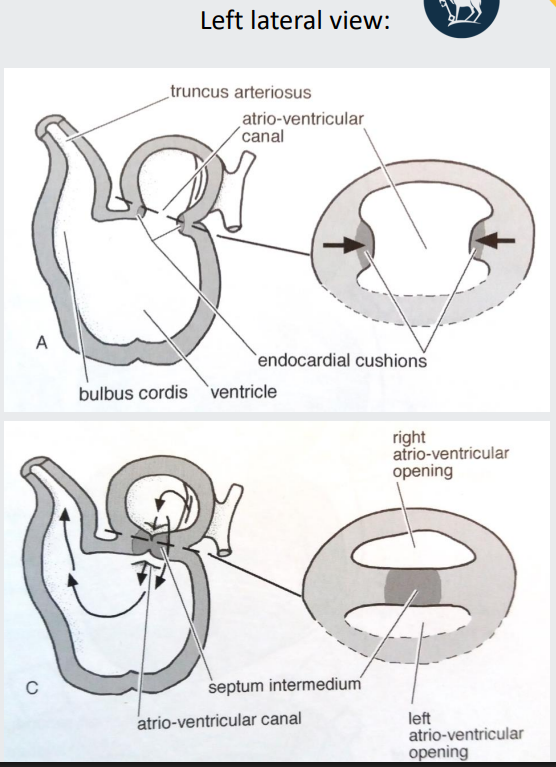
dividing atrium and ventricle -1 = cardiac cushions → septum intermedium
At the atrioventricular region, two masses of cardiac mesenchymal tissue form (cardiac cushions)
They extend towards each other and fuse
The fused cushions form the septum intermedium
Separates the atrio-ventricular canal into right and left atrio-ventricular openings
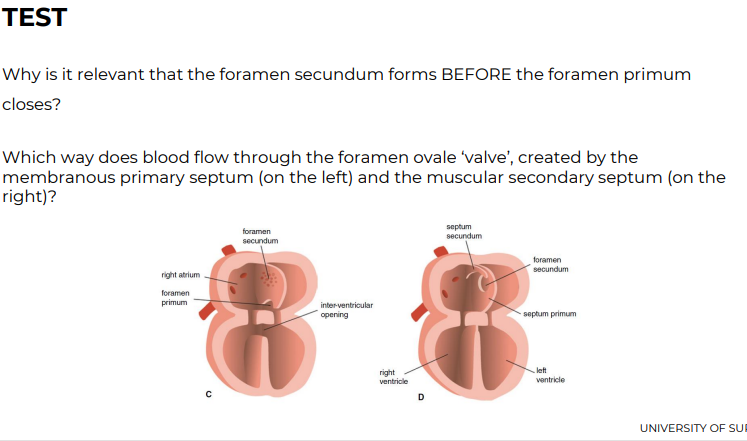
dividing atrium - 2 = septum primum and secundum
A membranous fold (primary septum) grows down from the dorsal wall of the atrium towards the endocardial cushions
Divides atrium into left and right atria
Primary septum leaves a small hole near the cushions, that will eventually close (primary foramen)
Before it closes, a second hole forms in the primary septum via apoptosis (secondary foramen)
Secondary septum grows from the cranial wall of the right atrium toward the caudal wall
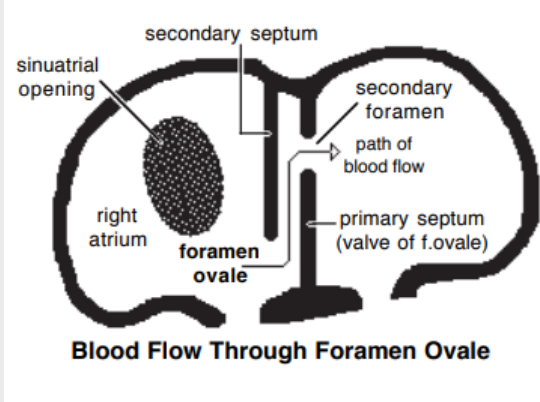
The septum remains incomplete, and its free edge forms the boundary of an opening called the Foramen Ovale*-left foramen ovale (oval shaped)
Asnwer to Q: Primary septum acts like a valve against the muscular secondary septum
• A shunt that allows oxygenated blood to bypass the nonfunctional fetal lungs to continue blood flow and allow oxygenated blood reaching the foetal heart
dividing ventricles (interventricular septum)
The expanded part of the bulbus cordis (right ventricle) and the ventricle form a common chamber
Externally, they are marked by a groove (the interventricular sulcus)
Internally, they are marked by a fold (primordial interventricular septum)
dividing ventricles pt 2 (interventricular septum)
At this stage:
The embryonic (primitive) ventricle = left ventricle
The embryonic bulbus cordis =right ventricle
As the ventricles expand, the interventricular septum elongates towards the endocardial cushions
separating outflows (Aortico-pulmonary septum)
The truncus arteriosus divides, to form two outflow tracts:
Aortic trunk and Pulmonary trunk
Ridges appear along the lumen wall, grow inward, and merge to create the spiral septum (aortico-pulmonary septum)
As a result, the aorta and pulmonary trunk spiral around one another
Growths from the spiral septum and endocardial cushions both contribute to the proper closure of the interventricular septum
separation of outflows
Why does it matter that the aortico-pulmonary septum spirals?
so can receive oxygenzated and deoxygenated blood from diff directions - aorta leave left ventricle and pulmonary leaves right ventricle
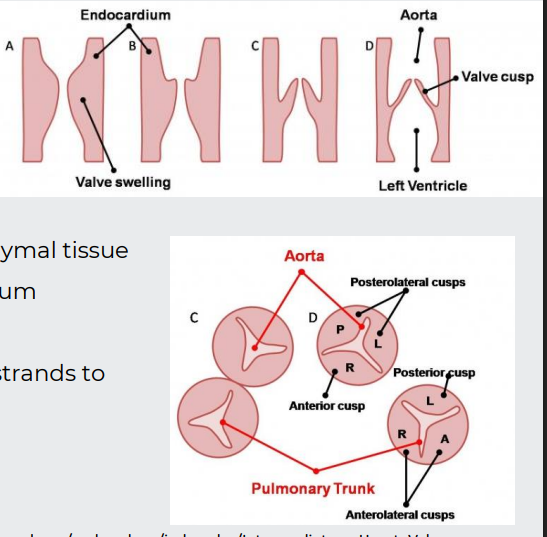
formation of valves
Aortic and pulmonary valves form from swellings of mesenchymal tissue
Then remodelled to form thin-walled cusps
The atrioventricular valves form from the proliferation of mesenchymal tissue at the rim of the AV opening, attached to the myocardium
Valves remodelled, but remain anchored by muscular strands to the ventricular walls
formation of blood vessels
Blood vessel formation occurs in 2 steps: vasculogenesis and angiogenesis
Vasculogenesis -Formation of blood vessels from blood islands
Vessel formation happens when island vesicles coalesce, sprout buds and fuse to form vascular channels
Angiogenesis- Budding of new vessels from existing vessels.
Begins in the splanchnic mesoderm of the yolk sac
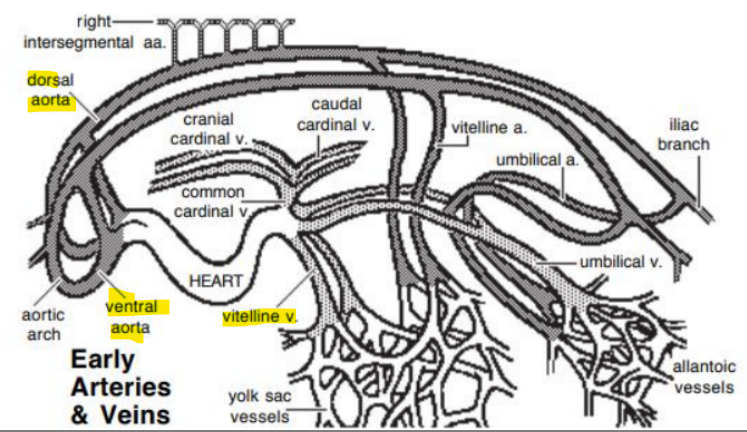
formation of arteries
The aortae fuse with the cardiac tubes
Cardiac tubes fuse with the vitelline veins (1) caudally
Note paired dorsal and ventral aortae
Due to embryo folding, the dorsal aorta ends up dorsal to the cardiac tube
Paired ventral aorta receive blood from truncus arteriosus and fuse to form the adult brachiocephalic trunk
formation of aortic arches
Bilaterally, ventral & dorsal aortae are connected by up to six aortic arches
The cranial fusion between dorsal aortae and cardiac tubes becomes the 1st aortic arches
In total, 6 pairs of aortic arches will develop
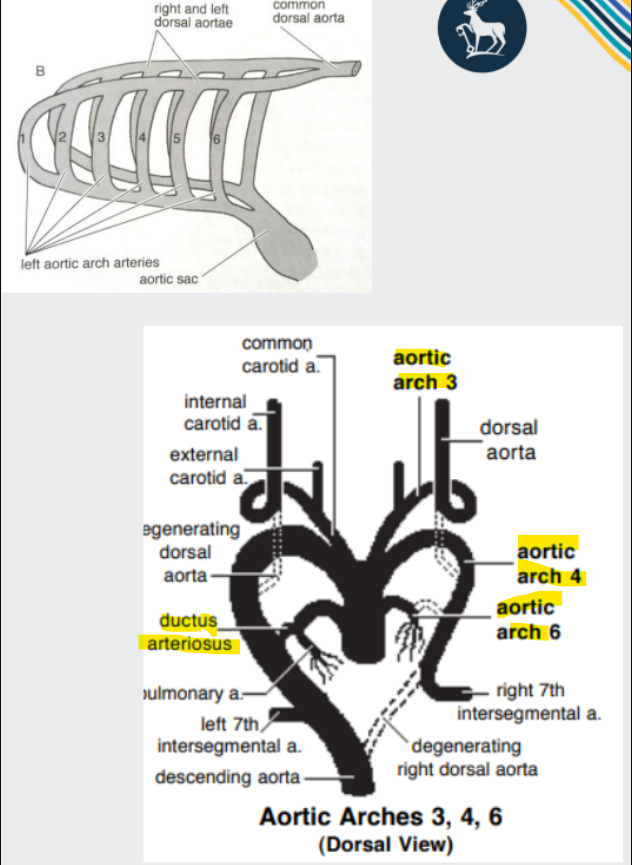
formation of aortic arches continued
The aortic arches give rise to major vascular structures:
3rd arches - internal and common carotid arteries
Left 4th arch - definitive aortic arch
Right 4th arch - proximal part of right subclavian artery
6th arches - pulmonary arteries (and ductus arteriosus)
formation of veins
Three paired veins drain into the heart tube:
Vitelline veins (return poorly oxygenated blood from the yolk sac) - eventually forms plexus on duodenum and liver→portal vein system
Umbilical veins (carry well-oxygenated blood from the primordial placenta)
Common cardinal veins (return poorly oxygenated blood from the body of the embryo)
Recall that venous return is shifted to the right side, and the right sinus venosus is incorporated into the right atrium. The left sinus venosus is reduced and becomes coronary sinus
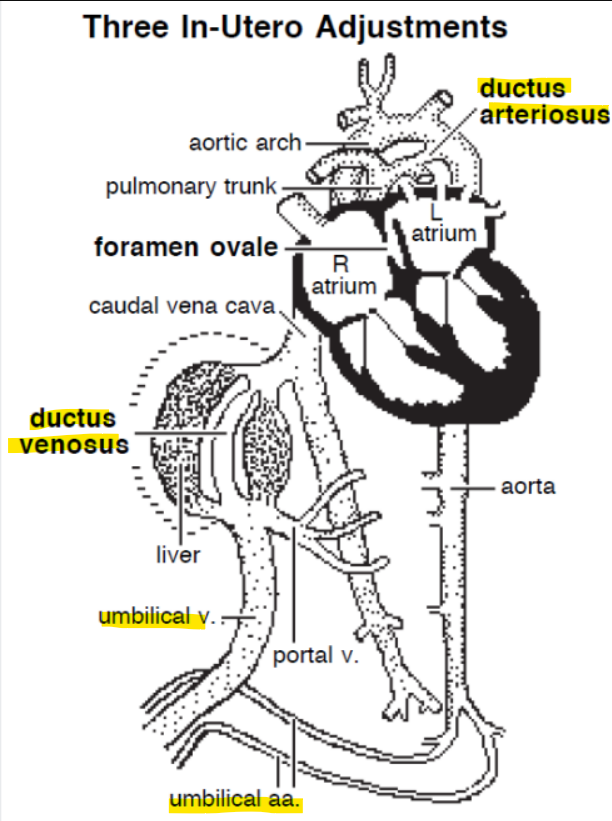
foetal shunts
Allow blood to bypass the lungs and liver:
1. Foramen ovale (fossa ovale)
(Between right and left atria - secundum septum on the primum septum)
2. Ductus arteriosus (ligamentum arteriosum)
(Between pulmonary trunk and aorta-shunts the blood from pulmonary trunk to aorta-allowing right ventricle to be exercised)
3. Ductus venosus
(Between umbilical vein and caudal vena cava-develops in the embryo as a shunt that diverts blood away from sinusoids and toward systemic veins)
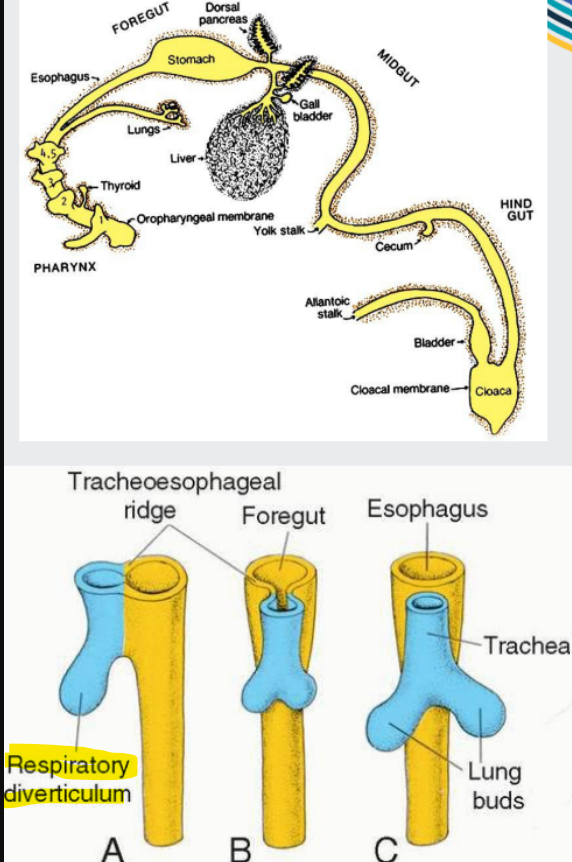
development of the respiratory system
Respiratory diverticulum (the bulge) arises from foregut endoderm, and goes on to form:
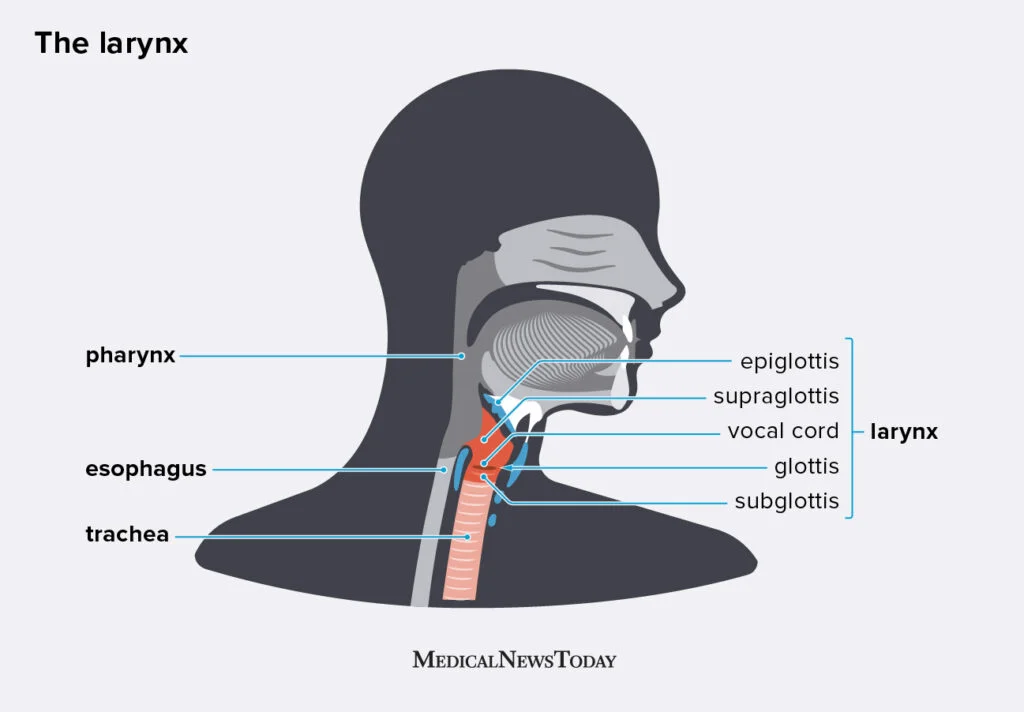
Epithelial lining of trachea
Larynx (voice box and protects airway)
Bronchi and alveoli
Lung buds form the left and right principal bronchi, which divide into ever-smaller branches, down to alveolar ducts and alveoli
Lungs are filled with fluid during development
Mostly glandular secretions, some amniotic fluid
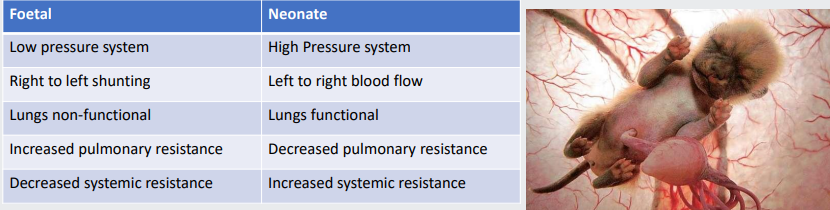
foetal cardiovascular system
The foetal blood pressure is low
The foetal heart is powering it (not mum)
Lots of blood spread out in placenta
Blood is shunted right-to-left by ductus arteriosus and foramen ovale
To bypass lungs
Lungs are non-functional-collapsed
No air to breathe
Pulmonary circulation has high resistance
Vessels here are collapsed
Systemic circulation has low resistance
The placenta is a low-resistance area
Placentae must receive a large proportion of foetus's circulating blood
Two large left and right umbilical arteries
Extending from the caudal end of the abdominal aorta
Umbilical vein
After passing through the capillary bed in the placentae
This highly oxygenated blood returning from placentae to the umbilical vein bypasses liver sinusoids –ductus venosus
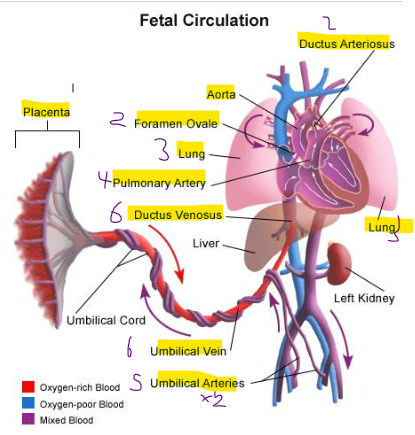
How does foetal heart allow blood to bypass lungs?
Foramen ovale- between the two atria
Ductus arteriosus- between the aorta and pulmonary trunk
(in foetus pressure in the right side is greater than left)
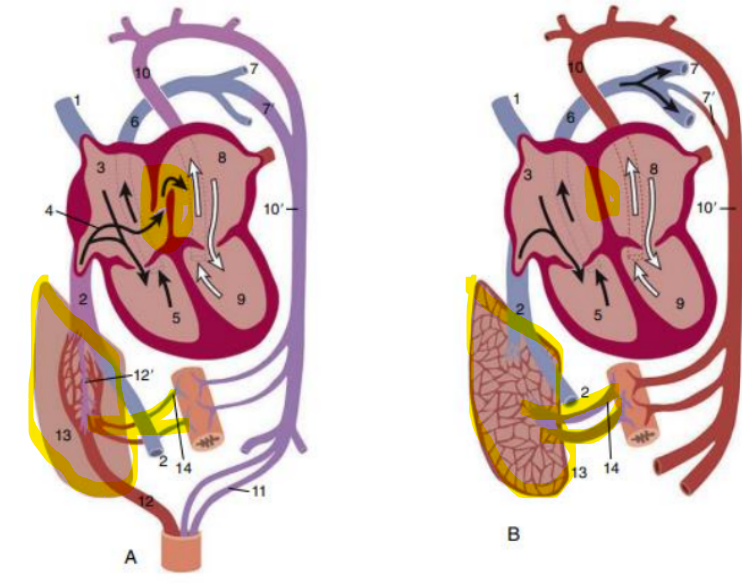
birth -3 adjustments
Contraction of umbilical arteries and veins
Prevent bleeding
Force placental blood into foetal circulation
Contraction of musculature in ductus arteriosus
Physiological shunt closure sends blood to lungs
Anatomical closure can take 2 months
May hear transient cardiac murmur in foals, calves, pigs
Reduced venous return through the umbilical vein and ductus venosus allows the latter to gradually close
Foramen ovale closes
Increased venous return from lungs to left atrium
Reduced venous flow from placenta to right atrium
Pressure in left > right, forces septum primum against
septum secundum
Anatomical closure takes up to 1 year in most species
Non-functional vessels regress, become ligaments
E.g. umbilical arteries -round ligament; ligamentum arteriosum
Compression of the thorax squeezes fluid out of the lungs
Lungs inflate
Pulmonary vascular resistance becomes lower
birth
common congenital conditions
Inter-atrial septal defects (e.g. patent foramen ovale)
Inter-ventricular septal defects
Congenital venous shunts (e.g. persistent ductus venosus)
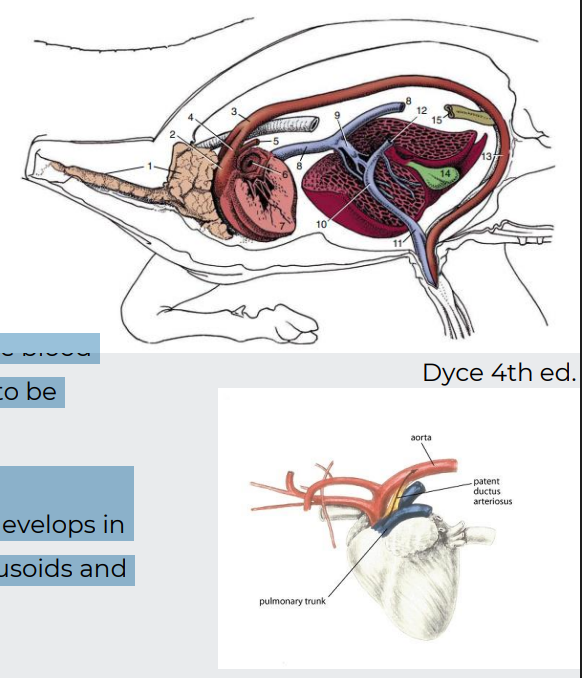
Vascular ring anomalies (e.g. persistent or additional aortic arches) -first pic - esophagus squeezed cos aorta and pulm artery not supposed to ocnnect
Pulmonary or aortic stenosis (abnormal narrowing of a passage in the body)
Abnormal positioning of the heart (e.g. ectopic heart in the neck-Ectopia cordis) - cow
Some occur commonly together
E.g. Tetralogy of Fallot = malformation of aortico-pulmonary septum (enlarged aorta and pulmonary stenosis) + ventricular septal defect (hole), right ventricular hypertrophy
tetra = 4 so 4 things happen
But you should be able to predict what happens functionally as a result
