HYMS Year 2 Critical Appraisal
1/79
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
80 Terms
What are background questions?
> general knowledge inquiries about patients condition that ask who, what, when , how, why
> eg what causes? how does? why does?
What are foreground questions?
> specific knowledge you require to manage patient condition
> question created through PICO framework
What is a cross-sectional study?
> descriptive study that provides a snapshot of the frequency of a disease at a given time
> used to generate a hypothesis as multiple exposures can be identified
> surveys are used to ID prevalence
What biases are seen in cross-sectional studies?
recall, selection and survivor
Strengths of cross sectional studies
> Cheap and quick to conduct
> Data on all variables collected at once
> Multiple outcomes and exposures can be studied
> Good for descriptive analysis and generating hypothesis
weaknesses of cross-sectional design
> Can't determine cause effect relationships
> Not suitable to study rare diseases or diseases with a short duration
> Can't determine incidence
> Susceptible to bias- low response and misclassification due to recall bias and selection bias
Best study design for diagnosis
cross sectional
What is a case-control study?
> groups with disease and without disease (2 different outcomes) are observed
> look back on any exposures (risk factors)- retrospective study- and whether they have any associations
Strengths of case-control study
> Efficient use of resources as you don't need a long time period, you just ask someone with a disease some questions
> Useful in studying rare diseases and those with a long latency period
> Can study multiple risk factors
Weaknesses of case- control studies
> Susceptible to selection and recall bias
> can be difficult to measure the exposure
> reverse causality- effects of the disease on the risk factor > bad for IDing rare exposure
Best study design for aetiology
> case-control study
> cohort study
What is a cohort study?
> observational study that compares incidence of disease over time where half have the exposure and half don't- prospective study
> historical- half have exposure, half don't and look back in time
Strengths of cohort studies
> can ask participants about multiple outcomes eg does diabetes lead to CVD, cancer,
> useful for studying rare exposures eg asbestos
> Historical cohort studies are effective in the investigation of diseases that have a long development time
> Reduces risk of survivor bias
Best study for prognosis
prospective cohort study
What are RCTs?
experimental studies where participants are randomly allocated into intervention and control groups, and compare the outcomes of each
Strengths of RCTs
Able to establish causation
Minimizes biases
One treatment can be directly compared to another
Publishable
Weaknesses of RCTs
> expensive
> selection and performance bias (eg those going to surgical intervention know they're having surgery so behave different)
> ethical limitations
> generalisability
best study design for treatment
RCTs
systematic review of RCTs
best study design for evaluation
survey
qualitative research
What is a meta-analysis?
a statistical technique where results from multiple individual studies for a specific question are combined and re-analysed and a summary estimate is given (often a forest plot)
What is a systematic review?
a rigorous summary of all the research evidence that relates to a specific question
What is the advantage of meta-analysis?
> overall sample size is increased, which can yield more precise estimates of benefits and harms of treatments
> top of evidence hierarchy
Strengths of systematic review
> include all available evidence to answer a question -unpublished and non-English
> increases total sample size therefore certainty and precision better
> indicates heterogeneity among studies
> can indicate need for further research
> permits sub-group analyses- how do different patient groups respond to intervention
> allows sensitivity analyses
What does critical appraisal assess?
Bias• Applicability (what type of data is collected from what type of ppl?) • Limits (is it unrepresentative sample size) • Overall value (useful for pt care?
steps of critical appraisal
> validity of results
> what are the results
> can they be applied to patient care
Why is the randomisation of treatments important (RCT)
confounidng fxs generally equally distributed between treatment arms, ethical as treatment not decided by a person, eliminates systematic bias in allocation of intervnetiins
How to randomise (RCT)
> centralised computer randomisation for multi-centre trials
> smaller trials may use an independent person eg hospital pharmacy to manage the randomisation
Why is it important that both groups are treated the same apart from the intervention? (RCT)
having more consultations, more tests etc could cause a difference in outcome rather than the intervention itself
Withdrawal in RCT
> stopped the intervention
> or withdrew from the trial
Loss to follow up
not providing data at a particular point
should be less than 20%
Why is it important that those who enter the trial are accounted for at its conclusion?
> losses may bias the results if loss more from one group than other
> reduces sample size
> small losses reduce power of study if the outcome of interest in a trial is infrequent
> patients should be analysed in the group they were randomised to even if they stop treatment although they are effectively a control- INTENTION TO TREAT
In what outcome in blinding important?
subjective outcomes- eg measurements of symptoms or functions, or patient self report
blinding is unimportant in objective measures eg death
What is risk?
a quantified uncertainty
What does relative risk tell you in RCT?
> how many times more likely an event will occur in a treatment group compared to control
> less than 1 means treatment decreases risk of outcome
> greater than one means it increases risk of outcome
What does relative risk reduction tell you in RCT?
tells us the reduction of the rate of the outcome in the treatment group relative to that in the control group
What does absolute risk reduction tell you in RCT?
tells us the absolute difference in the rates of events between the two groups- indication of baseline risk and treatment effect
What does numbers needed to treat tell us in RCT?
the number of patients you need to treat with experimental therapy to achieve one additional positive benefit
1/ARR
What is the 95% confidence interval?
range of values of the study sample within which we can be 95% sure the true value lies
What are some disadvantages to providing an intervention in RCTS?
> adverse effects of meds, risk of cancer in imaging
> additional treatment costs- new equipment, staff etc
> opportunity cost eg extra clinic appointment means loss of work for patient
Assessing external validity of RCTs
> checking whether the patient you have is similar to that in the study
> whether the treatment is feasible in my setting
Internal validity
the degree of confidence that the causal relationship you are testing is not influenced by other factors or variables.
What is one of the main problems with observational studies?
Recall bias- patients may both over and under estimate, which is a form of error, making relationships harder to identify
How can how an outcome is measured affect validity of cohort studies?
how the outcome is measured must be kept the same in exposed and non-exposed groups as this may lead to systematic bias ie identifying the outcome better in the exposure group due to better surveillance
What study designs is confounding seen the most?
observational studies- cohort, case-control, cross-sectional
Appropriate techniques to account for confounding in observational studies?
> restriction
> stratification
> matching
> multiple regression techniques
look out for whether something has been 'adjusted for' (cohort) or 'matched' (case-control)
What is statistical power?
to conclusively reject a null hypothesis when it is in fact false
increases with sample size
How can loss to follow up (attrition) affect observational studies?
> Attrition bias- If the participants lost to follow-up differ systematically from those who remain in the study, the results may be biased.
> reduced statistical power due to sample size, leads to type 2 error (null accepted)
Why is having too long a follow up period bad?
> wastes money
> unethical as it involves data collection of no scientific value
What is a weak value for relative measure of effect (odds ratio/relative risk)
less than 1.5 considered weak
Relative risk
risk in exposed/risk in unexposed
What studies usually report relative risk? Odd ratio?
> cohort
> case control
Why is it good to have 2 authors looking at the papers and assessing quality in systematic reviews?
> independent assessment can help counteract unconscious bias
> less likely errors are made
> increases transparency of process therefore unbiased by using pre-agreed criteria
> less chance of missing a relevant trial
When are studies acceptable to combine in systematic reviews?
when studies are similar (i.e. they used similar outcomes). If studies are very dissimilar, then results should not be combined.
- Because combined results provide stronger evidence, but only when appropriate to combine.
What are features of a good search strategy in systematic reviews?
hand-searching
conference proceedings
contacting authors
non-English papers
Bradford Hill criteria of causality
> temporal- risk precedes outcome
> specific- risk factor is specific
> dose-response: greater exposure leads to greater effect
> coherence- between epidemiological and lab findings
reverse causality
> biology of the disease/ patient behaviour modifies risk factor. Before disease is diagnosed, risk factors are altered. > eg decreased weight= lung cancer (lung cancer decreased weight before it was diagnosed)
> eg decreased alcohol= angina (pain began, behaviours altered before diagnosed)
Weaknesses of cohort studies
> expensive and timely
> difficult in measuring risk
> attrition, recall and selection bias
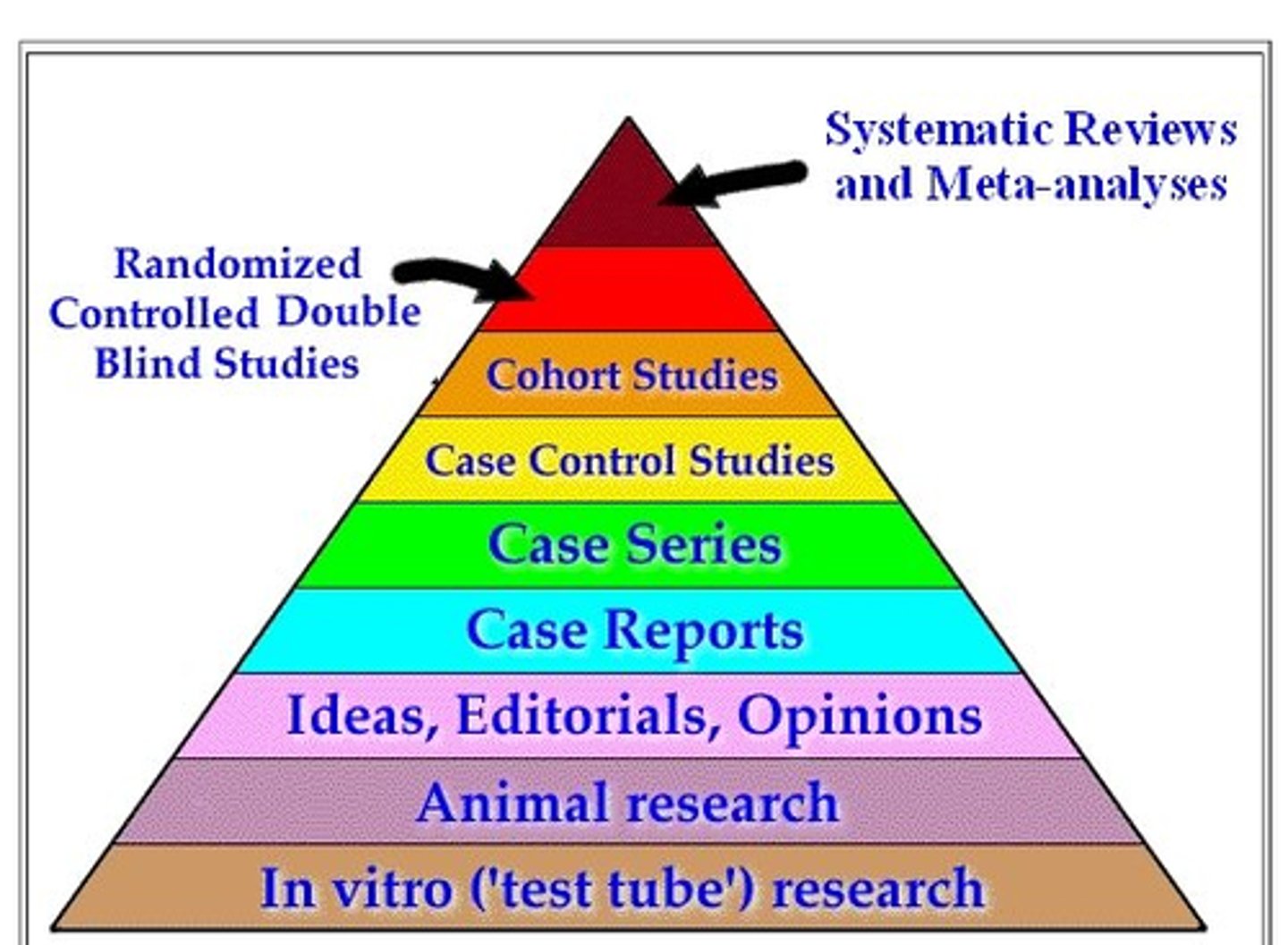
pyramid of evidence (top to bottom)
Weakness of meta-analysis
Publication bias.
Why is having just English language reports not favourable in systematic reviews and meta-analyses?
researchers more likely to publish statistically significant results in English-language journals, while reserving non-significant findings for non-English journals. Excluding non-English literature can artificially inflate perceived effectiveness of an intervention
What is intention to treat analysis?
participants in a trial are analysed within the group they were allocated in randomisation, even if they have not completed the trial or changed treatment
Importance of random allocation
t to ensure that the observed effects are uninfluenced by selection bias and that confounding factors are generally equally distributed between the treatment arms
Importance of placebo arm
ensures that any effect found is attributable to the active intervention and not to non-specific intervention of healthcare or healthcare professional
Features of case-control that distinguishes them from other studies
> retrospective
> at the start people with the condition are matched with those without from the same population to try and understand the causes of the condition
Define confounding
an apparent relationship between an exposure and and outcome that is false; that is, it implies a causal relationship that actually does not exist due to a shared relationship with something else
Purpose of controls in a case-control study
> offers a comparison group with people from the same population but without outcome of interest
> Allows a baseline value of the exposure in a normal population
Problems with restriction technique for confounding
> less data
> difficult when you have other possible confounders
What is systematic bias in RCT
any flaw in the study’s design, conduct, or analysis that distorts the results and leads to an inaccurate (overestimated or underestimated) conclusion about a treatment's true effect.
Purpose of testing for statistical heterogeneity
Assess variability in study results compared to chance alone
Waiting time from urgent cancer referral through to diagnosis and then treatment
62 days
The waiting time for treatment after a decision to treat is made
31 days
urgent cancer referral appt
2 weeks
Diagnostic confirmation target for cancer
28 days
Waiting time for non-urgent diagnostic test following a referral
6 weeks
Waiting time until start of consultant-led treatment for cancer
18 weeks
The Population Attributable Fraction (PAF)
expresses the proportion (percentage) of the total disease burden in the population that would be eliminated if the exposure were completely removed.
vital tool for prioritizing interventions because a common exposure with a small individual risk can have a larger PAF than a rare exposure with a high individual risk.
COst-benefit analysis
costs and benefits are expressed in monetary terms
The preferred option is the one with the greatest net benefit (benefits minus costs).
Icremental cost statistics
Incremental Cost-Effectiveness Ratio (ICER),
evaluate the additional costs and health outcomes of a new intervention compared to a standard alternative.
measures the extra cost required to gain one additional unit of health (usually a Quality-Adjusted Life Year or QALY)
cost new intervention - cost baseline/ difference in health outcome between interventuon - baseline
Net Monetary Benefit (NMB)
is a key metric in health economics. It translates health outcomes (like Quality-Adjusted Life Years, or QALYs) into a monetary value by multiplying them by a society's or organization's willingness-to-pay (WTP) threshold
Translational research gap
The First Gap (Bench to Bedside): Translating fundamental scientific discoveries (the "bench") into safe, actionable treatments and products for patients (the "bedside"). [1]
The Second Gap (Evidence to Practice): Implementing proven products, therapies, and clinical guidelines into routine daily practice for healthcare professionals. [1, 2]