PSY 349: Psych of Addiction Final Exam Study
1/66
Earn XP
Description and Tags
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
Treatment for AUD Social Skill Training
Learning to cope with high-risk and difficult social situations through:
Receiving criticism
Refusing alcohol
Learn to initiate interactions, express thoughts/feelings
Group format
Effective as stand-alone, or in combo with coping skills training
This can be done through role playing, getting feedback, and getting education.
Stress Management Training
Goal: reduce physiological and psychological stress response
Cognitive: increase mindfulness, reframe catastrophic thoughts
Behavioral: replace maladaptive with adaptive coping behaviors
Physical: deep breathing, progressive muscle relaxation
Integrated into other therapeutic approaches
What is AA (Alcoholics Anonymous)?
A peer-led meeting that uses community support to maintain sobriety alongside following the Twelve-Step Facilitation Intervention (TSF). Some main ideas are:
Addiction is a disease and abstinence is the only way to recovery
Reduce denial over alcohol
Surrender control to a "higher power" (issues may arise when it comes to this, but God does not have to be defined as something specific)
Is AA Effective?
Systematic review of over 35 studies
Included 10,080 participants
AA was nearly always found to become effective than psychotherapy in achieving abstinence.
In addition, most studies showed that AA participation lowered health care cost.
AA works because it’s based on social interaction.
What mechanisms explain the effectiveness of AA?
Substitute dependency
Increased caring relationships
Increased spirituality (I.e., trust in "higher power")
External supervision
AUD FDA approved drugs - DISULFIRAM
(Antabuse) blocks aldehyde dehydrogenase in the liver and the brain
Elevated acetaldehyde causes nausea, vomiting, headache, and flushing.
Leads to negative reinforcement/aversive conditioning -> alcohol avoidance
Modest efficacy in preventing relapse
Moderate effects in reducing heavy drinking
AUD FDA approved drugs - NALTREXONE
Naltrexone is dosed 50 mg by mouth once daily or 380 mg via IM injection once monthly.
Endogenous opioids are released when drinking, contributing to positive reinforcement effects
By blocking this activity, (Antagonist) naltrexone reduces the rewarding effects of alcohol and results in reduction in alcohol intake.
Reduces craving in some and has moderate effects
AUD FDA approved drugs - ACAMPROSATE
Works on multiple brain systems to reduce cravings-especially if just stopped drinking, including reducing glutamate activity
Better outcomes with longer abstinence before drinking
Primarily supports abstinence in "relief drinkers"
Amphetamines (History)
Given to soldiers during WW2 to enhance alertness, decrease need for sleep.
"Go pills"
Wasn't frowned upon like other drugs that provided "an escape" instead enhanced mental capacity in civilians as well.
Nazi were supplied with a methamphetamine called Pervitin
American and British -> Benzedrine
Methamphetamine (MA)
MA is a derivative of amphetamine
Amphetamines were studied first time in the early 1930s.
CNC Stimulant: Stimulates the sympathetic nervous system
Medical use as a nasal spray – bronchial passage dilation, narcolepsy, reducing activity in hyperactive children, suppressing appetite, and enabling people to stay awake for extended periods.
Methamphetamine Main Effect
Increases level of dopamine, also noradrenaline and serotonin
MA enters the neuron through the dopamine transporter (DAT) and increases dopamine inside the cell by releasing it from vesicles.
This causes the transporter to reverse direction, leaving dopamine being pumped out into the synapse.
Also – minimally breaks down monoamine oxidase (important for metabolism in drugs).
Illegally manufactured by combining the amphetamines ephedrine or pseudoephedrine with other chemicals and added to a solvent such as gasoline and heated to crystallize.
Which schedule is Methamphetamine?
It's in schedule 2, available in prescription as Desoxyn to treat obesity and ADHD.
Methamphetamine as an amphetamine
Amphetamine is a racemic mixture of d-amphetamine and l-amphetamine. The d-isomer is more potent in the CNC and is primarily responsible for the therapeutic effects. Many medications contain primarily the d-isomer like Adderall
For binge-eating disorder, Lisdexamfetamine is used.
Lisdexamfetamine
Taken as an inactive compound
The body (mainly in the blood) converts it into dextroamphetamine
This leads to a slower, more controlled effect
Who is using it?
Historically, adult male with a lower-than-average income.
More recently, of all ages and economic status use methamphetamine.
Slightly higher in minority populations of color.
National Survey – 9.6 million U.S. residents aged 12 and older used methamphetamine at least once in their lifetime (4.7% of respondents)
There reports of 8th, 10th, and 12 graders using in the past 12 months as well.
Production and Use
Methamphetamine usage has experienced a global surge since the 1990s, becoming the second most abused substance worldwide, trailing cannabis.
In the 1960s and 1970s in the USA, motorcycle gangs based in California were the primary producers and distributors of methamphetamine, primarily appealing to white, male, blue-collar workers. Though that has changed over time.
Currently, most methamphetamine is the US is produced by transnational criminal organizations (TCOs) in Mexico.
How is Methamphetamine made?
Methamphetamine is made by chemically modifying pseudo-ephedrine
Pseudoephedrine is an ingredient found in many over-the-counter cold medicines
By restricting access to this "starting material," the law makes it harder to produce meth.
The Combat Methamphetamine Epidemic Act (2005)
Passed to reduce methamphetamine production. It requires pharmacies and retailers to:
Keep logs of purchases of pseudo-ephedrine products
Limit how much an individual can buy per day
These restrictions have significantly reduced domestic meth productions in the U.S (not outside though).
Administration and Addiction
Smoking/IV Injection is the fastest administration (takes seconds)
Sniffing: takes 3-5 minutes
Oral: takes 20-60 minutes
Highly lipophilic, meaning it easily dissolves in fat, allowing it to rapidly cross the blood-brain barrier and enter the brain quickly.
Why is smoking the most addictive administration?
Rapid delivery to brain
Sharp dopamine spike
Intense euphoria
Strong reinforcement -> addiction
Peak effects typically occur around 1-2 hours, and duration can last 6-12 hours, depending on dose and route.
Effects can last 6-12 hours (sometimes longer).
Long-Term Associated Harm
Impaired impulse control
Impaired working memory
Impaired judgement
Psychosis (paranoid delusions, hallucinations)
Decreased working memory
Premature aging
Dental problems (tooth decay and loss)
Dental Issues
Research suggests MA smoking has more deleterious effects on teeth due to the chemicals contacting enamel.
Also causes oral sores and infections
Injectors experience some decay due to dry month and excessive clenching and grinding
Enamel begins to flake off, and eventually teeth deteriorate
Increased Risks
Parkinson's disease
Depression
Schizophrenia
This is attributed to the neurotoxicity (adverse effects of the structure and/or function of the nervous system) of methamphetamine.
Impairment in Social Cognition
Meta-analysis MUD -> social cognition impairments the most significant cognitive deficits, partially theory of mind (ToM) and emotion processing.
Ability to make inferences about others' mental states and use them to understand and predict behavior.
Impaired facial expression recognition
Persist after abstinence
Gradually improve with time, especially with sustained recovery
Sometimes remains partially impaired long-term.
Psychotic Symptoms
Positive symptoms: Paranoid delusions, disorganized behavior, unusual thought content.
Most episodes are brief (hours to days)
Can persist for months and recure during periods of non-use
Delayed Lasting Type: A persistent subtype lasting more than one month and associated with 5 or more years of use
Use of antipsychotic medications (risperidone)
Abstinence – Psychotic symptoms generally resolve within 1 week.
Substance-Induced Psychotic Disorder
Presence of prominent hallucinations or delusions
Hallucinations or delusions develop during, or soon after, intoxication or withdrawal from a substance or medication to be known to cause psychotic symptoms.
Psychotic symptoms are not actually part of a psychotic disorder that is not substance-induced.
Psychotic symptoms do not only occur during a delirium.
Methamphetamine Psychosis
26% - 46% of individuals with MA dependence have MA psychosis
Risk factors
Poly substance use
Affective (mood) disorders
Antisocial personality disorder
Family psychiatric history
Sleep deprivation
Reported Positive Effects from MA Use
Increases alertness, concentration, attention
Decreases fatigue
Improves cognition
Increases libido
Increases sexual performance time
Some report enhanced sexual experience
Increases sense of well being
Hallucinogenic effects
Contingency Management
Provides incentives to reinforce positive behaviors (e.g., abstinence, compliance with treatment)
Ex: Vouchers, Gift Cards, Cash if drug negative urine tox screen.
Not therapy in a traditional sense
Rewards can be provided by the clinic or family or patient
Can be stand-alone or in combination with CBT/12 step.
Though it is least effective for those who reported a longer history of drug use or reported more methamphetamine use during baseline.
Treatment: BEAT Meth
Intervention leads to identification, management, and treatment engagement of ER patients with psychosis from meth use.
Includes:
Early identification
Treatment of psychosis
Transitioning to addiction treatment.
Research on BEAT Meth
BEAT Meth patients compared with ER patients with MA psychosis who were discharged:
3 times more likely to attend an outpatient addiction appointment in 30 days, after discharge than comparison patients
Analyses suggested that increased attendance at outpatient treatment reduced ER utilization.
Cannabis Genetic Stains
Cannabis contains dozens of psychoactive compounds, most notably:
THC (∆9-tetrahydrocannabinol) - primary intoxicating compound
∆8-THC, THC – milder or modified psychoactive effects
CBD (cannabidiol) - not strongly intoxicating, but can modulate THC effects
Other cannabinoids that may have no, mild, or indirect psychoactive properties.
Cannabis contains over 100 different cannabinoids.
Marijuana Intoxication: Common Experiences Used Questionaries
Psychotropic Effects – ∆9 – tetrahydrocannabinol
Time perception: time seems slower
Has helped Interpersonal Relationships – may make a person more talkative
Cognition: varies- some focus, sometimes AD short term memory is disrupted
Sensory effects: visual, auditory, touch, taste
Thought process: attention, focuses, short term memory issues
Last 3-4 hours
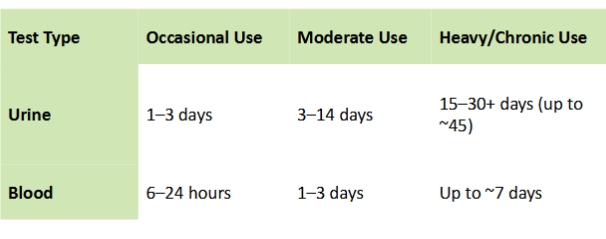
THC Detection Windows
Variety and Diversity
Different flowers like Sativa and Indica
Not well regulated in dispensaries
There are so many mixtures it's difficult to define the genetic profile of specific strains
Indica
Associated with Cannabis indica plants
Often described as producing more "body" or relaxing effects
Typically shorter, bushier plants with broader leaves
Commonly associated with:
Sedation or relation
"Couchlock" feeling (in higher THC varieties)
Sativa
Traditionally associated with Cannabis sativa plants
Often described as more "uplifting" or "energizing"
Taller plants with narrower leaves
Commonly associated with:
Increased alertness or stimulation
Is it really Sativa or Indica?
One study found that indica/sativa labeling was misleading, as well as the names given to strains.
Overall, strain names are often not reliable indicators of a plant's genetic identity and chemical profile.
Cannabis: Morphology (look) vs Chemistry
Morphology is not a reliable predictor of effects
Modern research shows:
Plants appearance (Morphology) does not reliably predict chemical composition
"Indica vs Sativa" is a poor proxy for pharmacological effects
Type 1: level of THC and CBD (Chemotypes)
THC level – High (>0.3%) can reach 30%
CBD level – Low (<0.5%)
Primary profile: THC-dominant (intoxicating, more of a high)
Type 2: level of THC and CBD (Chemotypes)
THC level: Moderate – High
CBD level: Moderate – High
Primary profile: Mixed ration profile of CBD and THC Balanced THC/CBD like Sativex mouth (oromucosal) spray containing equal parts of each. For MS in UK.
Type 3: level of THC and CBD (Chemotypes)
THC level – Low (<0.3)
CBD level – High
Primary profile: CBD dominant (non-intoxicating or minimal intoxication)
Is a prescribed cannabidiol for seizure associated in patients 1 year of age or older
Global Prevalence
~220 million people (about 4% of the global population aged 15-64) reported use in 2021.
Risk of addiction:
~10% of individuals who use cannabis develop Cannabis Use Disorder (CUD)
Cannabis Use in NYS (Adult 18+)
Based on a New York 2021 study, an estimated 1.6 million NYS adults (12.8%) report using cannabis in the past 30 days.
44% use it for non-medical reasons alone, 36% for medical and non-medical reasons, and 19% for medical reasons only.
Frequency of Use:
Less than 20 days/month: 6.8%
Daily or near daily use (20 days/month): ~6% of all adults
Mode of Use
Smoking: 73.8%
Edibles (eating): 12.1%
Vaporizing: 9.3%
Why do adults use cannabis?
Change states:
Creativity – Does it make people creative?
Convergent (logical, linear, analytical) to divergent thinking (Creative, free-flowing, associative)
Relaxation
Sleep (could be due to the withdrawal effects?)
Medical use
College Students
College students and young adults most commonly use cannabis to:
Socially Conform (42%)
Experiment (29%)
Enjoyment (24%)
12% - primarily use it for stress or relaxation.
Studies also report use for self-medication -> depression, anxiety, social anxiety, and post-traumatic stress disorder (PTSD).
Adolescents
Use typically begins during this time
Most use psychoactive substance
8% in the US and 16% in Europe
In 2022, 30.7% high school seniors reported using cannabis in the year.
6.3% in the past 30 days.
This is during a time of critical neurodevelopment where the endocannabinoid system plays a significant role in this process.
Adolescent Cannabis Use: PFC Morphology
Cannabis use assessed at (N=637) Ages 14 and age 19 using self-report questionnaire.
Strength of the connection between cannabis use and Dorsolateral Prefrontal Cortex thinning from ages 14 to 19 was 100%.
Paranoia/Psychosis
Approximately 30% during acute intoxication (THC)
Self-Consciousness
Hypervigilance
Social Anxiety
Conspiracies
Depersonalization (feeling detached from oneself)
Derealization (feeling detached from the surrounding world)
Risk factors for paranoia and psychosis
Individual differences
History of anxiety disorders, psychosis
Genetic predisposition (such as certain COMT gene variants) may be more susceptible to paranoia when using THC.
COMT gene helps break down and regulate dopamine in the brain
Two common variants affecting dopamine levels:
Val variant – higher COMT activity -> lower dopamine
Met variant – lower COMT activity -> higher dopamine
This effect may be stronger in people with the MET variant
This can increase risk of:
Psychosis – like symptoms
Worsening symptoms in those already vulnerable
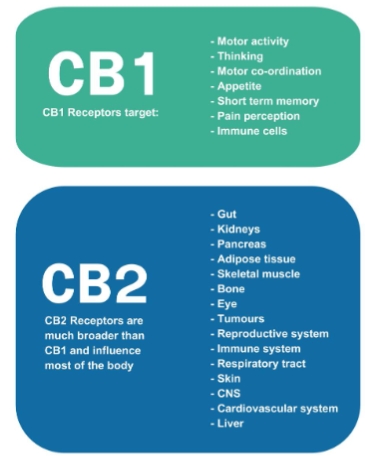
Endocannabinoid System
Activation of these receptors leads to the release of endocannabinoids, that function as neuromodulators, releasing other neurotransmitters.
Main Endogenous/Endocannabinoids: 2-Arachidonoylglycerol (2AG), and Anandamide (EAE)
Naturally produced inside the body
Main Exogenous Cannabinoids: ∆9
Come from cannabis and other similar drugs
∆9 – Tetrahydrocannabinol
Main compound that produces the psychoactive effects
Occurs in concentrations from 0.5%-20% depending on cultivar and processing.
Higher affinity for endogenous cannabinoid (CB1) receptors
Increases VTA dopamine
Main Exogenous Cannabinoids: CBD
CBD (Cannabidiol)
Much less noticeable psychoactive effects
Some report anxiolytic and analgesic
Modulates action of THC
Low affinity relative to THC
Some research suggests it negates negative effects of THC
Main Endogenous Cannabinoids: EAE
Anandamide (EAE) Sanskrit word Ananda, meaning "joy, bliss"
Affinity for CB1 cannabinoid receptors in the central nervous system
Affect neurotransmission of dopamine, serotonin, GABA, and glutamate
Levels can increase through:
Exercise
Social contact – mobilization of anandamide in the nucleus accumbens
Chocolate
Main Endogenous Cannabinoids: 2-AG
High binding to CB2 receptors, which are predominantly found in the brain and central nervous system
Bind to CB2 receptors in the immune system and has a role in immune response and inflammation.
Has been shown to protect neurons from damage and regulate neuroinflammatory responses.
Being studied in conditions like stroke and neurodegenerative diseases.
Down-Regulation (decrease in receptors/sensitivity) in the Endocannabinoid System leads to:
Anxiety
Difficulty sleeping
Depressed mood
Avolition (decrease in motivation)
Cannabis Withdrawal
Three or more of the following signs and symptoms develop within approximately 1 week after cessation of heavy, prolonged use:
Nervousness or anxiety
Sleeping difficulty (I.e., insomnia, disturbing dreams)
Decreased appetite or weight loss
Restlessness
Depressed mood
At least one of the following physical symptoms causing significant discomfort: abdominal pain, shakiness/tremors, sweating, fever, chills or a headache.
These signs or symptoms cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
Dopamine and THC
THC causes a release of dopamine in the ventral striatum in human imaging studies.
Decreased dopamine brain reactivity in marijuana abusers is associated with negative emotionality and addiction severity.
Research on Dopamine & THC
Researchers compared the brain's reactivity in heavy cannabis use vs control when challenged with methylphenidate (MP).
Results: Cannabis group display attenuated dopamine responses (DA) to MP, including reduced decreases in striatal distribution volumes (nucleus accumbens, reward, motivation, emotion)
Population Research
As cannabis use increases – rates of schizophrenia and psychosis increase.
Cannabis Potency - concentration of ∆9 – Tetrahydrocannabinol
20 studies N=229,581
Those who reported daily higher potency cannabis use were 5 times more likely to be diagnosed with a psychotic disorder compared with those who never used cannabis.
Strongest finding: Use of higher potency cannabis compared to lower potency was associated with an increased risk of psychosis and CUD.
Cannabis-induced Psychotic Disorder
Presence of delusions or hallucinations.
Evidence from the history, physical examination, or laboratory findings of either one of the following:
The symptoms in the first criterion developed during or soon after cannabis intoxication or withdrawal.
The disturbance is not accounted for by psychotic disorder that is not substance induced.
Long-Term Use and Cognitive Reserves Study
Longitudinal cohort study:
1,037 individuals from Dunedin, New Zealand born 1972-1973
Follow up: From childhood to age 45 (94% retention)
Assessments
Cannabis use/dependence: Ages 18, 21, 26, 43, 38, 45
IQ testing: Ages 7, 9 , 11, and 45
Age 45 measures:
Neuropsychological testing
Hippocampal brain volume (MRI)
Long-Term Use and Cognitive Reserves Study: Results
Long-term cannabis users showed:
IQ decreased ~5.5 point decline from childhood to midlife
Worse learning and processing speed
Memory and attention problems (informant reports)
Effects were not explained by:
Alcohol or tobacco use
Other drug use
Childhood SES or personality factors
Brain findings
Smaller hippocampal volume
But this did not explain cognitive decline
Cannabis Use and Schizophrenia
Landmark study (1987) 45,000 Swedish military enlisters at 19 and 15 years later.
Those who used cannabis more than 50 times before enlistment were 6x more likely to meet criteria for schizophrenia at 15 year check in.
After controlling for ACE's and other Psychiatric disorders.
Chicken-egg? (directionality)
Impairs in neuropsychiatric, physical, and social domains