Exam 5 - Comfort, Stress & Coping, Grief & Loss, Tissue Integrity
1/155
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
156 Terms
Norman
Age 58, 2nd post op day following abdominal surgery
Laughing, smiling
BP 126/76, P 67, R 16
Pain score of 8 when asked
What do you think his pain score is?
8
James
Age 25, 2nd post-op day following abdominal surgery
Quiet, expressionless, talking little
BP 122/76, P 70, R 18
Pain score 1 when asked
What do you think his pain score is?
1
nociceptive pain
acute pain; a pain sensation that results abruptly
a type of pain caused by damage to body
tissue•Initiated by nociceptors (pain receptors) that are activated by the injury to the body
Considered the normal pain process
phases of nociceptive pain
1. Transduction
2. Conduction
3. Transmission
4. Perception
5. Modulation
transduction of pain
painful stimuli is converted into nerveimpulses that travel to the CNS
transmission of pain
nerve impulses are transmitted to the CNS and then to the brain
-A-delta fibers are rapid
-C fibers carry impulses slower
perception of pain
the sensory process that occurs with painful stimuli, individual's interpretation of the pain
modulation of pain
the process by which the body alters a pain signal as it is transmitted to the CNS
-Neuromodulators
-Endorphins
-Drugs
gate control theory of pain
The theory that pain is a product of both physiological and psychological factors that cause spinal gates to open and relay patterns of intense stimulation to the brain, which perceives them as pain.
OPENING GATE
allows transmission of pain
Physical Factors Bodily injury
Emotional Factors Anxiety & Depression
Behavioral Factors Attending to the injury & concentrating on the pain
Closing the gate
Physical FactorsAnalgesic Remedies
Emotional FactorsBeing in a ‘good’ mood
Behavioral FactorsConcentrating on things other than the injury
Friction
When you rub a part of your body it causes friction, friction signals compete with pain signals to pass through the gate, if both signals are trying to get through, the friction signal will make it first.
types of pain
Acute
Chronic
Cutaneous
Somatic
Visceral
Referred
Phantom
Intractable
Cutaneous pain examples
affects the skin:
cut
sunburn

somatic pain
originating from muscle, bone, joints, tendons, or blood vessels
visceral pain
a poorly localized, dull, or diffuse pain that arises from the abdominal organs, or viscera
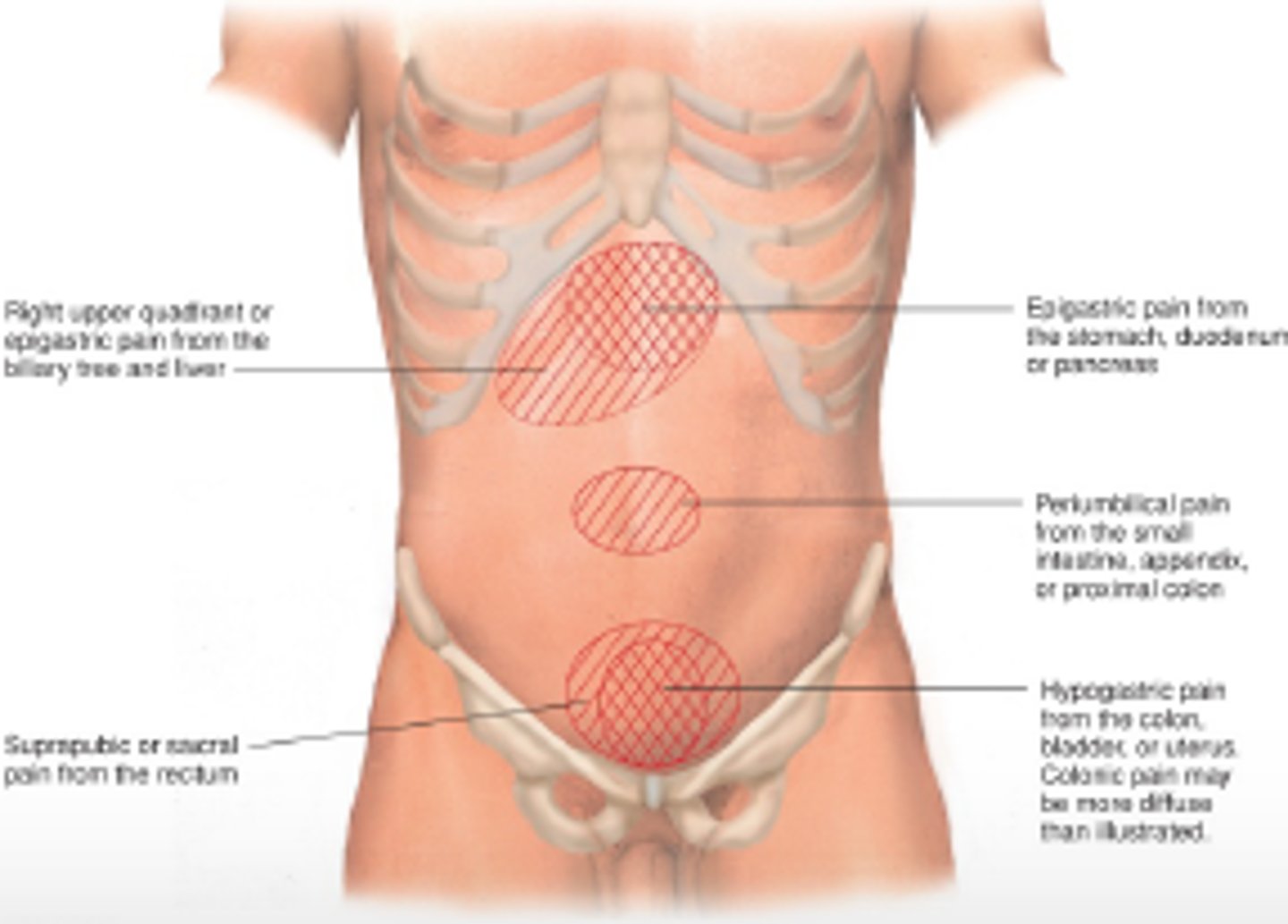
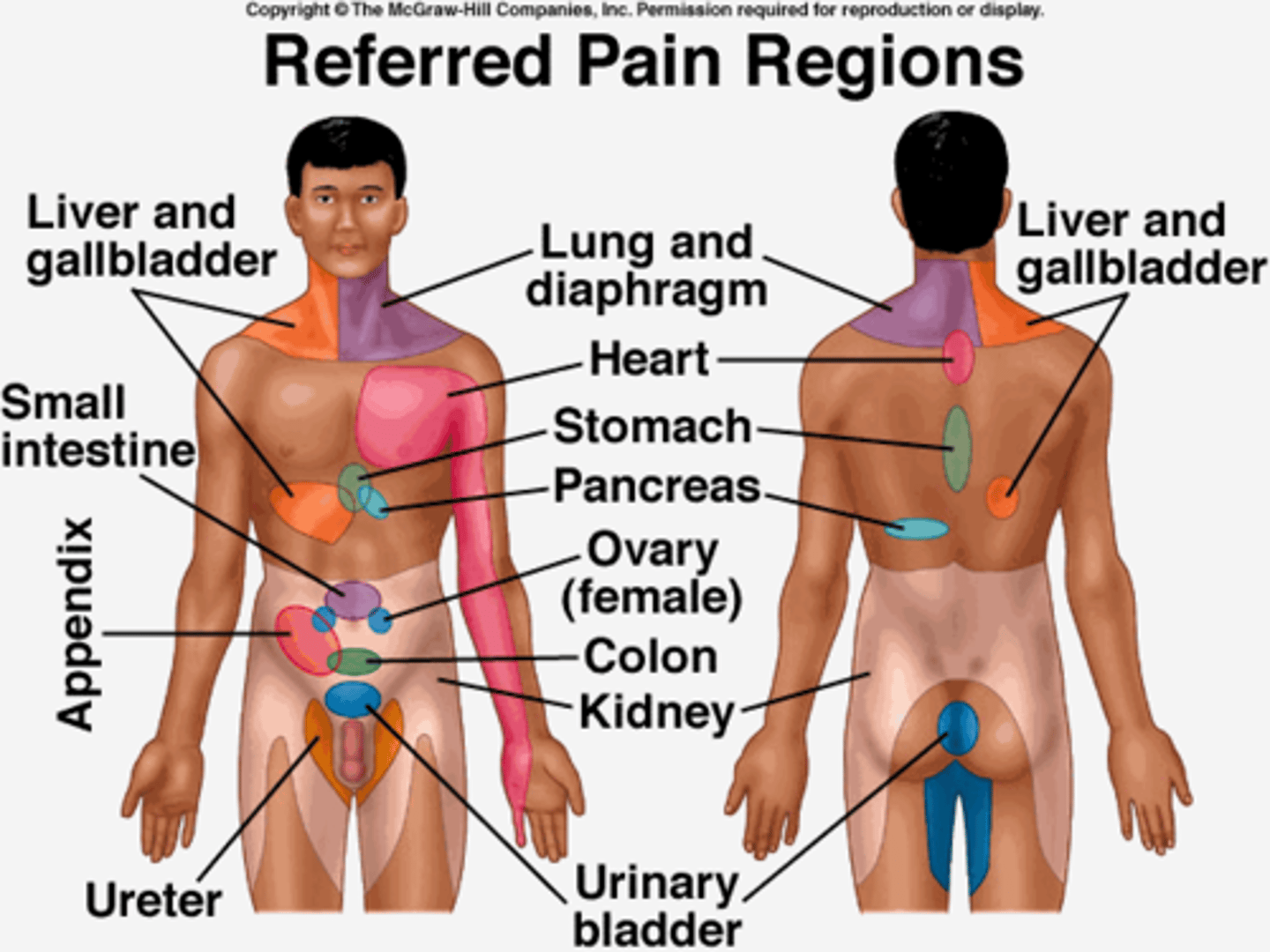
referred pain
pain felt in a part of the body other than its actual source
phantom pain
pain or discomfort felt in an amputated limb

intractable pain
severe pain that is extremely resistant to relief measures

Barriers to pain management
Multidisciplinary factors
- Lack of knowledge / skill to assess / treat pain
- Concern about regulation of controlled substances
- Personal values / feelings regarding the use of opioids
Patient factors
- Perception / unwillingness to report pain
- Fear of pain addiction, tolerance, and other side effects
of opioids
- High cost of medications
Common biases about pain
Drug abusers & alcoholics overreact to pain
False—they are actually giving you a more truthful perception since inhibitions are lowered
Patients with minor illnesses have less pain
False—for that patient, the experience could be major depending on previous experience
Giving analgesics regularly will start drug dependency
False—studies show only 3% of patients ever develop a true addiction
Amount of damage dictates pain intensity
False—minor injuries may cause excruciating pain
Health care personnel know best the nature of the patient’s pain
False—the patient knows best his or her pain
Pain Assessment
Provocative or Palliative (what makes it worse/better)
Quality or Quantity (For example, is the pain sharp or dull, throbbing?)
Region or Radiation(Location)
Severity Scale (Numeric pain intensity scale)
Timing (Onset)
Understand Patient's Perception (Activities of Daily Living assessment)
Pain indicators
•Vital signs initially showing an elevation in BP, P and RR
•With prolonged, severe, and visceral pain there can be a decrease in blood pressure and heart rate
•Muscle tension or rigidity
•Pallor
•Nausea and vomiting
•Fainting
•Withdrawal to pain
•Grimacing
•Restlessness
Guarding the area of pain
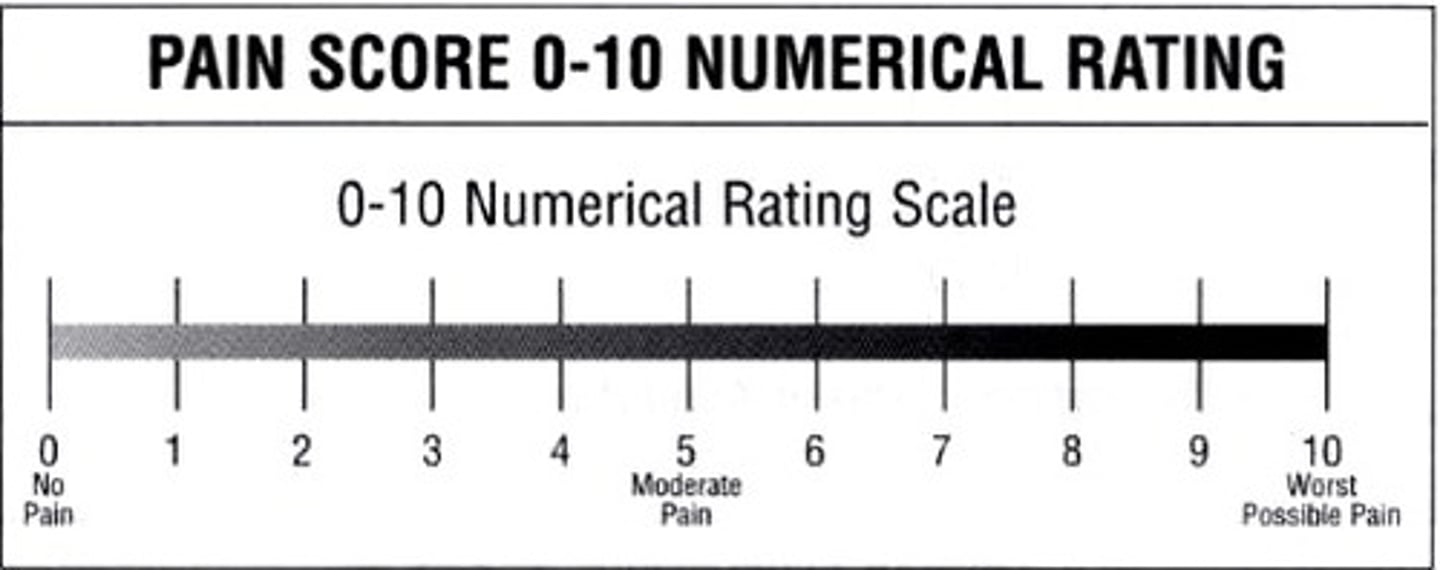
Numeric pain scale
0-10
>9 years old
FACES pain scale
for children 4-16, mentally disabled, or language barrier

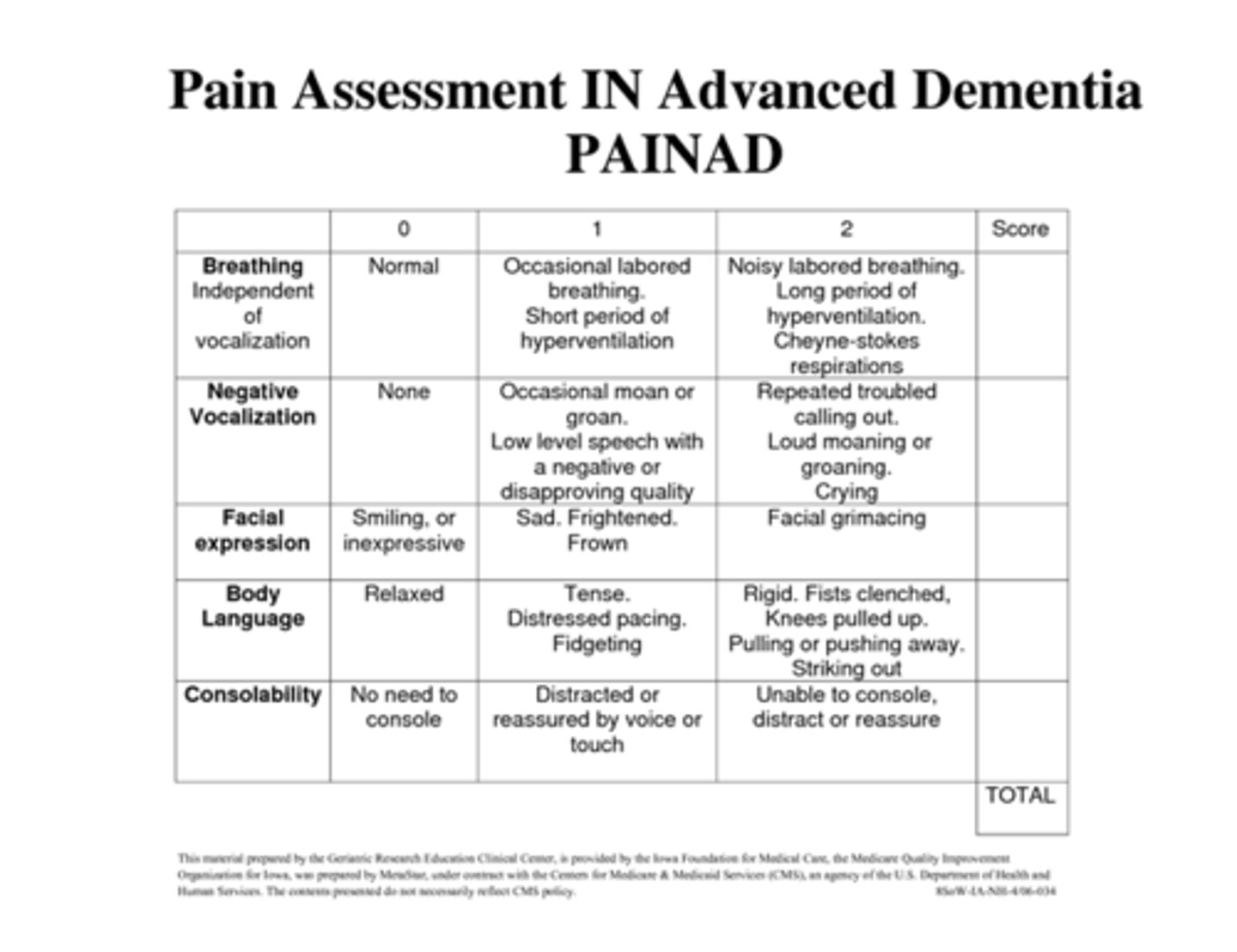
PAINAD
pain assessment in advanced dementia
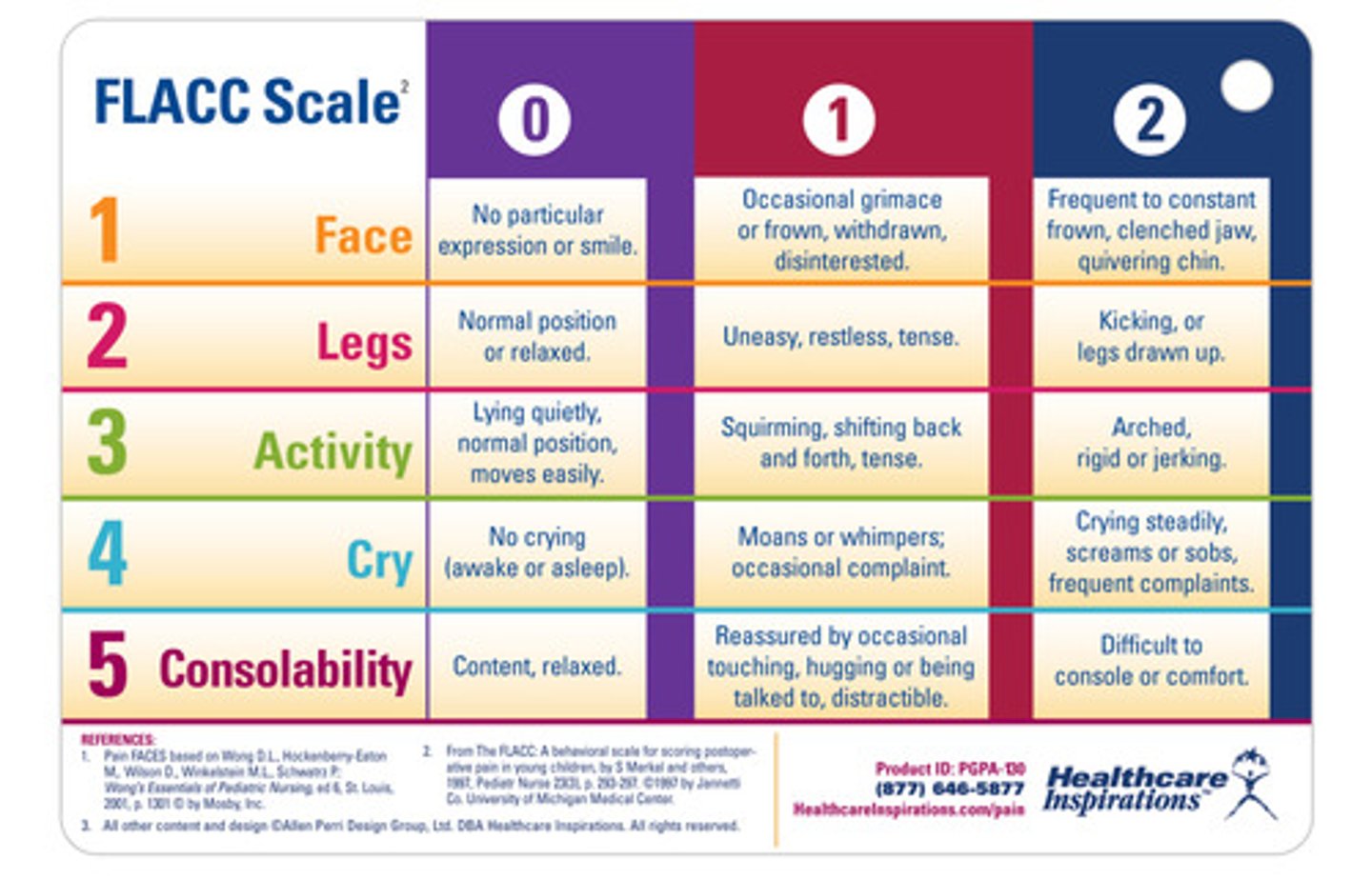
FLACC Behavioral Scale
Pediatric patients (2 months-7 years)
A RN is caring for a post-op patient who says he is worried about being discharged after surgery b/c he has no place to live. Describe how this can contribute to his pain perception.
Stress can increase pain perception
Get social worker or case manager involved
Can patients bring their own herbal remedies?
Yes w/ MD ok and they need to sign a waiver
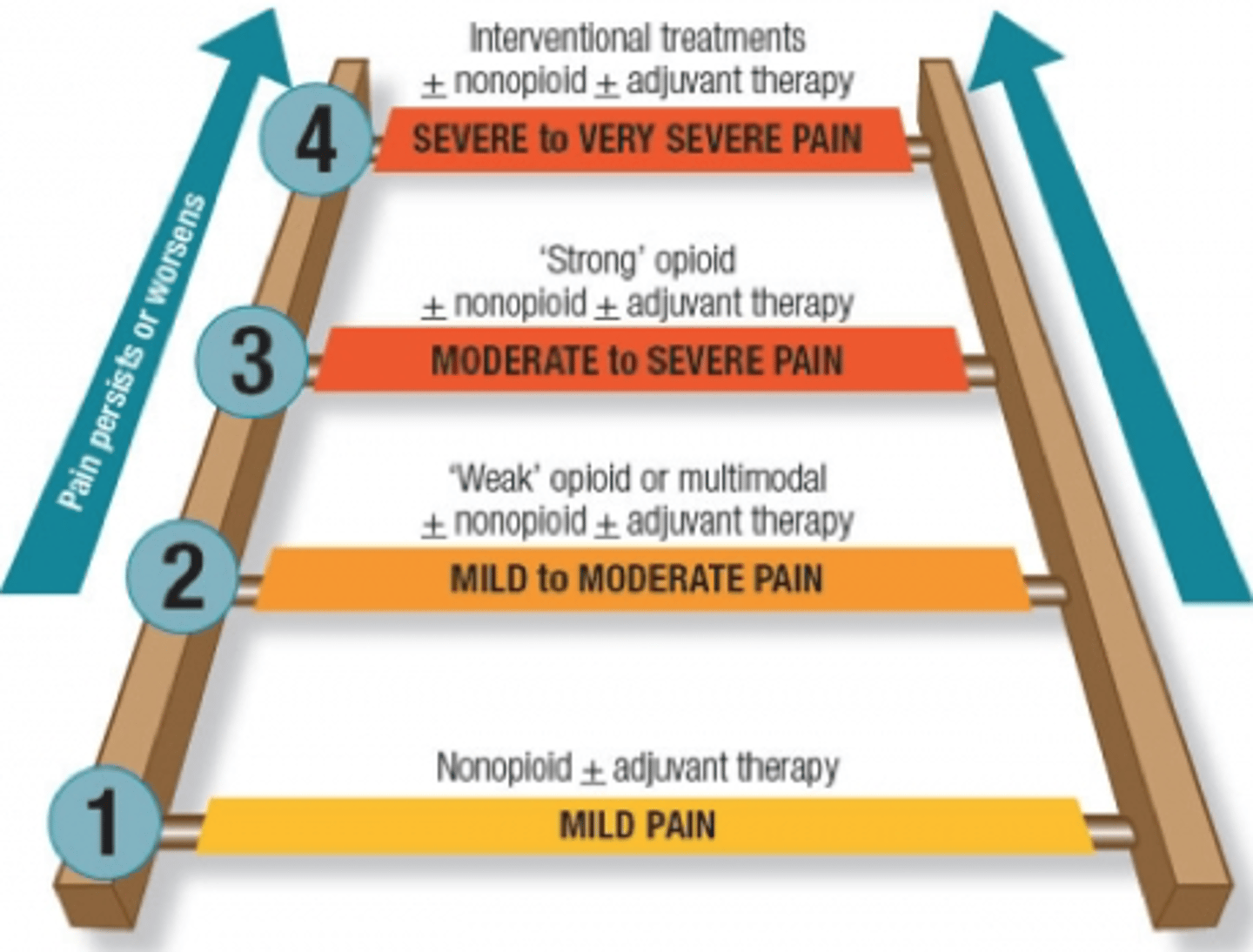
WHO pain ladder
1. tylenol/aspirin/NSAIDs
2. mild opioid - Tylenol/codeine/oxycodone
3. stronger opioids -
morphine/dilaudid/MS-Contin
What is the maximum amount of tylenol that should be given per day?
4000 mg
adjuvant therapy
Enhance pain control or relieve symptoms associated with pain:
•Sedatives, anti-anxiety, & muscle relaxants:
Vistaril, Elavil, Thorazine, Valium, Ativan, Xanax
•Antidepressants, anticonvulsants, topical analgesics, muscle relaxants, antianxiolytics, corticosteroids
PCA pump
patient-controlled analgesia administered intravenously with a machine
Only to be pressed by the patient!
Look for # times button pressed and doses received
-If they press 27 times tells us they are in a lot of pain
-If they press 1 time tells us they may not need PCA
•Adverse events occur 50% less with PCA than usual therapy
•Safe method for post-op, traumatic, or cancer pain
•Syringe is a prescribed opioid: morphine, fentanyl, or hydromorphone
***2nd RN must cosign the amount and machine setting***

side effects of pain medication & their interventions
Constipation
Fluids, fruit, prunes, Senokot, Colace
Nausea / Vomiting
Antiemetics- Zofran, Reglan
Sleepiness
Body will usually adjust
Itching
Benadryl may be useful for different things such as sleeping and itching. Order must have correct indication
Non-Pharmacologic pain interventions
•Relaxation
•Music
•Guided Imagery
•Distraction (music/movies)
•Acupressure/acupuncture
•Pastoral counseling/prayer
•Therapeutic touch
•Repositioning
•Heat/Cold Therapy (Caution w/ PVD)
•Electronic Stimulating Unit
When administering opioids, what should be available?
Naloxone
effects of undertreated acute pain
•Respiratory - decreased cough and lung volume, atelectasis, sputum retention, infection, hypoxemia
•Cardiovascular - tachycardia, hypertension, increased myocardial oxygen consumption, myocardial ischemia
•Gastrointestinal - decreased gastric and bowel motility
•Genitourinary - urinary retention
•Neuroendocrine - increase in levels of catecholamines, cortisol, glucagon, growth hormone, vasopressin, aldosterone and insulin
•Psychological - anxiety, fear, lack of sleep
•Musculoskeletal - muscle spasm, immobility (increasing risk of deep venous thrombosis)
A nurse is providing teaching to a client who is postoperative following coronary artery bypass graft (CABG) surgery and is receiving opioid medications to manage discomfort. Aside from managing pain, which of the following desired effects of medications should the nurse identify as most important for the client's recovery?
(a) It decreases the client's level of anxiety.
(b) It facilitates the client's deep breathing.
(c) It enhances the client's ability to sleep.
(d) It reduces the client's blood pressure.
(b) It facilitates the client's deep breathing.
A nurse is caring for a client who has peripheral vascular disease and reports difficulty sleeping because of cold feet. Which of the following nursing actions should the nurse take to promote the client's comfort?
(a) Rub the client's feet briskly for several minutes.
(b) Increase the client's oral fluid intake.
(c) Obtain a pair of slipper-socks for the client.
(d) Place a moist heating pad under the client's feet.
(c) Obtain a pair of slipper-socks for the client.
A nurse is caring for a client who came to the emergency department with abdominal distention and is now on the medical-surgical unit with an NG tube in place to low gastric suction. The client is reporting anxiety, discomfort, and a feeling of bloating. Which of the following actions is the nurse's priority?
(a) Request a prescription for a medication to ease the client's anxiety.
(b) Irrigate the NG tube with 100 mL of sterile water.
(c) Check to see if the suction equipment is working.
(d) Remove and reinsert the NG tube.
●
(c) Check to see if the suction equipment is working.
A nurse is providing teaching to a client who takes opioid pain medication and has a new prescription for docusate sodium. Which of the following statements by the client indicates an understanding of the teaching?
(a) "I will take the medication for diarrhea."
(b) "It might take up to 3 days for the medication to work."
(c) "I can take this medication along with mineral oil."
(d) "I should drink 4 ounces of water when I take the medication."
●
(b) "It might take up to 3 days for the medication to work."
John Mercuro is a 42 year old male with chronic back pain who receives Oxycontin 40 mg bid at home. He had surgery today for posterior spinal fusion of L5-S1. He came from PACU to the surgical floor 4 hours ago. He is currently receiving Hydromorphone (Dilaudid) PCA for pain control. PCA settings: 0.2 mg continuous, 0.1 mg bolus every 10 min with a 4 hour max of 6 mg. He has been complaining of increased pain the last 2 hours despite using the PCA every 10 min so you have increased the bolus to 0.2 mg every 10 min (which is the high range) the physician has stated in the initial post-op PCA orders.
What are your nursing priorities?
Get baseline vitals
Look for changes in LOC
Utilize other pain management techniques
Make sure to check pt frequently
24-hour pulse-ox
examples of physiological stressors
•Chemical agents
•Physical agents
•Infectious agents
•Nutritional imbalances
•Hypoxia (opioids, PE, ect.)
•Genetic or immune disorders
What is the #1 reason for nutritional imbalance caused in hospital?
NPO status
Examples of psychological stressors
•Accidents
•Stressful or traumatic experiences of family members and friends
•Horrors of history
•Fear of aggression or mutilation
•Events of history that are brought into our homes through television and the internet
•Rapid changes in the world
local adaptation syndrome (LAS)
localized response of the body to stress, precipitated by trauma or pathology
•Involves only a specific body part (such as a tissue or organ) instead of the whole body
•Stress precipitating the LAS may be traumatic or pathologic
•Primarily homeostatic short-term adaptive response
Two types: reflex pain response and inflammatory response
General Adaptation Syndrome (GAS)
a 3-stage physiological response that appears regardless of the stressor that is encountered
1. alarm
2. resistance
3. exhaustion
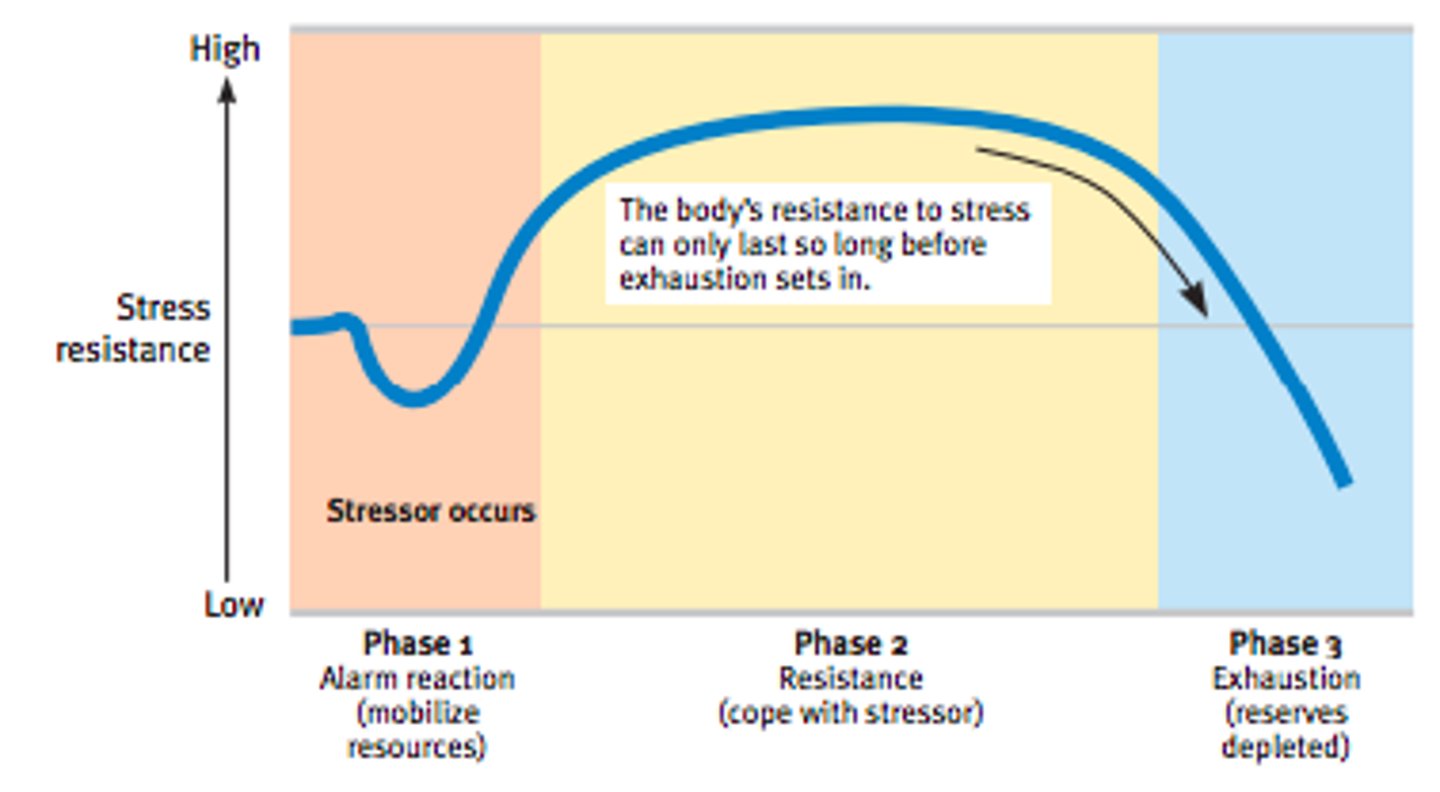
Alarm Reaction Stage
•Person perceives stressor, defense mechanisms activated
•Fight-or-flight response
•Hormone levels rise, body prepares to react (Epinephrine, Cortisol - decreases immune response)
•Shock and counter-shock phases
Elevated BP
Elevated HR
Elevated Muscle tension
Glucose regulation disrupted
Lowered immune system
stage of resistance
•Body attempts to adapt to stressor
•Vital signs, hormone levels, and energy production return to normal
Body regains homeostasis or adaptive mechanisms fail

stage of exhaustion
•Results when adaptive mechanisms are exhausted
•Body either rests and mobilizes its defenses to return to normal or dies
Chronic stage of stress
AKI & CHF from elevated BP
Best resource is social worker
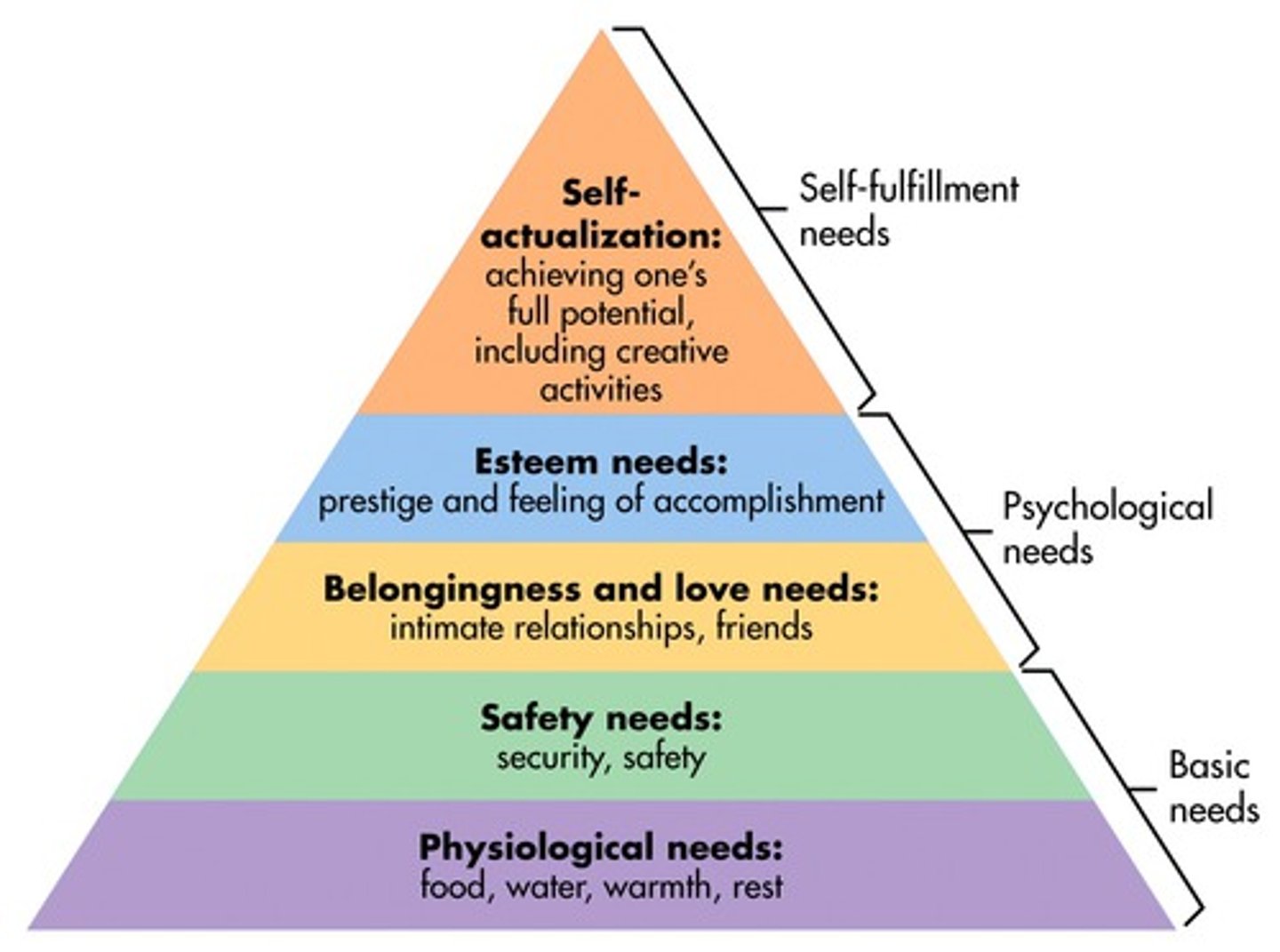
Maslow's needs pyramid
physiological, safety, belongingness and love, esteem, self-actualization
emotional responses to stress
Mind-body interaction
Coping mechanisms
Anxiety (most common)
>Mild
>Moderate
>Severe
>Panic
•Anger
•Depression
•Hopelessness
•Difficulty concentrating
•Difficulty in decision making

immune response to stress
*Inhibition of the immune system starts when stressors lessen in the recovery phase
pain
vasodilation
swelling
WBCs & lymphocytes
hyperglycemia [Normal blood sugar 70-110, at 150 start intervention (insulin)]
mild anxiety
This first level of anxiety occurs in the normal experience of everyday living and allows people to perceive reality in sharp focus.
moderate anxiety
•Occurs as anxiety escalates, perceptual field narrows, and details are excluded from observation
•Selective inattention: only certain things are seen and heard
•Manifested by increased HR, perspiration, mild somatic symptoms
severe anxiety
•Perceptual field is greatly reduced
•May focus on particular detail or scattered details
•Learning and problem solving not possible
•Manifested by erratic, uncoordinated, and impulsive behavior
severe anxiety
•Most extreme for and results in markedly disturbed behavior
•Loss of reality focus
•Manifested by confusion, shouting, screaming, withdrawal
stress coping mechanisms
•Crying, laughing, sleeping, cursing
•Physical activity, exercise
•Smoking, drinking
•Lack of eye contact, withdrawal
•Limiting relationships to those with similar values and interests
Task-Oriented Reactions to Stress
1. Attack behavior
2. Withdrawal behavior
3. Compromise behavior (normal)
defense mechanisms
in psychoanalytic theory, the ego's protective methods of reducing anxiety by unconsciously distorting reality
•Compensation
•Denial
•Displacement
•Introjection
•Projection
•Rationalization
Which defense mechanism is portrayed in the following scenario? After throwing his lunch tray on the floor, a patient complains to the nurse manager about the quality of the food he is being fed during his hospital stay.
A. Denial
B. Displacement
C. Rationalization
D. Reaction formation
Answer: C. Rationalization
Rationale: In rationalization, a person tries to give a logical or socially acceptable explanation for questionable behavior. A person in denial refuses to acknowledge the presence of a condition that is disturbing. Displacement refers to a person transferring an emotional reaction from one person to another. Reaction formation occurs when a person develops conscious attitudes or behaviors opposite to what he desires to do.
reaction formation example
being rude to someone you're attracted to
displacement example
A client is angry at his doctor, does not express it, but becomes verbally abusive with the nurse.
effects of long term stress
•Affects physical status
•Increases risk for disease or injury
•Compromises recovery and return to normal function
•Is associated with specific diseases
Family Stressors
•Changes in family structure and roles
•Anger and feelings of helplessness and guilt
•Loss of control over normal routines
•Concern for future financial stability
developmental stress
occurs when a person progresses through stages of growth and development
Examples: dealing with strangers as an infant, being separated from parents, starting or changing schools, and adjusting to puberty.
situational stress
short-term anxiety caused by a situational factor
•does not occur in predictable patterns
•E.g. illness or traumatic injury, marriage or divorce, loss, new job, role change
Tell whether the following statement is true or false:
An example of situational stress is the stress related to a marriage or divorce.
A. True
B. False
A. True
Rationale: An example of situational stress is the stress related to a marriage or divorce.
nursing stressors
•Assuming responsibilities for which one is not prepared
•Working with unqualified personnel
•Working in an environment in which supervisors are not supportive
•Caring for a patient in cardiac arrest or a dying person
Experiencing conflict with peers
Teaching Healthy Activities of Daily Living
1. Exercise
2. Rest and sleep
3. Nutrition
4. Use of support systems
5. Use of stress management techniques
Stress management techniques
•Relaxation
•Meditation
•Anticipatory guidance
•Guided imagery
•Biofeedback
•Crisis intervention
Anticipatory guidance
Patient/family counseling which includes information, advice, and suggestions about expected health-related life occurrences, health maintenance, and preventive plans.
Guided imagery
a technique of relaxation and pain control in which a person conjures up a calming picture that is held in mind during a painful or stressful experience.
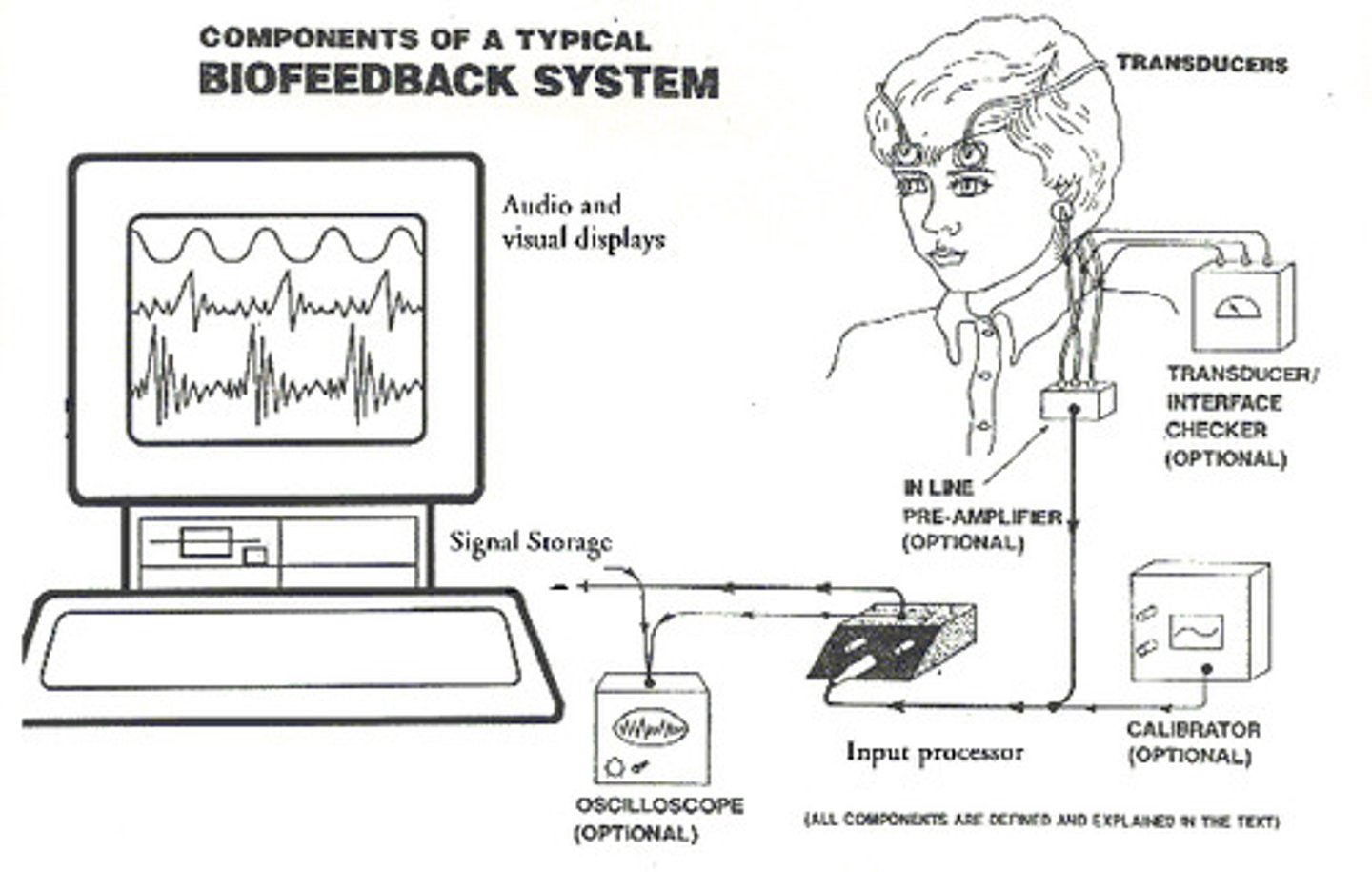
Biofeedback
the use of an external monitoring device to obtain information about a bodily function and possibly gain control over that function
Tell whether the following statement is true or false:
In the stress management technique known as anticipatory guidance, a person creates a mental image, concentrates on the image, and becomes less responsive to stimuli.
A.True
B.False
Answer: B. False
Rationale: In the stress management technique known as guided imagery, a person creates a mental image, concentrates on the image, and becomes less responsive to stimuli.
types of loss
Actual
Perceived
physical vs. psychological
maturational
Situational
Anticipatory
actual loss
loss that can be recognized by others
such as the loss of a limb or a spouse
perceived loss
felt by person but intangible to others
loss of youth, of financial independence, and of a valued environment experienced by a person, but intangible to others
Physical loss vs. psychological loss
Physical loss is the actual loss of a physical object (ex. Limb)
psychological loss relates to the altered self-image and the life changes that come with losing the limb
Maturational loss (developmental loss)
Any loss associated with the developmental processes of loss such as a child leaving their parents home for college
situational loss
experienced as a result of an unpredictable event
anticipatory loss
loss has not yet taken place
bereavement
state of sorrow over the death or departure of a loved one
mourning
the act of showing sorrow or grief, including the symbols and ceremonies that make up outward expression of grief
5 stages of grief
1. Denial
2. Anger
3. Bargaining
4. Depression
5. Acceptance
Symptoms of grief
Depression, sadness, Fatigue, apathy, lack of interest, Sleep alterations, Loss of appetite, Change in sexual interest, Anxiety, shortness of breath, Feeling helpless, restless, angry, irritable, Forgetfulness, tendency to make mistakes, Confusion, disorientation, Symptoms of the same illness the deceased suffered, Seeing the loved one's presence, hearing the loved one's voice= paranormal experiences, A need to tell and retell things about the loved one
Medical criteria used to certify a death
Cessation of breathing
No response to painful stimuli
Lack of reflexes
Lack of spontaneous movement
Flat encephalogram
Components of a Good Death
Control of symptoms
Preparation for death
Opportunity to have a sense of completion of one's life
Good relationship with health care professionals
Brain death criteria
•Irreversible loss of all brain functions including the brainstem
•Occurs when the cerebral cortex stops functioning or is destroyed
•Exact definition of death can be controversial
Needs of Dying Patients
1. Physiologic needs: physical needs, such as hygiene,pain control, nutritional needs
2. Psychological needs: patient needs control over fear of the unknown, pain, separation, leaving loved ones, loss of dignity, loss of control, unfinished business, isolation
4. Spiritual needs: patient needs meaning and purpose, love and relatedness, forgiveness and hope
palliative care vs hospice care
Palliative Care occurs *throughout the course of the illness* and in any setting. It allows for curative therapies.
Hospice care occurs during the *last six months of life*. It can occur in the home, inpatient hospice units, and long-term care settings. The patient decides against life-sustaining therapy.
advance directive (living will)
•For anyone 18 and older
•Provides instructions for future treatment
•Appoints a Health Care Representative
•Does not guide EmergencyMedical Personnel
•Guides inpatient treatment decisions when made available
special orders
Allow natural death, do-not-resuscitate, or no-code Orders
Terminal weaning
Voluntary cessation of eating and drinking
Active and passive euthanasia
Palliative sedation
Comfort measures only
POLST (Physician Orders for Life-Sustaining Treatment)
For persons with serious illness— at any age
Provides medical orders for current treatment
Guides actions by Emergency Medical Personnel when made available
Guides inpatient treatment decisions when made available
active euthanasia
death induced deliberately, as by injecting a lethal dose of a drug
passive euthanasia
A situation in which a seriously ill person is allowed to die naturally, through the cessation of medical intervention.
Postmortem Care of the Body
1.Prepare the body for discharge.
2.Place the body in anatomical position, replace dressings, and remove tubes (unless there is an autopsy scheduled).
3.Place identification tags on the body.
4.Follow local law if patient died of communicable disease
Postmortem Care of the Family
1.Listen to family's expressions of grief, loss, and helplessness.
2.Offer solace and support by being an attentive listener.
3.Arrange for family members to view the body.
4.In the case of sudden death, provide a private place for family to begin grieving.
5.It is appropriate for the nurse to attend the funeral and make a follow-up visit to the family.
Functions of the skin
Protects underlying tissues / structures
Enables sensation perception
Temperature regulation
Psychosocial
Assists with vitamin D production
Absorbs medications
Eliminates water/lytes/waste
Types of skin assessment
1. Quick peek assessment
2. Systematic head-to-toe skin assessment
3. Wound assessment (for ongoing wound monitoring)
Skin Assessment
color, moisture, temperature, texture, turgor, vascularity, edema, lesions