HSCI 204 Midterm ( practice questions before final exam) its already done, from past lecture.
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
Describe environmental health
relationships between people and their environment. Example, how environmental health impacts quality of life.
What is planetary health?
New field that focuses on health of civilians but also the system that civilians depend on (the planet).
Accounts for the importance of natural systems
How are planetary health and environmental health similar?
Both look at human health but also exposures outside of the body
Population growth and urbanization?
As population increases so does urbanization(overcrowding). People move from rural areas to urban areas.
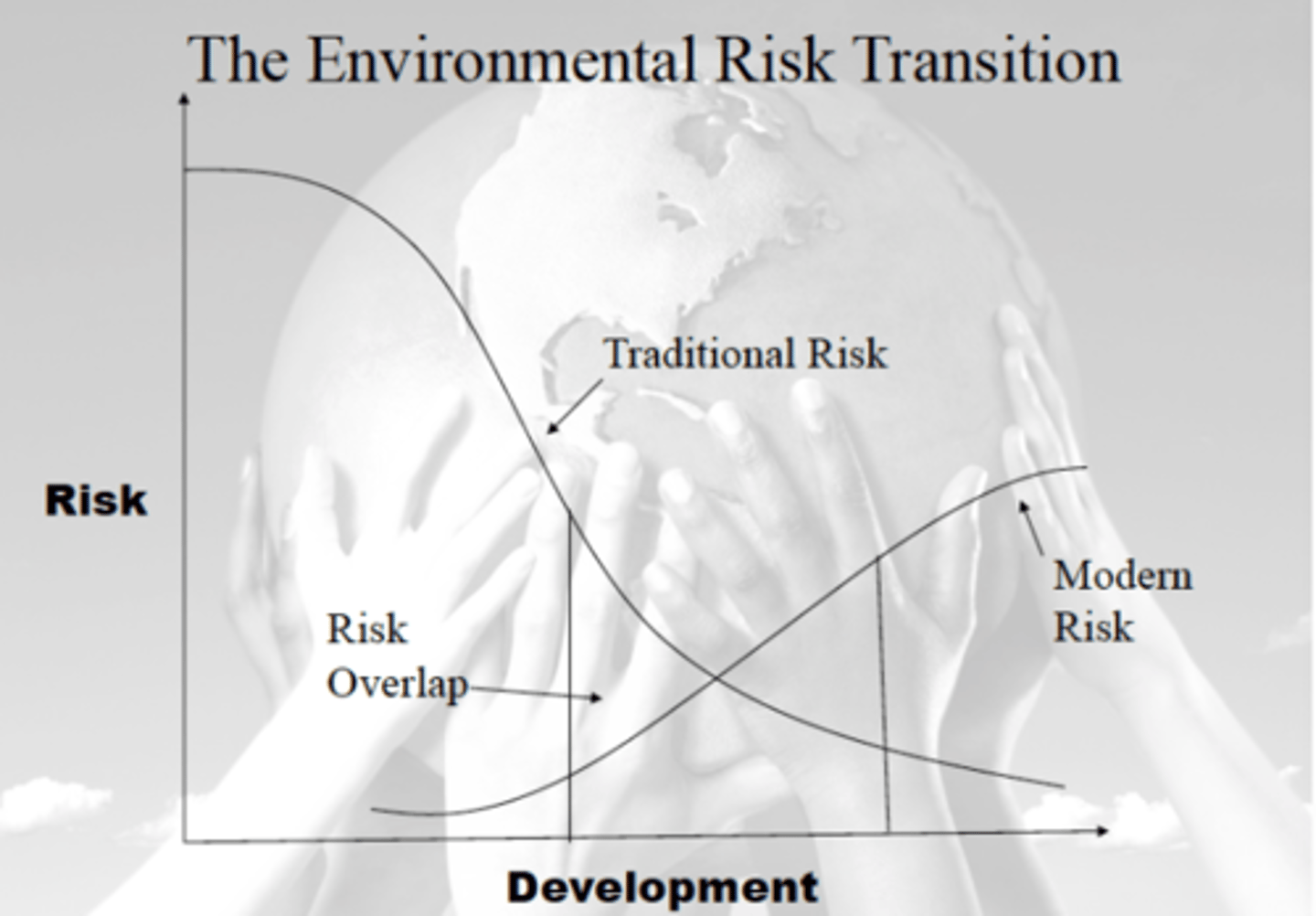
Describe environmental risk transition
Happens due to economic development in less developed regions. Go from local burdens to global burdens as development and wealth increases. Ex. poor sanitation in poor countries goes down as wealth increases but greenhouse emissions increase on a global level. Community risks like urban pollution increase then decrease.
What is the hierarchy of exposure controls?
Helps determine where to intervene- along the exposure pathway or individual level?
Upside triangle that goes top(most effective) to bottom (least effective)
1. Elimination: physically remove hazard
2. Substitution: replace the hazard
3. Engineering Controls: make modifications to control hazard
4. Administrative Control: change the way people work
5. PPE: personal protective equipment
Give an example of hierarchy of exposure controls?
Ex: traffic related air pollution
Looking at where to intervene
- Individual/Household level: Wearing masks, using air filters
-At the source: electric cars, driving less
- Along the exposure pathway: building homes and schools away from roads
Why do we study the past?
1. So we know how to intervene when new threats arise from past threats
2. Understand trends in burden
3. Learn why health inequities exist
Hippocrates
Said we want to learn about the health of a population we have to look at the AIR people breathe, the WATER people drink, and the PLACES people live
Paracelsus
"Dose makes the poison"
Said that all things are poison, but it's only the dose that makes things poison.
First environmental carcinogen?
Soot
What is soot?
Carbon produced during incomplete combustion. Tiny particles can be inhaled deep into the lungs.
Who discovered soot?
Percival Potts
What is the urban penalty?
When cities concentrate poor people and expose them to unhealthy environments
What is asbestos?
Fibrous mineral that are used for insulation because they're resistant to heat.
When they're breathed in, they get trapped in the lungs and remain there for a long time causing lung cancer.
What is the epidemiological triangle?
Has three parts:
Agent (capable of causing infection)
Host (Sufficient number of people susceptible)
Environment (allows agent to come in contact with host)
Who came up with the epidemiological triangle?
Wade Hampton Frost
Edwin Chadwick
Advocated sanitation:
Said that when circumstances are removed by proper cleaning so is the frequency of disease.
Comparison of field sparrows?
Looked at carbon deposition on two birds - before the clean air act and one where soot was a major environmental hazard.
The field sparrow with more carbon deposition during the soot area was darker than the one after the clean air act was established.
Typhoid Mortality and water
Typhoid fever is a life threatening infection caused by the bacteria salmonella. Spreads by contaminated food and water.
Causes of death in US in 1900 vs 1997?
1900-
1. Tuberculosis
2. Pneumonia
3. Diarrhea
1997-
1. Heart Disease
2. Cancer
3. Stroke
Who was the first anti smoking "crusader"(activist)?
Dr. Alton Ocshner
Recognized that smoking and lung cancer will become more frequent that any other cancer.
Dr. Richard Doll
Linked smoking to health problems: showed that cigarette smoking caused lung cancer
*Alongside Bradford Hill
What is the criteria of causation?
- Analogy
- Coherence
- Biological Gradient
- Plausibility
- Experiment
- Temporality
- Strength of association
- Consistency
- Specificity
What is the Love Canal Disaster? (1978)
Happened in Niagara Falls, where a company began dumping chemical waste into canals and this leaked into peoples home. Children were being born with deformities, mothers had cancer
Dr. Marie Curie
Discovered radium and polonium
Radium Girls
Female factory workers who got radium radiation poisoning from painting watches with tainted paint.
*Company said they had developed a rare disease, necrosis of the jaw. When a lady Katherine approached the company they told her, it was due to poor dental hygiene.
What is "fat man"
Atomic bomb dropped on Nagasaki in 1945
Minamata disease
mental impairments caused by mercury. First recognized in Japan
What are the stages of epidemiologic transition?
1. Pestilence and Famine
2. Receding Pandemics
3. Man Made diseases
What are upstream forces?
looking at factors that are causing the illness before it happens not after disease has happened.
What were the leading causes of death in 2019?
1. Ischemic Heart Disease
2. Stroke
2. Chronic Obstructive Pulmonary Disease
What are limitations of quantifying(measuring) health of populations?
1. Doesn't tell us when people are dying, as in their adulthood or when they're young.
2. Doesn't tell us causes of the causes. ie. upstream forces
3. There is more to health than avoiding death ie. death is not the only outcome
Why do most death and disease occur in low to moderate risk groups?
Think about the prevention paradox.
A large number of people at small risk
Describe how the GBD quantifies(measures) the impact of environmental hazards on public health
They use the approach, "population attributable fraction" and to do this they need four pieces of information.
1. Exposure: how many people are exposed and to how much
2. Exposure response relationship: how do health risks change as exposure changes
3. Counterfactual: what is the alternate scenario
4. Burden estimate for outcome: how many total deaths
To do so, they look at the change in risk reduced from current exposure to counterfactual(alternate) and by doing this it helps them measure the "population attributable fraction" and diseases attributable to current exposure.
Define DALY
Daly = YLL + YLD
= Years of life lost (dying prematurely) and Years lost due to disability
What does DALY stand for?
Disability Adjusted Life Years
What are the advantages of DALY's for quantifying impacts on public health?
It tells us how many people are dying prematurely and how long people are living with a disease. Allows us to compare countries globally. Tells us where to put money and resources.
What are some limitations of the GBD estimates?
- Doesn't consider climate changes
- many exposure outcomes are still not included
- still uncertainties in exposure assessments
- Disability weights (comparing back pain to the loss of a limb)
What are some obvious links between environment and human health?
Carbon monoxide poisoning
What does YLL stand for?
Years of life lost
ie. dying prematurely.
If the average life expectancy in a country for men is 75, but a man dies prematurely of cancer at 65 = 10 YYL
What does YLD stand for?
Years lived with disability
(how severe is the disability, living at less than ideal health)
What is a limitation of the DALY?
Only tells us life lost and lived with disability but not causes of the causes.
What does GBD stand for?
Global Burden of Disease
What does the GBD do?
Provide tools to measure health loss from different causes and risk factors in order to improve health systems
- Upstream (risk factors) and Downstream(causes)
What is the prevention paradox?
The prevention paradox says it doesn't matter what is more hazardous but instead it matters how many are exposed.
*Large number of people at a small risk
Example: 1 in 3 people don't have access to clean water, 2 billion people still lack basic sanitation
What are some upstream contributors to air pollution?
- Technology
- Climate change
- Policies
- Transportation
What is the precautionary principle?
Take precautionary measures even if there isn't an effect scientifically established.
*Assume chemical is dangerous until proven safe
burden of proof
If people are exposed to smt harmful, the burden of proof should prove that change is neccessary
What is the platt pickering debate?
Platt said: on a scale healthy people are on one side and sick people are on one side.
Pickering said: Health is a continuum.
Health is a _____
continuum
How do subtle shifts in risk have a substantial impact on health?
Taking kids with ADHD symptoms and looking at risk factors like lead means the average kid has 1 adhd symptom while the one at risk of lead has 3 symptoms. This subtle shift in the risk or graph puts over 500,000 more kids at risk.
*Essentially small shifts in risks have an effect on the community health.
Distinguish between clinical and population strategies
Clinical: Treatments and hospitals, 95% of health dollars go towards clinical strategies. This is downstream
Population: only 5% of health dollars go toward population strategies which are prevention strategies. Population strategies would help tackle risk factors that are making people sick in the first place
Triggers of Heart attacks?
- Air pollution vs Cocaine
Air pollution puts a large number of people at a small risk vs cocaine that puts a small number of people at a huge risk
Rose's 3 radical ideas?
1. Little shifts matter
2. A large number of people at a small risk cause more cases
3. There is no biological reason why every population should not be as healthy as the best
Dr. Ancel Keys
Mediterranean diet
Man that invented exercise
Dr. Jerry Morris
Lead and CVD
Lead enhances atherosclerosis by inactivating nitric oxide
List some of the reasons that environmental exposure assessments are conducted.
- Identify sources/ determinants of exposure
- Risk assessment/impact assessment
- Epidemiology
- Evaluation of exposure trends
List the routes of exposure for environmental hazards.
Dermal- skin
Inhalation- Respiratory Tract
Ingestion - GI Tract
Exposure control hierarchy
The exposure control hierarchy helps determine where to intervene to reduce exposure. The top is the most effective which is elimination- getting rid of the hazard and the bottom is the least effective which is PPE - personal protective equipment.
We can simplify this pyramid into three areas of where to intervene: At the source, along the exposure pathway, or at the household/individual level.
Describe some problems caused by exposure misclassification.
It is important because otherwise we would miss associations between health even when they are there. EX. we know that smoking causes lung cancer but if a poor job was done we would assume that smoking doesn't cause lung cancer.
-> essentially we would assume bias towards no problem between health and exposure.
If we underestimate exposure we underestimate impact
-> this would affect the relative risk or odds ratio
Discuss the role of exposure prevalence in determining population-level impacts of an environmental risk.
Describe the concepts of shifting the curve and the prevention paradox.
The prevention paradox says we should focus on the population strategy rather than the "high risk"clinical strategy because there is a large number of people at a small risk. In environmental health we need to reduce exposure of the entire population to environmental hazards.
Why are exposure assessments conducted? How is exposure information used?
- Used for epidemiology
- Determinants of exposure/identifying sources -> going upstream, looking at where pollutants are coming from and how are they making their way to people
- Exposure surveillance (see if exposure is going up or down), evaluating policies, or emerging issues
- To compare with guidelines-> work regulations like noise exposures
- Epidemiology
- Risk assessment/impact assessment
What are the three main routes of exposure?
Dermal
Ingestion
Inhalation
What is an exposure pathway?
The path the pollutant takes to go from source to subject.
Ex.
Pollutant emissions -> movement of pollutants -> exposure -> dose
What is an exposure biomarker?
Measure pollutants in a biological material.
Ex.Urine, blood, teeth, hair
Why are exposure controls at the source generally more preferable than controls at the level of the individual?
At the individual level it is harder because people don't like to change their behaviours and the best way to reduce exposure is to produce less of that hazard.
Why are randomized controlled relatively uncommon in environmental epidemiology?
1. Environmental hazards are widespread so it's hard to randomize exposure when everyone is exposed to it.
2. Hard to "blind" participants to a placebo
3. We don't want to increase exposure in the environment because that's unethical
Why is it important to assess exposure carefully? What "price" do we pay if exposure is assessed poorly?
It is important because otherwise we would miss associations between health even when they are there. EX. we know that smoking causes lung cancer but if a poor job was done we would assume that smoking doesn't cause lung cancer.
-> essentially we would assume bias towards no problem between health and exposure.
If we underestimate exposure we underestimate impact
Acute vs. Chronic
Acute: short term bursts of exposure
higher doses
may be followed immediately by symptoms
Chronic: long term exposures
lower doses
new onset of disease
What does exposure assessment look at?
Who was exposed
When were they exposed
How much
When
Where
What does the epidemiology method look at?
Health relationships in the "real world"
The effect of exposure on human populations
What are the 4 methods of environmental and occupational health
- Epidemiology
- Risk assessment
- Toxicology
- Exposure assessment
What are 3 places along the exposure pathway that we can intervene to reduce exposure?
At the source
Along the exposure pathway
At the household or individual level
What is an example of exposure information usage? (remember doesn't always have to be bad)
" Greenness and Birth outcomes"
Increased green space was associated with beneficial birth outcomes
What is temporal variation?
Variation is required: temporal variation is when concentrations vary in time (hourly) ex traffic
spatial variation
Concentrations vary place to place. ex. PM2.5 concentration higher in Asia.
Can also be place to place but just in Metro Vancouver
Direct vs Indirect exposure assessment methods
Direct: Personal measurements, biological markers
* Provides a more true estimate of exposures, expensive, and time consuming. Can be intrusive and puts a high demand on participants, small population
Indirect: Not done on a person, these are questionnaires, area measurements
* Provides a less accurate estimate of exposure, less time consuming and less expensive, bigger population
Indirect Methods of exposure assessment examples
"Area" measurements ex. looking at asthma related to traffic pollution
Questionnaires
What were the three major historical examples and how did they assess exposure?
1. Richard Doll and Hill Case control studied
- questionnaire based exposure assessment
-normally this doesn't work because people don't know how much air pollution they're exposed to but in this case the study was about smoking.
- People knew how much they smoked as it was "self administered" and it was in quantifiable units. ie. they knew how many cigarettes they had.
2. Asbestos exposure and neoplasia by Dr.Selikoff
- Factory workers that worked with asbestos came to Dr. Selikoff office and when he requested medical records the employer denied it.
-Eventually when he got their records he determined that however long these people worked with asbestos is how long they were exposed to it. The medical records gave data for onset of disease
3. Harvard Study - The New England Study
- put air pollution monitors in six of the cities and assumed the area measurement was reasonable
- findings were that higher pollution meant higher mortality rate.
____ is not the same as causation
Correlation
3 key ideas in epidemiology
1. Correlation is not the same as causation
ie. ashtrays don't cause lung cancer
2. Not everyone who is exposed to a hazard will develop disease from that exposure
ie. some ppl who don't smoke get cancer
3. Not every case is from that exposure
ie. non smokers get lung cancer
Explain correlation doesn't equal causation
Just because A and B are correlated does not mean A causes B or B causes A.
Hard to prove causality, but experimental designs provide stronger evidence. When we look at different studies we start to think maybe it isn't just correlation but also causation.
What are examples of observational design studies?
Observational is when we don't change anything. More common
- case control studies
- cohort studies
- Cross sectional
Examples of experimental design studies?
Experiment is when you change something. Less common.
- Randomized Control study
- Natural experiment
randomized controlled trial study aka _____ study design
The gold standard study design
What is an example of a randomized control study used in environmental health?
- UGAAR Study
Gave air purifiers to some women and no air purifiers to others. Hard to "blind" participants because women knew if they were getting air purifiers or not. The pregnant women with air purifiers had increase birth weights.
What are natural experiments
Type of experimental design study
The investigator does not change something but instead change happens on its own. Ie, a policy change
Ex. Beijing air pollution act. When this happened there was a decrease in air pollution and this was associated with higher birth weight.
What are cross sectional studies?
- snapshot of data collected at one time
- inexpensive and quick
- Not useful because it doesn't tell us if disease comes before exposure or if exposure caused disease
- doesn't provide evidence of causality
What are cohort studies?
More expensive
Follow people over time, take a similar group of people and see if they develop disease
Helps find rare exposures
What measurement do cohort studies use?
Relative risk
What measurements do case control studies use?
Odds ratio
What does it mean when the relative risk is greater, less than, or equal to one?
Greater than 1 relative risk means higher risk of developing disease
Less than 1 means, exposure is more protective, not that high of a risk
Equal to one risk means there is no risk
What are case-control studies?
Take people who have disease and then don't have it, then go back in time to see who was exposed and who wasn't
- small sample size is adequate
- can study rare disease
- retrospective -> looking back in time
Odds ratio (Case Control)
the ratio of odds that a case was exposed/odds that a control was exposed
Ubiquity of exposures
Basically everyone is exposed, so we need to focus on the prevention paradox and shifting the curve
Define threshold
A safe level of exposure where there is no harm to health.
Define NOAEL
No observed adverse effect level at the highest dose