medicine
1/187
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
188 Terms
approach to managing a COPD exacerabation resulting in resp failure
1. correct resp failure ( oxygenation/ventilation)
- oxygen, NIV
2. identify and treat underlying triggers
- antibiotics, allergies, PE, inhaled CSt
3. optimise recovery and prevent further exacerbations
- smoking cessation/nicotine replacement
- bronchodilators
- pulm rehab, Asthma/COPD aciton plan
- vaccine
mechanisms of hypoxia
- reduced Fio2 - high altitude
- obstruction / ventilation failure
- perfusion/ diffusion failure
- V/Q mismatch - causing shunting
- right to left heart shunt
approach to spirometry
check FEV1/FVC - target is 0.7
- below is obstructive
- above is normal or restrictive
check FEV1 against predicted ( severity of obstruction)
- post broncodilator improvement of 12% and 200ml = asthma
- non improvement = incomplete reversible obstruction = COPD
what to ask when px presents with dyspnea and wheeze
Dyspnea:
orthopnea,
exertional vs dysnpnea at rest,
paroxysmal noctural dyspnea
additional symptoms
wheeze ( small airways disease)
- inspiratory or expiratory
diagnosis of osteoperosis vs osteopenia
osteoperosis : DEXA scan , T score : ≤ -2.5
osteopenia : T score : -1 to -2.5
osteoclast activity > osteoblast activity
common osteoperotic fractures and complications
• Vertebral compression fractures (most common, often asymptomatic)
- Hip fractures
- Distal radius fractures
• Proximal humerus fractures
Clinical Consequences
• Morbidity: chronic pain, deformity (kyphosis), reduced mobility
• Mortality: hip fracture 1-year mortality ≈ 20- 30%
• Psychosocial: loss of independence, nursing home placement
prevention and management of osteoperotic fractures
Primary prevention
- Diet |exercise | falls prevention
Secondary prevention
- Calcium & Vitamin D
- Bisphosphonates ( bind to hydroxyappetite reducing OCs),
Denosumab (inhibits RANK ligand) ,
Teriparatide (severe - Parathyroid hormone)
• Orthopaedic input
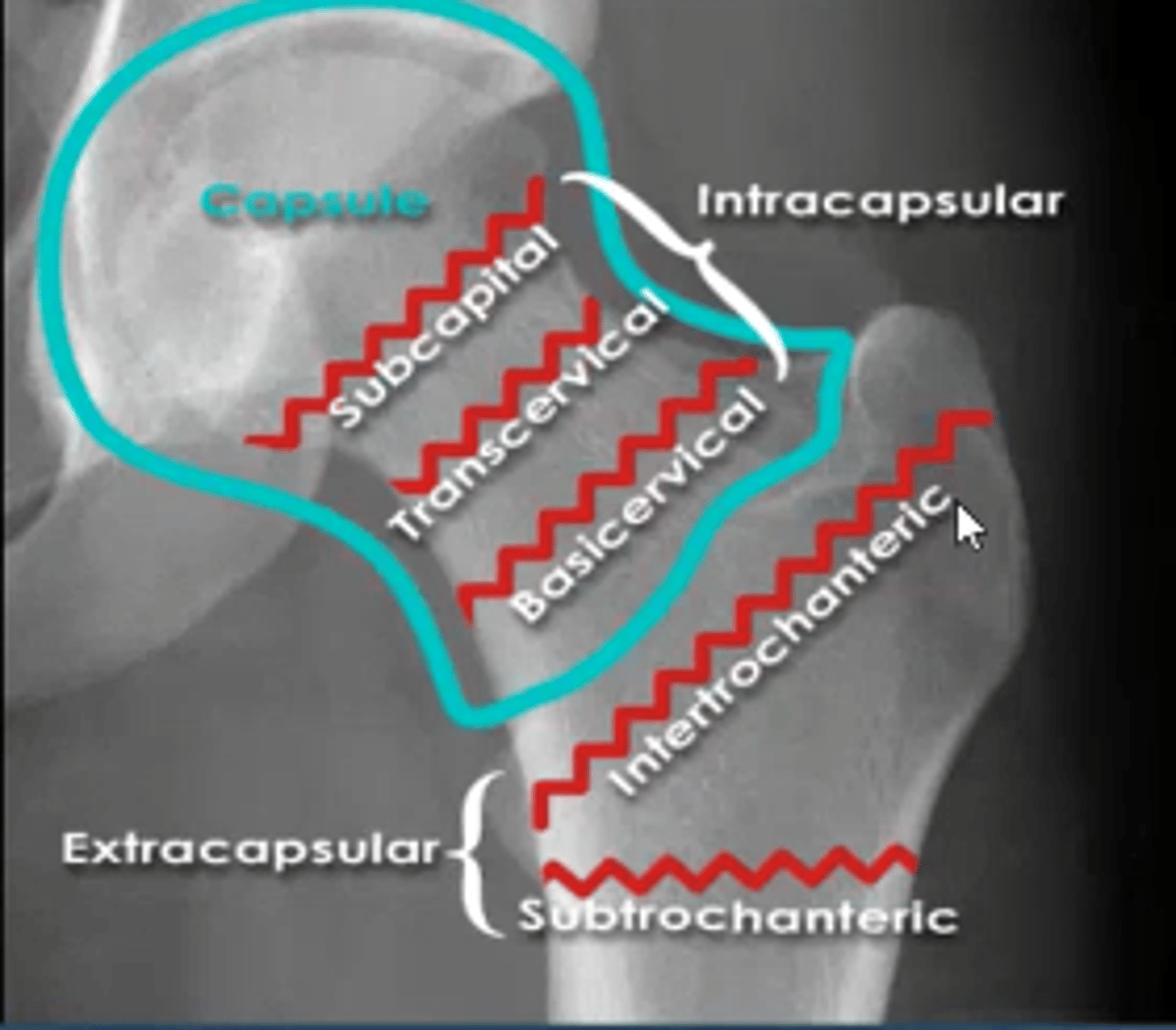
hip fracture classification
intracapsular:
head
neck ( subcaptial, midcervical, basic cervical)
*worse outcomes
extracapsular:
intertrochanteric
subtrochanteric
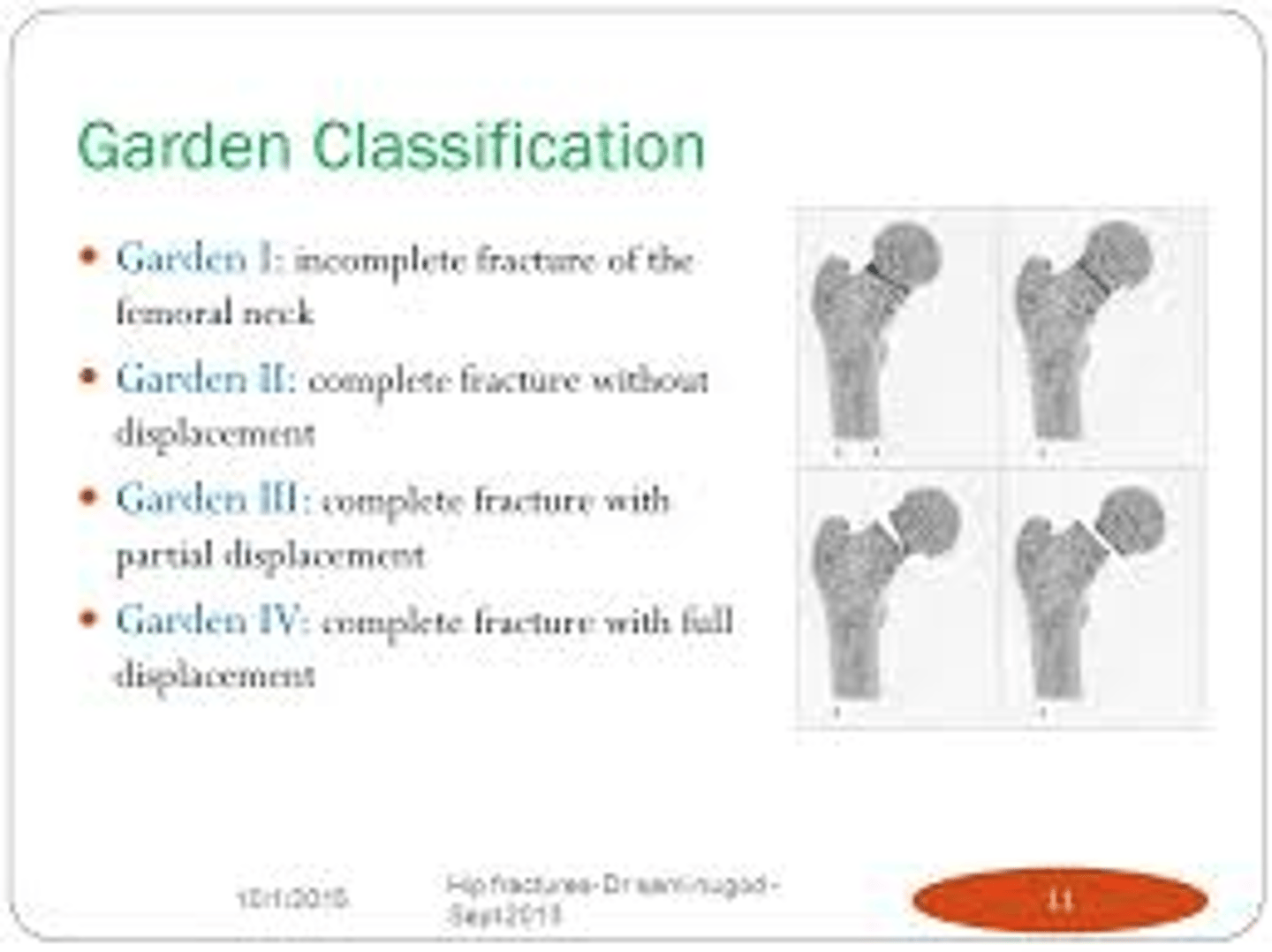
garden classification and treatment of intracapsular vs extracapsular fractures
Femoral neck fractures Intracapsular
Garden 1-2 ( undisplaced, stable)
- internal fixation ( dynamic hip screw/pin & plate)
Garden 3-4 ( displaced , unstable)
- internal fixation ( young), hemi arthoplasty or THR ( elderly)
extracapsular
- intertrochanteric (DHS or IM nail)
- subtrochanteric IM nail
system to desribe wrist fracture
Patient → Bone/location → Side → Pattern → Displacement/Angulation → Intra-articular? → Open/Closed → Named fracture → Associated injuries.
23 female - fracture of distal radial - right side - volar displacement with radial shortening ( distance compared to ulna) - closed fracture - consistent with smiths fracture- bruising on right elbow.
fracture healing
factors influencing?
direct vs indirect healing?
phases of healing
factors influencing:
Patient :
• age, smoking, nutrition,
Fracture:
• Adequate stability • Allow some motion, biomechanically stable
direct: anatomic fixation with compression - bone heals directly
indirect: callous formation
phases: haematoma, callous ( soft), bone remodelling
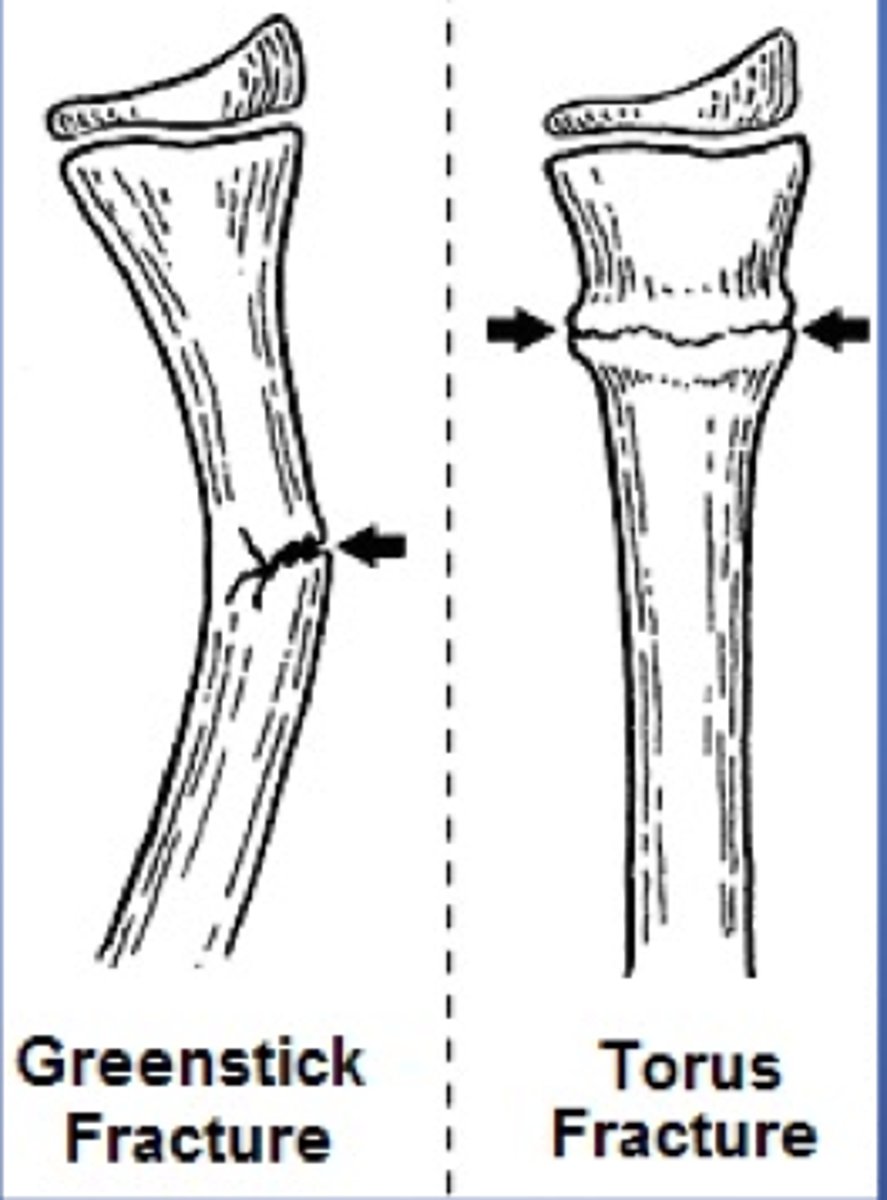
principles of paediatric fractures
aim
periosteum
types
classification
principles of paediatric fractures
aim : avoid growth disturbance
periosteum : thicker - rapid healing
types: torus, buckle
classification: salter harris
Definition of cirrhosis and 4 aetiologies
Cirrhosis
- final stage CLD characterised by regenerative nodules and fibrous septal in liver parenchyma due to chronic hepatic injury
Aetiology
- ethol abuse
- NAFLD
- autoimmune hepatitis
- Hep c
- Primary biliary cirrhosis
Rarer causes
_hameachromatosis
- Alpha -1 antitrysin deficiency
- Wilson disease
cirrhosis
Name 4 symptoms and complications
Symptoms
- ascites
- Hepatosplenomegaly
- Jaundice
- Spider nevi
- Palmar erythema
- Gynacomastia , hypogonadism ?? - increase in estrogen
- Pruritis
- Dupentren contracture
-
Complications
- hepatic ensephalopathy
- Hepatorenal syndrome - acute or non acute kidney injury ( need liver transplant)
- Varices, caput medusa, haemorroids
- HCC
What labs would you order and what would expect to see in cirrhosis
LFTs
- raised enzymes
- hyperbilirubineamia
INR
- prolonged PT time
Ultrasound
- atrophic heterogenous liver with nodular surface
- CT abdo if ultrasound inconclusive
CBC
- thrombocytopenia, leukopenia
CMP
- low albumin, hyponatremia
* liver chemistries may be normal in early cirrhosis
Prognosis and management of cirrhosis
MELD and Child - Pugh scores ( used to prioritise patients for liver transplant - determine 3 month mortality rate)
Score 6-40
Child's ABCDEs:
Albumin, bilirubin, coagulopathy (INR), distended abdomen ( ascites), encephalopathy
Management:
- treat underlying disease - avoid toxins, antivirals
- reconcile medications list - avoid NSAIDs , opioids, benzos
- immunise
- treat complications - oesophageal varices ( non selective beta blockers - reduce CO & vasoconstriction - propranolol)
- parecentesis
- liver transplant
contraindications of NIV
reduced consciousness
Recent facial trauma
Signifcant hypotension
Pneumothorax
clinical features of pneumonia
- dyspnea
- chest pain
- cough
- radiographic evidence of consolidation
antibiotics for CApneumonia
mild - monotherapy doxycycline
moderate ( in ED) - dual therapy - benzopenicillin and doxycycline
severe- ceftriaxone ( broader coverage including gram neg)
- cefalexin doesnt penetrate lungs
common. organisms in CAP
HAP
px with high dose prednisone/immunosuppressed
cap - strep pneumoniae, myocoplasma,
HAP - staph aureus
immunosuppressed/prednisone - pneumocystitis jerovicis
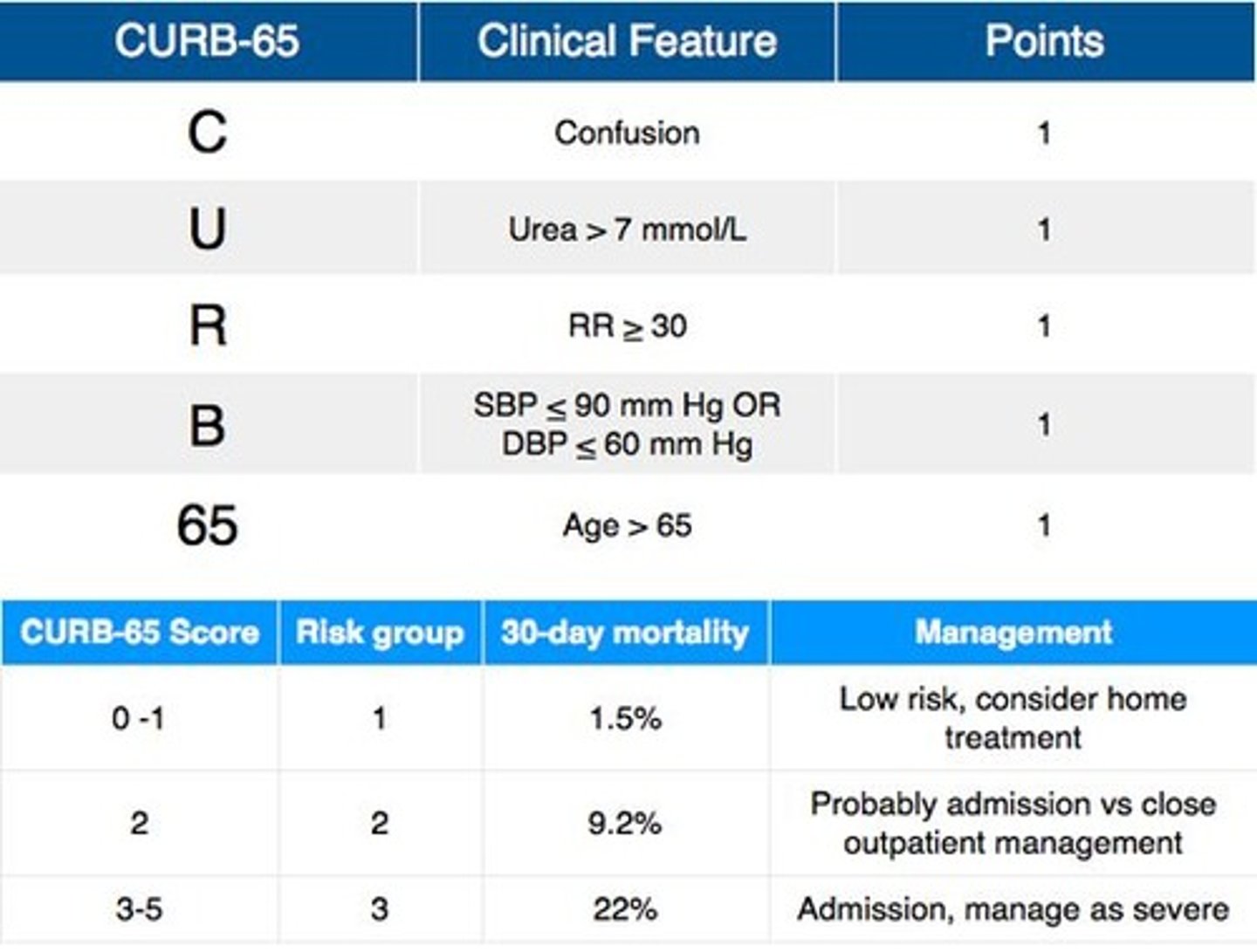
describe curb 65
tool used for pneumonia management
causes of hypercalcemia
1. primary hyperparathyroidism
2. maliganacy
3. prolonged bed rest ( reduced osteoblast activity from mechanical loading, osteoclasts unopposed)
4. medications
- thiazide diuretics ( reduce Ca2 excreation
- lithium ( shift PTH set point up)
- vit a toxicity ( increases OC act)
5. VIT D toxicity ( increases Ca uptake)
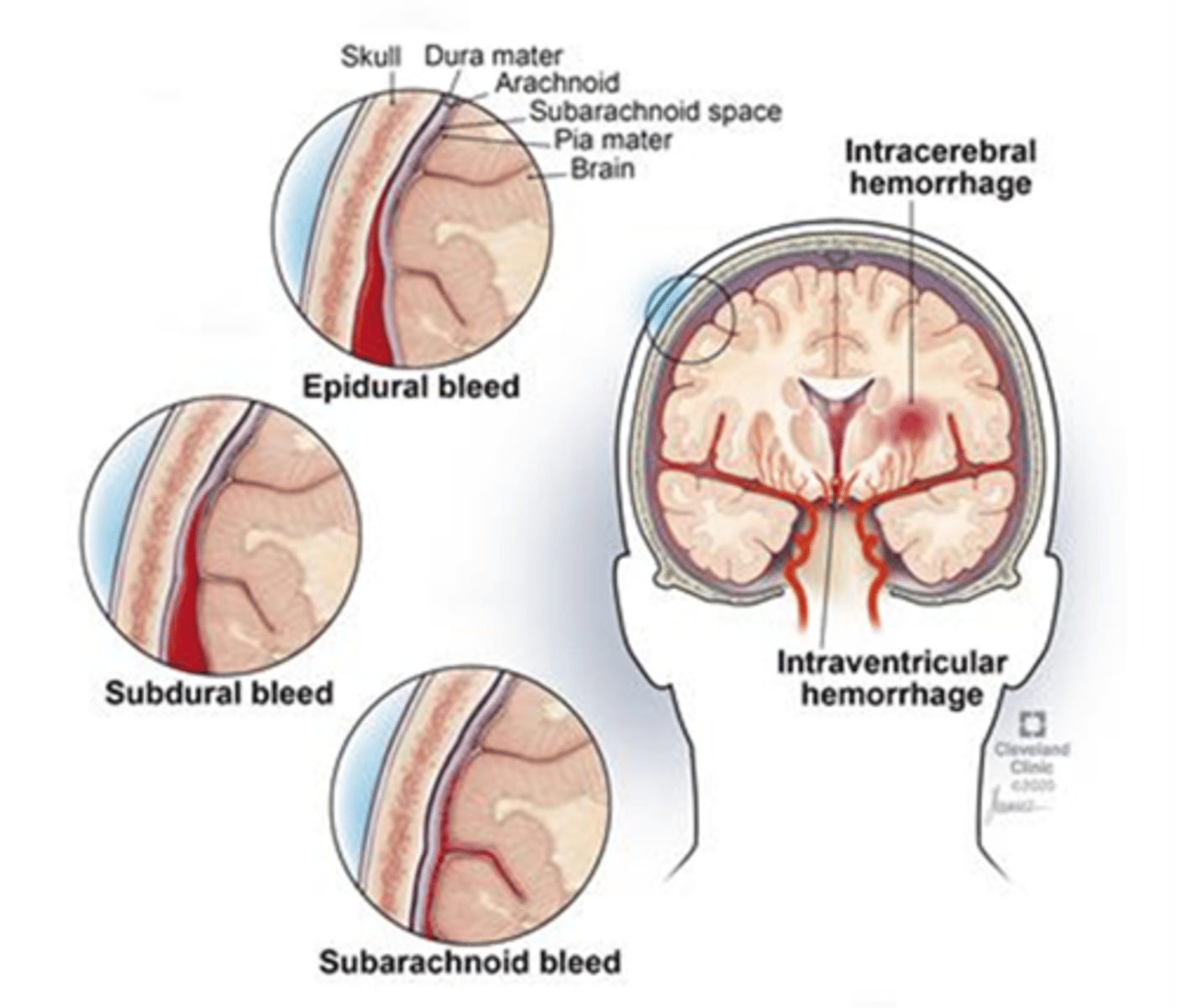
What are the key presentations of ischaemic stroke and haemorrhagic stroke (ICH + SAH)?
A:
Ischaemic:
-sudden focal deficit
- negative symptoms - loss of function
(hemiparesis, facial droop, aphasia, Visual loss - amorsis fugax, ataxia)
ICH:
- sudden onset of neurosymptoms
-vomiting, ↓ consciousness, severe hypertension.
- hyperdensity within brain parenchyma
SAH: thunderclap headache, neck stiffness, photophobia, collapse.
- circle of willis shadowing
* Epidural - lucid period
subdural - gradual decline
Q: What are major risk factors for ischaemic stroke and haemorrhagic stroke?
A:
Ischaemic: hypertension (strongest), AF, diabetes, hyperlipidaemia, smoking, age, prior TIA/stroke, carotid stenosis.
Haemorrhagic: hypertension, amyloid angiopathy, anticoagulation, berry aneurysms - SAH, AVMs, heavy alcohol use.
Q: What common conditions mimic stroke and how do they present?
A:
Seizure (Todd's paresis): transient unilateral weakness post-ictal usually resolving in 24 hours ( brain exhaustion)
Migraine aura: gradual spread of positive symptoms (visual zig-zags, tingling).
Hypoglycaemia: altered consciousness ± focal deficits.
Functional neurological disorder.
Q: What are the indications and limitations of CT, CTA, and CT perfusion?
A:
CT (non-contrast): first-line to rule out haemorrhage; limited sensitivity early in ischaemia.
CTA: identifies large vessel occlusion (ICA/M1) for EVT.
CTP: defines infarct core vs salvagable penumbra ( scans blood flow); extends reperfusion window to 24h.
Q: When is MRI (especially DWI) used in acute stroke and what are its limitations?
A:Use: highest sensitivity for acute ischaemia, posterior circulation events, uncertain diagnosis.
Limitations: slower, less available, contraindications (implants), not ideal for unstable patients.
What is the FAST stroke protocol?
1. FAST-positive = Code Stroke activation
Triggers:
- Immediate triage to resus bay
- Urgent neuro exam
- Non-contrast CT within 20 minutes ( rule out bleed)
- CT angiography if stroke suspected ( not sensitive for acute ischemic stroke)
- Notification of stroke team
2. determine eligbility for reperfusion
- assess for IV thrombylysis ( up to 4.5 hours)
- assess for endovascular thrombectomy ( up to 24 hrs with favourable imagine - CTP)
* better in large vessel occlusion
In FAST protocol , how do you assess a patient?
Facial droop
- ask patient to smile
Arms weakness or drift
- pronator drift test, ask patient to hold out arms
Assess speech coherence/slurring
what is the role of magnesium
50% in bone , 20% in muscle
antagonises calcium influx - cell metabolism
inhibits glutamate from binding to NMDA recepetors - reduced excitablity ( neuroprotective)
e.g status epilepticus - give mag sulphate Iv
hypomagnesium = <0.75 - give oral or iv mag
mechanism of calcium and symptoms of hyper /hypo calcemia
what is an ecg sign for severe hypocalcemia
stabilises sodium channels
needed for osteoblast activity
symptoms
hypercalcemia ( >2.6), severe > 3.5
stones(renal), bones(pain), groans/thrones(pancreatitis, consipation, psychiatric undertones (anxiety/altered
conciousness)
hypocalcemia
- reduced sodium channel stability - lowered threshold - muscle twitching, contraction - tetany
* tausaddes du point - prolonged QTC
most common esophageal cancer?
clinical symptoms/signs
adenocarcinoma- GORD
- PROGRESSIVE DYSPHAGIA ' i was fine drinking coffee 2 weeks ago but now i can't swallow food properly'... cancer invaded muscles causing dysmotility
haematological emergencies:
febrile neutropenia vs leukostasis
definition and action
febrile neutropenia
<0.5 neutrophils and fever may be the only sign of sepsis
action : cultures, antibiotics within 1 hour
leukostasis
blast count >100 WCC
( sludging in brain and lung capillaries)
- hypoxia, headache, confusion
action: emergent cytoreduction ( leukapheresis)
definition, signs of tumour lysis syndrome and treatment
definition:
rapid cell death releasing toxic contents
labs : high potassium, phosphate, uric acid, low calcium
management
aggressive hydration, allopurinol, raburicase
signs pointing to Acute Promyelocytic Leukemia ( APML) - medical emergency
blasts > 20% abnormal and presence of abnormal coagulopathy - DIC
treat immediately with ATRA ( all-trans retinoic acid)
- forces cell to mature and stop releasing granules - 95% cure rate
diagnostic genetic confirmation:
t(15:17)
investigations and diagnostics for leukemia:
FBC & smear
coag profile ( DIC)
metabolic panel ( tumour lysis syndrome)
viral serologies ( pre chemo screening)
bone marrow biopsy
MPO stain + = AML
MPO stain - = ALL
flow cytometry/ immunophenotyping
cytogenetics -classifcation to determine if favourable or adverse prognosis
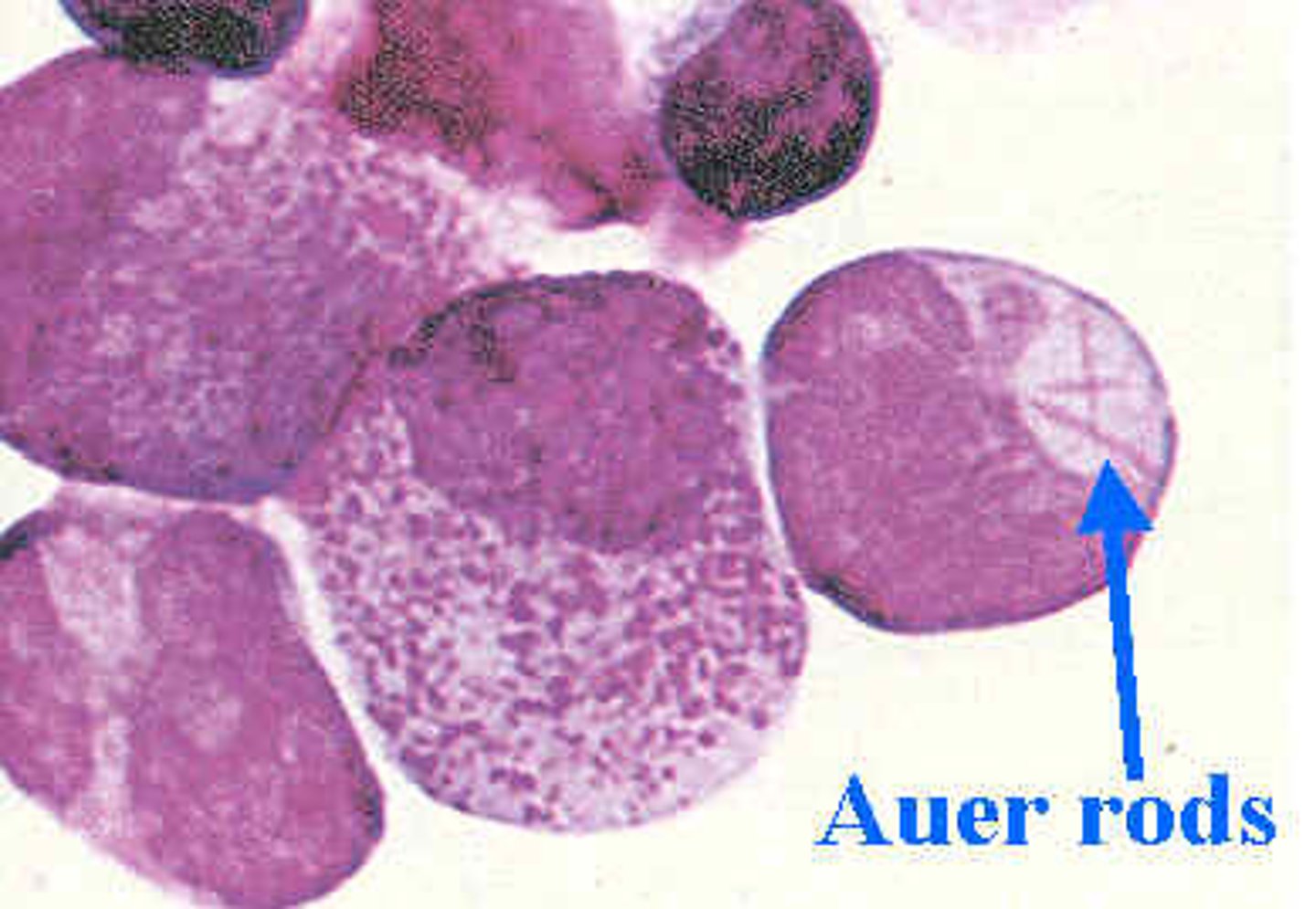
>20% blasts and presence of auer rods, gum hypertrophy is indicative of ?
AML
* median diagnostic age 67 years old
clinical presentation of leukemia
- anemia ( pale, fatige , SOB)
-thrombocytopenia
( bruising, petechia, gum bleeding)
- neutropenia ( fever, recurrent infections)
why do you need a lumbar puncture in AML
what makes is a confirmatory LP test for AML
treatment?
to see if leukemia has crossed the BBB and affected CNS
- CSF > 5 WCs with blasts confirmatory
manage with prophylactic intrathecal chemotherapy
( treatment is 2-3 years )
immediate vs delayed compensatory mechanisms of the heart
immediate - within mins
- TPR & CO
- Arteriole & venous constriction
- HR & contractility - PSNS - inhibitory centre + SNS accelatory centre via baroreceptors cartoid & aortic arch
delayed ( hours to days
RAAS, ADH release, Thirst stimulation
4 classifications of shock
Oxygen Delivery Can't Happen
Obstructive - pipes are blocked
Distributive ( septic, anaphylactic, neurogenic) * warm shock
Cardiogenic - pump no good
Hypovolemic - tank is empty
*cytotoxic shock- poison related, oxygen delivered but can't be utilised
aetiology of hypovolemic shock and explain the lethal diamond of severe blood loss
inadequate intake
haemorrage
fluid loss - burns
lethal diamond
hypothermia- impaired clotting and platelets
coaguloapathy - impaired oxygen tissue delivery
acidosis - further degrades clotting
hypocalcemia - acidodic intracellular shift
management and resus for haemorrage
1. ABCDE
2. 2x large bore IV access
3. FBC, G+H
4. monitering ecg + art line , TTE
5. MAP target 50-60mmHG ( unless TBI >80)
6. Early source control ( direct pressure, torniquet, code crimson)
7. correct coagoloapthy
8. temp control (WARMED FLUIDS)
9. damage control resus ( 1:1:1, minimal crystalloid , prioritise blood, TXA 1g, MTP activation, permissive hypotension)
targets for MTP
temp
fibrinogen
iCal
pH
lactate
Plt
PT/APTT
INR
temp >35
fibrinogen >2
iCal >1
pH > 7.2
lactate ><4
Plt >50
PT/APTT <1.5 normal
INR <1.5
symptoms and investigations for
- malaria
-dengue
- typhoid
- measels
malaria
-microscopy thick and thin films (gold standard)
rapid test for plasmodium falciparum
- variety of symptoms , splenomegaly
dengue - serology IGM , NS1 antigen test
- break bone fever ( arthralgia), biphasic rash ( handprint stays)
- typhoid - blood cultures
- fever , rose spots , salmon rash, constipation
* food contamination
Measles
Pcr , IGM ( + indicates recent infection/vaccination)
high fever , coryzal symptoms, rash
at rsk groups for syphilis
MSM
indigenous or those living in such communities
women of child bearing age
IV drug users
* notifiable disease, contact tracing
routes of transmission of syphilis( treponema palladium)
- contact with infected lesion
e.g condomless sex
- verticle transmission ( crosses placenta) - screen every trimester , can occurr as early as 8 weeks gestation. 90-100% transmission if untreated
- contact with infected blood
symptoms and complications of syphilis( treponema palladium)
chancre sores ( anything that looks like an ucler/sore - TEST)
- truncal red rash, patchy hairloss ( scalp eyebrows)
pathophys: widespread inflam/immune response
complications:
neurosyphilis - hearing, vision loss, menigitis, cog impaired
cardiovascular issues - aneurysm, valve damage
skin problems, infertility
staging, diagnostics and treatment of syphilis
staging
-early latent - <2 years since first transmission
-late latent - >2 years "
-tertiary syphilis - symptoms develop 7-30 years after transmission
DIAGNOSTICS
-PCR dry swab on lesion
-serology - TPPA antibodies
* can take 2-4 weeks to be detected in blood, swab first!
99% specificity
TREATMENT
penicillin
* monitor for JH jarisch-Herxheimer reaction ( transient fever, headache malaise, worsening rash)
transmission routes of HIV
unprotected vaginal or anal sex
* anal mucosa highest risk area
Percutanous contact
- needle sharing, transfusions
Mother to child
- intrauterine, perpartum, breastfeeding
*not by hugging kissing, urine, saliva
what cell does HIV target
screening test?
diagnostic ?
CD4
screening : Enzyme Immunoassay EIA
- test by 6 and 12 weeks since last high risk exposure
confirmatory: western blot
What regimine is given before and after HIV exposure
before - PREP ( 2 pil regimine daily or 1 injection every 2months)
after - PEP (within 72 hours of exposure) post exposure prophylaxis
signs of raised ICP
what is cushings triad?
.deteriorating level of consciousness
abnormal posturing ( decoricate or decerebrate)
abnormal pupillary response, uni/bilateral dilatation
abnormal breathing patterns
cushings triad - LATE SIGN
hypertension
bradycardia
irregular breathing
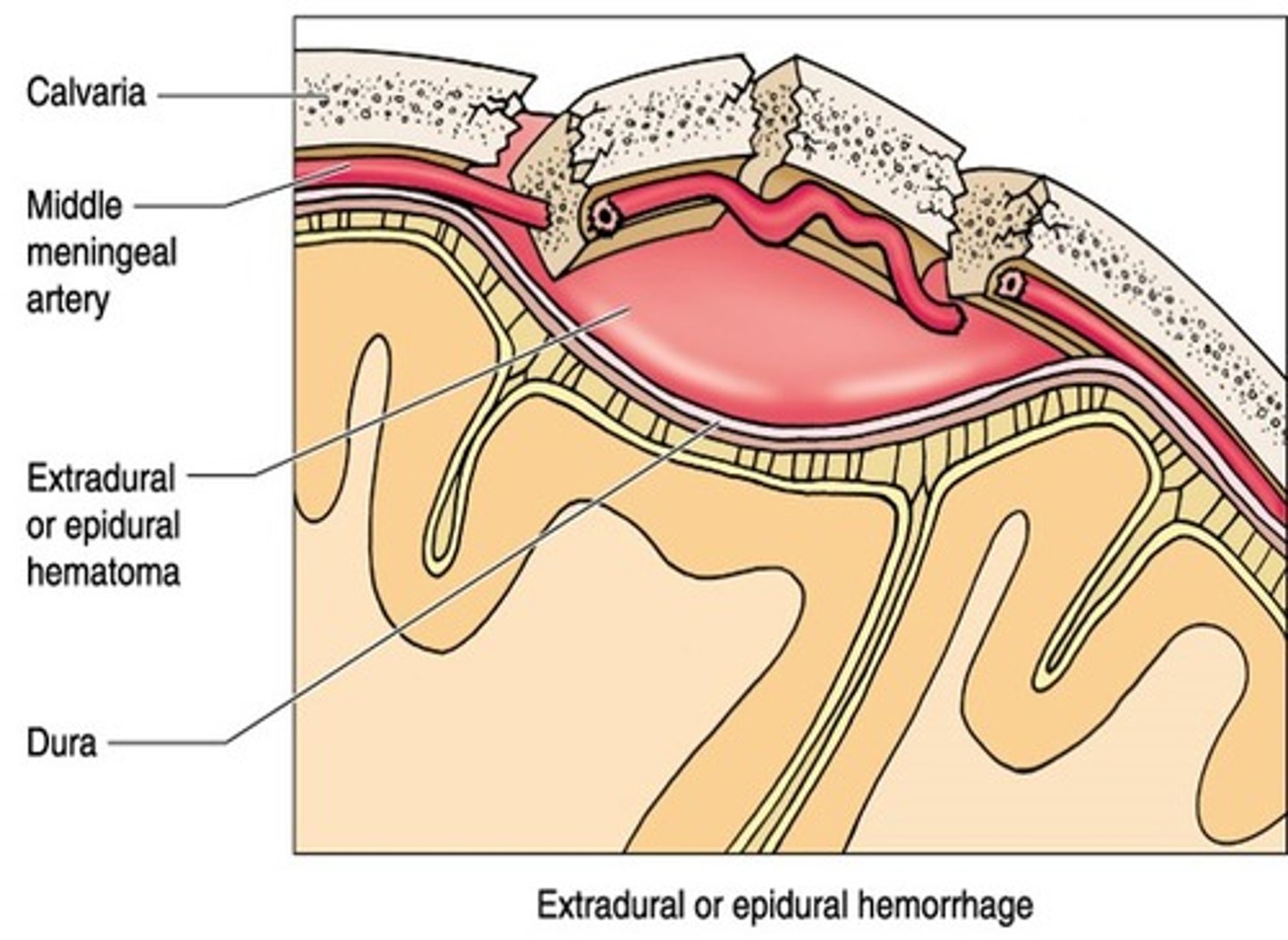
extradural hematoma
epidemiology?
bleeding from where?
epidural haemorrage
younger population - dura becomes more fused to skull as you get older
can be a torn venous sinus but mostly from middle meningeal artery
* bleeding cant cross a suture line
definition of cholecystitis vs choliangitis
investigations
cholecystitis: inflammation of the gall bladder
choliangitis: infection of the common bile duct
- jaundice must be present
investigations
US
CRP, WCC, LFTs, amylase, lipase ( >3x normal suggests pancreatitis)
pathophys of gallstones
cholstrol stones
- supersaturation ( high fat diet, pregnancy)
- biliary stasis ( high fat diet, rapid weight loss)
pigmented stones
- haemolysis
- cirrhosis
cholecystitis clinical presentation vs choliangitis ( name charcots + raynauds)
gall stones
RUQ, fever, nausea, vomiting, pain self limits <4 hours, biliary colic, murphys sign, bloating ,dyspepsia ( indigestion)
choliangitis
charcots triad
- Fever
-RUQ pain
- JAUNDICE
raynauds - late sign emergency
- charcots
- hypotension
- confusion
diagnosis on ultrasound of cholecystitis
presence of gall stones
thickened wall
pericholecystic fluid
management of cholecystitis
( which antibiotics)
Inital and definitive
initial:
- admit
- nil by mouth
- IV fluids
- pain releif
- IV antibiotics ( ceftriaxone and metronidazole)
definitve
cholecystectomy
management of choleangitis
initial:
- admit
- nil by mouth
- IV fluids
- pain releif
- IV antibiotics ( ceftriaxone and metronidazole)
Decompress/removal of obstruction
- ERCP or percutaneous drainage ( if not fit for surgery)
definitve
cholecystectomy
oncology referral if inidicated
pathophys of pancreatitis
signs of mild , moderate ,severe
obstruction of pancreatic duct causing congestion and ductal hypertension resulting in autodigestion and necrosis
mild - minimal symptoms
moderate - raised WBC and amylase
severe - shock, organ failure, raised CRP & lactate
treatment for pancreatitis
supportive care
- IV fluids
- pain control
- nil by mouth
enteral feeding
Address cause
- ERCP for stones
- stop alcohol
classifcation for HF
HFrEF - <40%
HFpEF >50%
NYHA
symptoms & signs of HF
symptoms
fatigue
exertional dyspnea/ reduced exercise tolerance
orthopnea
parosymal noctural dyspnea
ankle swelling
signs
elevated JVP, HJ reflux
displaced apex beat
fine bibasal crackles
3rd heart sound
heart murmur
pitting oedema ( ankle, sacrum)
investigations for HF
bedside
bloods : FBC, EUC, CMP, Pro BNP
ecg
imaging
CXR
Transthoracic Echo
management for HFrEf and HFpEf
- treat underlying cause
HFrEF
mortality reducing agents - 4 pillars
- ace/arni - Entresto
- beta blocker - Carvedilol
- Mineralcorticoid receptor antagonist MRA - finerenone, spironlactone
- SGLT2 inhibitors - empagliflozin
symptom reducing - loop diuretic
HFpef
- SGLT2 inhibitors - empagliflozin
- symptom relief - diuretics
Front: Addison’s disease – pathophysiology & signs/symptoms
Pathophysiology: Primary adrenal insufficiency → ↓ cortisol + ↓ aldosterone + ↑ ACTH (usually autoimmune destruction)
Mechanisms: ↓ aldosterone → ↓ Na⁺, ↑ K⁺ → hypotension ↑ ACTH → ↑ MSH → hyperpigmentation
Signs/Symptoms: Fatigue, weakness, weight loss Nausea, vomiting, abdominal pain Hyperpigmentation Hypotension, salt craving Hyponatraemia, hyperkalaemia, ± hypoglycaemia
Addison's disease - investigations & management
Investigations: ↓ morning cortisol Short Synacthen test → no rise in cortisol (confirms) ↑ ACTH (primary) Electrolytes: ↓ Na⁺, ↑ K⁺
Management:
Chronic: Hydrocortisone (glucocorticoid) Fludrocortisone (mineralocorticoid) Sick day rules + medical alert
Addisonian crisis: IV hydrocortisone + IV normal saline ± treat trigger ( surgery,infection, illness, non adherence meds)
infective endocarditis
signs/symp, investigations, RFs, complications
diagnosing criteria, management
Front: How does radiotherapy kill cancer cells & what is the oxygen effect?
Ionising radiation → free radicals → DNA double-strand breaks
Oxygen fixes DNA damage → prevents repair
Hypoxic tumours = radioresistant
Why is radiotherapy given in fractions & what are the 4 Rs?
Fractionation allows normal tissue recovery while damaging tumour
4 Rs:
Repair (normal cells recover)
Reoxygenation (tumour becomes more sensitive)
Redistribution (cell cycle)
Repopulation
What are key side effects and oncologic emergencies of radiotherapy?
Acute: skin erythema, mucositis, fatigue
Late: fibrosis, infertility, secondary malignancy (irreversible)
Emergencies:
Spinal cord compression → steroids + urgent RT
SVC obstruction → RT ± chemo
Front: What are the major Duke criteria for diagnosing infective endocarditis?
Positive blood cultures with typical organisms
(e.g. Staph aureus, viridans strep, enterococcus, HACEK)
Evidence of endocardial involvement:
- Vegetation/abscess on echo (TOE > TTE)
- New valvular regurgitation
📌 Memory: “Blood + Echo”
Front: What are the major & minor Duke criteria and how is infective endocarditis diagnosed?
major:
postive blood cultures + changes on echo
Minor criteria:
- Predisposition
(IVDU, valve disease)
- Fever ≥38°C
- Vascular phenomena (emboli, Janeway lesions)
- Immunological phenomena (Osler nodes, Roth spots, GN)
Diagnosis:
Definite:
- 2 major
- OR 1 major + 3 minor
- OR 5 minor
Possible:
1 major + 1 minor
OR 3 minor
What is the initial and medical management of infective endocarditis?
empirical therapy for native and prosthetic valve
if suspected MRSA ( iv drug user), what change in antibiotic?
Back:
Take ≥3 blood cultures before antibiotics
-Start empiric IV antibiotics (then tailor to cultures)
Prolonged therapy: 4–6 weeks IV
TG empiric cover:
Native valve:
Benzylpenicillin 1.8g 4hrly + flucoxacillin 2g 4hrly + gentamycin
prosthetic valve
flucoxacillin 2g 4 hrly + vancomycin + gentamycin
MRSA: replace benzyl with vancomycin
Monitor:
Blood cultures (clearance)
Renal function (drug toxicity)
📌 Key principle: “Culture first, then treat long and IV”
antibiotic therapy for MSSA in IE
- include standard, non severe + severe reaction
standard = flucox 2 g 4 hrly
non severe = cefazolin 2g 8hourly
severe = vanc -
triad of cardiac tamponade
common blood pressure sign?
Beck's triad
hypotension, raised JVP, muffled heart sounds
- widened pulse pressure
pericarditis features associated with poor prognosis
- high fever >38 degrees
-subacute course—symptoms developing over several days
-without a clear acute onset
-large pericardial effusion
-cardiac tamponade
-failure to respond within 7 days to drug therapy.
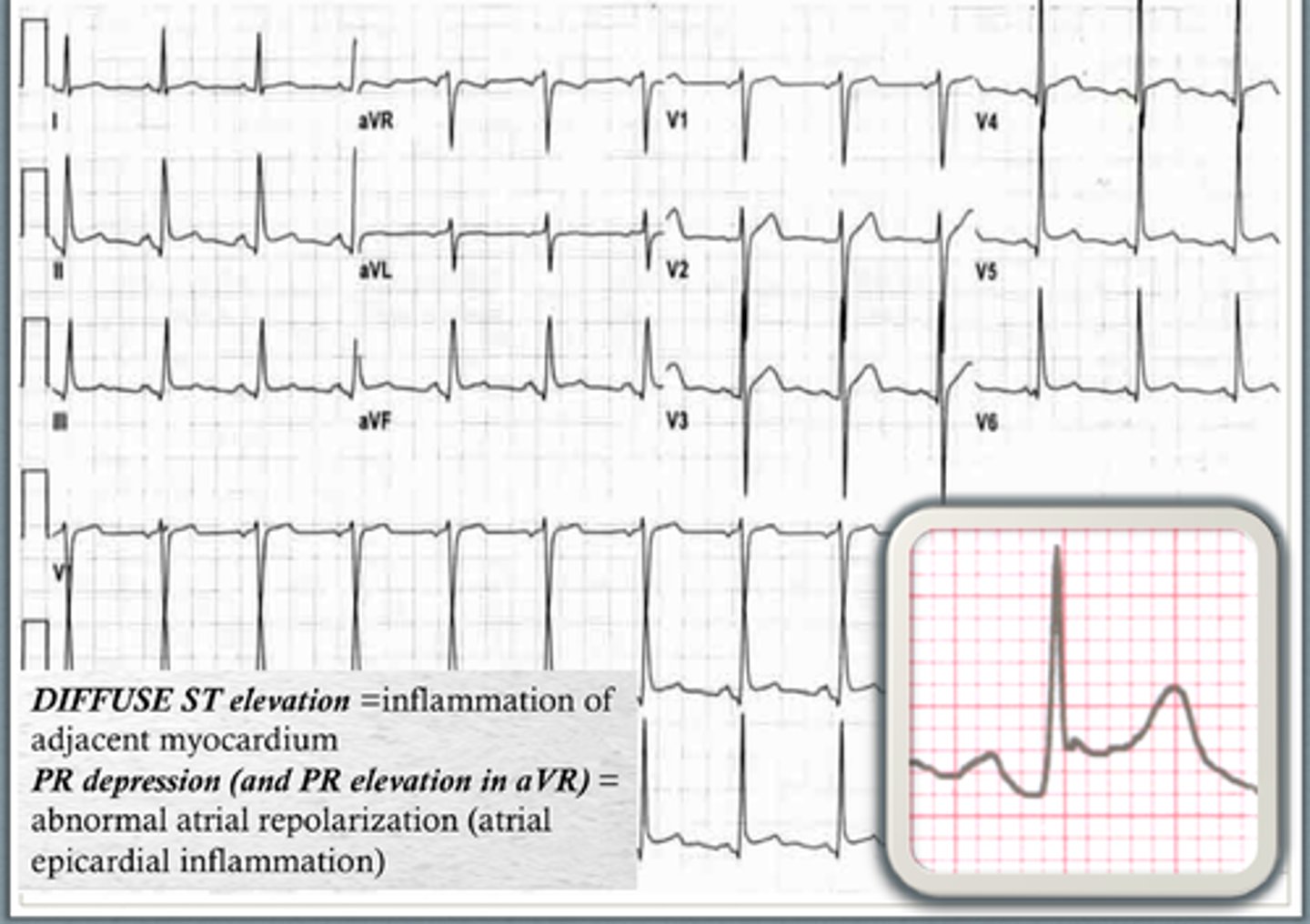
What are the epidemiology, risk factors, and key investigations/diagnostic features of acute pericarditis?
📊 Epidemiology
Most common cause of acute pericarditis: viral
⚠️ Risk factors / causes
-Viral infections (Coxsackie most common)
- non infectious - autoimmune, malignancy ,metabolic, traumatic, iatrogenic ( covid vaccine)
🔬 Investigations
ECG: diffuse ST elevation + PR depression
Troponin: may be mildly elevated (myopericarditis)
CRP/ESR: elevated inflammatory markers
TTE: assess effusion/tamponade
CXR: may show enlarged cardiac silhouette if effusion
🧠 Diagnosis (clinical)
need 2 of following:
- Pleuritic Chest pain -pericardial rub
-ECG changes
- effusion
What is the management and complications of acute pericarditis?
💊 Management
First-line:
Colchicine (reduces recurrence)
NSAIDs (ibuprofen high dose)
If severe/refractory:
Corticosteroids (careful: ↑ recurrence risk)
Treat underlying cause (e.g. TB, uraemia)
Restrict strenuous exercise until resolution
🚨 Complications
Pericardial effusion
Cardiac tamponade (emergency)
Recurrent pericarditis
Constrictive pericarditis (chronic fibrosis)
risk factors and complciations of IE
RFs:
prosthetic valves
congenital heart defects, intravenous drug use,
iatrogenic
poor dental hygiene
immunosuppressed
complications
heart failure
stroke
septic emboli- kidney, spleen limb
immune mediated GN
Haematuria
Front: Causes and key features of haematuria?
Glomerular:
Glomerulonephritis
Dysmorphic RBCs, RBC casts
Non-glomerular:
Stones
Infection
Malignancy
📌 Exam clues:
Painful → stones/infection
Painless → malignancy until proven otherwise
Reduced GFR
: Causes and consequences of reduced GFR?
Causes:
AKI (pre/intra/post renal)
CKD
Hypoperfusion
Consequences:
Uraemia
Hyperkalaemia
Fluid overload
Metabolic acidosis
Flashcard 7: Dialysis Indications (in renal replacement therapy)
Front: What are the indications for dialysis?
AEIOU:
Acidosis (refractory)
Electrolytes (↑K⁺, Ca2) refractory
Intoxication of poisons ( lithium)
Overload (fluid) refractory to medical management
Uraemia (encephalopathy, pericarditis)
haemodyalysis, peritoneal, kidney transplant
Complications of CKD
Front: What are the major complications of chronic kidney disease (CKD)?
❤️ Cardiovascular (most common cause of death)
Hypertension
Accelerated atherosclerosis
Heart failure
🩸 Haematological
Anaemia → ↓ erythropoietin ( give EPO stim + iron)
⚡ Electrolyte / metabolic
Hyperkalaemia
Metabolic acidosis
Fluid overload
🦴 Bone & mineral (CKD-MBD)
↓ vitamin D activation
↑ phosphate → ↑ PTH (secondary hyperparathyroidism)
Renal osteodystrophy, fractures
🧠 Uraemia
Encephalopathy
Pericarditis
📌 Memory: “Blood, Bones, Electrolytes, Heart, Uraemia”
risk factors, signs ( nemonic) and mangement of serotonin syndrome
risk factors:
- use of serotonergic drugs or combo use of cyp450 inhibitors e.g MAOs, SSRIs, ondanz, MDMA, tramadol, merepiridine
signs
SHIVERS
shivering
hyperreflexia + myoclonus
increased temp < 41
vitals unstable ( ↑HR, ↑ RR, labile BP)
Encephalopathy - altered/LOC
Restless
Sweating
management
cease causative drugs
supportive care e.g oxygen , IV fluids, agitation ( benzos), active cooling ( fan + mist, ice bath, ice packs, cold IV fluids)
What are the 4 H’s in cardiac arrest and how are they managed?
🟠 Hypoxia
Oxygen, airway support, ventilation/intubation
🟡 Hypovolaemia
IV fluids ± blood products
Control bleeding
🔵 Hypo-/Hyperkalaemia (± metabolic)
Hyperkalaemia: IV calcium, insulin + glucose, dialysis( refractory)
Hypokalaemia: IV potassium
Acidosis: treat cause ± sodium bicarbonate
🟣 Hypothermia
Active rewarming
Warm IV fluids
📌 Key idea: Fix oxygen, volume, electrolytes, temperature
What are the 4 T’s in cardiac arrest and how are they managed?
⚡ Tension pneumothorax
Immediate needle decompression → chest drain
❤️ Cardiac tamponade
Urgent pericardiocentesis
🫁 Thrombosis
Pulmonary embolism → thrombolysis
Coronary (MI) → PCI/thrombolysis
☠️ Toxins
Antidotes (e.g. naloxone, sodium bicarbonate(TCAs))
Supportive care
📌 Key idea: Relieve pressure, remove fluid, treat clots, reverse toxins
Discontinuation Syndrome
Front: What is discontinuation syndrome and how is it recognised and managed?
🧠 Definition
Symptoms after abrupt cessation or rapid dose reduction of antidepressants
Common with short half-life drugs (e.g. paroxetine, venlafaxine)
⚡ Symptoms (FINISH)
Flu-like symptoms
Insomnia
Nausea
Imbalance (dizziness)
Sensory disturbances (“brain zaps”)
Hyperarousal (anxiety, irritability)
⏱️ Timing
Onset: 1–3 days after stopping
Duration: ~1–2 weeks
💊 Management
Prevention: gradual taper
If occurs:
Restart drug → taper slowly
Consider switching to fluoxetine ( long acting SSRI)
Discontinuation Syndrome vs Relapse
Front: How do you differentiate discontinuation syndrome from depression relapse after stopping antidepressants?
⏱️ Timing
Discontinuation: rapid onset (1–3 days)
Relapse: gradual (weeks)
⚡ Symptoms
Discontinuation: physical + neurological
Dizziness, nausea, “brain zaps”, flu-like
Relapse: psychological
Low mood, anhedonia, hopelessness
💊 Response to restarting meds
Discontinuation: improves quickly (days)
Relapse: improves slowly (weeks)
Fast + physical = discontinuation
Slow + psychological = relapse
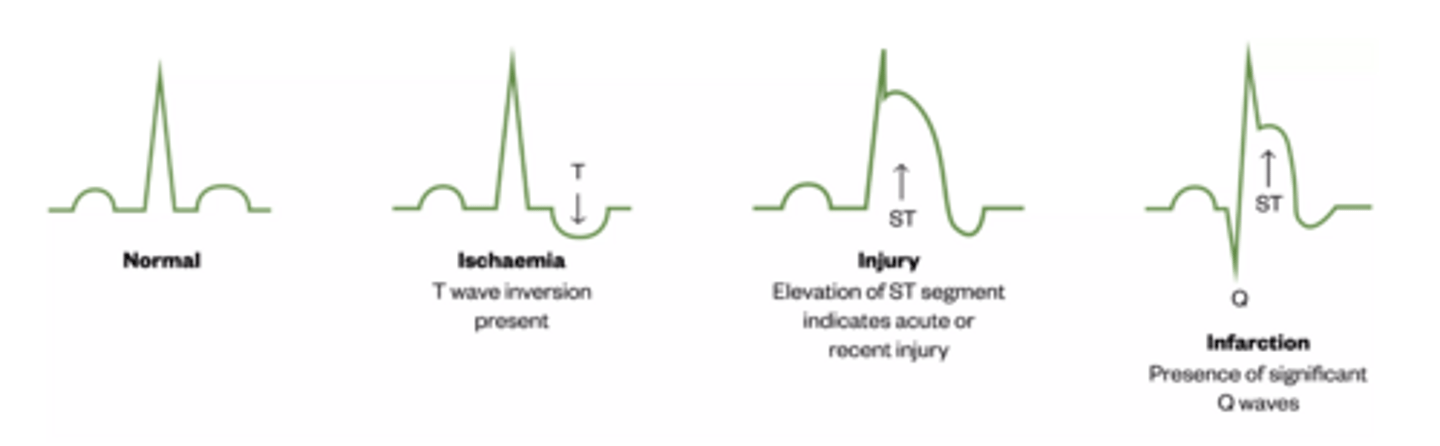
Pathophys + Symptoms and ecg changes for angina/ CAD
CAD Pathophysiology
Endothelial injury → LDL oxidation → foam cells → plaque
Plaque → stenosis → ↓ coronary flow
Demand > supply → ischaemia → angina
Plaque rupture → thrombosis → MI
Angina Features
Central, crushing pain
Radiates to arm/jaw
Exertional ( can measure metres they can walk until)
Relieved by rest/GTN
Ischaemia ECG
ST depression, T inversion ( v2-25)
MI ECG
ST elevation, Q waves
DDx + Ix + Management of angina
DDX
Life-threatening chest pain
ACS, PE, aortic dissection, tamponade, pneumothorax
Mimics
GORD, oesophageal spasm, costochondritis, anxiety
Key Investigations
ECG (first)
Troponin (serial)
CXR ± CTangio/aorta ( rule out PE)
Stable Angina Management
Lifestyle changes- SNAP
GTN (symptom relief)
Beta blockers (↓ demand)
Aspirin + statin
PCI/CABG if severe
ecg signs for pericarditis?
criteria for STEMI
Diffuse ST elevation + PR depression.
ST elevation in ≥2 continguous leads
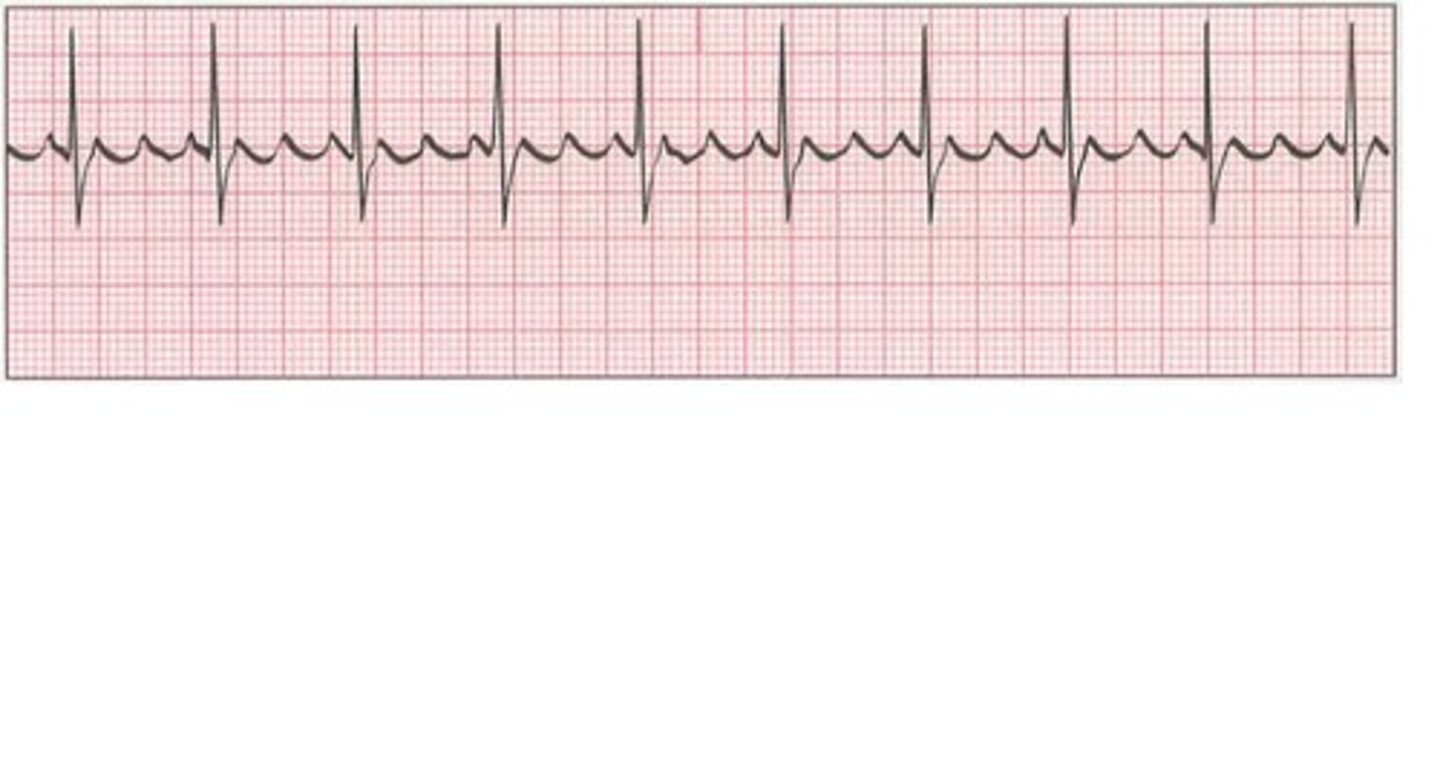
sawtooth pattern on ecg is suggestive of which cardiac condition?
management?
atrial flutter
* often misdiagnosed as SVT
ventricular rate ≥150 bpm + narrow QRS
management
unstable = cardiovert
stable - same as AF, rate vs rhythm control
QRS width = differentials for narrow vs wide
management of SVT
Narrow (<120 ms)
Supraventricular
AF (irregularly irregular)
Flutter (sawtooth)
SVT (regular, fast)
Wide (>120 ms)
Ventricular tachycardia (assume first)
- monomophic VT , polymorphic tausades
SVT with aberrancy/ BBB ( narrow but appears wide)
WPW - delta wave
SVT managemment
- vagal maneurvers ( carotid sinus massage, valsalva)
- adenosine 6mg IV bolus followed by saline flush, give 12mg if ineffective after 2 mins ( continue titration)
ecg recognition of types of blcok Heart block
QUICK ECG RECOGNITION
Long PR only → 1st degree
PR progressivly longer then drop → Mobitz I - atropine if symptomatic
Sudden drop, PR constant → Mobitz II 🚨pacemaker
P & QRS unrelated → Complete heart block 🚨- urgent pacing , syncope
PATHOPHYS + DDx of restrictive lung disease
aetiologies of interstitial lung disease
how does spironmetry look in restrictive disease
Restrictive lung disease
↓ compliance → ↓ lung volumes → dyspnoea
Intra-thoracic
ILD, fibrosis, sarcoidosis
Crackles present
↓ DLCO ( diffusion of gas across membrane)
Extra-thoracic
Obesity, neuromuscular MG/MND, chest wall, kyphoscoliosis
- Normal DLCO
aetiologies
idiopathic
environmental - asbestos, silica, smoking
autoimmune - RA, scleroderma
drugs - methotrexate, amioderone ( pulm toxic)
spirometry
volumes reduced but normal ratios
management of interstitial lung disease vs restrictive
Goals:
Slow fibrosis
Reduce inflammation
Improve oxygenation
General
Smoking cessation
vaccinations
Pulmonary rehab - physio
Oxygen
Drugs
Anti-fibrotic (pirfenidone, nintedanib) → IdiopathicPF
Steroids/immunosuppressants → inflammatory ILD
Advanced
Lung transplant
restrictive
- improve mechanics
obesity - weight loss, CPAP
neuromuscular - treat underylying cause (immunosuppress in MG), BiPAP
scoliosis- physiotherapy
Causes of AKI and general management
Causes
60% Pre-renal → ↓ perfusion
- hypovolemia ( haemorrage, dehydration)
- hypotension ( shock, sepsis)
- decreased circulating volume ( heart,liver failure, nephrotic syndrome(>3.5g protein/day)
- renal artery stenosis
- drugs ( Ace, Arbs, NSAIDs)
35% Intrinsic → internal damage
ATN (85% cause of intrinsic AKI) - muddy casts
- ischemia ( prolonged hypotension
- nephrotoxic drugs (contrast, amingoglycosides, methotrexate)
- endogenous toxins ( myoglobin- rhabdo, haemoglobin in haemolysis, bence jones proteins - multiple myeloma)
AIN
- medication( antibiotics, PPIs, Phenytoin, interferon)
- infection
- infiltrative disease ( amyloid/sarcoidosis)
Vascular disease ( scleroderma, hypertensive emergency)
GN - RBC casts
5% Post-renal → obstruction
acquired- stones, BPH, clots, tumor, iatrogenic
neurogenic - MS, spinal cord lesion, peripheral neuropathy
congenital malformation ( posterior urethral valves )
Management
Treat cause
Stop nephrotoxic drugs (NSAIDs, ACEi)
Fluid balance
Monitor electrolytes
investigations you would order in AKI?
urinalysis in AKI
what would you see in pre renal, ATB, GN & interstitial nephritis
bloods :
-FBC, UEC, albumin:creatinine ratio (ACR), egfr
-ultrasound to rule out post renal
-biopsy in suspected GN, nephrotic syndrome(>3.5g protein/day), unexplained AKI
🚽 Urinalysis
Bland urine
No cells/casts
ATN
Muddy brown casts
GN
RBC casts + haematuria
Interstitial nephritis
WBCs ± eosinophils