kale GERD
1/80
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
what are the aggressive and defensive factors for GER
aggressive (makes it worse):
1. gastric acid, pepsin
2. bile salts, pancreatic enzymes
3. prostaglandins (lower LES pressure)
defense:
1. LES pressure increase
2. esophageal clearance
3. mucosa
4. increased gastric emptying
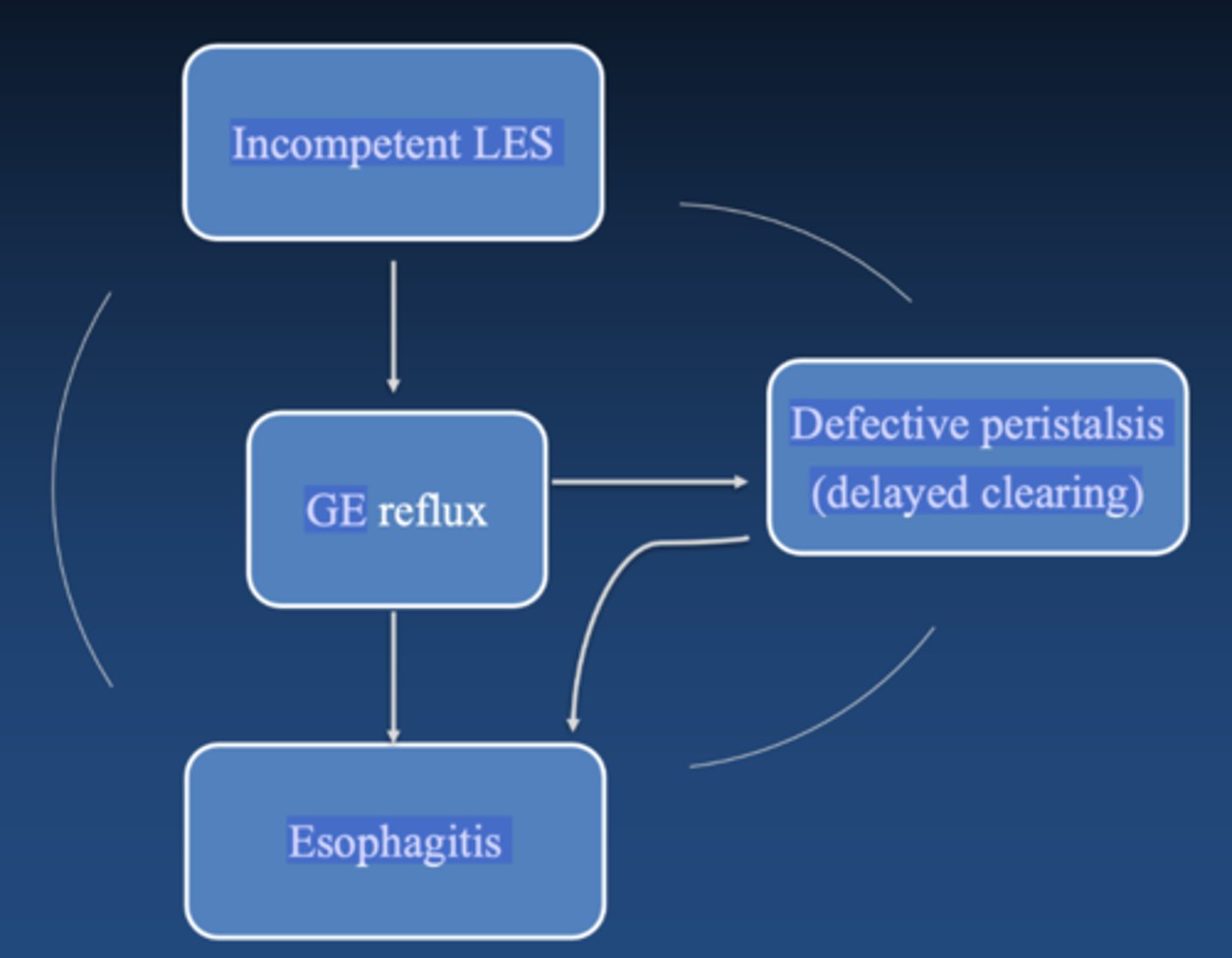
explain cyclic nature of GER
incompetent LES causes reflux and delayed clearing which causes esophagitis which makes LES more incompetent
RISK FACTORS FOR GERD
intra abdominal pressure= pregnancy, obesity, ascites
lower tone= surgery, hiatal hernia, chalasia, nasogastric intubation
other: scleroderma, cigarette smoking
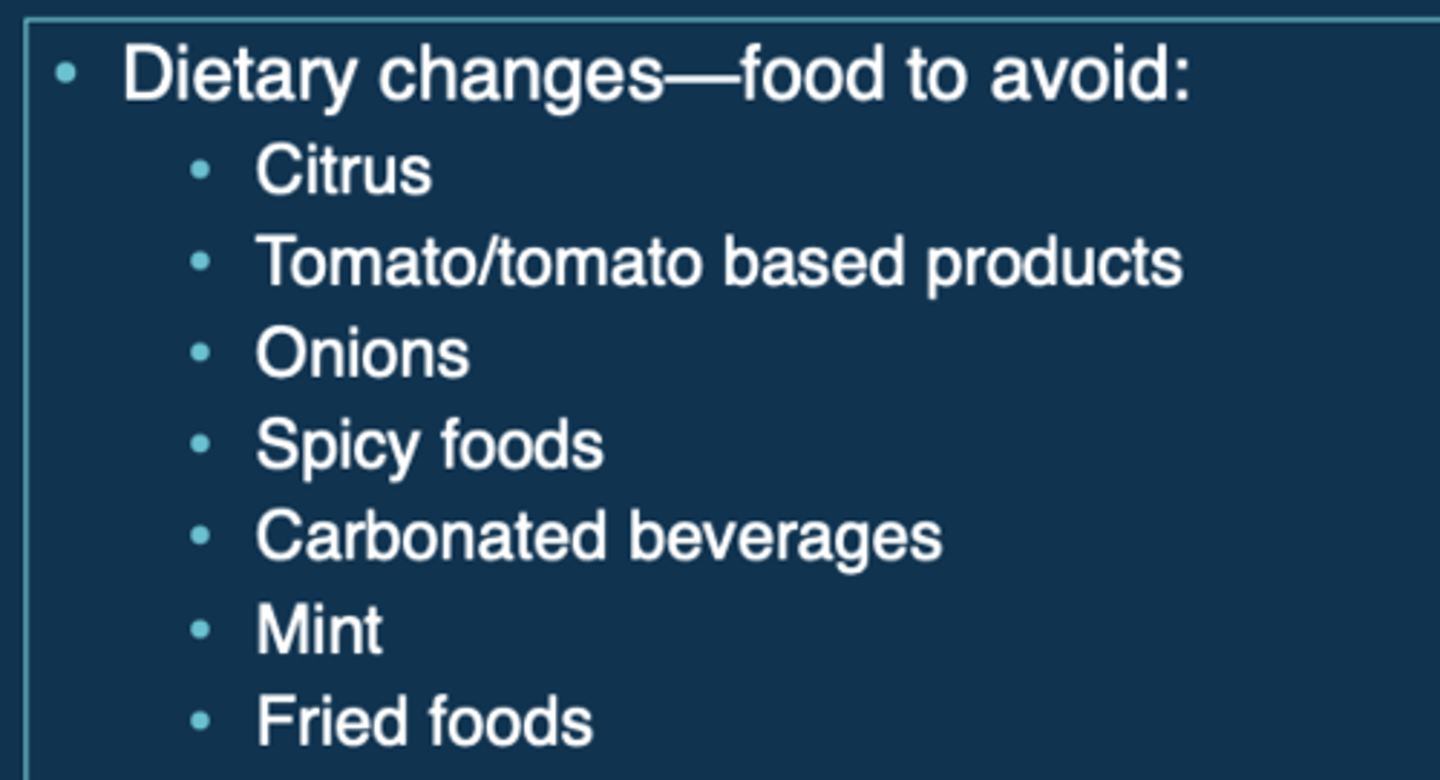
foods causing lower LES pressure and increased GERD
- fatty meals
- garlic
- carminatives (peppermint, spearmint)
- onions
- chocolate
- chilli peppers
- caffeine (coffee, cola, tea)
medications causing decreased LES pressure and increased GERD
-ANTIcholinergics (remember Cholinergics actually constrict LES)
- barbiturates (ex: phenobarbital)
- nicotine, caffeine/theophylline, ethanol
- CCB (amlodipine, nifedipine), nitrates
- progesterone/ estrogens
- dopamine
- tetracycline
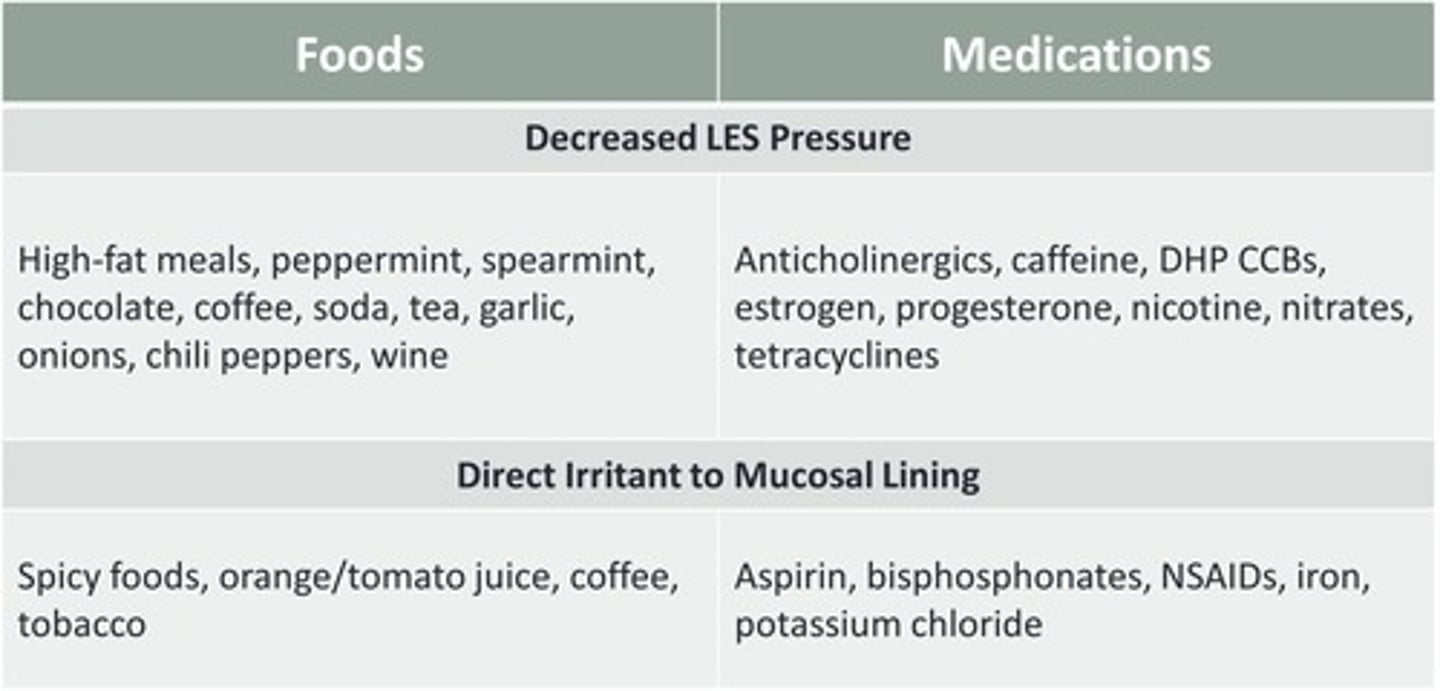
foods that are DIRECTLY irritating to esophageal mucosa
spicy foods, tomato juice, orange juice, coffee
meds that are DIRECTLY irritating to esophageal mucosa
alendronate, iron, aspirin, quinidine, NSAIDs, KCl
risk factors for POOR OUTCOMES/COMPLICATIONS in GERD
Age: over 40
Sx for 3 years
dysphagia (hard to swallow)
bleeding, anemia
weight loss
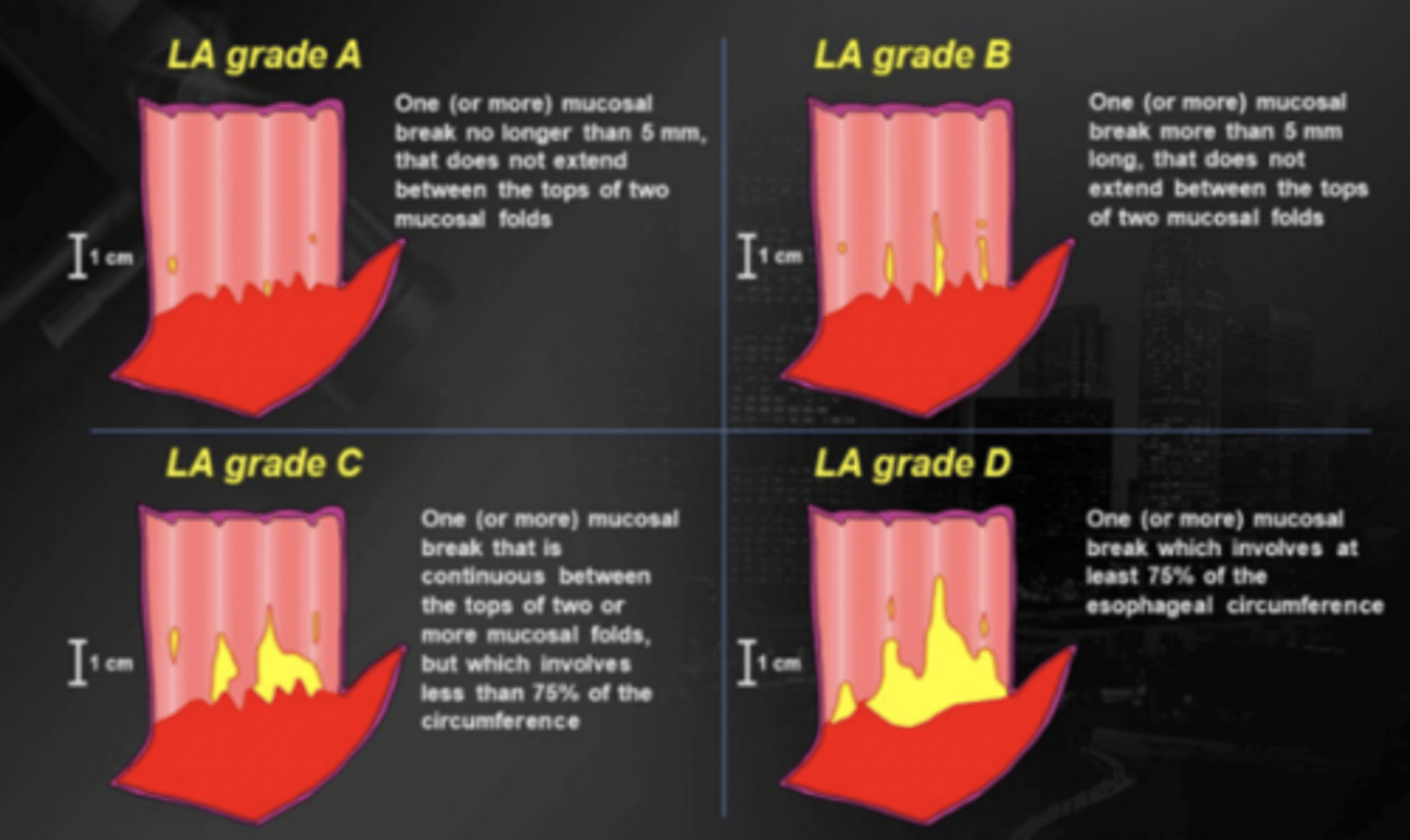
los angeles classifications of reflux esophagitis
LA grade A: best, mucosal break <5mm
LA grade D: worst, break >75%
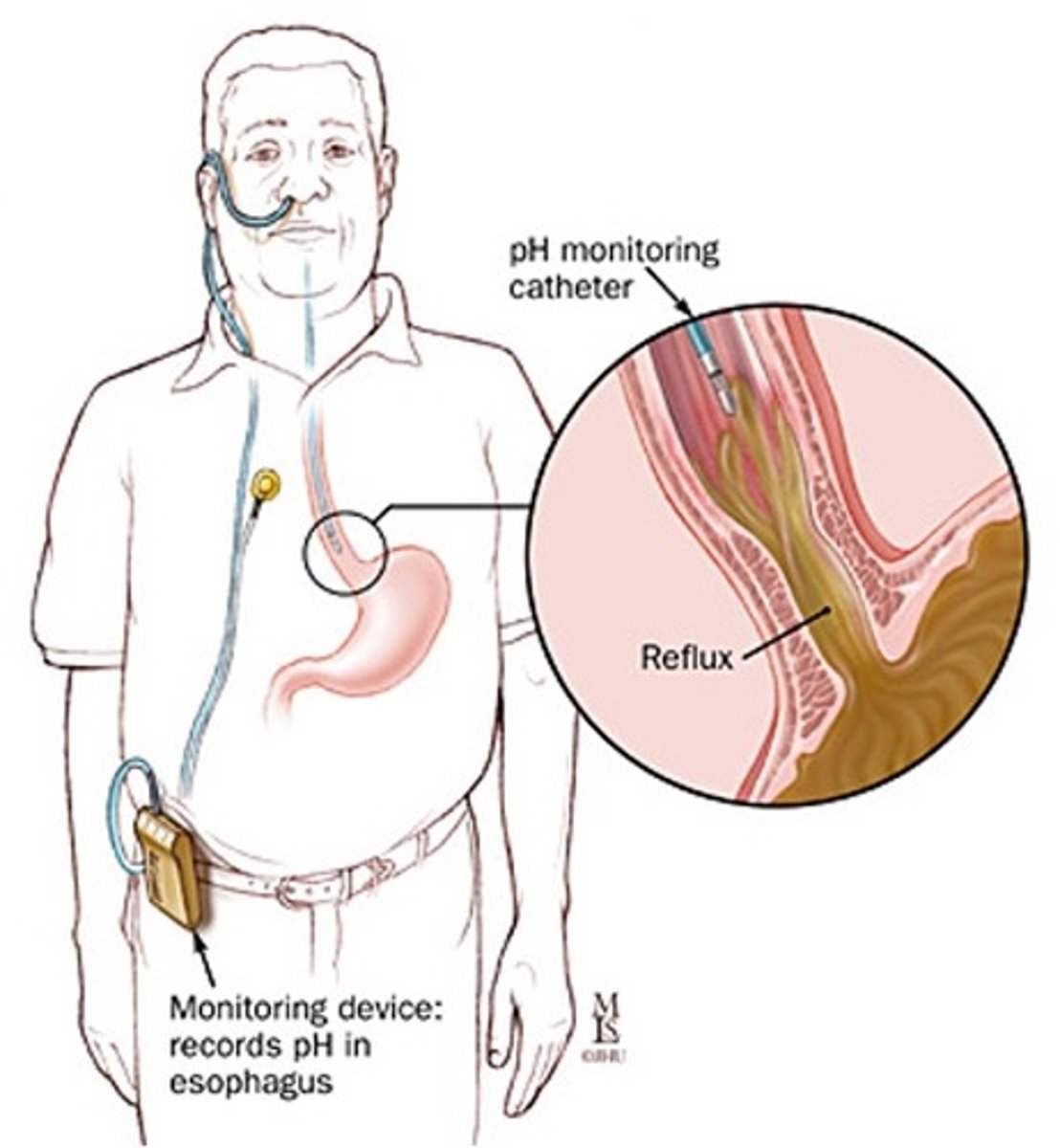
test of choice for diagnosing GERD
ambulatory pH monitoring
- monitoring device inserted in esophagus, if pH drops then reflux is occuring
-costly; used for pts with atypical sx
barium esophagogram
- shows motility abnormalities, hiatal hernia, esophageal stricture
-not helpful in diagnosing GERD with no esophageal damage
[use amb pH monitoring]
![<p>- shows motility abnormalities, hiatal hernia, esophageal stricture</p><p>-not helpful in diagnosing GERD with no esophageal damage</p><p>[use amb pH monitoring]</p>](https://knowt-user-attachments.s3.amazonaws.com/5a3241a6-6bf2-4fcc-8ef0-b102d04bb970.png)
endoscopy
-useful for dx of esophagitis or Barrett's
-not helpful in diagnosing GERD with no esophageal damage [use amb pH monitoring]
![<p>-useful for dx of esophagitis or Barrett's</p><p>-not helpful in diagnosing GERD with no esophageal damage [use amb pH monitoring]</p>](https://knowt-user-attachments.s3.amazonaws.com/40250bdc-d2d1-4295-82c8-192a212db4f2.jpg)
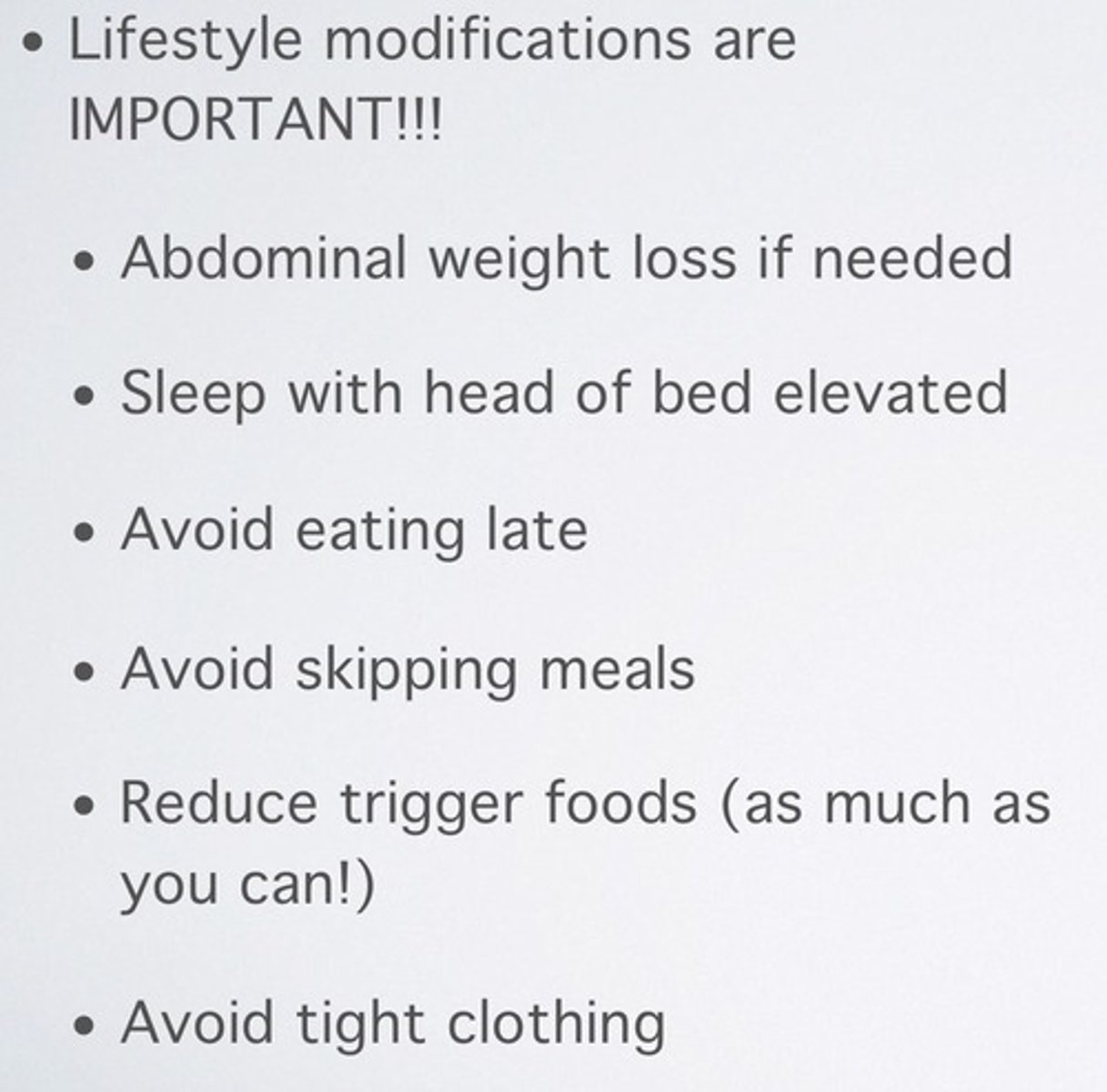
lifestyle modifications for GERD management
1. elevate head of bed
2. modify diet= avoid spice, fatty, mint, chocolate, caffeine
- eat high protein small meals
- avoid eating before lying down
3. avoid tight fitting clothes
4. stop smoking
5. avoid agents that lower LES tone
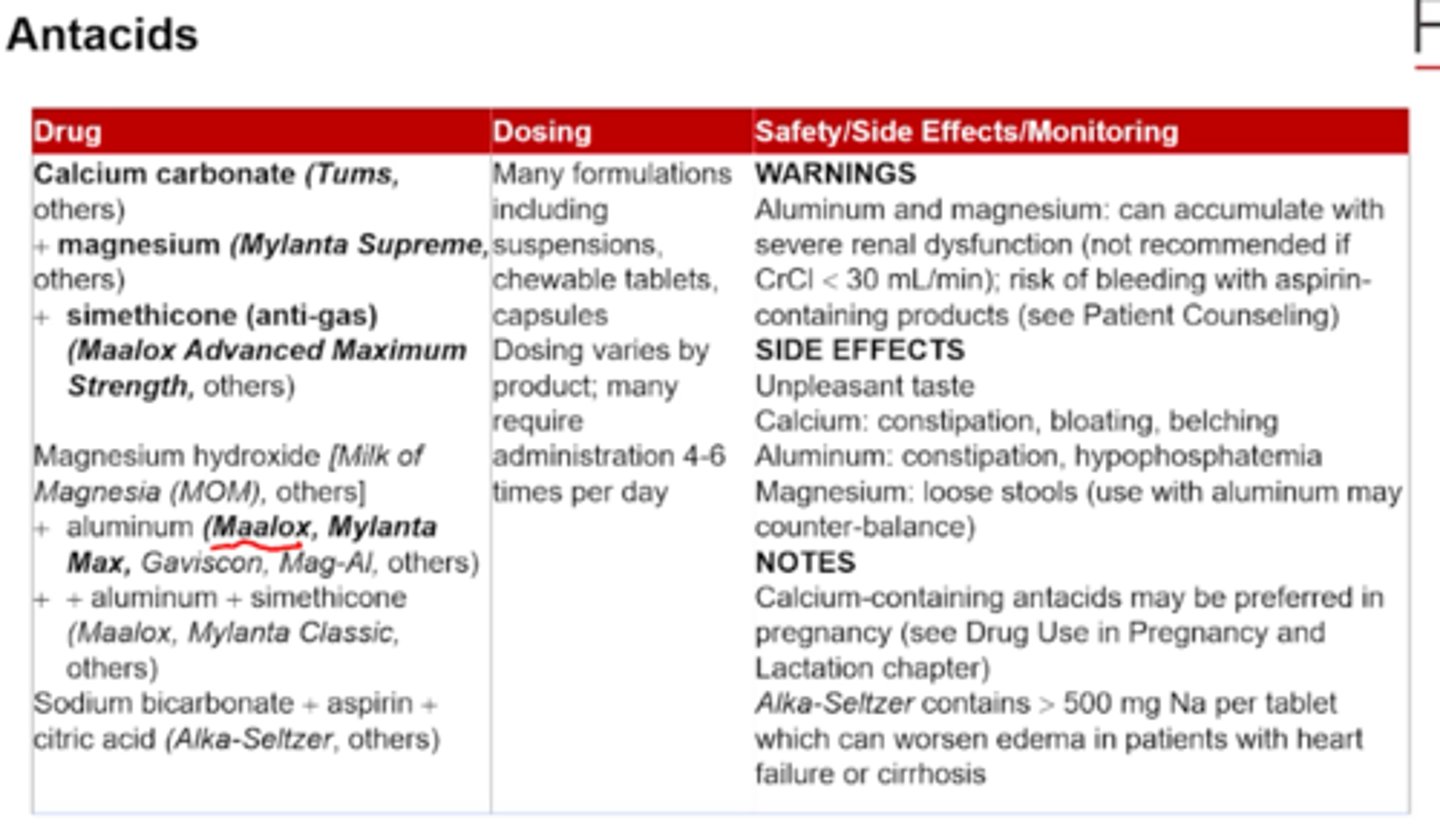
antacids for GERD
MOA
rank from most to least potent
MOA: neutralize acid, bind bile acids and salts, bind pepsin
- relieve symptoms
- liquids preferred
from most to least potent: calcium carbonate (Tums)> sodium bicarb> Mg> Al
antacids
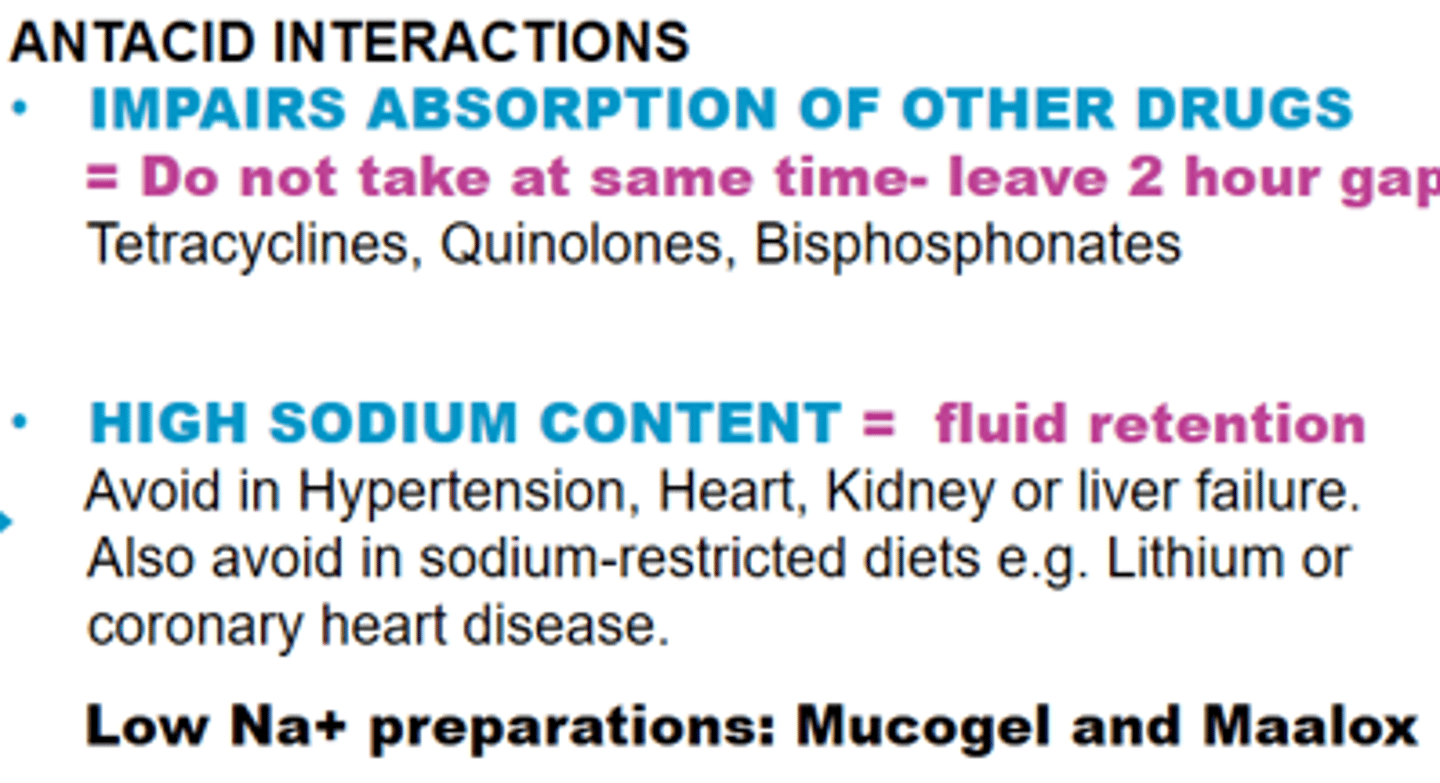
drug interactions may result from:
- formation of insoluble complex
- adsorption
- increase gastric pH (some drugs need acidity-iron)
- increase urinary pH (basic drugs less excreted)
pros and cons of antacids for GERD management
pros:
-OTC, rapid symptom relief
cons:
- frequent dose regimen
- costly to use regularly
-ADE: constipation (Al), diarrhea (Mg), electrolyte changes
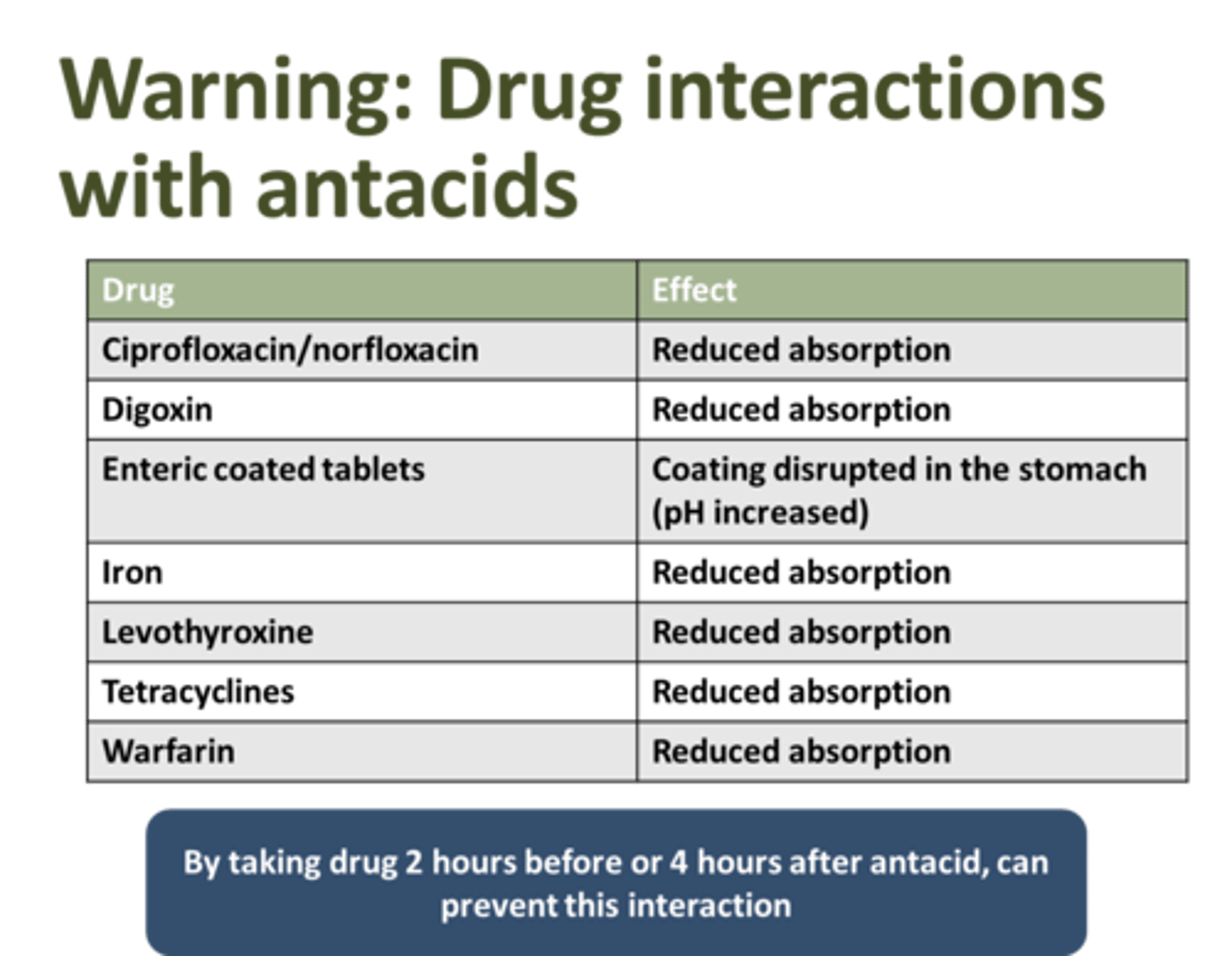
- drug interactions: tetracyclines, iron, quinolones, antifungals
which drugs do antacids interact with, and require dose separation
tetracycline
iron= lower absorption
quinolones (floxacins)
antifungals (azoles)
which ingredients in antacids can lead to diarrhea and which lead to constipation
Mg= diarrhea
Al, Ca= constipation
alginic acid
use in GERD:
MOA:
Gaviscon
= both lower sx AND endo healing
MOA: reacts w saliva to form viscous solution that acts as mucosal barrier
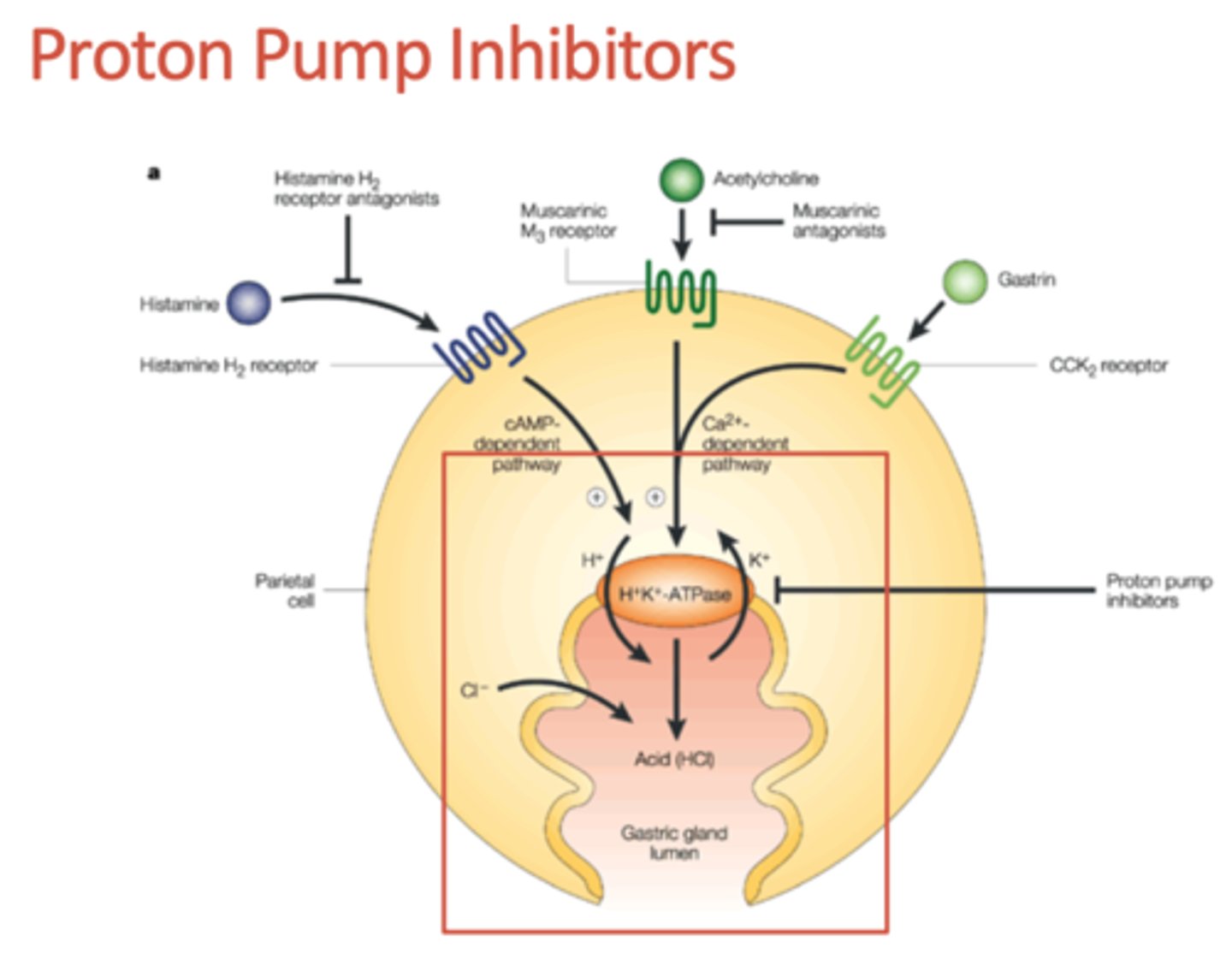
H2RAs
MOA:
reversibly bind to H2 in parietal cells
- decreases cAMP, decreases activation of proton pump, lowers H+ secretion== increased gastric pH
- also decreases secretion of pepsinogen!
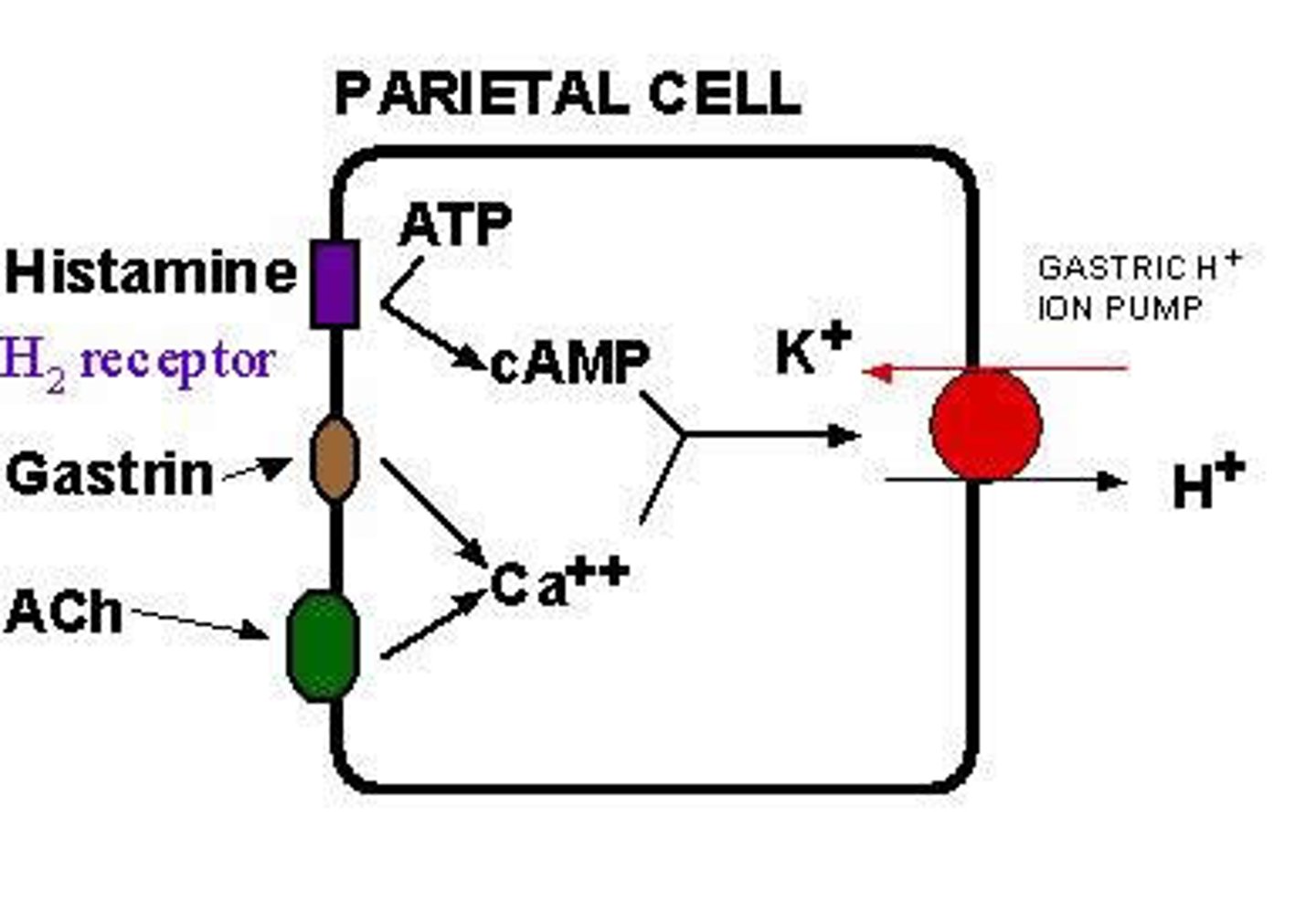
which agents stimulate the parietal cell to secrete H+ via increased cAMP and calcium
histamine= stimulates cAMP
acetylcholine= releases calcium
gastrin= releases calcium
==== activates proton pump
H2RA agents available OTC (generic and brand)
cimetidine (Tagamet)
nizatidine (Axid)
famotidine (Pepcid, Zantac 360)
[ranitidine/zantac was removed bc of NMDA levels]
![<p>cimetidine (Tagamet)</p><p>nizatidine (Axid)</p><p>famotidine (Pepcid, Zantac 360)</p><p>[ranitidine/zantac was removed bc of NMDA levels]</p>](https://knowt-user-attachments.s3.amazonaws.com/ccc39fbf-7c20-4aa1-8b5b-766c6980c287.png)
H2RAs OTC dosing (not prescription!!)
cimetidine:
famotidine:
ranitidine-> not available anymore
over 12 years old
cimetidine (tagamet): 200mg tab w water [max 2]
famotidine (pepcid): 10mg tab w water [max 2]
famotidine (pepcid(: 20mg tab w water [max 2]
which H2RAs may cause diarrhea? which one doesnt have major GI side effects?
cimetidine= diarrhea
nizatidine= diarrhea, constipation, flatulence
famotidine== XXX
which H2RAs have hepatic ADR's? dont?
cimetidine= hepatic fibrosis
nizatidine= increased LFTs
famotidine= XXX
CNS and endocrine ADRs for H2RAs
dizziness, headache, somnolence (drowsy), decreased libido
H2RAs drug interactions mechanisms and drug examples
1. inhibits renal tubular secretion
== creatinine, theophylline, procainamide
2. increases gastric pH, lower absorption for drugs that need acid
== ketoconazole, itraconazole, cefpodoxime
3. inhibit CYPs
== warfarin, theophylline, phenytoin, carbamazepine, propranolol, lidocaine, quinidine
C>N>F
compare H2RAs based on which one has most drug interactions
cimetidine>nizatidine> famotidine
- famotidine has least amount of side effects
- cimetidine known to increase creatinine in blood (may present as AKI)
which PPIs are available and which are OTC vs RX only
OTC:
-lansoprazole (Prevacid)
- omeprazole (Prilosec)
- esomeprazole (Nexium)
RX:
- dexlansoprazole (Dexilant)
- pantoprazole (Protonix)
- rabeprazole (Aciphex)
PPIs MOA
-sulfonamide group on PPI IRREVERSIBLY bind to proton pump and inhibits final step in acid secretion
- reduces secretion of pepsinogen slightly
- increases serum gastrin
mayy develop carcinoid tumors bc of increased gastrin
how are PPIs activated
exposure to gastric acid degrades the PPI, so theyre formulated to be released only when pH> 7 (in intestines)
which PPIs have an interaction with warfarin and what is it
omeprazole and esomeprazole
== inhibit CYP2C19 therefore increasing warfarin's effects-> bleeding risk
PPIs drug interactions
1. decreased absorption bc increased pH
== ketoconazole, itraconazole, cefpodoxime
2. OMEP AND ESOMEP inhibit 2C19
== warfarin!! diphenhydramine, carbamazepine, diazepam
3. reduce oral bioavailability of atazanavir (for HIV)
zegerid
omeprazole/sodium bicarbonate
GERD
-> take combo product on empty stomach or hour before meals
when should PPIs be taken
once a day: 15-30mins before breakfast
twice a day: separate second dose from morning by 10-12hrs
[this is differential!! PUD is always once a day, GERD can be 2x a day]
FDA warnings regarding PPIs
- risk of fractures (give Vit D and calcium)
- risk of C. diff diarrhea
- pneumonia
OTC dosing for PPIs
omeprazole:
Zegerid:
lansoprazole:
esomeprazole:
omeprazole (Prilosec): 20.6mg [1 tab 30mins before breakfast for 14 days]
omep 20mg/ sodium bicarb 1100mg [Zegerid]: 1 cap 1 hr before breakfast for 14 days
lansoprazole (Prevacid) 15mg: 1 cap 30mins before breakfast for 14 days
esomeprazole (Nexium): 20 mg: 1 cap 30mins before breakfast for 14 days]
-> max 1 per day for OTC
compare antacids, H2RAs, and PPIs based on onset and duration of relief
onset:
1. antacids= less than 5 mins
2. H2RAs= 30-45mins
3. PPIs= 2-3hrs
duration of relief
1. antacids= 20-30mins (shortest but PROLONGED w food)
2. H2RAs= 4-10hrs
3. PPIs= 12-24hrs (longest onset but longest duration)
if pt is experiencing
episodic heartburn treat with->
heartburn >2 days per week treat with->
episodic
1. lifestyle/diet modifiers
2. antacid or alginic acid or H2RA
frequent more than 2 days per week
1. lifestyle/ diet modifiers
2. PPI for 14 days or H2RA as needed
when do you know you can stop an OTC PPI? when can you repeat the regimen?
stop if heartburn has resolved after the 2 weeks of PPI (if not-> referral)
repeat regimen every 4 months if needed, or continue H2RA as needed
EXCLUSIONS TO SELF TREAT GERD/HEARTBURN
1. heartburn more than 3 months
2. heartburn persists with use of OTC H2RA or PPI (14 days)
3. severe heartburn and dyspepsia
4. nocturnal heartburn
5. difficulty/pain when swallowing
6. vomiting blood or black tarry stools
7. chronic hoarseness, wheezing, coughing, choking
8. unexplained weight loss
9. N/V/ diarrhea
10. chest pain w sweating, radiating to arm/neck/jaw, SOB
AGES:
- children less than 2 (for antacids)
- children less than 12 (for H2RAs)
- children less than 18 (for PPIs)
- adults >45 with new onset dyspepsia
age exclusions for GERD self treatment
- children less than 2 (for antacids) "Tums Two"
- children less than 12 (for H2RAs) "Tagamet Twelve
- children less than 18 (for PPIs)
- adults >45 with new onset dyspepsia
5 targets for pharm intervention for GERD
1. esophageal clearance
-> bethanechol, cisapride
2. esophageal mucosal resistance
-> alginic acid, sucralfate
3. LES pressure
-> bethanechol, metoclopramide, cisapride
4. gastric emptying
-> metoclopramide, cisapride
5. gastric acid
-> antacids, H2RAs, PPIs
indication for tx of GERD with Rx PPIs
- severe erosive esophagitis (LA grades C or D)
- maintenance tx of GERD
what is the initial dosage regimen for RX PPIs for 4-8 weeks? what about for unresponsive pts- for how long?
initial 4-8 weeks:
omeprazole, esomeprazole, rabeprazole= 20mg qd
lansoprazole= 15-30mg qd
dexlansoprazole= 30mg qd
pantoprazole= 40mg qd
INCREASE DOSE TO TWICE DAILY in unresponsive pts for 4-16 weeks total
adverse rxns for RX PPIs
- headaches
- diarrhea, ab pain, nausea
- bacterial overgrowth
risk of carcinogenesis is not supported
when are RX PPIs the drug of choice?
- moderate to severe GERD
- pts not responding to H2RAs
- pts with complicated symptoms (Barrets, strictures)
PPIs are usually first line tx for GERD
how can PPIs be deprescribed in eligible pts (uncomplicated GERD/ not severe)
1. wean down to lowest effective dose (if sx continue use PPI as needed, or add on H2RAs/antacids for nocturnal sx)
2. reduce twice daily PPI to once daily
which pts are INELIGIBLE to be de-prescribed off of PPIs
1. complicated GERD: severe erosive esophagitis, esophageal ulcer, strictures
2. Barret's esophagus
3. eosinophilic esophagitis
4. idiopathic pulmonary fibrosis
5. high risk of GI bleed
what can occur after PPI discontinuation and how should the pt be educated
rebound acid hypersecretion
-pts can use PPIs, H2RAs, antacids to control sx short term
BUT if sx last >2 months after stopping, they may require continued PPI therapy
t/f: if rebound acid hypersecretion lasts for more than 2 weeks in pts who stopped PPIs, they may require continued PPI therapy
false. if lasts more than 2 months
t/f: data has shown that all PPIs are equally effective in GERD
true
t/f: data has shown that PPIs are just as effective as H2RAs in treating GERD
false. data has shown that PPIs are more effective in healing. H2RAs are only recommended as adjunctive therapy to PPIs or nocturnal breakthrough symptoms
[remember nocturnal cant be self treated tho!]
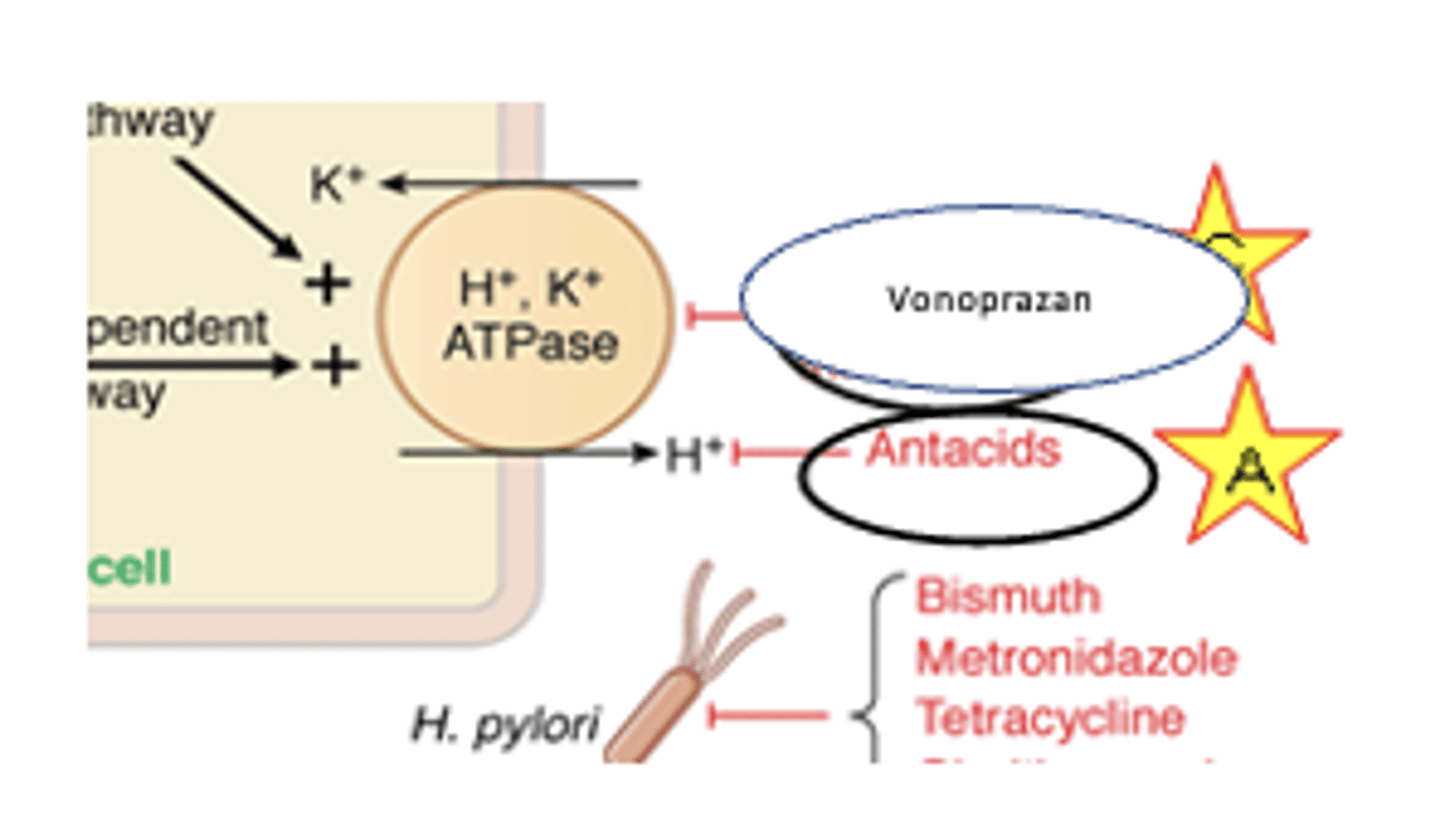
vonoprazan moa
PCAB=potassium competitive acid blocker
REVERSIBLY binds to proton pump
how is vonoprazan metabolized
CYP 3A4 mainly
2B6, 2C19, 2C9, 2D6
-> has longer half life and also a lot of potential drug interactions
t/f: vonoprazan is similar in effectiveness to PPIs in healing erosive esophagitis and improving GERD sx
true
which warnings come with vonoprazan
1. gastric malignancy
2. nephritis
3. c. diff diarrhea
vonoprazan drug interactions
1. CYP 2C19: attenuates/lowers clopidogrel effectiveness
2. lowers absorption of drugs that need acid= atazanavir, nelfinavir, rilpivirine
bethanechol
moa:
dosage regimen:
ADE:
CI:
cholinergic agonist increases LES tone
dosage: 25mg po QID
ADE: pain, diarrhea, urinary frequency, salivation, sweating, lacrimation
CI: asthma, COPD, PUD
NOT RLLY USED BC POOR EFFICACY AND ADRs
metoclopramide
MOA:
dosage:
dopamine antagonist that increases LES tone and accelerates gastric emptying
dosage: 10mg po ac and hs
metoclopramide
ADEs:
drug interactions:
CIs:
efficacy:
ADEs: CNS, extrapyramidal rxn, diarrhea, rash
drug interactions: altered absorption
CIs: Parkinsons, use of other dopamine antagonists or anticholinergics
efficacy: poor efficacy, not rlly used
sucralfate
MOA:
dosage:
mucosal protection, adsorbs to damaged mucosa, binds pepsin and bile salts
dosage: 1gm 1hr before meals (ac) and qhs [suspension!!]
sucralfate
ADE:
drug interactions:
clinical efficacy:
ADE: constipation, hypophosphatemia, aluminum absorption in renal failure pts
drug interactions: adsorbs meds, decreases their absorption
clinical efficacy: NOT FDA APPROVED FOR GERD but helps some
indications for surgery for GERD tx
1. sx dont improve with tx
2. stricture formation
3. severe bleeding
4. dysplastic epithelium
5. pulmonary complications
what is the general approach to treating a pt with mild infrequent sx (<2 days a week) with no signs of erosive esophagitis
1. lifestyle changes
2. antacids, alginic acid, H2RAs prn
3. H2RAs in divided doses
how can erosive esophagitis be treated
REFERRAL
1. lifestyle
2. PPIs
3. combo PPI with promotility agent (remember CNS effects tho! not good for elders)
maintenance tx for GERD
(most relapse after 6 months if dont maintain)
1. lifestyle
2. acid suppression with PPIs
3. refractory pts: combo PPI and promotility
how can pediatrics be treated for GERD
liquid formulations
1. RX PPIs: omeprazole, lansoprazole, esomeprazole, pantoprazole
2. H2RAs: cimetidine, famotidine
but remember you cant SELF treat the following:
- children less than 2 (for antacids) "Tums Two"
- children less than 12 (for H2RAs) "Tagamet Twelve
- children less than 18 (for PPIs)
which drugs are excreted in breastmilk?
H2RAs and PPIs
(risk vs benefit)
which drug is the first line choice in pregnancy
famotidine
(PPIs can still be used when clinically indicated)
notes for treating geriatrics for GERD
- may think this is normal part of aging
- decreased motility is common problem
- metoclopramide and H2RAs may cause confusion/delirium bc of their CNS effects
when should single dose PPI therapy be assessed to see if it worked? what if it DID work?
4-8 weeks
if symptoms got better:
1. wean to lowest effective dose
2. continue on lowest dose or switch to prn
pts on chronic PPI for _______ should be offered reflux testing to determine requirement for lifelong therapy
1 year
when should single dose PPI therapy be assessed to see if it worked? what if it DID NOT work?
4-8 weeks
didnt work:
1. assess compliance
2. increase dose to 2x a day PPI [not fda approved tho]
------> assess again
if still not improved
1. EGD and wireless pH testing OFF of the PPI
what is the overall tx algorithm for GERD (summary)
weeks 1-8:
weeks 9-16: (if sx persist)
weeks 17+: (if sx persist)
weeks 1-8
1. start with PPI qd
2. use H2RA for nocturnal breakthrough
----> if sx improve, dc or taper
weeks 9-16
1. increase PPI to BID, change PPI, or split PPI dose
2. use H2RA for nocturnal breakthrough
3. add alginate antacid for sx control
weeks 17+
1. continue HD PPI
2. use H2RA for nocturnal breakthrough
3. add ons: baclofen, metoclopramid if concomitant gastroparesis
which drug can be added on for GERD tx with gastroparesis
metoclopramide (note CNS sedation in elders)
how should dose be altered for ultrarapid metabolizers
increase starting dose by 100%
-> may be given in divided doses
for rapid or normal metabolizers, dose may be increased by __________ for tx of H. pylori infection and erosive esophagitis
50-100%
how should dose be altered for intermediate/poor metabolizers
initiate standard dose
- consider 50% reduction for chronic therapy (>12 weeks)
why may asthma worsen in the presence of GERD
GERD can trigger asthma symptoms through vagus nerve stimulation and bronchoconstriction
pt MR presented to doctor with erosive esophagitis. she has been prescribed pantoprazole and has not had any other sx since. is she eligible for discontinuation?
no, she has erosive esophagitis and needs to stay on it long term
remember exclusions for de-prescribing:
1. complicated GERD: severe erosive esophagitis, esophageal ulcer, strictures
2. Barret's esophagus
3. eosinophilic esophagitis
4. idiopathic pulmonary fibrosis
5. high risk of GI bleed