Lecture 3 MARK k Lectures
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
Calcium Channel Blockers
*Calcium-Channel Blockers are like Valium for your heart
Valium -> calm’s you down; so CCB’s calm your heart down
(ex. if tachycardic, give CCB’s but not in shock)
THEY REST YOUR HEART (not stimulants)
Positive Inotropes, Chronotropes, Dromotropes
Cardiac Stimulants- stimulate, speed (up the heart)
Negative Inotropes, Chronotropes, Dromotropes
Cardiac Depressants: calm the heart down, (weaken & slow down)
When do you want to “depress” the heart? What do CCB’s treat?
A: anti-hypertensives: Relax heart & blood vessels to bring down BP
AA: anti-angina’s: Relax heart to use less O2 to make angina go away
/ treats angina by addressing oxygen demand
AAA: anti-atrial arrhythmia: atrial flutter, A-fib, premature atrial contractions
* Never ventricular
what about supra-ventricular tachycardia??
Because it means ‘above the ventricles’ (which (are the atria)
What are the side effects of CCB?
****“H & H” ****
HYPO tension (low blood pressure)
Headache: vasodilation to the brain
* Hint: headache is a good thing to select for (‘select all that apply’ questions.
Names of CCB’s (calcium channel blockers)
Anything ending in ‘-dipine’
- ex. amlodipine, nifedipine
Name of OTHER CCB’s that DONT end in -dipine’
VERAPAMIL & CARDIZEM
Which CCB can be given on a continous IV drip??
Cardizem
What VS needs to be assessed before giving a CCB?
BP = because of risk of hypotension (low blood pressure)
Parameters/guidelines - hold CCB if systolic is (under 100)
You need to monitor BP if PT is on a Cardizem (continuous drip (if it’s under 100 then you may (have to stop or change the drip rate)
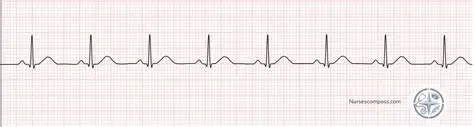
Normal Sinus Rhythm
P wave before every QRS & followed by a T wave for every single complex,
All P wave peaks are equally distant from each (other, QRS evenly spaced)
V-Fib
Chaotic squiggly line, no pattern

V-tach
sharp peaks, has a pattern

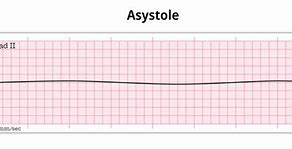
A-Systole
flat-line
QRS depolarization,
it’s talking about ventricular ( (so rule out anything atrial)(
P-wave
then it’s talking about atrial
The word “chaotic” is used to describe
A-fib: with “p-wave”
V-fib: with QRS
The word “bizarre” is used to describe
Atrial Tachycardia if w/ P wave
Ventricular Tachycardia if with QRS
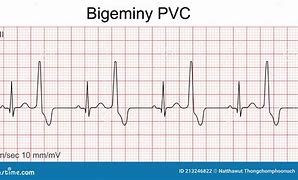
PVC’s
(premature ventricular contractions)
Also known periodic wide bizarre QRS (ventricular because QRS)
Bizarre -> tachycardia (- you can call a group of PVC’s a short run of V-tach)
Do Physician’s care about PT’s having PVC’s?
NO, not a high priority = low priority
They NEVER reach top priority (highest is moderate priority)
How do you know if PVC’s should be moderate priority?
i. If there are more than 6 PVC’s in a minute
ii. If there are more than 6 PVC’s in a row
iii.If the PVC fall on the T-wave of the previous beat (R on T phenomenon)
Lethal Arrhythmia’s (HIGH PRIORITY (Will kill you in 8 mins or less)
Asystole
V-Fib
BOTH HAVE NO CARDIAC OUTPUT
What is the medication for V-Tach and PVC’s
for ventricular use LIDOCAINE/****AMIODARONE***
Atrial arrhythmias use ABCD’s
A: Adenocard (Adenosine)
B: Beta blockers
C: Calcium channel blockers
D: Dig/ Lanoxin
ADENOCARD (Adenosine)
- Have to push in less than 8 seconds (FAST IV (push)
Slam this drug, followed by a flush; use a big vein; BUT the problem w/ slamming it fast is (the risk of PT going into A-Systole for 30 seconds. THEY WILL come out of it so don’t worry …unless longer than 30 sec.
for IV pushes: when you don’t know you go slow
BETA-BLOCKERS
all end in ‘-lol’
Are negative inotropes, chronotropes, & dromotropes like calcium-channel blockers (a.k.a. valium for your heart so they treat A, AA, AAA & (have same side-effects)
** generally speaking, don’t make a big difference (between Beta- & Calcium channel blockers
CCB are better for PT’s w/ asthma ( or COPD -> Beta-B’s bronchoconstrict
Digitalis
Med: Lanoxin
Used for patients with heart failure (to improve blood circulation)
Control’s A-Fib (rate and rhythm)
S&S of DIG TOXICITY (lanoxin)
Bradycardia (↓ HR) ⚠
Dysrhythmias (irregular heart rhythms)
Anorexia (early sign)
Nausea, vomiting
Fatigue, weakness
Confusion, dizziness
Yellow/green vision, halos
Risk ↑ with hypokalemia
How do you trat V-Fib?
you SHOCK them!!!
How do you trat asystole??
Use EPINEPHRINE & ATROPINE (in this order!)
*if epinephrine doesn’t work then use atropine
Chest Tubes??
Purpose is to re-establish negative pressure in the pleural space (so that the lung expands when the chest wall moves)
Pleural space -> negative is good (negative pressure (makes things stick together)
Ex. gunshot to the lung adds positive pressure
Hint: when you get a chest tube question, look at the reason for which it was placed (will tell you what to expect & what not to expect
Pneumothorax
to remove air (because air (created the positive pressure)
Hemothorax
to remove blood
Pneumohemothorax
to remove blood & air
Apical placement
The chest tube is way up high, thus it is ( removing air (because air rises)
ex. it’s bad if you’re apical tube is draining 200 mL or it is not bubbling
Basilar placement
At the bottom of the lungs, thus it is (removing blood/liquid (because of gravity)
ex. it’s bad if your basilar tube is bubbling or not draining any mL
How many chest tubes & where would you place them for a unilateral pneumohemothorax?
2 chest tubes (apical for pneumo, basilar for hemo)
How many chest tubes & where would you place them for a bi-lateral pneumothorax?
2 tubes (apical on left, apical on right)
How many chest tubes & where would place them for post-op chest surgery?
2 tubes (apical & basilar on the side of the surgery)
*you are to assume that chest surgery/trauma is (unilateral unless otherwise specified (they will say bilateral)
How many chest tubes would you need and where would you place them for a post-op right pneumonectomy?
NONE! because you are removing the lung so you ( don’t need to re-establish any pressure (there is not ( pleural space)!
What do you do if you knock over the plastic containers that certain tubes are attached to?
Set it back up & have PT take some deep breaths
NOT a medical emergency! (don’t call MD)
What do you do if the water seal breaks?? like the actual device breaks?
First = CLAMP it!!! because now positive pressure (can get in! don’t let anything get in
Second = CUT the tube away from the broken device
Third = stick that open end into sterile water (-> then unclamp it because you’ve re-established the water seal doesn’t need clamp if it’s under water)
*** BETTER for the tube to be under water THAN clamped! -> air can’t go in and stuff can still keep coming out (if clamped, nothing can come out, which is what the tube is for)
What is the first thing to do when the if the seal breaks?
Clamp the tube!!
What’s the best thing to do when the seal breaks??
Put the end of the tube under water!!
You notice the PT has V-fib on the monitor. You run to the room and they are non-responsive with no pulse. What is the first thing you do?
A. place a backboard
B. Start chest compressions
A. place a backboard
You notice the PT has V-fib on the monitor. You run to the room, and they are non-responsive with no pulse. What is the best thing to do?
A. place a backboard
B. Start chest compressions
B. Start chest compressions
What is the first thing you do if the chest tube gets pulled out?
A. Take a gloved hand and cover the hole
B. Cover the hole with vaseline gauze
A. Take a gloved hand and cover the hole
What is the best thing you do if the chest tube gets pulled out?
A. Take a gloved hand and cover the hole
B. Cover the hole with vaseline gauze
B. Cover the hole with vaseline gauze
Bubbling chest tubes, what are the two questions you ask?
A) Where is it bubbling?
B) When is it bubbling?
Intermittent bubbling in the water seal?
It is a good sign, the water seal is supposed to be bubbling intermittently
Continuous bubbling in the water seal??
It is a BAD sign; the water seal is NOT supposed to be continuously bubbling, means a leak in the system that you need to find and tape it until it stops leaking.
Intermittent in suction control chamber
BAD sign, means suction is not high enough, turn it up on the (wall until bubbling is continuous)
Continuous in suction control chamber
Good sign, the suction is supposed to be suctioning continuously.
What is a thoracentesis??
Second alternative, that assist with reestablishing negative pressure into the pleural cavity.
“temporary”
A straight Cath to a foley is what a thoracentesis is to a chest tube.
between a chest tub and a thoracentesis, a chest tube has a higher risk of infection.
How long can you clamp a chest tube for??
15 Seconds (MAX)
Use rubber tipped clamps, to not puncture the tube.
Congenital Heart defects YOU NEED TO REMEBER
REMEMBER THE WORD TRouBLe
Every congenital heart defect is either TROUBLE or NO TROUBLE (ALL BAD or NO BAD)
Either causes a lot of problems or it’s no big deal (no in-between defect)
Trouble congenital heart defects
All of the “trouble” congenital heart defects start with the letter “T”
Surgery is required
Growth, development and life expectancy: Slow, delayed and short
Parents experience: Grief, financial stress, lot’s of caregiving issues.
Going home: apnea monitor
Hospital stay at growth: weeks
Who follows care: Pediatrician, Cardiologist
Shunting: R to L (tRoubLe)
Cyanosis: Blue (trouBle)
Congential heart defects that are not trouble
Don’t need surgery
growth and development: normal
life expectancy: normal
parent’s experience: regular average person issues
going home: no apnea monitor
Hospital stay at birth: 24-48 hours
Who follows care: pediatrician/ pediatric NP
Cyanosis: Acyanotic
If the question on the NCLEX refers that you are teaching parents about a congenital heart defect that is trouble ..
Pick the answer choices that are trouble, teach the parent’s that it is going to be alot of trouble.
If the question on the NCLEX refers that you are teaching parents about a congenital heart defect that is not going to be trouble
Pick all the answer choices that are not trouble; teach the parents that it is not going to be trouble.
Kids with a Trouble or NOT trouble congenital heart defect will ALL have a ….
MURMUR
Why? = because of the shunting of the blood regardless of direction of shunt
All have an Echocardiogram done to find out what the defect is or why there’s a murmur.
4 Defects of Tetralogy of Fallout:
“VarieD PictureS Of A RancH”
1. VD = ventricular defect
2. PS = pulmonary stenosis
3. OA = overriding aorta
4. RH = right hypertrophy
Contact precautions
For anything enteric = can be caught from intestine, fecal, oral.
C-Diff,
Hep. A
Cholera
Dysentery
Staph infections
C-Diff
Herpes infections
Shingles
Zoster (varicella)
What PPE do you use for contact precautions?
NO: mask, eye/face shield (unless for universal), ( special filter mask, PT mask, neg. air flow.
YES: gloves, gown, hand-washing, special supplies & dedicated equipment (includes toys) ** disposable supply vs. dedicated equipment, thermometer cover - BP cuff that stays in room.
Private or non-private room for CONTACT precautions??
Private room is preffered (but not required)
This means two kids with RSV can be in the same room together
Can one kid with RSV and one kid with SUSPECTED RSV can be roomed together?? NO NO NO we need positive cultures to CONFIRM that the child has RSV.
DROPLET precautions
For bugs that travel 3 feet on large particles due to sneezing/coughing
- all meningitis: cultured through lumbar puncture
H Flu (haemophilus)
Influenza B -> commonly causes epiglotitis( never stick something down throat because it will cause obstruction.
For DROPLET precautions is it a private or non-private room
PRIVATE ROOM
What is the PPE for DROPLET precautions??
NO: gown, eye/face shield, special filter mask, (neg. air flow
YES: mask, gloves, hand-washing, PT worn (mask when leaving room), disposable supplies (& dedicated equipment)
Airborne precautions
M-M-R
TB
Varicella (chicken pox)
Private or non-private room for Airborne precautions
PRIVATE ROOM (repeated answer)
PPE for AIRBORNE precautions?
NO: gown (mostly for contact), eye/face shields
YES: mask, gloves, hand-washing, special filter (mask ONLY for TB, PT mask for leaving room (but really shouldn’t be leaving).
Neg. Air flow disposable supplies & dedicated equipment is a good thing but not really as essential.
PPE = Personal Protective Equipment
ALWAYS TAKE OFF IN ALPHABETICAL ORDER
ex: gloves, goggles, gown, mask
putting on is reverse alphabetically for the ‘g’s’ & mask comes 2nd
ex:gown, mask, goggles, gloves