Hemodialsysi Access Grafts (13)
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
what are the risk facots for renal disease?
age
hypertension
race
diabetes
kidney disease
smoking
hyperlipidemia
obesity
cad
Qs what are the superficial veins in UE?
basilic
cephalic
median antecubital
what are the deep veins in UE?
internal jugular vein
subclavian vein
axillary vein
brachial veins
ulnar veins
radial veins
what are the arteries of the UE?
brachiocephalic artery
subclavian artery
axillary artery
brachial artery
ulnar artery
radial artery
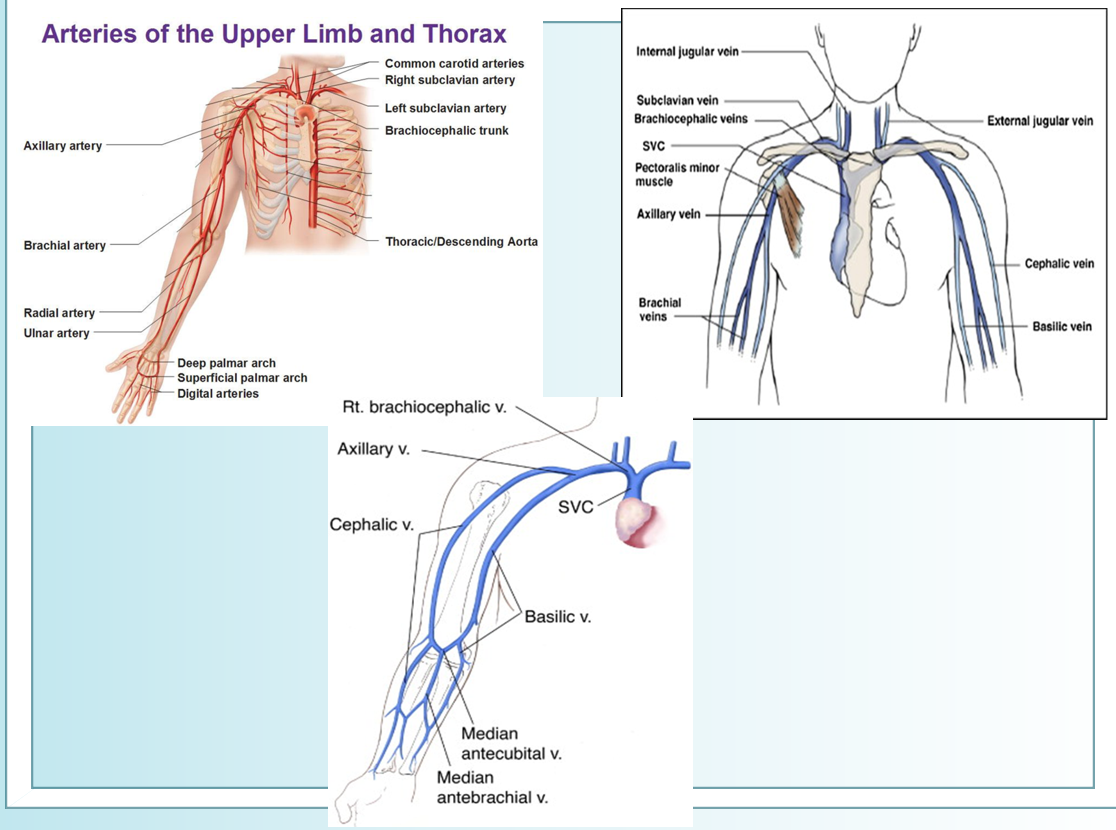
deep palmar arch is formed by
radial art and branch of ulnar
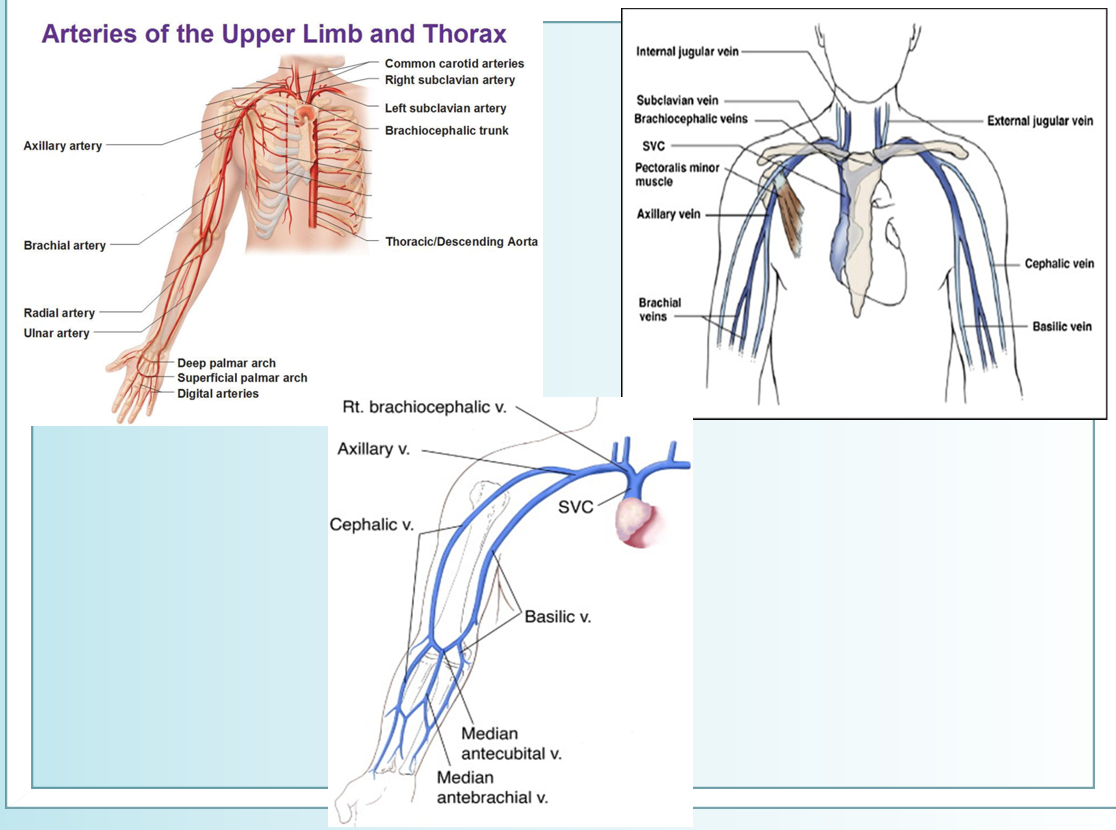
superficial palmar arch is formed by
ulnar art and branch of radial art
what is hemodialysis?
method used to remove waste products such as creatinine and urea from blood
blood cleansed by diffusion across a semipermeable membrane - dialyzer
for patients with end stage renal disease
accesses centeral circulation via AVF, graft or central venous dialysis catheter
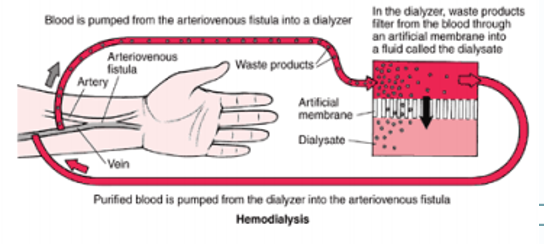
how do we create high flow situations for hemodialysis?
creating arteriovenous fistulas
connects artery and vein together
in hemodialysis
distal needle →
prox needle →
distal needle → artery → to hemodialysis machine
prox needle → venous flow → from hemodialysis machine
best site for hemodialysis?
forearm
then upper arm graft
then thigh graft
Qs what is venous mapping?
mapping of both superficial venous system and arterial system in the upper and lower extremities before access placement
Qs which veins are mapped in UE?
basilic
upper arm : prox, mid, distal
forearm : prox mid distal
wrist
cephalic
upper arm : prox mid dist
forearm : prox mid dist
wrist
Qs how are the increments evaluated in UE mapping
compressibility (coaptation)
diameter (AP measurement in trv)
continuity (grayscale)
AP measurement (sag)
color dopp (sag)
PSV (sag)
which veins are mapped in LE?
great and/or small saphenous veins are mapped
high mid distal thigh
knee and below knee
prox, mid, distal calf
ankle
the increments for LE mapping are evaluated for
compressibility (coaptation of vessel walls)
diameter (AP measurement in trv)
continuity
*also look for wall thickening and mural classifications
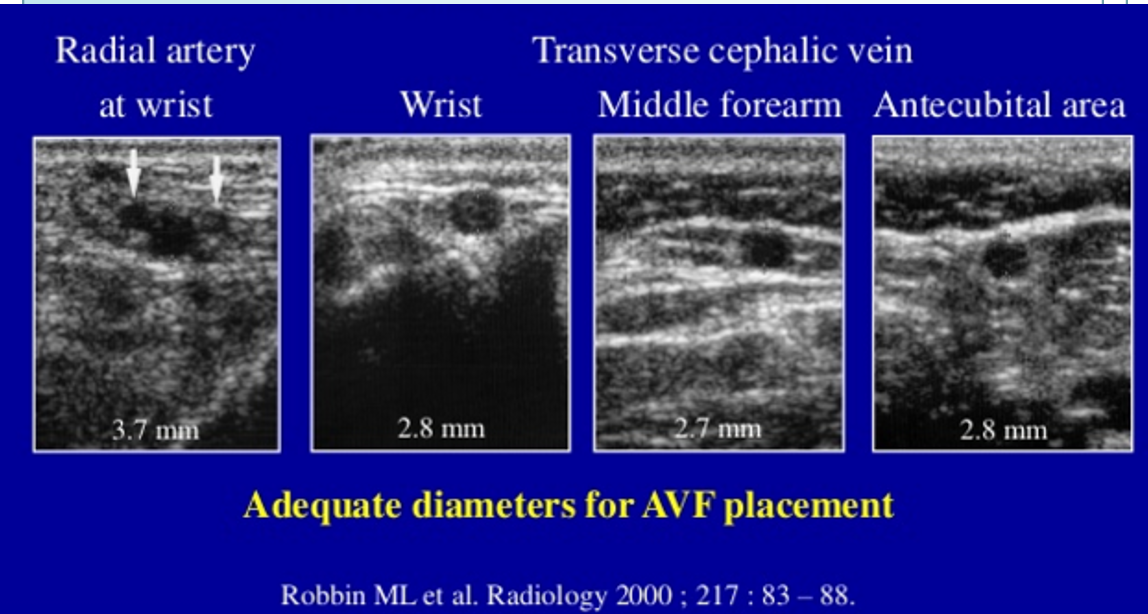
adequate diameters for AVF placement
what is the optimal patient positioning for LE mapping?
hip externally rotated and knee slightly flexed
Qs after the first rib the subclavian v becomes the
axillary vein
Qs how central circulation for hemodialysis is accessed?
central venous catheter is inserted into large central vein that leads to heart
usually basilic because it is large
can be through AVF (surgical connection between artery and vein)
can be through AVG (tube that connects artery and vein)
Qs what is the most desirable site for hemodialysis access?
forearm
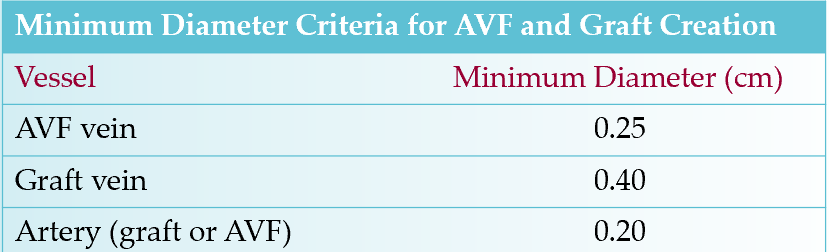
Qs what is the minimum diameter criteria for AVF? graft? artery?
AVF : .25
graft : .4
artery : .2
what are the types of grafts?
prosthetic
biological (bovine, heterografts,cryopreserved)
synthetic
autogenous
in situ vein (using native veins as a conduit)
basilic
cephalic
great saphenous
femoral
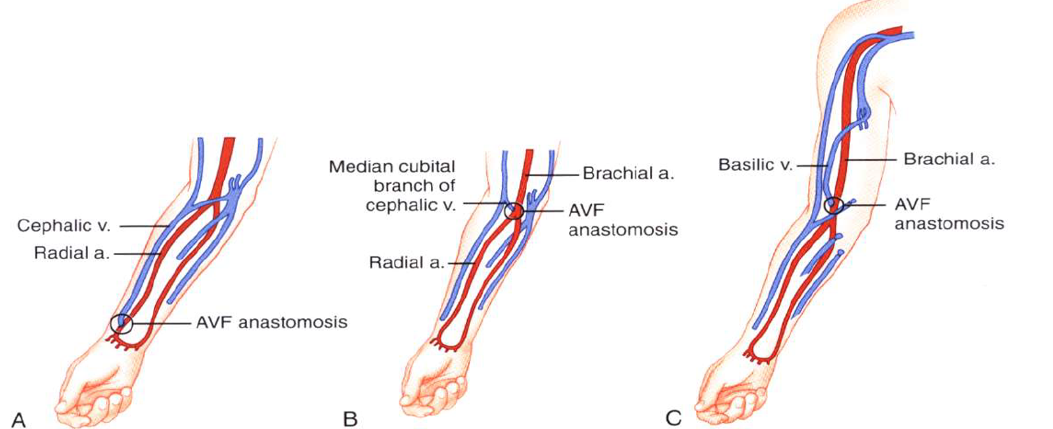
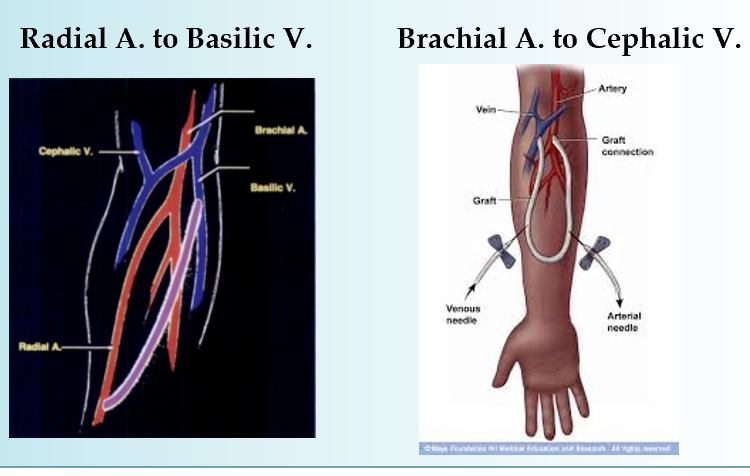
what are the common connections of AVF/AVG?
brescia cimino (A)
radial artery to cephalic vein
radial artery-basilic vein
forearm transposition
brachial artery to cephalic vein (B)
antecubital area
upper arm
snuffbox fisutal
branch radial artery - cephalic vein
brachial artery to upper arm basilic vein transposition (C)
great saphenous, common fem or femoral vein
common femoral artery or superficial femo artery
axillary artery - axillary vien
axillary artery - ipsilateral or contralateral jugular vein
subclavian artery - contralateral subclavian vein
“necklace graft”
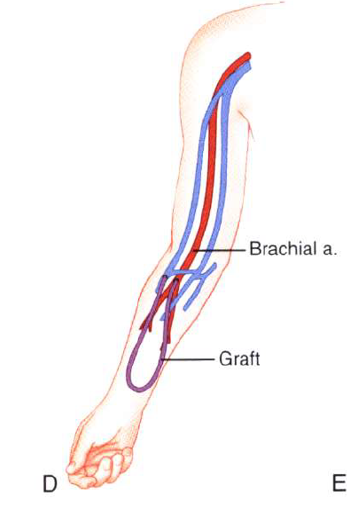
in forearm and upper arm grafts are usually -
in thigh grafts -
forearm and upper arm : loop or straight
thigh grafts : loop
shows what
forearm loop graft
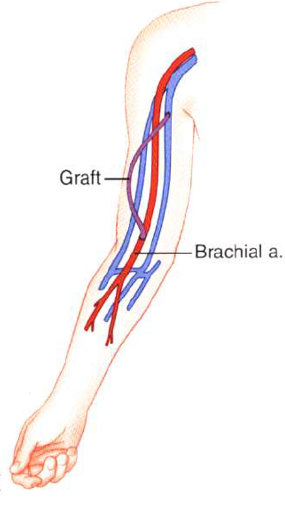
shows what
upper arm straight graft
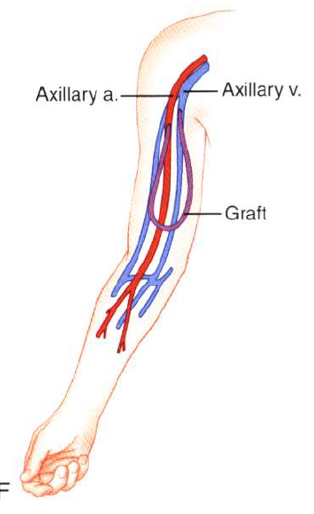
what does this show?
axillary loop graft
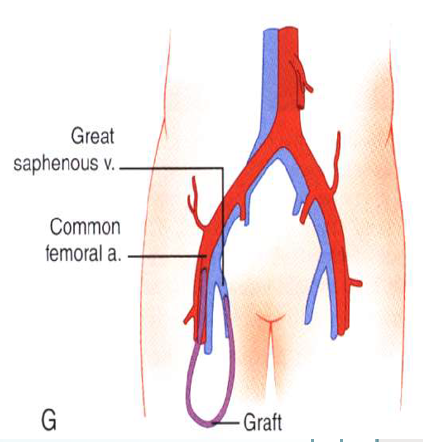
what does this show
thigh graft
what are the inflow sites?
ALL ARTERIES
radial artery at wrist
brachial artery at antecubital fossa
prox brachial artery
axillary artery
common fem artery
superficial fem artery
subclavian artery
what are the outflow sites?
cephalic vein
median antecubital vein
basilic vein
great saphenous vein
femoral vein
subclavian vein
what are the access anastomoses?
end to side
end to end
side to side
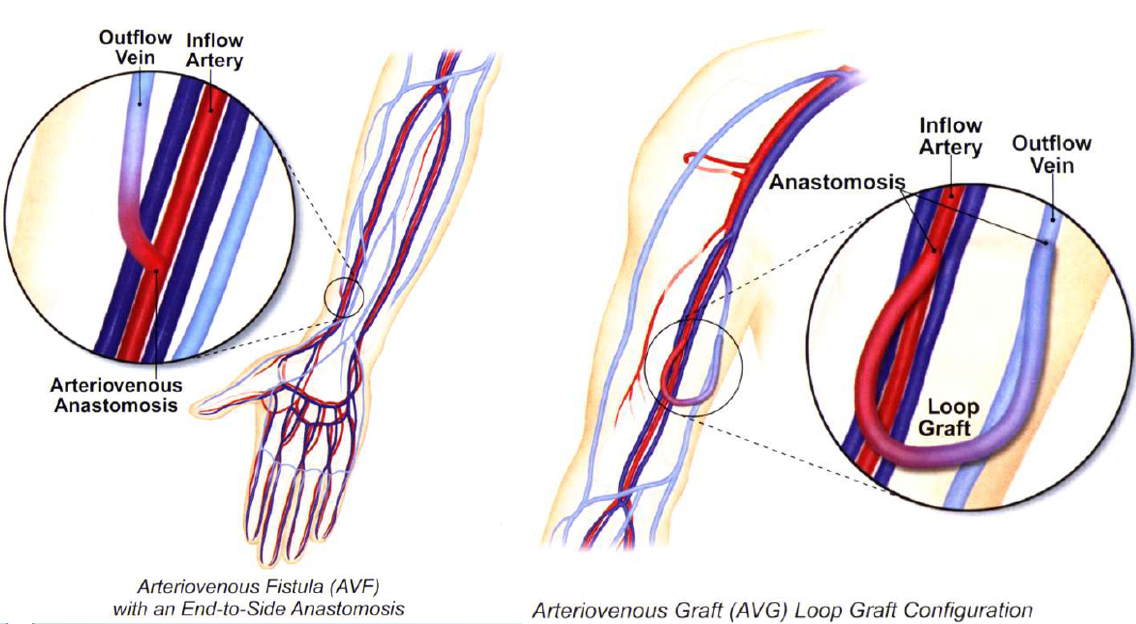
Qs what is an AV fistula?
when native artery is connected to native vein
how long does it take for an AV fisutal to mature?
up to 24 months after surgery
more blood flow into the vein causing it to grow larger and stronger
if fails to grow twice → AV graft
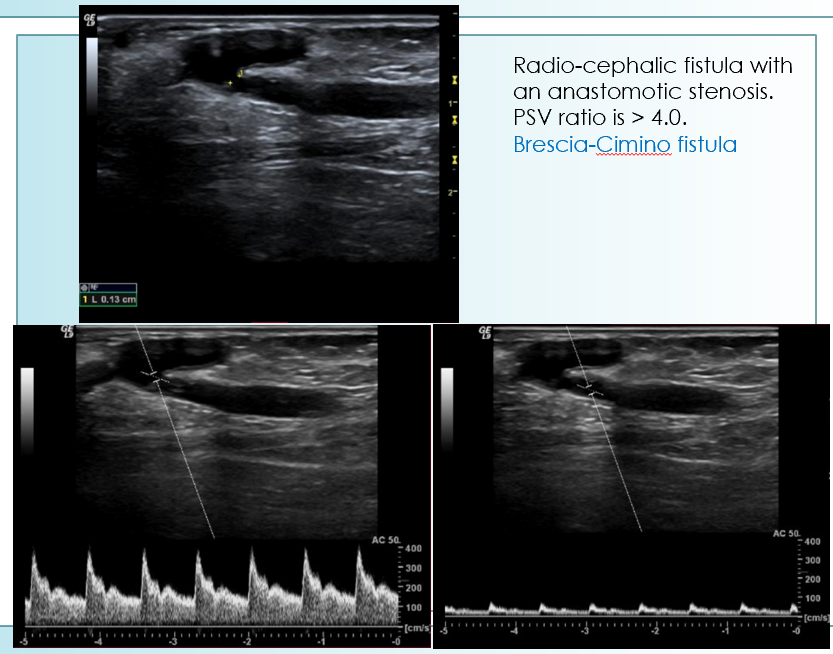
which fistula is most commonly performed?
brescia cimino
radial artery to cephalic vein
end to side vein to artery anastomosis
Qs why is AVF preferred over AVG for vascular access in hemodialysis?
provides adequate blood flow
lasts longer than other types of access (can function up to 20 years)
lower complication rate
less likely to be infected/cause blood clots

review

what is this?
side to end AVF
what is this?
side to side AVF
what is this?
end to end AVF
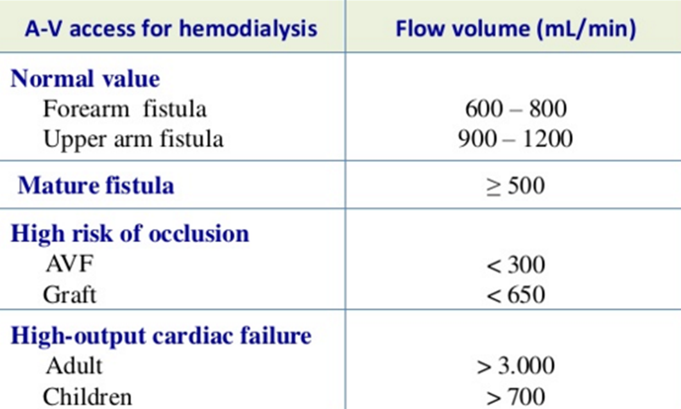
Qs an AVF is mature when
venous diamter is >/= 4mm
flow volume is >/= 500 ml/min
*blood flow measured at midportion
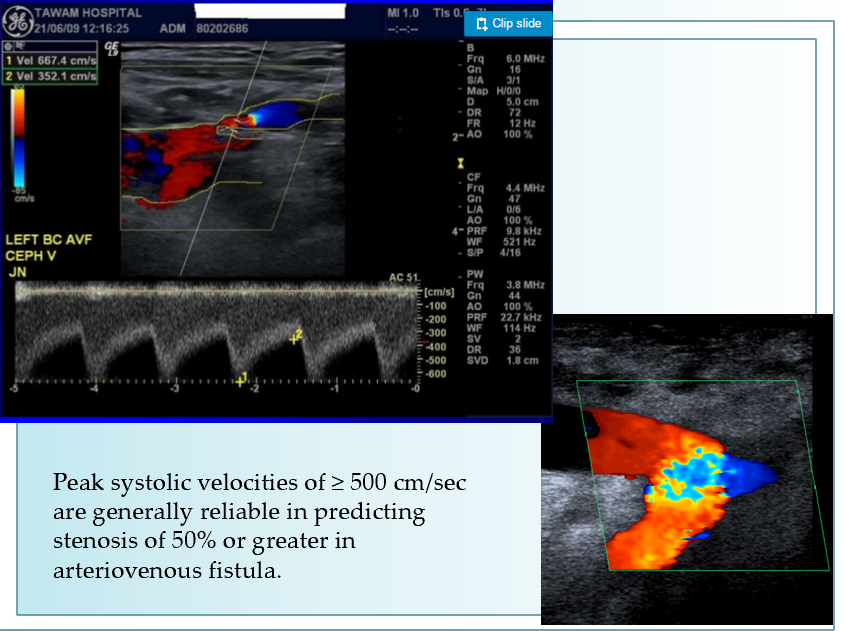
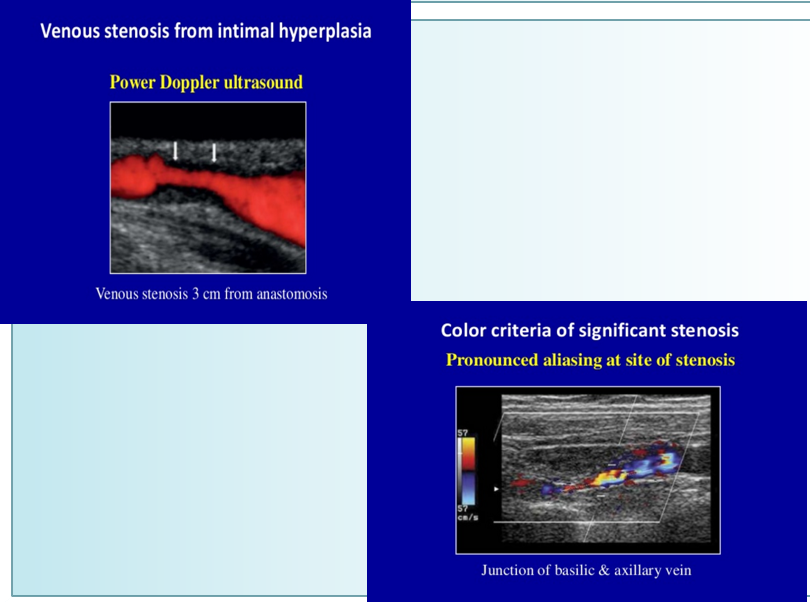
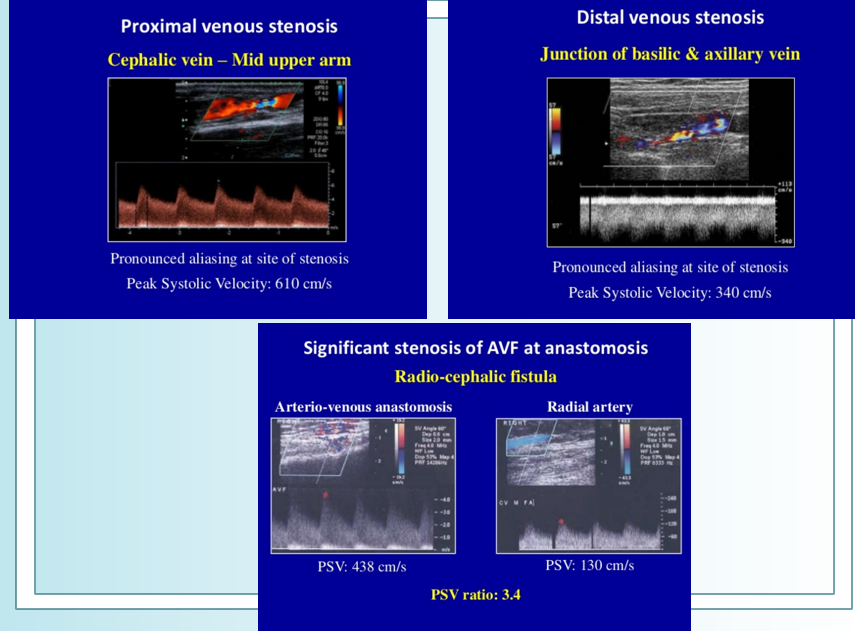
stenosis in AVF is present when
PSV ratio is >/= 2
>/= 50% diameter reduction
sample gate encompasses the entire vessel width
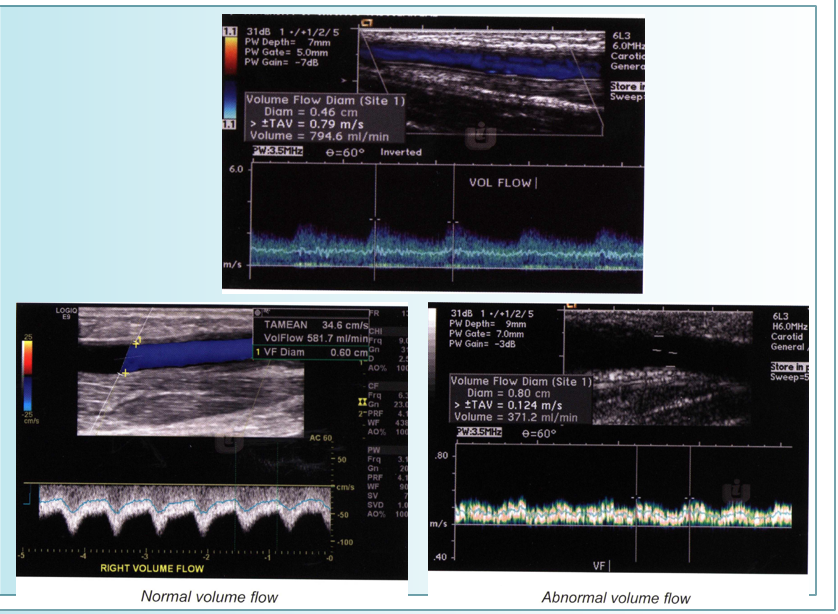
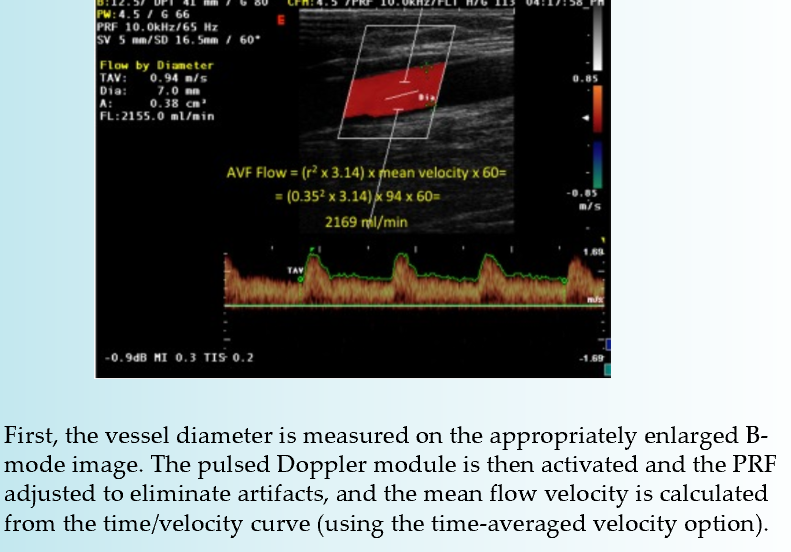
how do you obtain volume in AVF?
use straight, non tapering segment
activate time averae maximum
measure diameter of segment
at same location ^ open doppler gate - entire width of vessel
measure at least one cycle (PSV to PSV or EDV to EDV)
obtain volume
Qs what is an AV graft?
synthetic connection between artery and vein
looped plastic tube that essentially becomes an artificial vein
no need to develop (can be used 2 weeks after placement)
used when small veins do not mature into fistula
what are the indications for exam?
decreased bruit or thrill in access conduit
evaluate AVF maturity
pulsatile mass
pain
swelling
occlusion
edema
trauma
stenosis
collections/perigraft mass
low urea reduction rate less than 60%
access collapse → poor arterial inflow
infection
cold hands/fingers
what is the normal criteria for arteries and veins in AVF?
arterial
PSV 150-300cm/s
EDV 60-200 cm/s
venous
PSV 30-100 cm/s
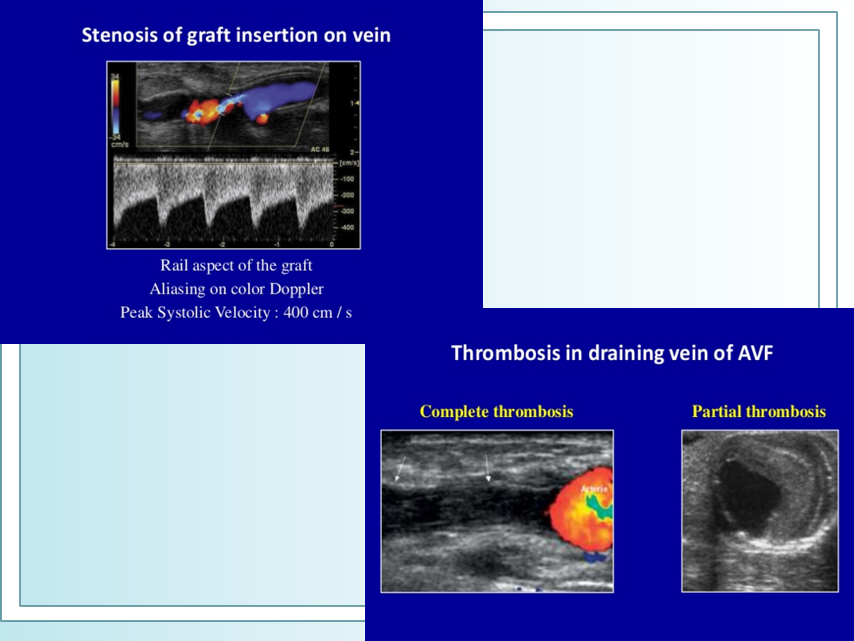
what is the most common cause of graft thrombosis?
stenosis at venous anastomosis
arterial anastomosis is uncommon
high grade stenoses produce velocity ratio
>2
what is the normal flow volume in AVG?
normal flow volume : >800ml/min
severe stenosis L : <500 ml/min
review
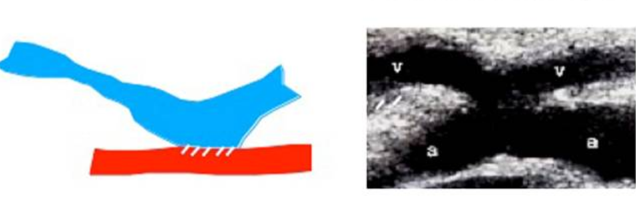
in AVF prox arterial flow has
greatly increased diastolic flow
in AVF distal arterial flow has
normal triphasic pattern
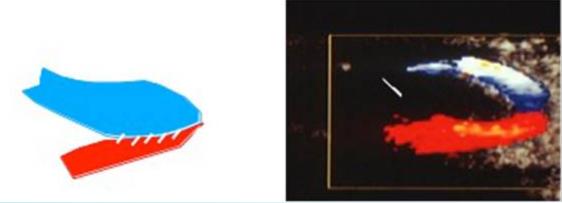
what is flow like through AVF?
turbulent
in AVF venous outflow has
pulsatile quality
review
Qs how many anastomoses does an AVF have?
1
Qs how many anastomoses does an AV graft have?
two
Qs what is normal diagnostic criteria of an AVF?
arterial velocity : 150-300
venous velocity : 30-100
Qs what is abnormal diagnostic criteria?
velocity ratio >2
focal velocity increase by 100% compared to more prox segment
indicates flow reducing stenosis
Qs what flow pattern does venous outflow usually take?
pulsatile
Qs what complications are associated with hemodialysis?
stenosis
thrombus
PSA
Qs what is most likely to lead to hemodialysis access failure?
stenosis
increase in venous pressure during dialysis indicates
outflow problems
high resistance pulsatile waveform within graft indicates
outflow stenosis
low resistance within graft indicates
arterial inflow problems