Mood disorders pt 2 (MOST IMPORTANT)
1/16
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
17 Terms
Manic episode DSM criteria
Elevated, expansive or irritable mood and increased goal-directed activity or energy
three or more of the following
Grandiosity
Decreased need for sleep
More talkative
Racing thoughts/ideas
distractibility
Increase in goal directed activity or psychomotor agiation
High involvement in high risk activities
Bipolar disorder 1
Usually major depressive episodes and always full manic episodes
Previously known as manic depression
Bipolar disorder 2
Usually major depressive episodes
Hypomanic episodes
Min 4 days
Less severe mania
There has never been a manic episode
More seasonal variation
Cyclothymic disorder
Chronic alteration of mood elevation and depression that does not meet severity of manic or major depressive episodes
At least 2 years
Rapid cycling disorder
Specifier of bipolar 1 and 2
At least 4 depressive/manic episodes in a year (any mix but can’t be one type)
Bipolar disorders: onset and duration
Bipolar 1: 18
Bipolar 2: 22
Both can begin in childhood
Very rare to develop after 40
Chronic and suicide is a common consequence of these disorders
Developmental influences of depressive and bipolar disorders
The elderly:
Symptoms of depression are skyrocketing in older people → caused by lack of integration into communities and lower birth rates (which means older people don’t get as much care)
Across cultures
Higher rates of depression in individualistic cultures
Among the creative
Bipolar disorders are more prevalent among creative people
Causes of mood disorders: bio
There is joint heritability of anxiety and depression (why they are quite comorbid)
Neurotransmitter systems
Cortisol, neurohormones
Sleep and circadian rythms
More intense REM sleep, reduction of deep sleep
Proband
the first individual identified in a study or family who has the condition being investigated. They are essentially the starting point for examining patterns of a disorder among groups/families.
Causes of mood disorders: Psychological dimensions
Stressful life events
learned helplessness
Lack of perceived control of their life
Depressive attributional style: internal, stable, and global
Negative cognitive styles
Negative cognitions about the Depressive cognitive triad: selves, immediate world, future
“I am worthless”, “the world is cruel”, “Things will never get better”
Causes of mood disorders: social and cultural dimensions
Marital dysfunction
Women have more disorders because:
Feelings of loss of control
Value of social relationships are higher (so if they go poorly they will be affected more)
Rumination
Poverty and abuse
Lack of social support
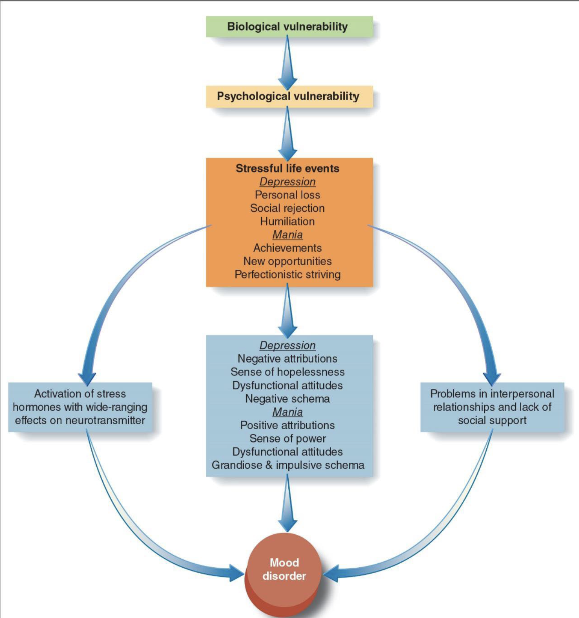
Causes of mood disorders: Integrative theory
Treatment for mood disorders pt 1
Medications:
Tricyclics, MAOI’s, SSRI’s (antidepressants)
Lithium - mood stabilizer
Electroconvulsive therapy
Transcranial magnetic stimulation:
Localized electromagnetic pulse
Treatment for mood disorder pt 2
Psychosocial treatments:
Cognitive therapy
Interpersonal therapy - combined treatments
Psychosocial + medication
Preventing relapse - mindfulness-based cognitive therapy
Suicide components
Suicidal ideation
Suicidal attempts
Parasuicides/None suicidal self injury
Suicide completion
Psychological autopsy
investigation into a deceased person’s mental state, behavioral patterns, and life stressors
Suicide risk factors
family history
Strong predictor
Neurobiology
Low serotonin
Psychological disorders
Estimated 90% of completed suicides; mood disorders, alcohol use disorder; borderline PD
Stressful life events
Suicide treatment
Problem-solving CB interventions
Coping-based interventions
Stress reduction techniques