EM Cardiology + EKG Practice
1/41
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
Tricuspid
What valve is most affected by infective endocarditis in IVDU?
Mitral
What valve is most affected by infective endocarditis?
Vancomycin + Ceftriaxone
What antibiotic combination should be given in infective endocarditis?
Infective endocarditis
A 42-year-old man with a history of intravenous heroin use presents to the emergency department with fever, fatigue, and shortness of breath for 1 week. His temperature is 101.8°F, blood pressure is 108/64 mm Hg, and heart rate is 112 bpm. Physical examination reveals a new holosystolic murmur best heard at the left lower sternal border and multiple painless erythematous lesions on the palms. Laboratory studies show leukocytosis. Blood cultures grow gram-positive cocci in clusters. What is the most likely diagnosis?
Dilated Cardiomyopathy
Dilation and impaired contraction of the LV or both ventricles, most often idiopathic
-Sx: exertional dyspnea, fatigue, peripheral edema, pulmonary congestion, cough, hepatomegaly, S3 gallop
-ECHO: LV dilation, thin ventricular walls, decreased LVEF, and ventricular hypokinesis
-Tx: ACE, BB, diuretic
Dilated cardiomyopathy
A 54-year-old man with a history of chronic alcohol use presents to the clinic with progressive fatigue, dyspnea on exertion, and bilateral lower extremity swelling for the past 3 months. Vital signs reveal blood pressure of 102/68 mm Hg and heart rate of 108 bpm. Physical examination shows jugular venous distention, bibasilar crackles, and 2+ pitting edema of the legs. Cardiac auscultation reveals an S3 gallop. Echocardiogram demonstrates four-chamber enlargement with reduced ejection fraction. What is the most likely diagnosis?
Hypertrophic Cardiomyopathy
Autosomal dominant genetic disorder of inappropriate LVH or RVH with diastolic dysfunction, which worsens with increased contractility and decreased LV volume
-Sx: dyspnea, fatigue, angina, syncope, dizziness, arrhythmia, sudden cardiac death, harsh systolic murmur heard at LLSB that increases with Valsalva and standing
-ECHO: asymmetric ventricular wall thickness, systolic anterior motion of the mitral valve
-Tx: beta blockers
Hypertrophic cardiomyopathy
A 19-year-old man collapses during basketball practice after experiencing sudden lightheadedness and chest pain. His father died suddenly at age 35. Vital signs are stable. Cardiac examination reveals a harsh systolic murmur best heard along the left sternal border that increases with Valsalva maneuver and decreases with squatting. ECG shows left ventricular hypertrophy. What is the most likely diagnosis?
Restrictive Cardiomyopathy
Diastolic dysfunction in a non-dilated ventricle, which impedes ventricular filling
-Sx: peripheral edema, JVD, hepatomegaly, ascites, dyspnea, fatigue, Kussmaul’s sign (increased JVP with inspiration)
-ECHO: non-dilated ventricles with normal thickness, diastolic dysfunction, marked dilation of both atria
Restrictive Cardiomyopathy
A 68 y/o woman with a history of amyloidosis presents with progressive fatigue, dyspnea on exertion, and lower extremity edema. Physical examination reveals jugular venous distention, hepatomegaly, and bilateral pitting edema. Lungs are CTA. Echocardiogram shows normal ventricular size and preserved ejection fraction with impaired ventricular filling and biatrial enlargement. What is the most likely diagnosis?
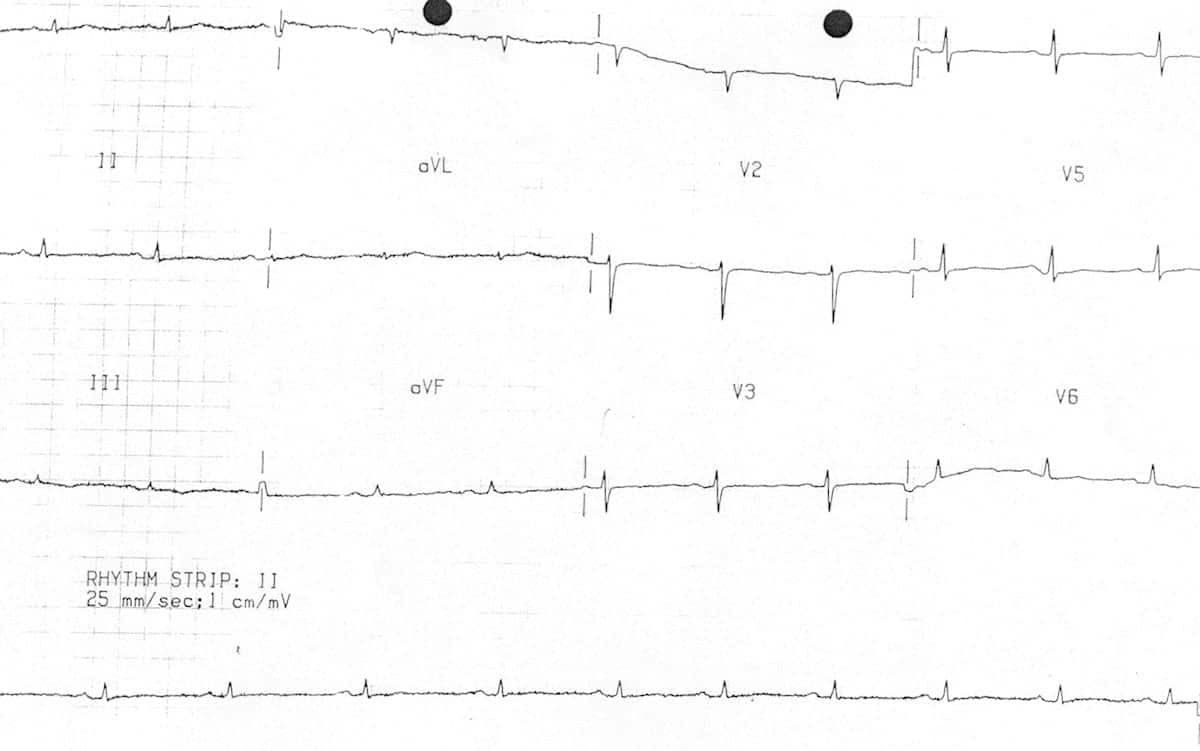
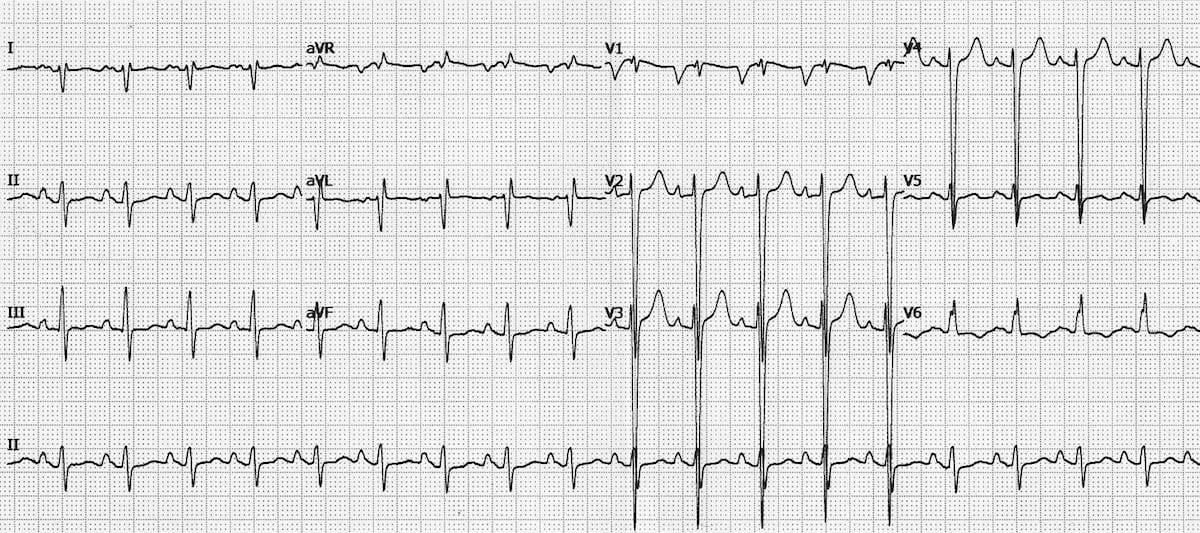
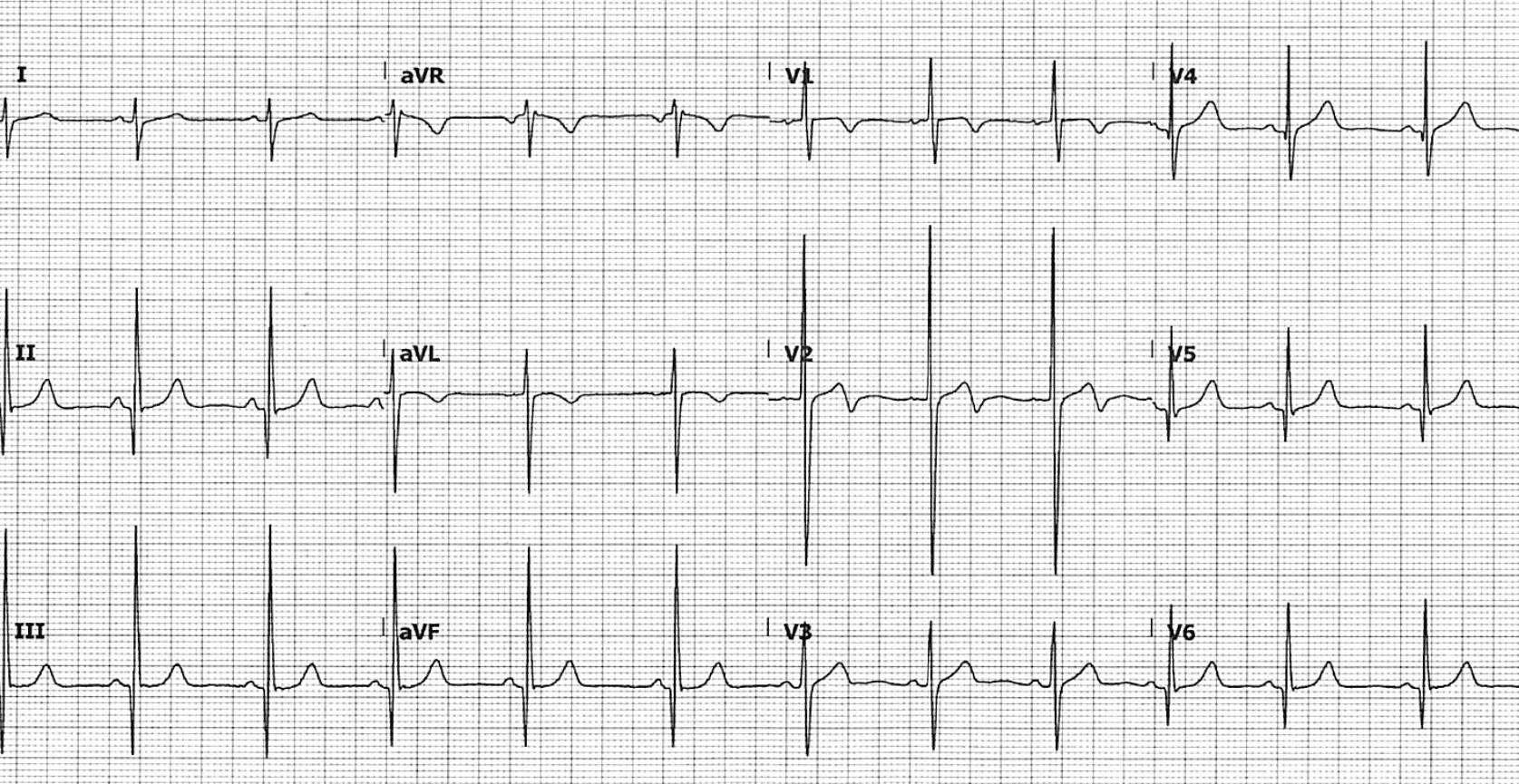
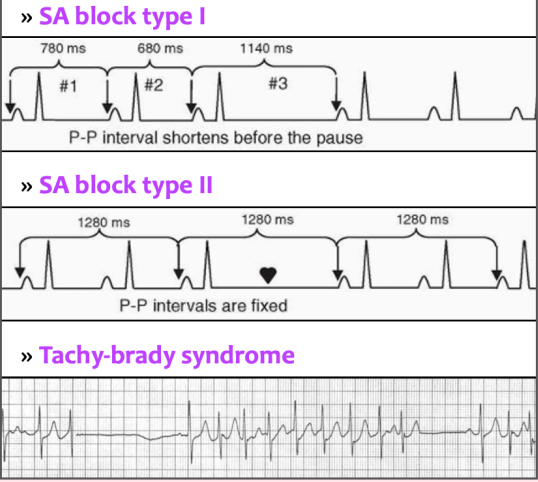
Sick Sinus Syndrome
Abnormality in SA node action potential generation or conduction, causing inappropriate sinus bradycardia, alternating bradycardia and tachycardia, sinus pause, SA nodal block, or chronotropic incompetence
-Sx: exercise intolerance, fatigue, dizziness, HA, nausea, palpitations, CP, SOB, syncope
-Tx: atropine, percutaneous pacing
First degree, Mobitz 1
Which two AV blocks occur in the AV node?
Mobitz 2, third degree
Which two AV blocks occur below the AV node?
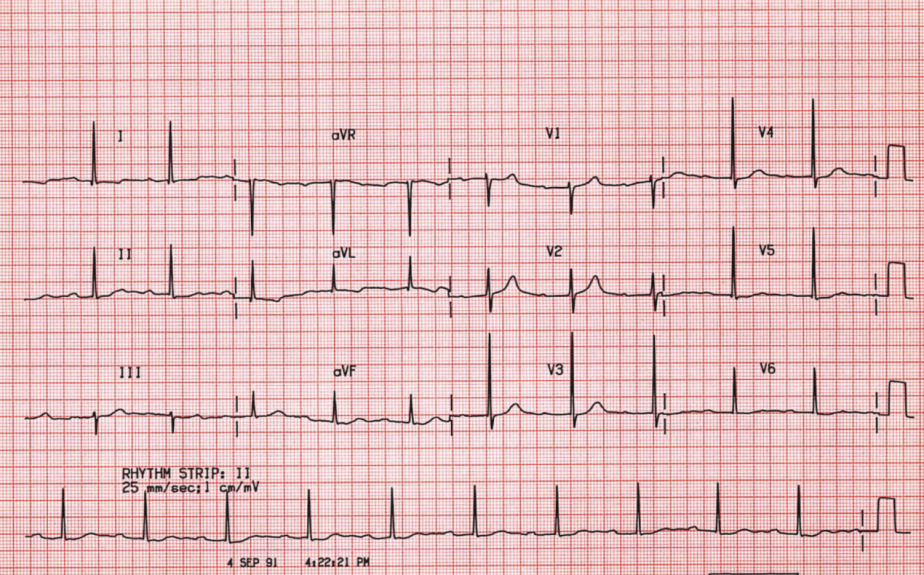
First degree AV block
What does this EKG show?
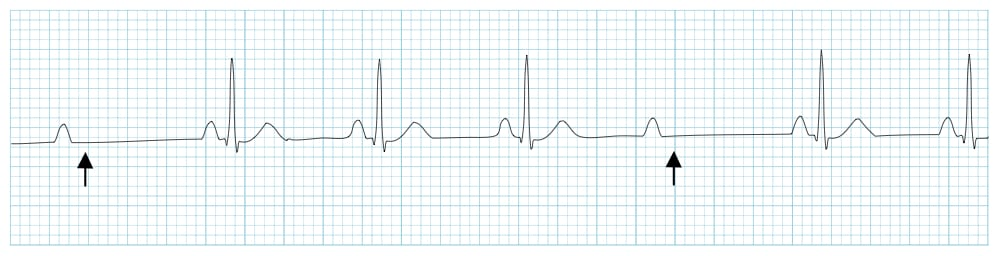
Mobitz I
What does this EKG show?
Mobitz 2
What does this EKG show?
Complete AV block
What does this EKG show?
Pacemaker
What is the treatment of choice for a Mobitz II or third degree AV block?
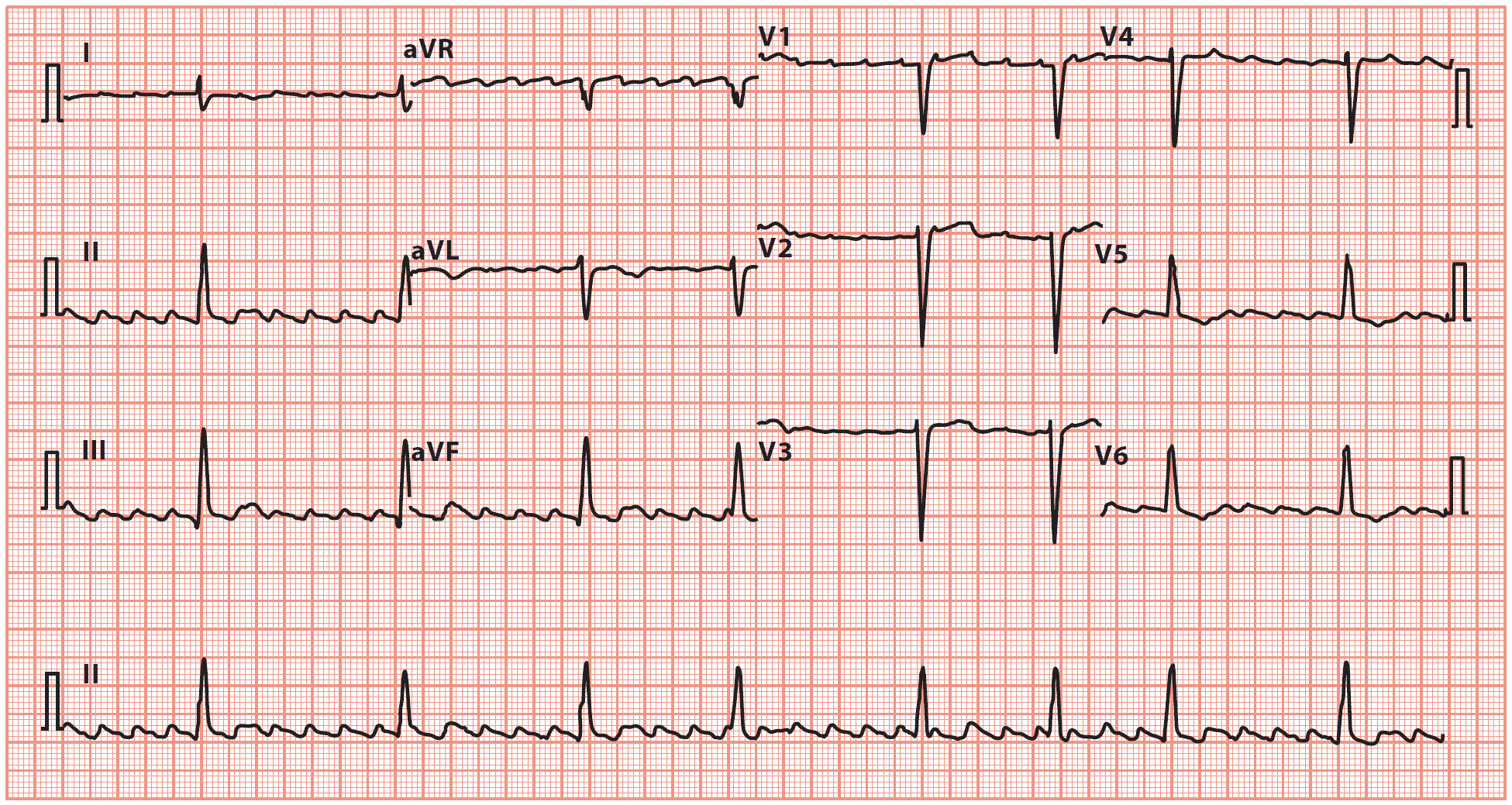
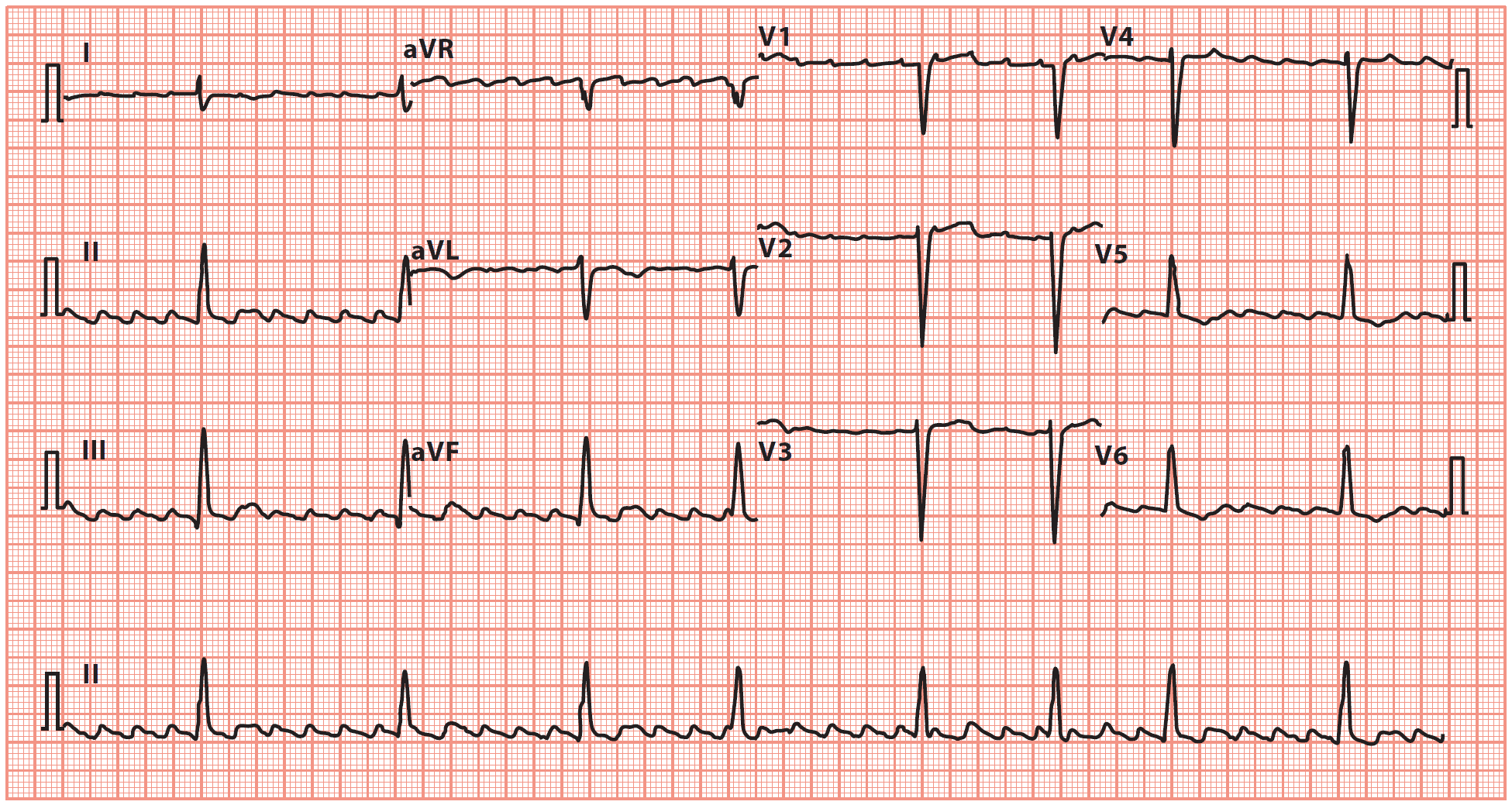
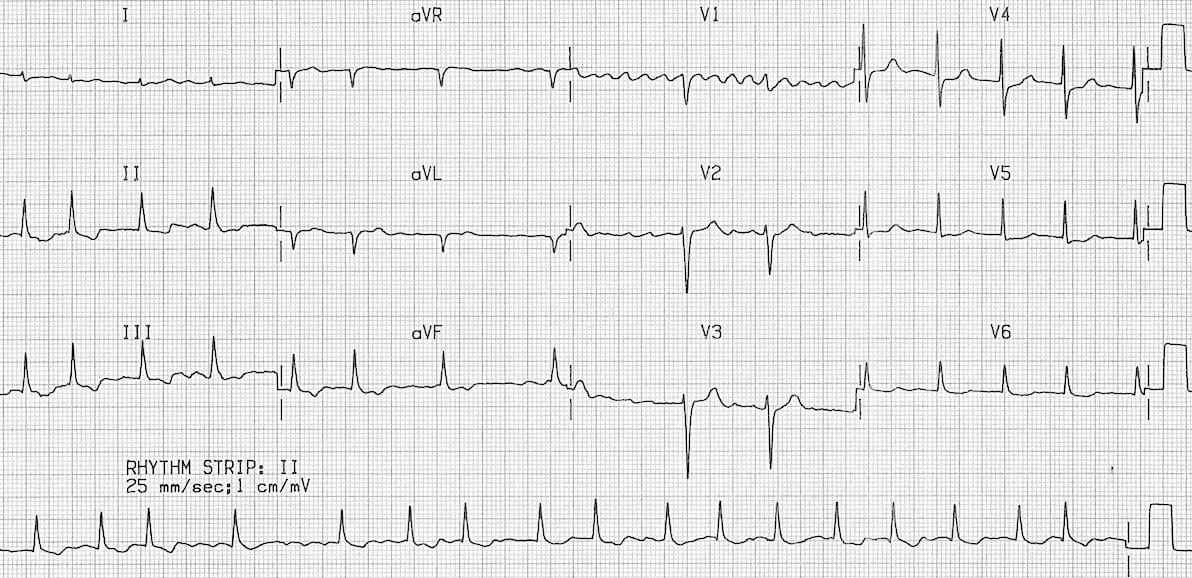
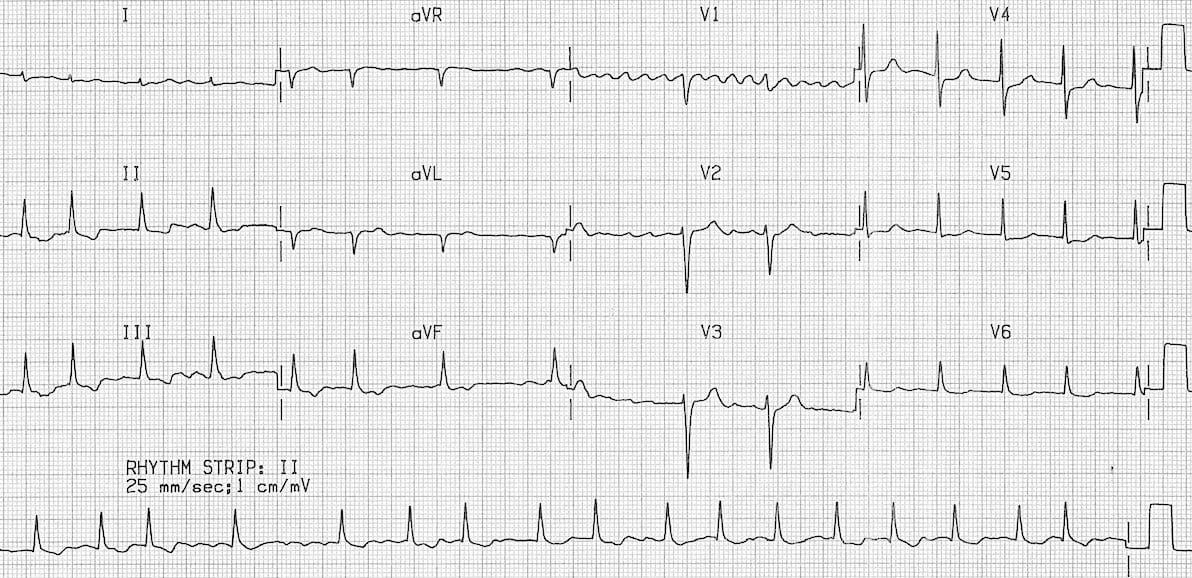
Right Bundle Branch Block
Delay in depolarization of RV, which can occur in a healthy heart
-See terminal R wave in V1/V2 with discordant ST/T waves, broad S waves in V5/V6
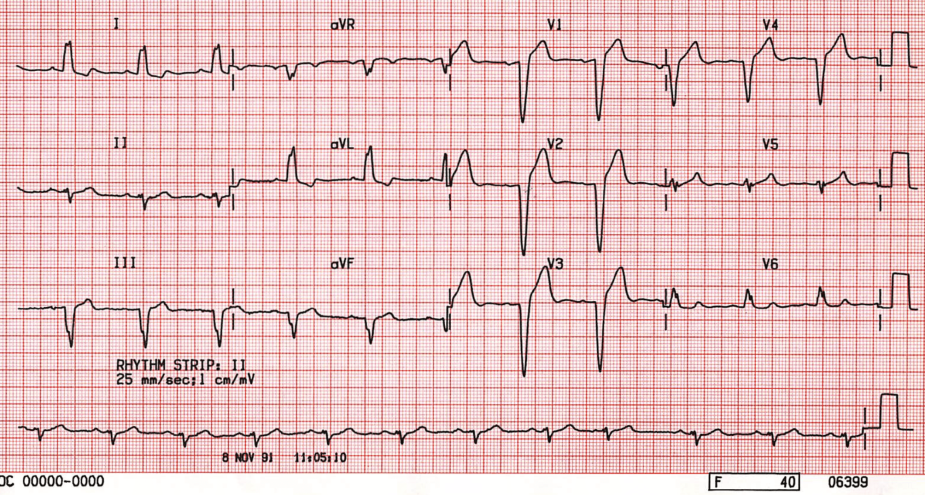
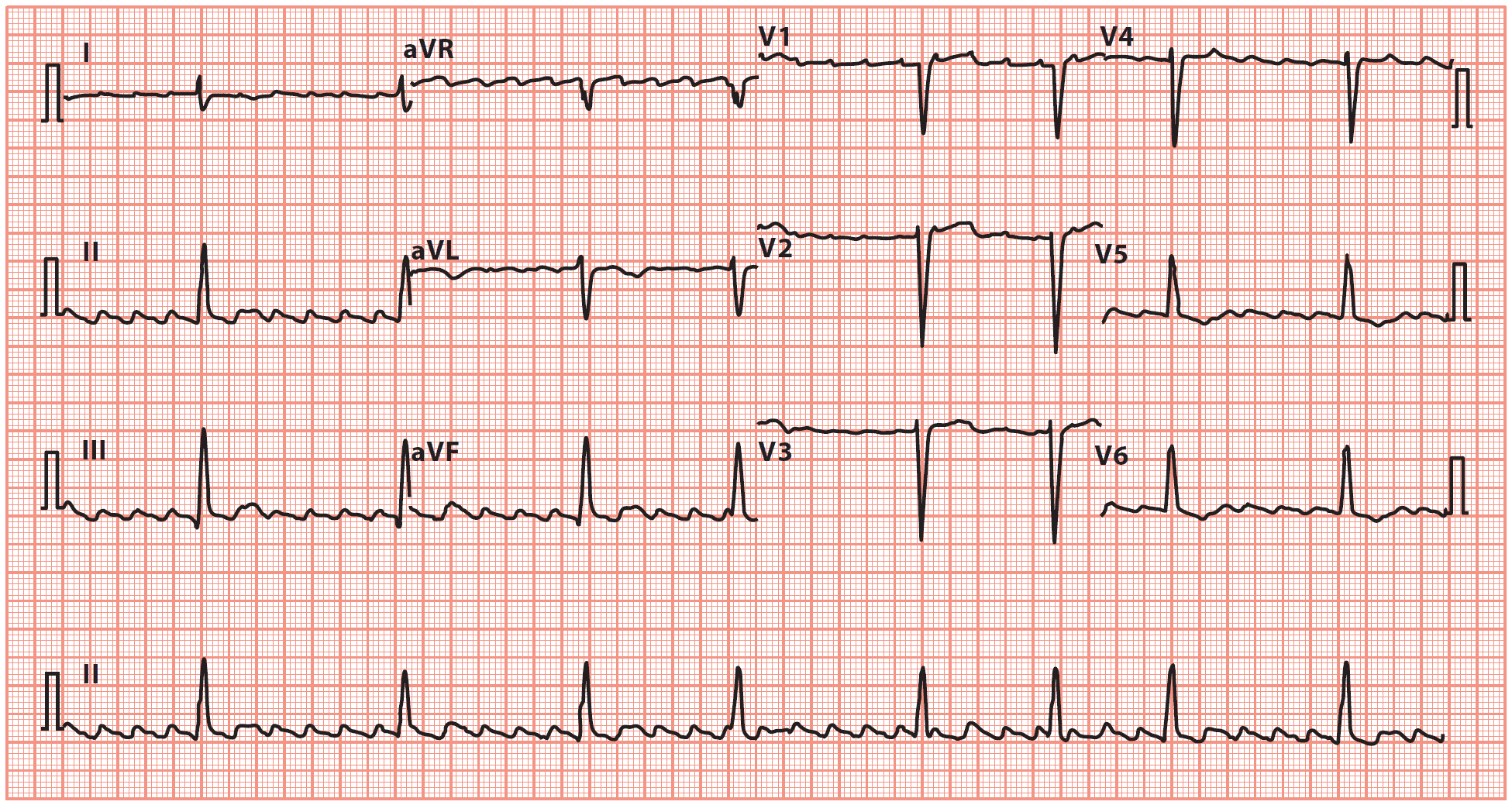
Left Bundle Branch Block
Delay in depolarization of LV; entire sequence of ventricular activation is altered, affecting both the initial septal and subsequent ventricular forces. Does NOT occur in a healthy heart
-Broad, notched, or slurred R waves in leads I, aVL, V5/V6, and dominant S wave in lead 1
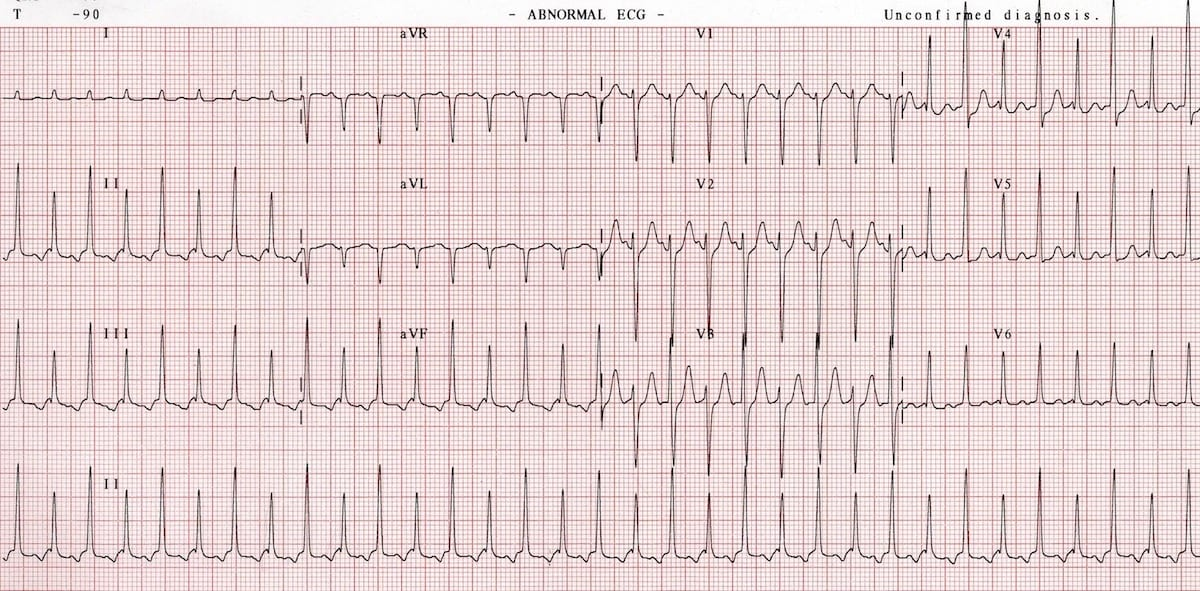
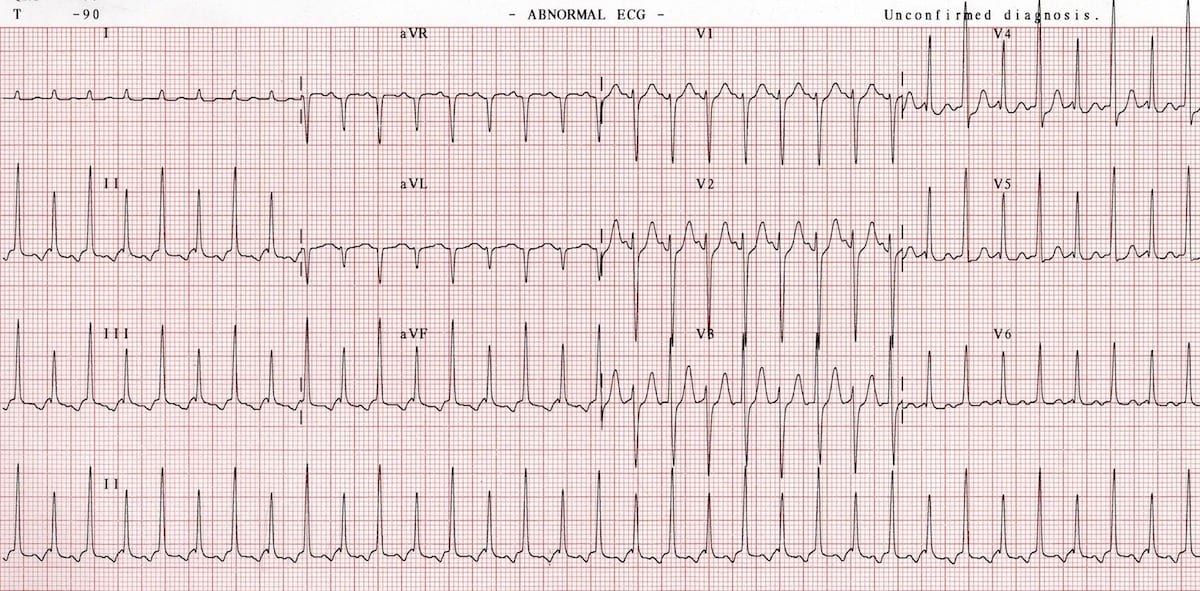
Atrial Flutter
Isthmus dependent, single reentrant circuit around tricuspid annulus (R atrium)
-Sx: palpitations, fatigue, dyspnea, presyncope, sx of HF
-EKG: atrial rate ~300 bpm, ventricular ~150bpm. See the waves in a sawtooth pattern
-Definitive treatment is radiofrequency ablation
Cardioversion
In an unstable patient with this EKG, what is the treatment of choice?
Flecainide
In a stable patient with this EKG, what is the treatment of choice?
Atrial Fibrillation
MC arrhythmia in the general population, with a prevalence that increases with age
-Sx: palpitations, fatigue, dyspnea, dizziness, diaphoresis, HF sx
-EKG: irregularly irregular rhythm. Absence of discrete P waves
Rate control
In a stable patient with this EKG, what should be done?
CHADS-VASC
What scoring system determines the risk of stroke in a patient with A. Fib>
-Congestive heart failure
-Hypertension
-Age >75
-Diabetes
-Stroke history
-Vascular disease
-Age 65074
-Sex female
VTach
What arrhythmia is a patient with >3 PVCs at a high likelihood of going into?
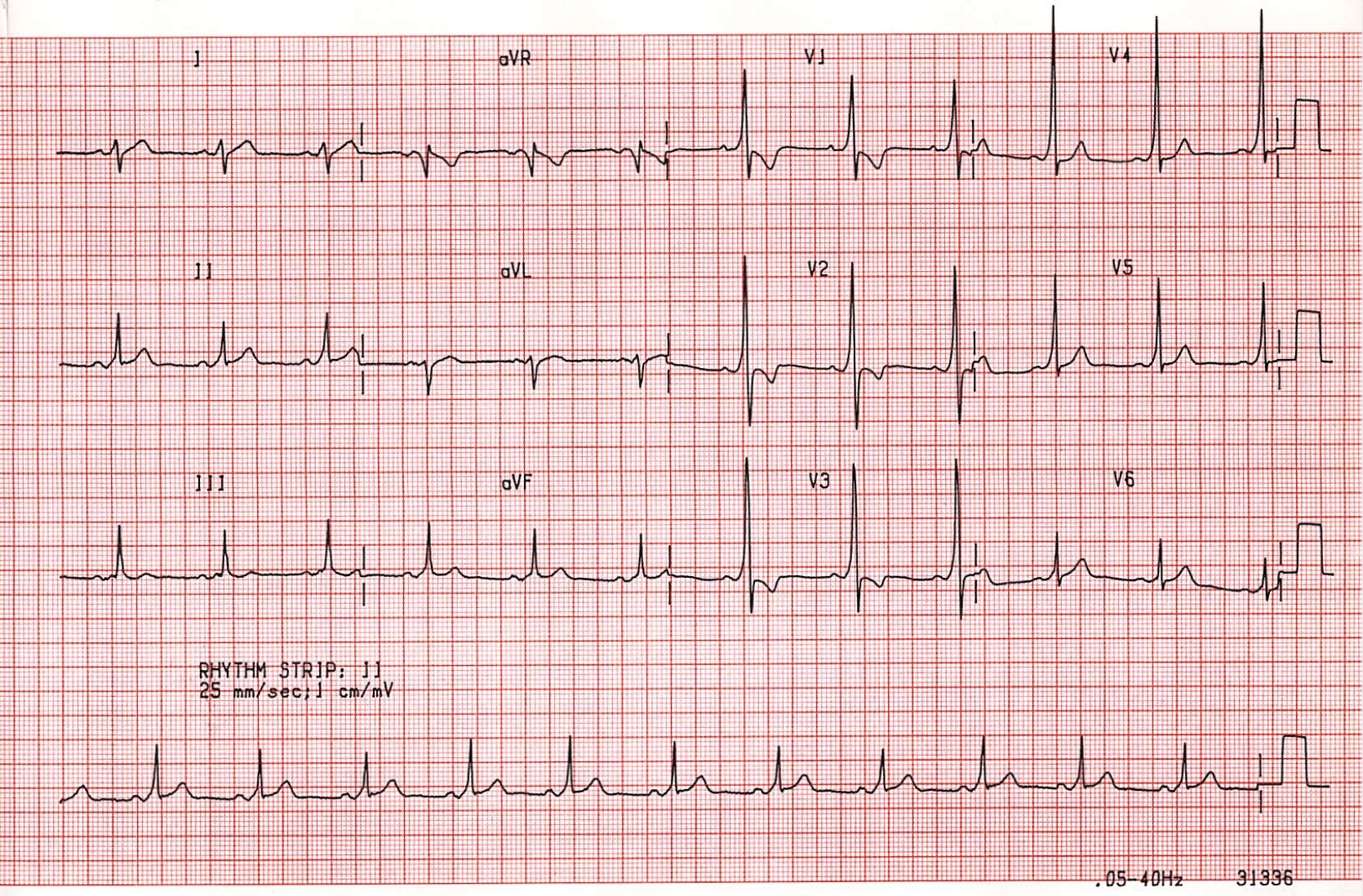
SVT
What does this EKG show?
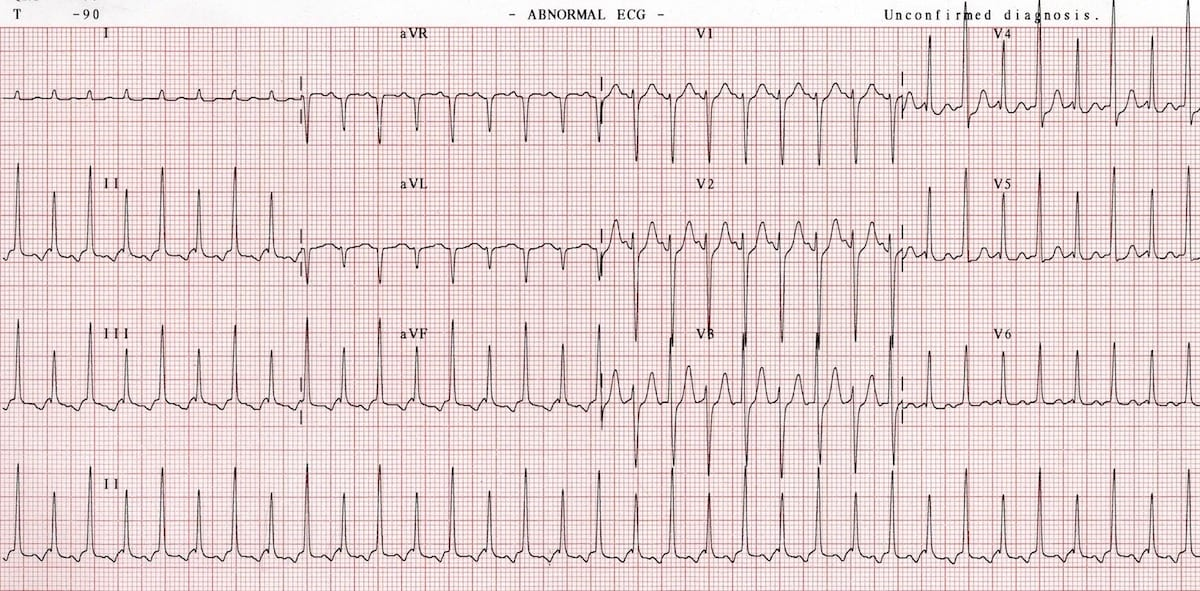
Vagal maneuvers
What is the first line treatment for a patient with this EKG?A
Adenosine
If vagal maneuvers fail in this patient, what can be tried next?
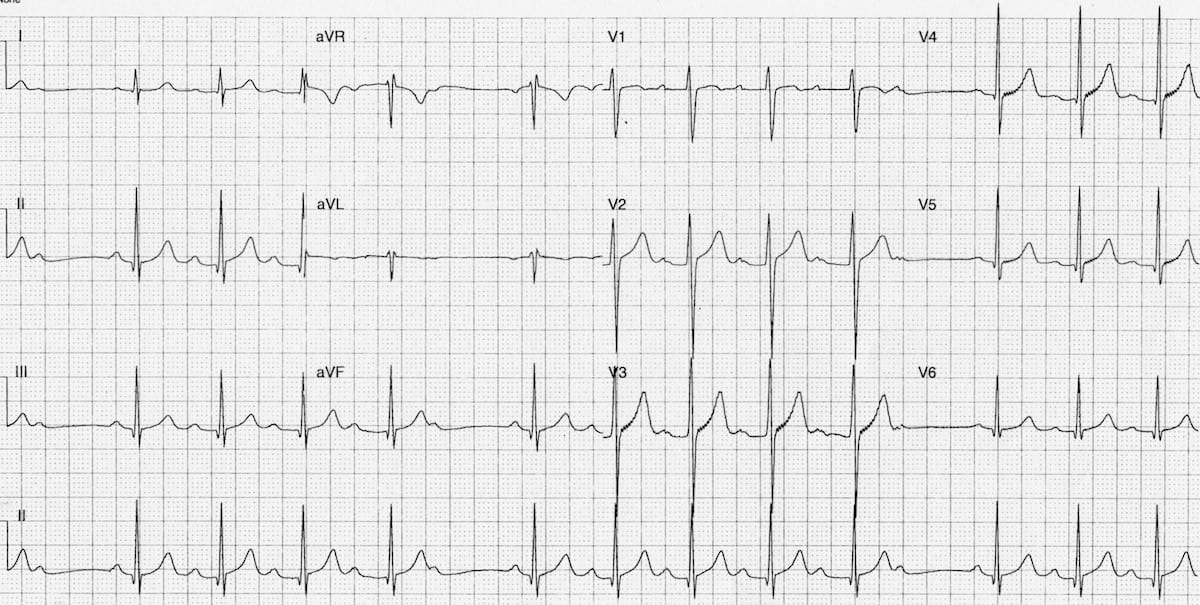
WPW
Congenital accessory pathway (Bundle of Kent) with associated SVT
-Sx: palpitations, dizziness, mild chest pain
-EKG shows delta wave, short PR interval, and wide QRS
-Procainamide if stable
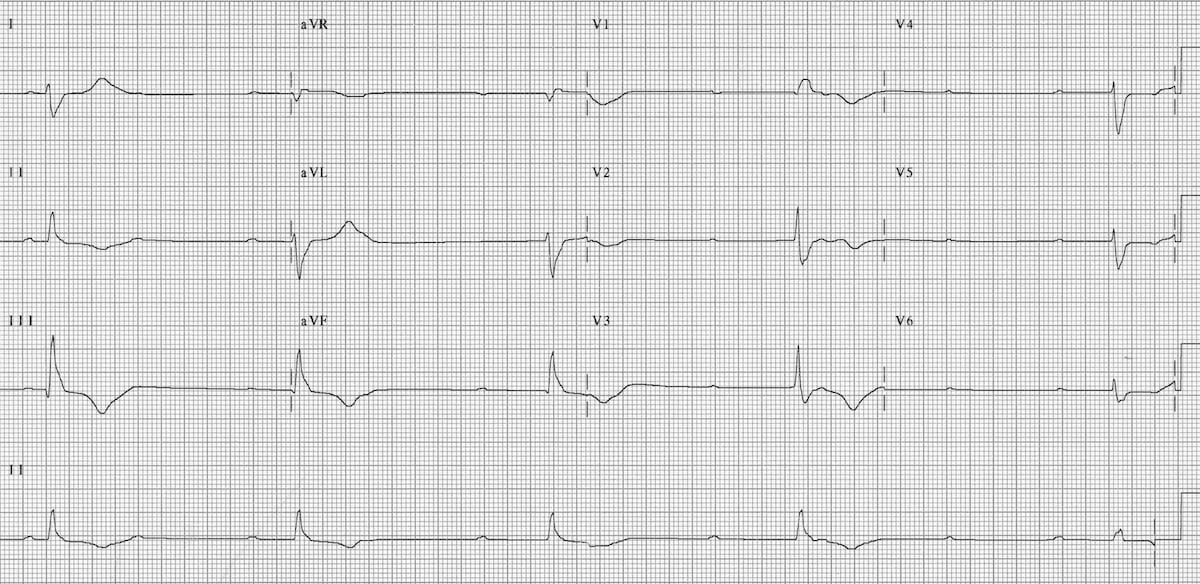
COPD
What condition is associated with this EKG finding?
-Give verapamil

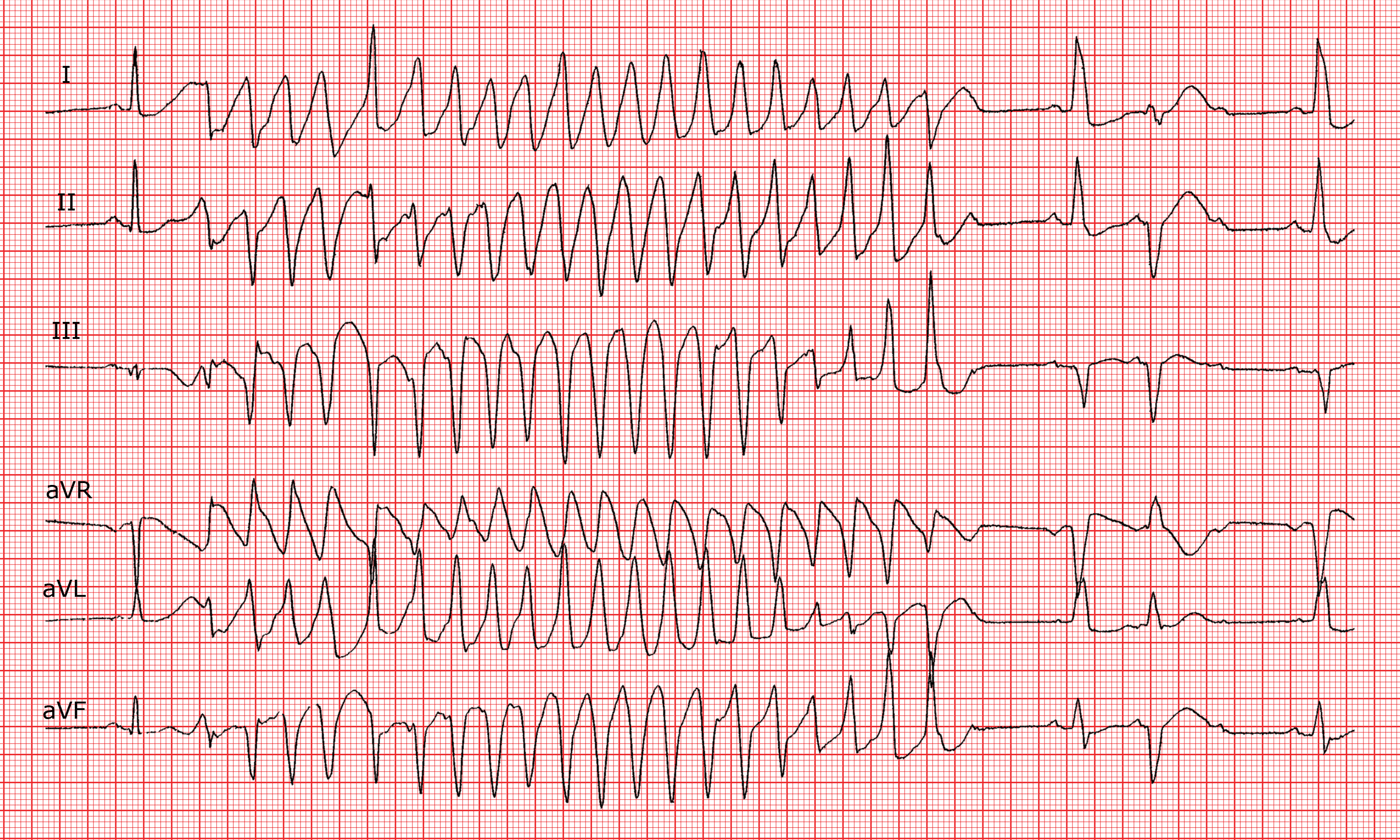
Monomorphic VTach
Regular, broad complex tachycardia with uniform QRS complexes
-Usually associated with a myocardial scar
-Sx: CP, dyspnea, syncope, SCD

Amiodarone
What is the first line pharmacological treatment for stable VT?

Cardioversion
In an unstable patient with this EKG, what is the treatment of choice?

Magnesium
What should be pushed in this patient?

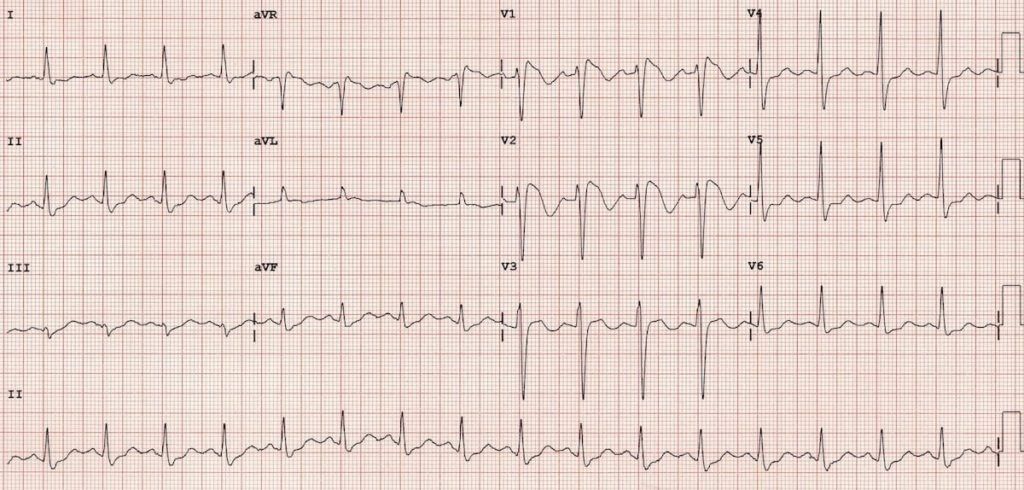
Brugada
Hereditary, characterized by structurally normal heart and associated with ventricular dysrhythmias
-Due to mutation in cardiac Na gene channel, predominantly in Asian men

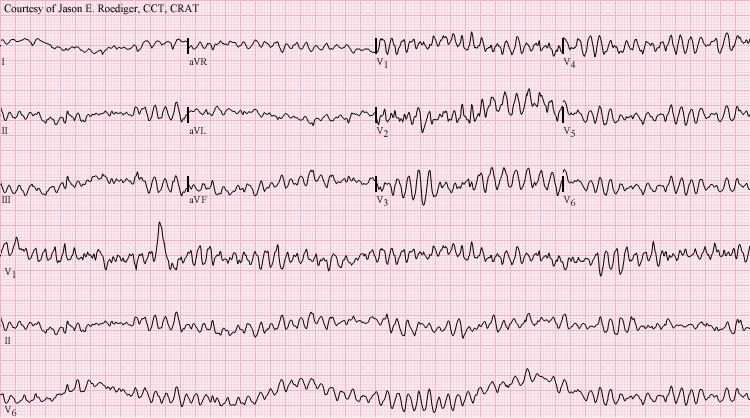
Torsades
Paroxysmal form of polymorphic VT, occurring secondary to QT prolongation
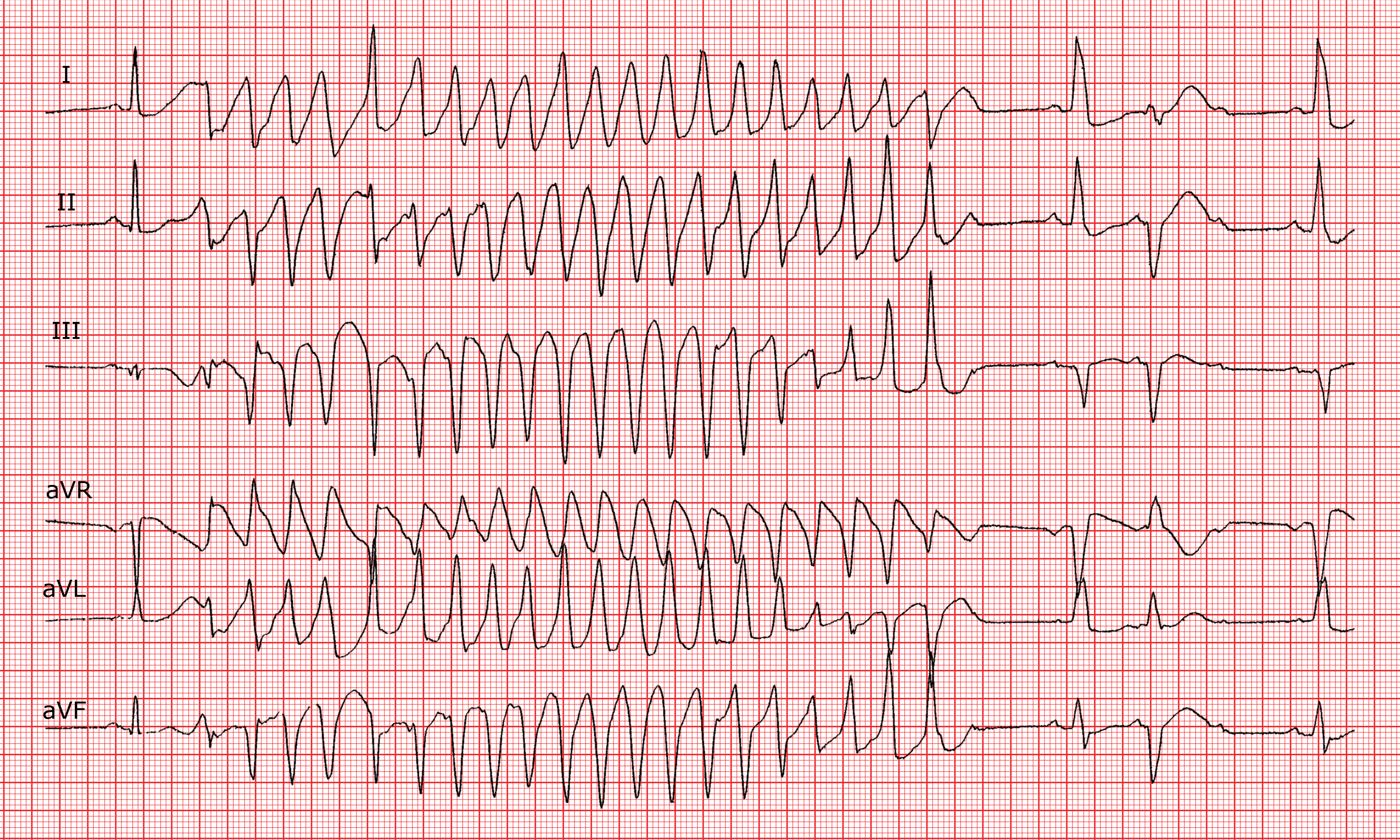
Magnesium
In a patient with this EKG, what medication should be given?
ACLS
What should be done for a patient with this EKG?
Aspirin
What decreases mortality in patients with CAD?
CCBs
What class of drug should be given to patients with prinzmetal angina to prevent vasoconstriction and promote vasodilation in coronary vasculature?
-Avoid BBs