GIT, liver +mental health
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Severe complications of HG
malnutrition
affects fetal growth (IUGR)
Renal impairment
Dehydration
electrolyte imbalance
weight loss
ketosis
Negatively affect Mental health
Loss of work
Ketosis
Sign that mother and fetus are not getting enough energy fuel in their diet
ketones are metabolic end products of fatty acid metabolism
Body using fat for fuel instead of glucose
may affect babies developing brain cells
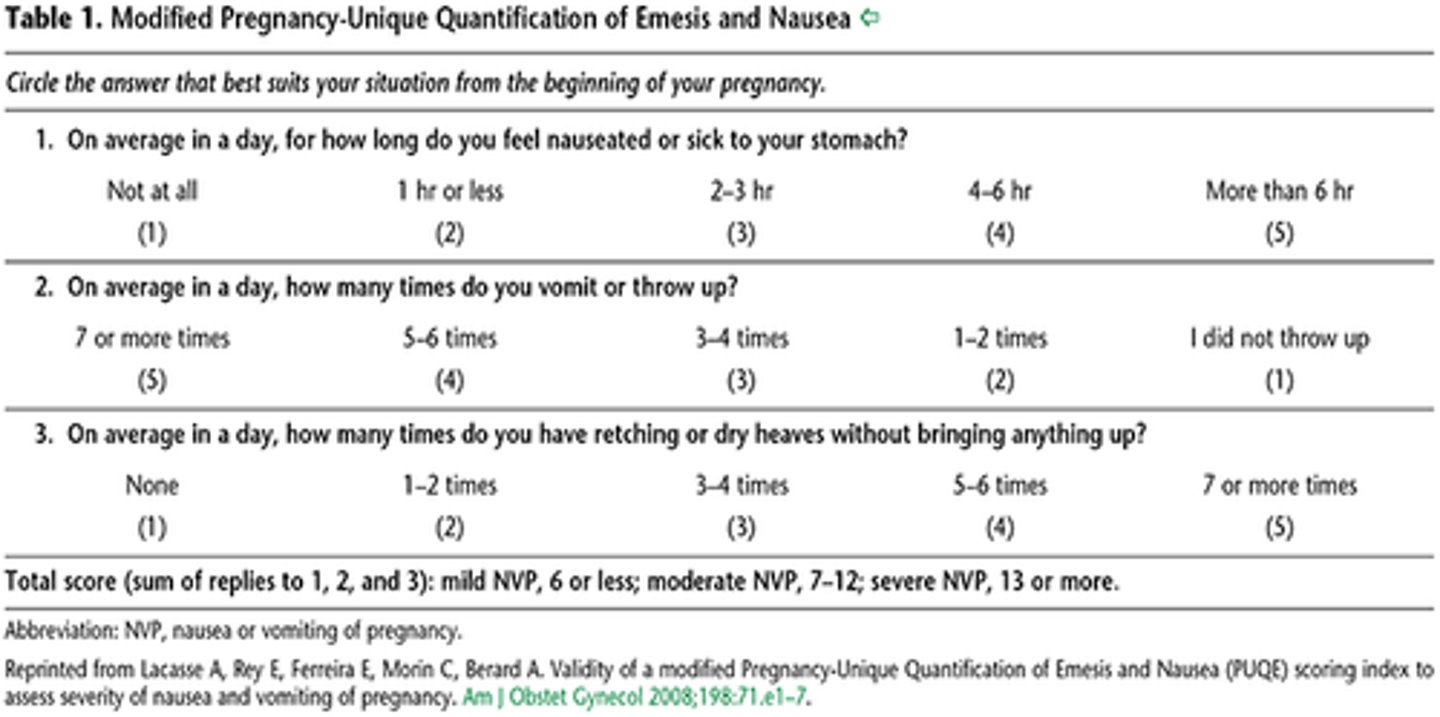
How to assess the severity of HG
Pregnancy-unique quantification of emesis and nausea (PUQE)
Non-Pharmacological Treatment for NVP
Reassurance and empathy
Vitamin B
Ginger
Small and frequent snacks
Address fatigue
Discontinue prenatal vitamins with iron
Pharmacological Treatment for NVP
Try to avoid until 14 weeks
Doxylamine
Promethazine
Prochloroperazine
Metoclopramide
Ondansteron
GERD (gastroesophageal reflux disease)
stomach acid or bile irritates the food pipe lining
very common especially later in gestation
Treatment for GERD
-Lifestyle changes → small frequent meals, eat upright, eat slowly, avoid spicy/v acidic foods
Antacids
-Acid lowering drugs → H2 blockers, PPI, antacids
Further investigations
IBS (irritable bowel syndrome)
Abdominal pain or discomfort
altered bowel habits and bloating or distention
IBS and pregnancy
can cause increased constipation, heartburn, nausea and stool frequency
Changes in ovarian hormones and physical pressure of growing fetus on bowel wall may contribute to GI symptoms
IBD (inflammatory bowel disease)
severe inflammation of the intestinal tract
Crohns disease
Ulcerative colitis
Crohn's disease
a chronic autoimmune disorder that can occur anywhere in the digestive tract; however, it is most often found in the ileum and in the colon
Affects all layers of the bowel
ulcerative colitis
chronic inflammation of the colorectal mucosa, with ulcerations
IBD in pregnancy
- Can improve symptoms due to inhibition of inflammation, but can be exacerbated during pregnancy
- should stay on meds
- can affect the development of a baby's GIT leading to mild intestinal inflammation
- main concern is malnutrition, inadequate weight gain and IUGR
- Women with active disease or who have had colon surgery normally have C/S due to risk a vaginal delivery can result in an anal sphincter injury
Anal incontinence
Indirect and direct trauma following vaginal birth can negatively impact the pelvic floor function increasing risk of AI
Liver function
-Production of bile, certain blood plasma proteins, cholesterol
-Storage of excess glucose in the form of glycogen
-*detoxification and degradation of body wastes and hormones
break down RBC
-Controlling infections by boosting immune factors and removing bacteria.
liver anatomy
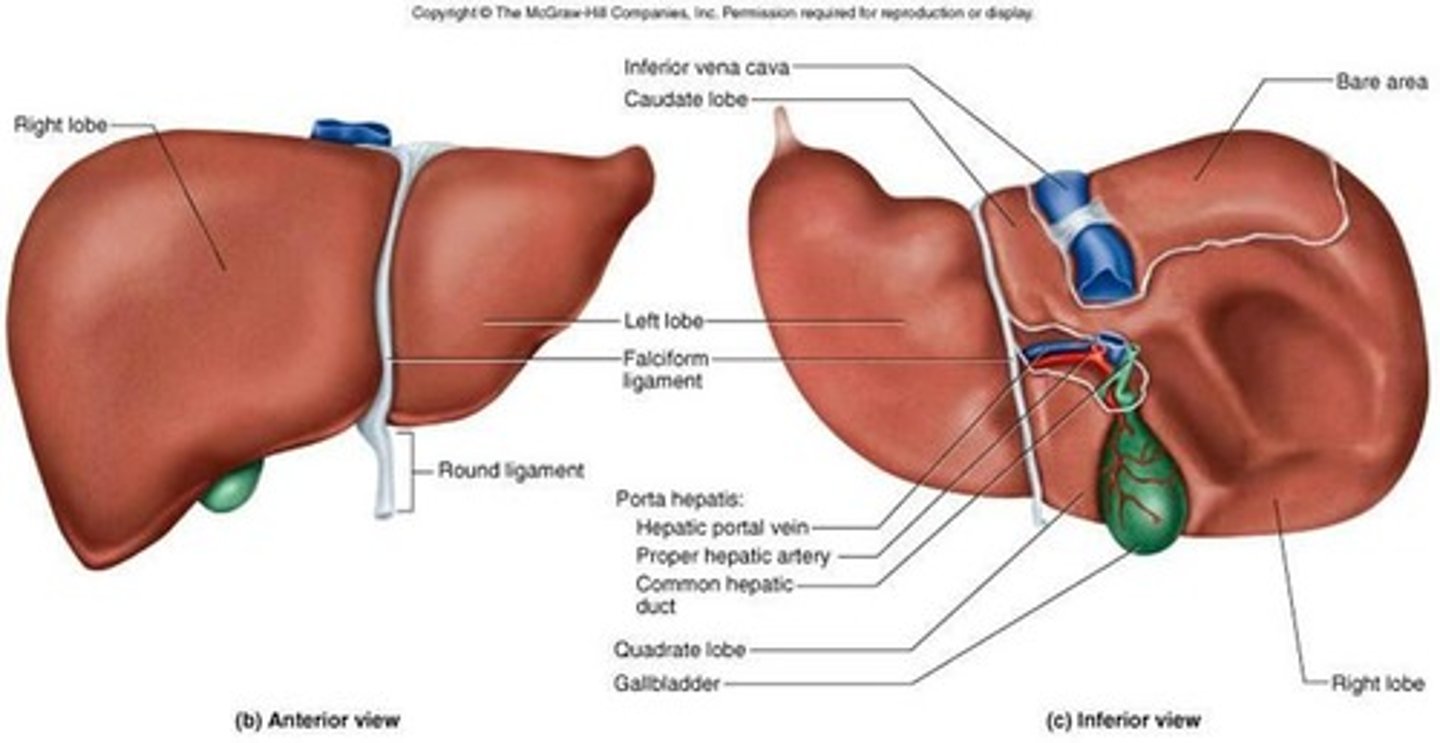
Portal vein
Responsible for directing blood from parts of the GI tract to the liver. Absorbed nutrients are then absorbed, stored or detoxified
Intrahepatic cholestasis of pregnancy
A condition where bile cannot flow from the liver to the duodenum
Most common liver disease in pregnancy
T3 with pruritis and high Bile acid levels
Types of ICP
Obstructive where there is a mechanical blockage in the duct system that can occur from a gallstone or malignancy
Metabolic: disturbances in bile formation that can occur because of genetic defects (transporters) or acquired as a side effect of medications
risk factors for ICP
HCV-positive pregnant woman
Seasonal onset (winter)
Low selenium levels
Low vitamin D
Multiple gestations
Advanced age >35years
Genetic defects in canalicular transporters
Treatment for ICP
Ursodeoxycholic acid (UDCA)
Provides cytoprotection against the hepatotoxic effects of the hydrophobic bile acids and improves hepatobiliary bile acid transport
ICP and birth outcomes
associated with increased rates of preterm birth, meconium-stained amniotic fluid, fetal hypoxia, prolonged admission to the neonatal unit, and stillbirth
HELLP syndrome
hemolysis, elevated liver enzymes, low platelets
Develops in women with severe pre-eclampsia
Placental dysfunction causing Abnormal oxidation of fatty acids by the fetus and release of metabolic intermediates into the mother's circulation cause liver and vascular dysfunction
HELLP syndrome symptoms
nausea, vomiting, viral like illness, epigastric pain, headache, weight gain
HELLP syndrome management
hospitalization
lower BP
prevent with mag sulfate
correct coagulopathies
blood or FFP to treat hemolytic anemia
steroids for fetal lungs
prepare for preterm delivery
Acute fatty liver of pregnancy
abnormal accumulation of triglycerides
Changes to GIT with pregnancy
Propulsion, digestion and elimination slow down due to the effected of hormones on smooth muscles (Relaxing them)
Lower Oesophageal sphincter tone is also reduced
The uterus compresses teh duodenum and stomach
More susceptible to nausea, vomiting, reflux, constipation and diarrhoea
Hyperemesis Gravidarum (HG)
extreme nausea and vomiting during pregnancy 1.2% affected
Nausea and vomiting in pregnancy
Begins at 4 weeks, peaks at 9 and gone by 20
70% affected