ORTHOPEDIE
1/251
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
252 Terms
SCHOUDER
Wat is er speciaal aan het coraco-acromion ligament?
Vestigial structuur (verbindt structureren beide behorend tot de scapula)
= dak van de schouder
SCHOUDER
Wat is het n suprascapularis entrapment syndroom?
N suprascapularis ligt onder lig. transversum scapulae, in incisura scapulae.
E: Bij bovenhandssporten, zware atrofie van infra- of supraspinatus
P: inklemming (erboven ligt AV suprascapularis)
R: ligament doorknippen
SCHOUDER
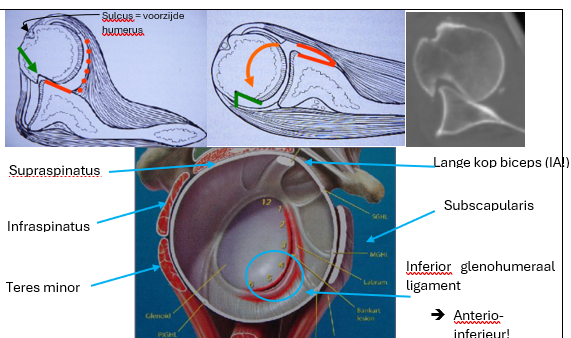
Benoem de rotatorcuff spieren
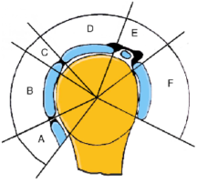
A: M teres minor
B: M infraspinatus
C: X
D: M supraspinatus
E: rotator interval/biceps
F: M subscapularispees
SCHOUDER
Hoe evalueer je exorotatie klinisch?
Hoe evalueer je endorotatie klinisch?
Wat is de gemiddelde hand-rug hoogte?
Hand-nek
Hand-rug
T12
SCHOUDER
Welke structuren zorgen voor gewrichtsstabiliteit?
Congruentie (kom glenoïd, kraakbeen, labrum)
Ligamenten
Spieren (negatieve IA druk tgv RC-spieren)
SCHOUDER
Wat is scapulohumeraal ritme?
Samenwerking tussen scapula en humerus tijdens beweging → abductie tot 60° (daarna tov ribbenrooster)
SCHOUDER
AC-luxatie
Typische anamnese
Kliniek
Diagnose
Zware laterale val (/handen te plaatsen) → overbelasting AC-ligament
Drukpijn
Pianotoets (pathognomisch)
RX
SCHOUDER
AC-luxatie
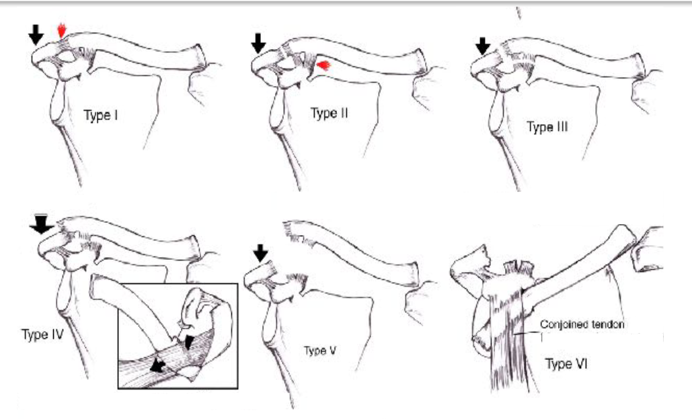
Leg de classificatie van Rockwood uit voor acromioclaviculaire luxaties.
TYPE I → STABIEL
AC-ligament: sprain
CC-ligament: intact
TYPE II → MIN. DISLOCATIE
AC-ligament: ruptuur
CC-ligament: intact
TYPE III → DISLOCATIE CLAVICULA
AC-ligament: ruptuur
CC-ligament: ruptuur
TYPE IV → POSTERIEURE DISLOCATIE
AC-ligament en CC-ligament ruptuur
High-velocity trauma + posterieure dislocatie dmv trapezius
TYPE V → FLOATING CLAVICULA
AC-ligament en CC-ligament ruptuur
Verdere anterieure verplaarsing
TYPE VI
Luxatie onder conjoined tendon (coracobrachialis + korte kop biceps)
onder proc. coracoideus
SCHOUDER
AC-luxatie
Therapie (~ Roclwood classificatie)
TYPE I-II: conservatief
rust
pijnstilling
draagdoek
TYPE III: ± geval
TYPE IV-VI: chirurgie
plaat- en schroeffixatie → cave: impingement, na 6 weken verwijderen ikv bewegingsbeperking
synthetische draad tussen clavicula en coracoid
SCHOUDER
Clavicula#
Typische anamnese?
Kliniek?
Diagnose?
Laterale impact zonder handen plaatsen (~AC-luxatie)
Pijn
Misvorming
Crepitatie
RX
SCHOUDER
Clavicula#
Therapie?
Conservatief:
Niet-verplaatse fracturen
cijfer 8 verband gedurende 2 weken
Chirurgie:
>2 cm verschuiving, huid-schade, open, sporters, falende conservatief
sneller terug schouder gebruik, maar risico op infectie, complicatie, esthetisch, …
SCHOUDER
Clavicula#
Prognose?
Gunstig, callus verdwijnt na tijd, functioneel herstel ad integrum
SCHOUDER
Anterieure schouderluxatie
Typisch mechanisme?
Abductie + exorotatie
SCHOUDER
Anterieure luxatie
Welke complicaties
Bankart-letsel: scheur (+ avulsie) anterieur labrum
Hillsachs-letsel: compressiefractuur posterolaterale humeruskop
N axillaris letsel: verminderd abductie, atrofie deloitdeus, gevoelsverlies laterale bovenarm.
RC-scheur
SCHOUDER
Anterieure luxatie
Bankart-letsel
Wat is het?
Gevolg?
Rol duur luxatie?
Anterieure avulsie van het glenoidlabrum ± botfragment
minder congruentie → instabiliteit
geen rol
SCHOUDER
Anterieure luxatie
Bony bankletsel R/
Technisch moeilijk: hard glenoïd
Oplossing bij ernstig botverlies: bot-blok (vergroting oppervlak glenoïd) dmv Latarjet-procedure
SCHOUDER
Anterieure luxatie
Hill-Sachs laesie
Voorkomen
Wat is het?
Ontstaan?
‘Engaging Hill-Sachs’?
Duur luxatie rol?
54% < 40 jaar
Impactie op posterolaterale humeruskop
Achterste deel humeruskop slaat tegen anterieure rand glenoïd.
Engaging: letsel haakt opnieuw in glenoïd (recidief luxatie)
Geen rol
SCHOUDER
Anterieure luxatie
N. axillaris letsel
Voorkomen?
Mechanisme letsel?
Klinisch beeld?
Diagnose?
Therapie?
10%
Tractie bij anterieure luxatie
deltoideus atrofie, paresthesie laterale bovenarm
ALTIJD CONTROLEREN
L-R vergelijken: atrofie, sensibiliteit
R/
Acuut: pijnstilling, immobilisatie
Elektrische stimulatie (atrofie voorkomen)
Mobilisatie schouder
SCHOUDER
Anterieure luxatie
Waarom verhoogt verlies van glenoid-oppervlak luxatiekans?
Kleiner contactoppervlak → minder stabiliteit. (+ Bankart-letsel: labrum letsel)
SCHOUDER
Anterieure luxatie
Wat is de balance stability angle? Wat gebeurt er met deze hoek na glenoïddefect?
Maximale hoek vóór luxatie optreedt.
Wordt kleiner → minder stabiliteit.
SCHOUDER
Anterieure luxatie
Groen: Hill sachs
Rood: Bankart letsel
SCHOUDER
Anterieure luxatie
Diagnose anterieure luxatie?
typische houding?
typisch anatomisch teken?
beeldvorming?
Geïmmobiliseerd: aductie met lichte abductie (uitzondering: luxatio erecta)
Epaulette-teken: hoekige schouder
RX (transscapulair, axillair, AP, AP + exorotatie)
SCHOUDER
Anterieure luxatie
Wat is het epaulette teken?
Hoekige afvlakking van de schouder → typisch voor anterieure luxatie schouder
SCHOUDER
Anterieure luxatie
Behandeling?
Pijnstilling
Relatief urgent
Reductie (hippocrates, kocher, …)
3 weken draagdoek <=> oud: mobilisatie
SCHOUDER
Anterieure luxatie
Nazorg na reductie bij jongeren?
Nazorg na reductie bij ouderen?
Jong: 3 weken draagdoek
Oud: mobilisatie (cfr. frozen shoulder)
Beide: evt. tonificatie m subscapularis (anterieure spier)
SCHOUDER
Anterieure luxatie
Belangrijkste complicatie bij jongeren?
Belangrijkste complicatie bij ouderen?
Chronische instabiliteit
Frozen shoulder
SCHOUDER
Chronische posttraumatische instabiliteit
RF?
Kliniek?
Testen?
Beeldvorming?
Behandeling?
Acute luxatie, werpsporten
Pijn, ‘dead arm’', rec. luxaties
Testen:
abd+exorot
ant. apprehensietest
relocatietest
Arthro MRI
R/
proprioceptie, kracht oefeningen
chirurgie: latarjet procedure ikv Bankart
(dead arm = plots krachtverlies bij abductie/exorotatie)
SCHOUDER
Anterieure luxatie
Kenmerken van habituele luxaties?
Behandeling?
Hyperlaxiteit
Sulcus sign, exorotatie > 90°
Bilateraal
Multidirectioneel
R/ revalidatie
SCHOUDER
Anterieure luxatie
Kenmerken spontane luxatie?
Behandeling?
Psychische afwijkingen
R/ psychotherapie (gn chirurgie!)
SCHOUDER
Posterieure luxatie
Mechanisme?
Pathognomisch teken?
Gevolgen?
Diagnose?
Behandeling?
Traumatischn epilepsie, …
Geen exorotatie mogelijk
Anterieure hill-sachs
gn exorotatie + light-bulb teken op RX (CT >>)
Tractie
SCHOUDER
Frozen shoulder
belangrijkste klinisch kenmerk?
Zowel actieve als passieve mobiliteit beperkt. (<=> psychomotorisch: enkel actief)
SCHOUDER - EXAMEN
Frozen shoulder
Etiologie
PRIMAIR (60%): idiopathisch (inflammatie)
SECUNDAIR:
systemic: DM, hypoT, hyperT
extrinsiek: cardio, CVA, parkinson, …
intrinsiek: rotator cuff-scheur, bursitis calcarea, impingement, …
SCHOUDER
Frozen shoulder
behandeling
gesloten mobilisatie onder verdoving
infiltraties
SCHOUDER
Bursitis/tendinitis calcarea
Pathogenese
Neerslag hydroxyapatiet
in supraspinatuspees of subacromiale bursa
SCHOUDER
Bursitis/tendinitis calcarea
Welke fase is pijnloos/pijnlijk?
pijnloos: calcificerende fase
pijnlijk: resorptie fase
SCHOUDER
Bursitis/tendinitis calcarea
Behandeling
NSAID
Mobilisatie
Infiltratie met xylocaïne en medrol
evt chirurgie bij recidief
SCHOUDER
Impingement
Pathogenese
Inklemming RC (vnl. supraspinatuspees) en bursa tussen acromion en humeruskop → repetieif: inflammatie
Anatomisch: ongunstig acromion (type 2, 3)
Functioneel: verzwakte RC geeft onvoldoende depressie humeruskop.
SCHOUDER
Impingement
RF
>40 jaar
Bovenhandse sporten
Acromion type 2 (gebogen), 3 (haak)
SCHOUDER
Impingement
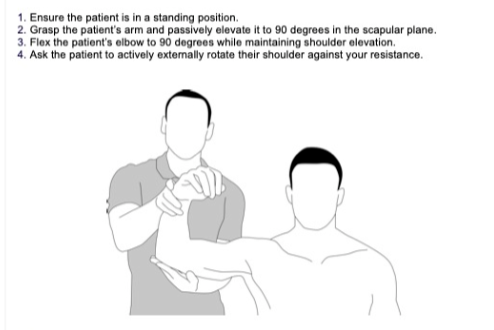
Kliniek + testen
Nachtelijke pijn (inflammatie)
Pijn bij abductie of endorotatie
Neer-test: passieve elevatie
Hawkins-test: flexie + 90° endorotatie + duim naar beneden (tuberculum maj draait onder lig. CA)
SCHOUDER
RC-scheur
Belangrijkste oorzaak RC-scheur?
Degeneratie
SCHOUDER
RC-scheur
Biomechanisch gevolg scheur?
Afname stabilisatoren: humeruskop botst tegen acromion
Secundaire artrose en pijn
SCHOUDER
RC-scheur
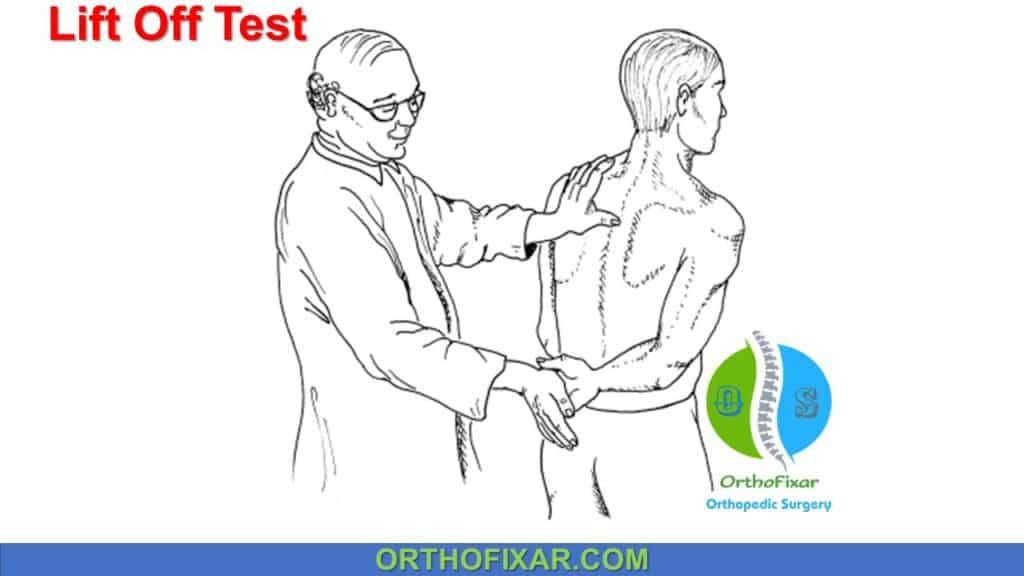
Diagnose
Pijn en krachtverlies
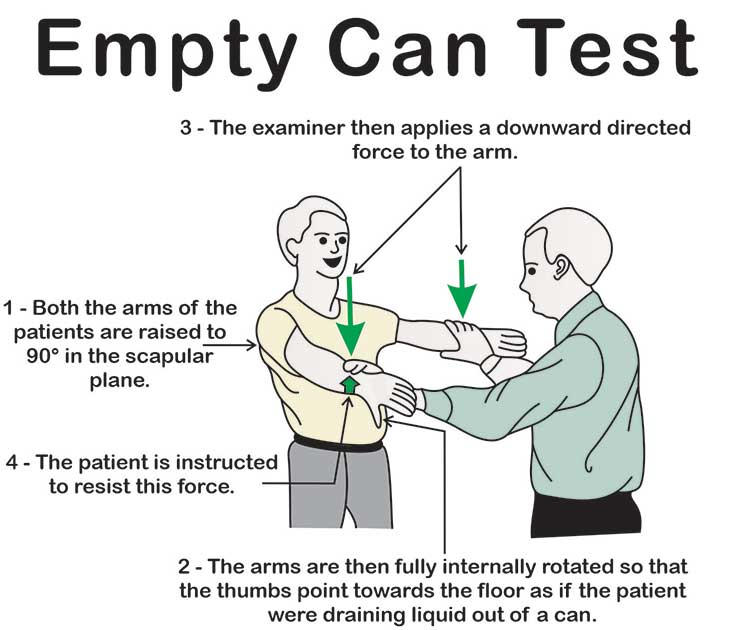
Provocatietest: Jobe, Gerber
Teken van hornblower
RX, echografie
SCHOUDER
RC-scheur
Welke spier test Jobe-test?
Supraspinatus
SCHOUDER
RC-scheur
Welke spier test Gerber?
Subscapularis
SCHOUDER
RC-scheur
Wat is het hornblower’s sign?
Teken posterieur cuff schade (vnl. teres minor)
SCHOUDER
Bicepspeesscheur
K?
D?
R?
Acute plotse pijnscheut
Popeye sign
Conservatief (<=> distale bicepspeesscheur)
SCHOUDER
Omartrose
Primair E?
Secundair E?
Primair: KB verlies + intact RC
Secundair: RC pathologie (humerus botst tegen acromion)
SCHOUDER
Humerus#
Types?
Classificatie van Neer
Humeruskop
Tuberculum majus
Tuberculum minus
Humerus diafyse
SCHOUDER
Humerus#
Behandeling fractuur humerus diafyse?
Conservatief
IM nagel (cave moet door RC)
Plaats (cave n radialis → drop hand)
SCHOUDER
Gerefereerde pijn
Wat zijn oorzaken van anterieure schouderpijn?
Impingement
AC
Clavicula#
RC-scheur
Frozen shoulder
Arthritis
TOS
SCHOUDER
Gerefereerde pijn
Wat zijn oorzaken van lateraal schouderpijn?
RC-scheur
Impingement
Frozen shoulder
Cervicale radiculopathie
SCHOUDER
Gerefereerde pijn
Wat zijn oorzaken van posterieur schouderpijn?
Cervicale radiculopathie
Frozen shoulder
RC-scheur
Fractuur scapula
ELLEBOOG
Wat is de radiocapitellaire lijn?
Een lijn door de radiusnek die door het centrum van het capitellum moet lopen.
Indien afwijkend: vermoeden van radioskop luxatie.
ELLEBOOG
Hoe beoordeel je de radiocapitellaire lijn bij kinderen?
Probleem: capitellum onvolledige ossificatie
Oplossing: positie wordt geschat op ongeveer 30° voorwaarts in sagittaal vlak.
ELLEBOOG
Functie lig. annulare
Radiuskop ter plaatse houden
ELLEBOOG
Punctie in ellebooggewricht
Indicatie
Methode
Indicatie:
posttraumatische pijnlijke zwelling
vermoeden septische arthritis
Methode:
postero-laterale hoek boven lig. anulare.
vóór AB
ELLEBOOG
Pronatie-supinatie-as
Flexie-extensie-as
pronatie-supinatie
door radiuskop en capitellum
door distale einde ulna
flexie-extensie
niet loodrecht op humeruslengte
valgushoek: 10-15%
ELLEBOOG- EXAMEN
Waarom is anatomische reconstructie belangrijk bij voorarmfracturen?
Voor behoud van pronatie-supinatie.
radius: kromming
ulna: recht
ELLEBOOG
Ligamentaire stabiliteit van elleboog?
ulnair ligament (voor, achter, schuin) → belang valgusstress!
lig annulare
ELLEBOOG
Fysiologische valgushoek?
Bij wie groter?
10-15°
Vrouwen
ELLEBOOG
Luxatie
Epidemiologie
Bij wie meest f. luxatie?
Bij wie 2e meest f. luxatie?
1e bij kinderen
2e bij volwassenen
ELLEBOOG
Luxatie
Welke structuur is altijd betrokken bij een elleboog luxatie?
Associaties?
Altijd: ulnair collaterale ligament
Associaties
Radiuskopfractuur (volw)
Mediale epicondylusfractuur (kind)
ELLEBOOG
Luxatie
Waarom krijgen kinderen avulsiefracturen bij luxatie elleboog?
Ligamenten sterker dan bot
ELLEBOOG
Luxatie
Diagnose elleboogluxatie
Pijn
Misvormd
Zwelling
urgent neurovasculair onderzoek
pols
capillaire refill
n. ulnaris (spreiden vingers, sens pink en ringvinger)
ELLEBOOG
Luxatie
Behandeling elleboogluxatie
ASAP
Algemene narcose
Lengte as tractie in lichte flexie
ELLEBOOG
Luxatie
Nazorg na reductie elleboog-luxatie
Open gips: zwelling toelaten (a brachialis)
Mobilisatie na 1 week
ELLEBOOG
Luxatie
Typische anamnese elleboog luxatie
Val op gestrekte arm
ELLEBOOG
Luxatie
Complicaties
Neurovasculair (a brachialis, n medianus, n ulnaris)
Verstijving (meest frequent bij elleboog)
Peri-articulaire calcificaties
Chronisch instabiliteit (~proc. coronoideus)
ELLEBOOG
Distale humerusfractuur
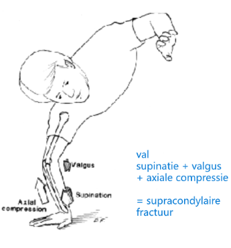
Typische anamnese
Val op uitgestrekte arm
Supracondylair:
supinatie
valgus
axiale compressie
ELLEBOOG
Distale humerusfractuur
Classificatie
Supracondylair
Transcondylair
Intercondylair
T-condylair
Lateraal/mediaal
ELLEBOOG
Distale humerusfractuur (supracondylair)
E?
K?
R? (stabiel vs. instabiel)
val + supinatie + valgus + axiale compressie
N interosseus anterior syndroom (geen OK-sign), sens ok.
R:
stabiel: gips
instabiel: fixatie met pins
NB: niet veel flexie → a brachialis
ELLEBOOG
Distale humerusfractuur
Welke zenuw is typisch betrokken bij supracondylaire fracturen van de humerus?
N interosseus anterior
K: geen OK-sign
ELLEBOOG
Olecranonfractuur
E?
R?
Directe impact op olecranon
Vaak verplaatst door triceps
R/ chirurgie (pinnen + cerclage + tension band)
Goede prognose
ELLEBOOG
Radiuskopfractuur
Hoe controleer je de positie van de radiuskop op RX?
Radiocapitellaire lijn: midden radiuskop door centrum capitellum.
ELLEBOOG
Radiuskopfractuur
Kliniek
Beperkte pro- en supinatie
Drukpijn radiuskop
± crepitatie
ELLEBOOG
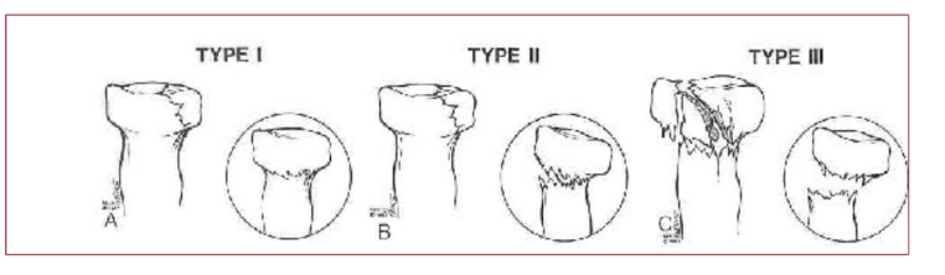
Radiuskopfractuur
TYPES + behandeling
TYPE 1 (onverplaatst)
RX negatief
R/ draagdoek/splint + snelle mobilisatie
TYPE 2 (verplaatst)
RX positief
Controle pro/supinatie dmv IA anestheticum
R/
fragment <30 EN geen pro/sup block: draagdoek/splint
fragment >30% OF pro-sup block: open reductie met interne fixatie (ORIF)
TYPE 3 (COMMUNITIEF)
RX: meervoudige fragmenten
R/ resectie (+ 2e tijd prothese)
ELLEBOOG
Radiusfractuur
Behandeling type III
risico bij resectie?
risico bij radioskopresectie?
osteonecrose
radius migreert → polspijn
ELLEBOOG
radiusluxatie
associatie?
diagnose?
Monteggia-fractuur:
fractuur ulna
luxatie radiuskop
radiocapitellaire lijn klopt niet
ELLEBOOG
Radiusfractuur/luxatie
Wat is het verschil tussen monteggia en een galeazzi fractuur? behandeling?
MONTEGGIA
fractuur ulna
luxatie radiuskop
R/ anatomische repositie en fixatie
GALEAZZI
fractuur radius
luxatie ulna aan de pols
R/ anatomische repositie en fixatie
(alle fracturen voorarm vereisen anatomische reconstructie)
ELLEBOOG
Pronation douloureuse
Synoniem?
E?
K?
D?
R?
Pulled elbow
Radius uit lig anulare
Pijnlijke pronatie
RX om fractuur uit te sluiten
R/ korte supinatie ± anestheticum
ELLEBOOG
Verschil tussen tenniselleboog en golferselleboog?
Tenniselleboog
Epicondylitis lateralis
extensoren
Golferselleboog
Epicondylitis medialis
flexoren
ELLEBOOG
Epicondylitis lateralis
P?
K/D?
R?
Insertietendinopathie extensoren tgv overbelasting
Kliniek
Drukpijn epicondylus lat.
Pijn polsextensie tegen R
Pijnlijke stoeltest
R/
conservatief
activiteiten aanpassen
stretching
NSAID
ELLEBOOG
Distale bicepspeesruptuur
E?
K?
D?
R?
E: 5%, M > (100/1)
K:
acute scherpe pijn
krachtverlies (flexie/supinatie)
proximale spierbuik
D: MRI
R: chirurgie ! <=> prox. biceps
ELLEBOOG
Bursitis olecrani
E?
R?
E:
primair
secundair: jicht, RA, infectie, trauma, punctie
R:
causaal (jicht, RA, …)
infectie: AB ± drainage
mechanische: druk vermijden + NSAID
ELLEBOOG
Distale radiusfractuur
Voorkomen?
17%
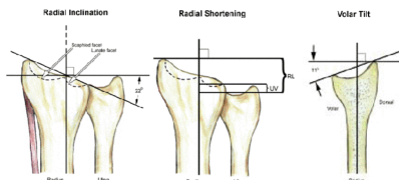
ELLEBOOG - EXAMEN
Distale radiusfractuur
Biomechanica distale radius (3 kenmerken)
Radiale inclinatie: ~20°
Radiale vekrorting: radius > ulna distaal
Volar tilt: articulair vlak kijkt naar beneden (~10° palmair gekanteld)
ELLEBOOG - EXAMEN
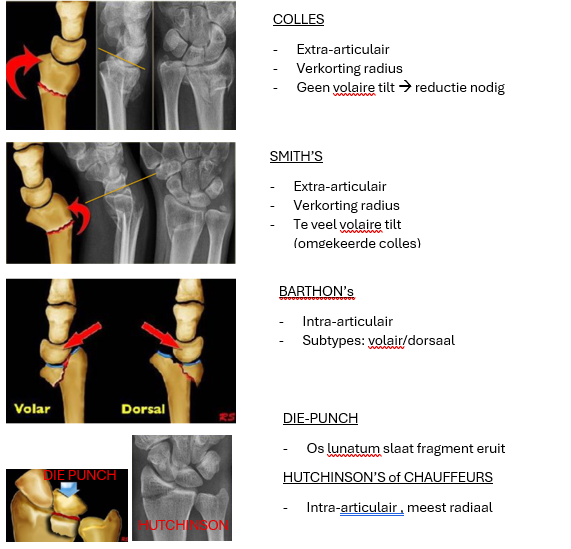
Distale radisufractuur
Types
Colles?
Smith?
Barton?
Die-punch?
Hutchinson/chauffeurs?
Colles | Extra-articulair Verkorting radius Geen volaire tilt | |
Smith | Extra-articulair Verkorting radius Te veel volaire tilt | |
Barton | Intra-articulair volair/dorsaal | |
Die-punch | os lunatum slaat fragment van distale radius eruit | |
Hutchinsons | Intra-articulair radiaal distaal deel afgebroken |
ELLEBOOG
Distale radiusfractuur
Behandeling
Wanneer conservatief?
Wanneer chirurgie?
Conservatief: gesloten reductie (gips)
Niet verplaatst
Stabiel
<10° dorsaal angulatie
<1 mm laterale shift
en <2 mm verkorting
Chirurgie: ORIF
ernstige dorsale angulatie
significante verkorting (>2mm)
IA-fragmenten
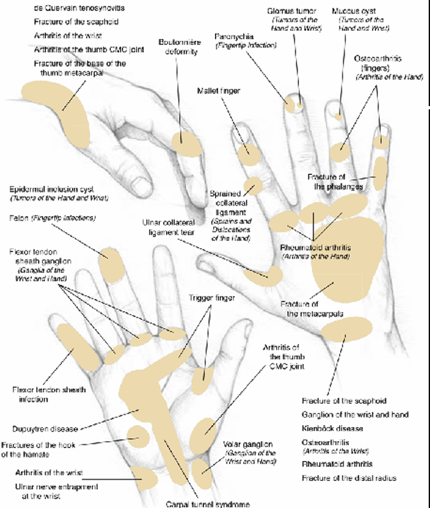
POLS/HAND
Pijndiagram kennen
POLS/HAND
CTS
E?
Bij welke groep vaker?
K?
Meest f. zenuwcompressie BL
tenosynovitis, DM, hypoT, …
Mannen 50 j en zwangeren
K:
paresthesie n. medianus
nachtelijke pijn (altijd)
laat: krachtverlies, thenar atrofie
POLS/HAND
CTS
Behandeling carpaal tunnel syndroom
Conservatief
nachtsplint
kortdurend NSAID
Stretching
infiltratie cortico eenmalig (niet bij zwangeren)
Chirurgisch
indien geen beterschap na 3 maand.
POLS/HAND
Quervain tenosynovitis
E?
E?
K?
D?
Inklemming comp. 1 (APL, EPB)
Vrouwen, ± 50j
Crepitatie, zwelling thv thenar
Test van Finkelstein (duim in hand + ulnaire deviatie → pijn)
POLS/HAND
Quervain tenosynovitis
Behandeling
Rust
NSAID
Spalk
Infiltratie
Heelkunde indien geen beterschap
(minder tijdsdruk itt carpaal tunnelsyndroom waar hypothenaratrofie ontstaat)
POLS/HAND
Triggervinger/springvinger
E?
P?
R?
E: reumatologisch, DM, idiopathisch (meestal)
P: nodulaire verdikking op pees zit vast thv pulley A1 (thv MCP)
R: opensnijden pulley A1
POLS/HAND
Dupuytren
Epidemiologie
50% bilateraal
Mannen >
50 jaar >
Progressief
Aggressief: vroege onset, radiaire zijde, ledderhose, peyronie
POLS/HAND
Dupuytren
P?
K?
Welke vingers meestal aangetast?
Evolutie?
P: palmaire fibromatose (verdikking en contractie palmaire fascia)
K:
pijnloze noduli handpalm + putjes
1) ringvinger 2) pink 3) middenvinger
E:
fascia strengen
→ MCP flexiecontractuur
→ PIP flexiecontractuur
HAND/POLS
Dupuytren
Behandeling
collagenase injectie (cave peesruptuur)
chirurgische resectie fasciastrengen indien patiënt hand niet plat op tafel kan leggen.
HAND/POLS
Vingertipinfecties
Verschil tussen paronychia en felon?
paronychia: infectie rond nagel
felon: infectie in pulpa
HAND/POLS
Vingertipinfecties
K?
R?
Hoe verdoof je een vinger?
K: rood, warm, zwelling, pijn
R: draineren
digitaal blok (radiaal + ulnair)
HAND/POLS
Flexorpeesscheede infectie
Urgentie?
Typisch teken?
R?
URGENTIE!
Drukgevoelig, pijn bij passieve extensie en vingers in flexie
R/ chirurgisch debridement + IV AB