Pulmonary Embolism
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Pulmonary Embolism
A common, serious, and potentially fatal complication of thrombus formation within the deep venous circulation
It can happen silently
Can be symptomatic in the LE because of the DVT but the danger PE brings is really grave, you think the danger is in the LE but it is actually in the heart and the lungs
An embolism is a clot that is formed elsewhere and travels to the heart and the lungs, and obstructs the pulmonary vasculature that’s going to cause all the symptoms; usually comes from DVT
Deep Venous Thrombosis
The process of thrombosis is blood clotting
Usually forms in LE in the venous system (in the deep veins not the superficial veins)
There is a deep venous and superficial venous system (varicosities you see in legs)
Can’t really see the deep venous system but can be felt if involved
When we talk about DVT proceeding into Pulmonary Embolism, we only think of one disease process:
Venothromboembolism
Which occurs more often: DVT or PE?
DVT occurs about 3 times more often than PE
Not all patients with DVT will go through PE
There is a big chance; of 3 DVTs, 1 will only progress to PE
That is why, we should be aggressive in identifying and managing patients with PE
PE can be fatal or can cause chronic ___________
thromboembolic pulmonary hypertension
Elevation of BP in the pulmonary arteries
If not controlled and the BP in the pulmonary arteries continues to go higher, it will lead to the development of (R) sided heart failure in the end. That is because of the thromboembolism since the thrombus may just gather up in the pulmonary arteries, that might be causing injuries to the pulmonary artery which may negatively affect the pressures inside the artery.
DVT: Post-Phlebitic Syndrome
Inflammatory process
Major adverse outcome of DVT alone, without PE
Occurs in more than half of patients with DVT
Valve incompetence and exudation of interstitial fluid
Chronic ankle swelling and calf swelling and aching (especially after prolonged standing), skin ulceration
Usually occurs at the end of the day; severity of the edema depends on the severity of valve insufficiency
DVT: Post Phlebitic Syndrome caused by ____________
permanent damage to the venous valves of the leg
Cannot prevent blood regurgitation
Due to inflammation, the valve will not function properly (valve incompetence)
Epidemiology
Afflict millions of individuals worldwide
Account for hundred thousand deaths annually in the US
15% mortality rate, exceeds mortality rate of AM
Between heart attacks and PE, death rate is higher in PE
Still remain difficult to detect; happens instantly, leaving no time to investigate
Death rate from PE increases with age
Higher in African-american than in whites
Men = women
≈50% are idiopathic
Pulmonary Embolism: Pulmonary Infarction
Pleuritic chest pain that may be unremitting or may wax and wane
Clot from the legs will dislodge, passes through the pulmonary artery and end up in the pulmonary system, causing obstruction → infarction in the lungs and presenting as a painful event (called pain pleurisy or pleuritic chest pain)
Painful near the pleura, making it more painful d/t presence of receptors
Hemoptysis - d/t infarction which injured and killed the pulmonary parenchyma
Pulmonary Infarction: tissue infarction occurs ___ after embolism / obstruction
3-7 days
Pulmonary Infarction presents with:
fever
leukocytosis - predominance of WBCs
elevated ESR - sign of inflammation
Radiologic evidence of infarction
Pulmonary Infarction syndrome
Caused by a tiny peripheral pulmonary embolism
Pleuritic chest pain, often not responsive to narcotics
Lancinating pain which isn’t resolved by analgesics
Low-grade fever
Pleural rub
Parang nagkikiskisan yung pleura because it is inflammatory
Occasional scant hemoptysis
Not in large amounts
Small as it is mostly in the periphery
Leukocytosis
Predominance of neutrophil or WBC
5 most common co-morbidities in PE
Hypertension
Surgery within 3 months
Immobility within 30 days
Cancer
Obesity
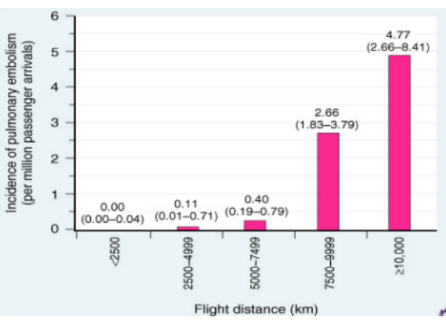
Incidence in Air travel
Higher altitudes = higher propensity to develop DVT
Passengers are advised to move around, stretching and pumping the legs every 2 hours
Virchow’s Triad
Circulatory stasis
Blood circulation slows down especially in conditions which require prolonged immobilization
Endothelial Injury
Always starts with endothelial injury so if the endothelium is injured → trigger for blood to clot.
Even if the endothelium is not injured (inflammatory stage), it can still bring about thrombosis.
Hypercoagulable State
obese, diabetic, HTN cancer
blood is thicker → higher tendency to adhere to each other
DVT Formation - Deep Veins
pass through the deep tissues of the leg
transport blood from the legs and feet back up to the heart
run between muscles of the leg
Contractions of these muscles while we move our leg and ankle help to squeeze the blood back up toward the heart
How embolus produces effects based on ocation
If it largely affects the alveolar sacs, good exchange of O2 & CO2 would be affected.
Capillary area - where O2 & CO2 exchange takes place
Smaller and fewer obstructed arteries → not too much hypoxemia; can still survive otherwise if several → significant hypoxemia since majority of the lung parenchyma is involved
Small embolus (smaller portion of the lung parenchyma involved) → more pain rather than dyspnea
When a pulmonary embolus blocks the ® ventricle, there is a sudden increase in pressure in the pulmonary artery. As a result the ® ventricle has to work harder to keep pumping blood; after a certain threshold it fails which disrupts blood flow to vital organs leading to death AKA _______
Hemodynamic Collapse
Pulmonary Embolism - Risk Factors
Old age
Pneumonia
Surgery
Fractures
Immobility
Diseases of the coagulation cascade
Sickle cell disease
COPD
Pulmonary Embolism - Treatments
Direct Oral Anticoagulants
Vitamin K antagonist
Low Molecular Weight Heparin
Reperfusion Therapy
Classic Dichotomy in PE Pathogenesis
Inherited/ primary - unusual
Acquired/secondary - common d/t certain medical conditions or lifestyle
Major Acquired Risk Factors for VTE
Advancing age
Arterial disease including carotid and coronary disease
Obesity
Cigarette smoking
Chronic obstructive pulmonary disease
Personal or family hx of venous thromboembolism
Recent surgery, trauma, or immobility including stroke
Acute infection
may promote inflammation in the blood vessels
Long-haul air travel
Cancer
Pregnancy, oral contraceptive pills, or hormone replacement therapy (estrogen, testosterone
Pacemaker, implantable cardiac defibrillator leads, or indwelling central venous catheters
Major Thrombophilias associated with venous thromboembolism - Inherited
Factor V Leiden resulting in activated protein C resistance
Prothrombin gene mutation 20210
Antithrombin III deficiency
Inherited predisposition to blood clotting
Protein C deficiency
Responsible for maintaining blood in its fluid form
Protein S deficiency
Protein C and S have tendency of blood to clot more in fluid
Major Thrombophilias associated with venous thromboembolism - Acquired
Antiphospholipid antibody syndrome (APAS)
Similar to lupus
For mothers who experienced miscarriage
Predisposed to blood clot
Hyperhomocysteinemia
High levels will signify greater likelihood of blood clotting
Substance in the body for homosustain
Right Ventricular Dysfunction & Ventricular Dependency
If Pulmonary embolism greatly obstructs the pulmonary artery, expect an increase in pressure in PA
Increased RV afterload
Overtime, it gets tired getting bigger and dilates becoming dysfunctional and leading to Right ventricular sided heart failure
Resulting in decreased o2 supply → decreased RV output → decreased systemic perfusion → decreased LV output, less ejection fraction, less cardiac output → hypotension→ systemic hypoperfusion
If it happens fast and pt is left unattended the pt may die instantly
Massive Acute Pulmonary embolism
Presentation |
|
Right ventricular dysfunction | Rare |
Therapy | Heparin plus thrombolytic therapy or mechanical intervention |
Moderate to Large / Submassive Acute Pulmonary Embolism
Presentation | Normal systemic arterial blood pressure; typically, >30 percent perfusion defect on lung scan |
Right ventricular dysfunction | Present |
Therapy | Heparin and NSAIDs |
Small to Moderate Acute PE
Presentation | Pleuritic chest pain, hemoptysis, pleural rub, or evidence of lung consolidation; typically, small peripheral emboli |
Right ventricular dysfunction | Absent |
Therapy | Heparin |
Pulmonary Infarction PE
Presentation | Pleuritic chest pain, hemoptysis, pleural rub, or evidence of lung consolidation; typically, small peripheral emboli |
Right ventricular dysfunction | Rare |
Therapy | Heparin and NSAIDs |
Paradoxical PE
Presentation | Sudden systemic embolic event such as stroke |
Right ventricular dysfunction | Rare |
Therapy | Anticoagulation ± closure of the right-to-left cardiac shunt |
Nonthrombotic PE
Presentation | Most commonly air, fat, tumor fragments, or ambiotic fluid |
Right ventricular dysfunction | Rare |
Therapy | Supportive |
Most common symptom
Dyspnea
Most common sign; reflective of dyspnea
Tachypnea
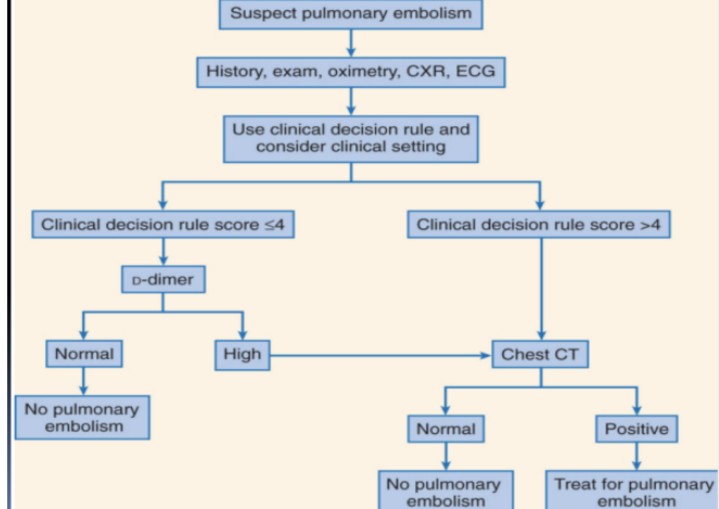
Clinical Decision Rule
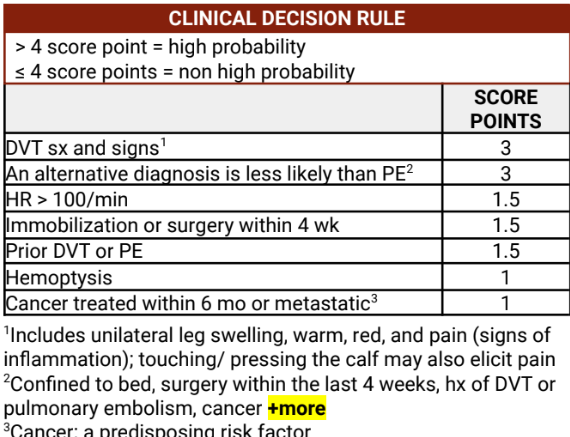
Cardinal manifestations of inflammation
Calor - warm
Dolor - pain
Rubor - redness
Tumor - swelling
Functionless
Differential Diagnosis
Myocardial infarction | Pericarditis |
Pneumonia | Intrathoracic cancer |
L sided Congestive HF | Rib fracture |
Cardiomyopathy | Pneumothorax |
Primary pulmonary htn | Costochondritis |
Asthma | Musculoskeletal pain |
Anxiety |
Diagnostic - Plasma D-dimer ELISA
Advantages | Disadvantages |
A normal result in this rapid turnaround blood test makes PE exceedingly unlikely. | Level is elevated in patients with many systemic illnesses that mimic PE, such as pneumonia and myocardial infarction. Level is elevated in patients with sepsis, cancer, postoperative state, and pregnancy |
Diagnostics - Electrocardiogram
Advantages | Disadvantages |
Universally available; may indicate ominous acute cor pulmonale or benign pericarditis | Acute cor pulmonale on electrocardiogram is not specific or PE; not a sensitive test |
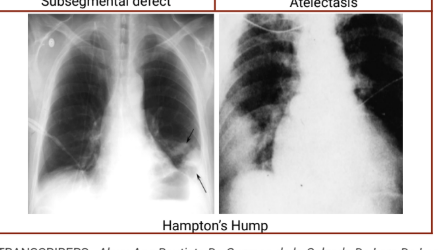
Diagnostics - Chest radiography
Advantages | Disadvantages |
Usually, has minor abnormalities but occasionally pathognomonic; may indicate alternative diagnosis such as pneumothorax | Not specific |
Diagnostics - Chest computed tomography
Advantages | Disadvantages |
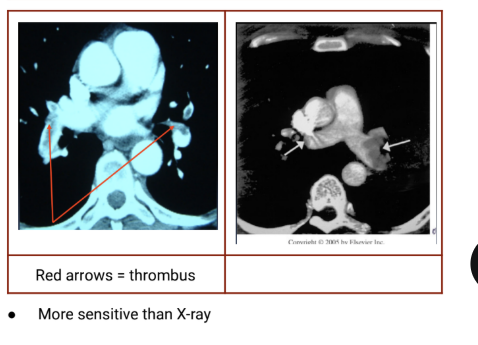
New-generation scanners constitute the new gold standard for diagnosis | Older generation scanners are insensitive for important but distal PE |
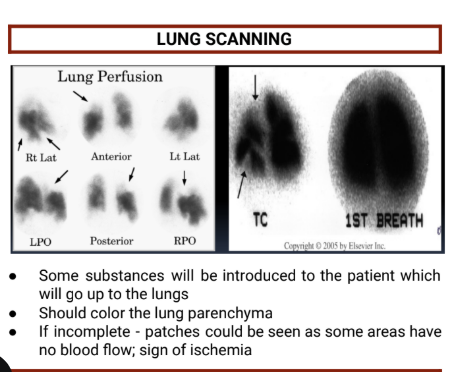
Diagnostics - Lung scanning
Advantages | Disadvantages |
High-probability scans are reliable for detecting PE; normal/near-normal scans are reliable for excluding PE | Most scans are neither high probability nor normal/near-normal; lung scans are falling out of favor; most test results are equivocal |
Diagnostics - MRI
Advantages | Disadvantages |
Excellent for anatomy and cardiac function; the contrast agent does not cause renal failure | In preliminary use; not widely available; experience very limited |
Diagnostics - Echocardiography
Advantages | Disadvantages |
Excellent for identifying right ventricular dilation and dysfunction that is not obvious clinically, thus providing an early warning of potentially adverse outcome | Not specific; many patients with PE have normal echocardiograms; the last cannot reliably differentiate causes of right ventricular dysfunction |
Diagnostics - Pulmonary angiography
Advantages | Disadvantages |
Necessary for catheter-based interventions | Invasive, costly, uncomfortable |
Diagnostics - Venous ultrasonography
Advantages | Disadvantages |
Excellent for detecting symptomatic proximal DVT; surrogate for PE | Cannot image iliac vein thrombosis; imaging of calf is operator dependent; DVT may have embolized completely, resulting in anormal finding |
Diagnostics - Contrast venography
Advantages | Disadvantages |
Used to be a gold standard; excellent for calf veins; necessary for catheter-based interventions | Can cause chemical phlebitis; uncomfortable; costly; may fail to diagnose massive DVT because veins are filled with thrombus and cannot be opacified |
Chest radiography - Subsegmental defect
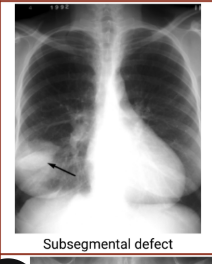
Chest radiography - Atelectasis

Chest radiography - Hampton’s Hump
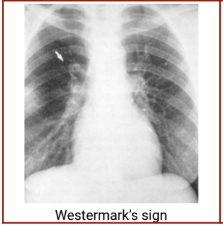
Chest radiography - Westermark’s sign
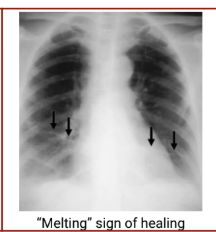
Chest radiography - Melting sign of healing
Chest Computed Tomography Pictures
Lung Scanning Pictures
Venous ultrasonography pictures

Integrated Diagnostic Approach
Components of Management - Anticoagulation
To thin out the blod
Heparin
Low molecular weight heparin
Coumadin
Newer ones include: dabigatran, apixaban, rivaroxaban
-aban = anticoagulant
Components of Management - Fibrinolysis
Streptokinase
Alteplase
Components of Management - Embolectomy
open heart surgery to take out the blood clot from artery (great risk of death)
If you don’t do it, the patient will die anyway
Do it so that there’s still a chance to save the patient’s life
Components of Management - List
Anticoagulation
Fibrinolysis
Embolectomy
Vena cava filters
Primary Prevention
Secondary Prevention
Clinical predictors of increased mortality
Systolic BP less than or equal to 100 mmHg
Age older than 70 years
HR higher than 100 bpm (tachycardia)
Congestive heart failure
Chronic lung disease (e.g. COPD, emphysema, chronic bronchitis)
Cancer