Skin Injuries - Burns and Wounds
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
Sunburn?
Overexposure to UVA and UVB rays from sunlight or tanning beds/lampss
MAY BE ELIGIBLE FOR SELF CARE → UNDER PROPER CONDITIONS
Thermal Injury?
Flames, scalding liquids, hot objects → cause burn
MAY BE ELIGIBLE FOR SELF CARE → UNDER PROPER CONDITIONS
Electrical burn?
Electricity flows through body, with an entry and exit → and heat causes damage
MUST BE REFERRED
Chemical burn?
Exposure to corrosive or reactive chemicals causing tissue damage
MUST BE REFERRED
How do you assess extent of burns?
Extent → Palmar method → patient’s hand ≈ 1% TBSA
<2 handprints (<2% TBSA) → may be self-treatable
What patient factors increase burn severity/risk?
Elderly patients → thinner/loose skin, decrease in healing → even small burns can be serious
Diabetes mellitus / peripheral vascular disease → increase in risk of complications and poor healing
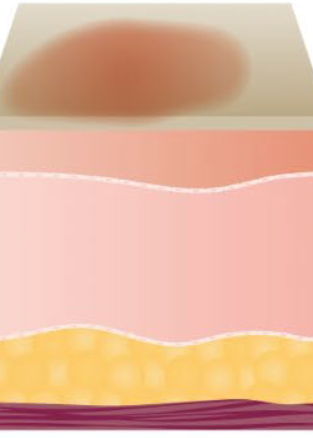
Superficial thickness / first degree burn?
Painful, does not blister or scar
Redness, no blanching, unbroken surface
Recovery → 3-7 days
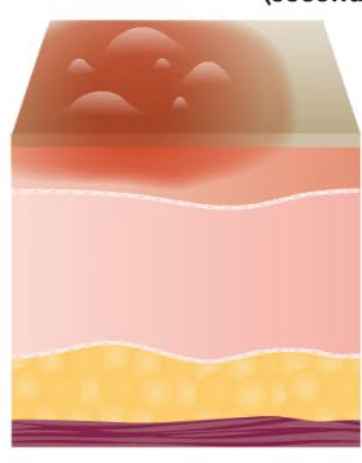
Superficial thickness Second Degree burn?
Do not require surgery but → can scar and be more painful
Blisters/weeps
B’n’B → Break and blanching
2 weeks recovery
Which degree burns can be treated with self care?
First degree / superficial thickness
Second degree / superficial partial thickness
Less than 2% of BSA
Unless burn meets exclusion criteria
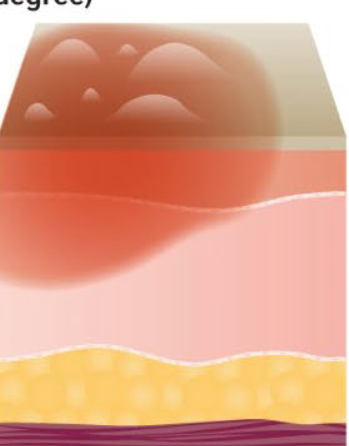
Deep partial thickness Second degree burn?
Require surgery → form more scars and are less painful
Break in skin, less blanching, blisters are uncommon, altered pain
2-9 weeks recovery

Full thickness / Third degree burn?
Dry, insensitive to light touch/pin prick, small areas will heal with substantial scar
Large areas require skin graft and high risk of infection
White/brown, dry, leathery
Little to no pain
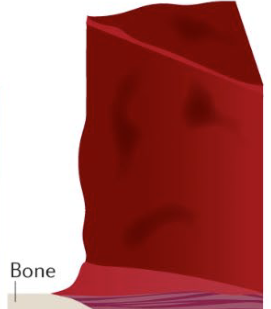
Fourth degree burn?
Involves muscle/bone
Leads to loss of the burned part
Black/charred, no sensation
Which degree burns need hospitalization?
Second degree / intermediate thickness → Notify PCP if 2-10% BSA or hospitalization if over 10% BSA
Third degree → Hospitalization and PT required
Fourth degree → Hospitalization and PT required
Exclusions for burn self treatment?
Sunburn:
Signs of infection → redness/red streaks spreading or moving away from open blisters
Open blisters that are draining pus
Minor burns:
Chemical/electrical/inhalation burns
Elderly
Diabetes Mellitus
Site of injury → hands, face, feet, major joints, genitals/perineum
What are key features of sunburn assessment?
Superficial UV-induced burn
Symptoms peak 12–24 hours after exposure
Most cases have intact skin barrier
When should sunburn be referred for further evaluation?
Blistering
Fever or chills → systemic symptoms
Extensive body surface area involvement
Initial management of sunburns?
Remove further UV exposure immediately
Cool showers/compresses → comfort only, does not limit injury progression
Use of emollients/petrolatum based products
APAP
Avoid topical anesthetics on large areas/broken skin
What are key sun protection counseling points?
Protective clothing + shade
Avoid peak UV hours
Emphasize cumulative skin damage + cancer risk
Use sunscreen regularly
What are the two main types of sunscreen?
Physical/Mineral → zinc oxide, titanium dioxide → reflect UV → good for sensitive skin
Standard chemical → absorbs into the skin and then absorbs UV → needs 15–30 min to activate
How does SPF work?
SPF = time to burn compared to no sunscreen
Ex; 10 min to normally burn → SPF 30 = ~300 min protection
SPF ranges?
Generally SPF is enough unless out for longer than an hour
15 – stops up to 93%
30 – stops up to 97%
50 – stops up to 98%
100 – stops up to 99%
Reapply every 2 hours
Diminishing returns
What are key counseling points for sun protection?
Sun protection needed year-round
“All-day protection” is not reliable → reapply sunscreen regularly
Water/sweat-resistant lasts ~80 min → reapply sooner if rubbed/toweled off
Burned skin is more UV-sensitive → protect carefully
Dark skin still needs sun protection to prevent damage and skin cancer
How should minor burns be cleansed?
Cool → NOT ice-cold water for → 20 min → benefit up to 3 hrs post-burn
Helps reduce pain and limit tissue damage
Mild antiseptic soap to remove debris
Saline not better than clean tap water
Should minor burns be covered?
Sunburn/superficial → no dressing needed, use skin protectant
Partial thickness → non-adherent dressing preferred → gauze or non-stick pads
Plastic wrap can be used if no dressing available
How should minor burns be managed day-to-day?
Cleanse 3-4 times daily with water or mild antiseptic
Let area air dry
Use non-adherent dressing if needed → partial thickness burns
Do not pop blisters or remove loose skin
What should be done if the burn skin is broken?
Clean with soap and water
Apply moist dressing
Use topical antibiotic → triple antibiotic ointment for prevention
Re-cover after ~30 minutes
Continue protective dressing to prevent infection and promote healing
Scar prevention for minor burns?
Keep wound moist → promotes healing and epithelial migration
Avoid UV exposure, use sunscreen → prevents darkening of scars
Silicone therapy (sheets or gels) → occludes + hydrates tissue to improve/prevent scars (e.g., ScarAway)
What are pharmacologic options for pain management in minor burns?
Acetaminophen → preferred first-line
NSAIDs → caution, stop 48 hrs prior if chance of hospitalization/debridement/skin grafting
What are skin protectants/moisturizers used in minor burn care?
First-line → petrolatum-based products (e.g., Aquaphor®, Vaseline)
Promote moist wound healing
Protect from friction + prevent skin drying
Help reduce scarring
Higher oil content → more moisturizing but greasier/less acceptable to patients
What are topical antibiotics used in minor burn care?
Neosporin → triple antibiotic → bacitracin + neomycin + polymyxin B
Polysporin → bacitracin + polymyxin B
Apply TID with dressing changes
Used for infection prevention → NOT treatment
What are topical anesthetics in minor burn care?
Topical anesthetics → ex; benzocaine, lidocaine
MOA: block sodium channels → stop nerve pain/itch signals
Short acting → 15–45 min relief
Use only on small areas (<2% BSA) and intact skin
What is no longer recommended for minor burn care?
Antiseptics
Acute minor wounds?
Expected to heal normally
Ex; Abrasions, cuts, minor burns
Chronic wounds?
Fail to progress through healing after 4-6 weeks
Are not self care conditions
How do you assess if a minor wound can be treated without referral?
Acute → (<24–48 hrs)
Bleeding controlled with gentle pressure
Superficial → no fat, muscle, or bone exposed
No retained foreign body → no debris left behind
No high-risk factors → ex; diabetes, immunocompromised, advanced age, etc..
If any are NO → refer
Cleaning in managing minor wounds?
Rinse with clean running water to remove debris
Mild soap on surrounding skin only → avoid wound bed scrubbing
Saline not superior to tap water
Avoid routine antiseptics → cytotoxic → delays healing
Controlling bleeding in managing minor wounds?
Apply direct pressure with clean gauze (1–2 min)
Elevate if needed
If uncontrolled → refer
Cover or leave open while managing a minor wound?
Small superficial wounds → may be left open after cleansing + skin protectant
If friction/contamination risk → cover with clean wet dressing
Change daily or if soiled
What is first-line topical therapy for minor wounds?
Petrolatum based products → Vaseline or Aquaphor
Promote moist healing
Decrease scarring and scab formation
What topical antibiotics may be used in minor wounds?
Short-term use for contaminated/high-risk wounds
Prevent infection only → not faster healing
Risk → allergic contact dermatitis → especially neomycin
What is recommended for pain management in minor wounds?
Acetaminophen → preferred first-line
NSAIDs may be used if no contraindications (e.g., bleeding risk/procedures)
What is NOT recommended for routine cleansing of minor wounds?
Routine hydrogen peroxide, chlorohexidine, alcohol, or povidone-iodine
Damages fibroblasts and keratinocytes → delays healing
What is daily antiseptic cleansing NOT recommended for minor wound care?
Not better than water or saline
Can disrupt tissue formation, prolong inflammation, or increase irritation/dermatitis risk
Rapidly neutralized by blood/exudate → very limited antimicrobial benefit
Why are silver containing products not recommended for minor wound care?
No proven benefit in minor wounds
May be cytotoxic to fibroblasts and keratinocytes
Prolonged use may cause antimicrobial resistance
Why should minor wounds NOT be left dry to “air out”?
Oxygen for healing comes from blood → not air
Dry wounds form scabs → which then act as a physical barrier to new skin cell migration → forcing cells to grow under instead of across
Leads to slower healing under scab instead of across surface
Why is moist wound healing preferred?
Faster healing
Less inflammation
Less scarring
What are risk factors for chronic wounds?
Disease state → Diabetes mellitus
Excessive pressure
Immobility
Poor circulation
Immunodeficiency
Infection
Poor nutrition
Advanced age
Obesity
What medications are risk factors for chronic wounds?
Sedative hypnotics
Diuretics
Anticholinergics
Immunosuppressive/anti-neoplastic
coticosteroids
What are venous stasis ulcers?
Irregular, exudative ulcers
Lower extremities → often inner side of ankle
What are arterial ulcers?
Dry, necrotic, painful ulcers
Distal locations → below ankle
What are neuropathic/diabetic ulcers?
Often painless → loss of sensation
Bottom of foot → plantar foot location
Slow to heal
What are pressure injuries / ulcers?
Occur over bony prominences
Most common chronic wound type
Also called bedsores/decubitus ulcers
Staged I–IV based on depth
What are the main goals of chronic wound treatment?
Maintain moist environment to promote healing
Protect from infection → often with occlusive dressings
Protect from trauma → cushioning + non-traumatic dressing removal
Minimize scarring
How are chronic wounds generally treated?
Cleanse with normal saline → best option
Alternatives → commercial cleansers or maggot therapy
Treat infection if present
Debride/remove necrotic tissue as needed
Apply appropriate dressing
Hydrocolloid dressing?
“Melts” into wound environment
Protects skin + reduces pressure
Used for pressure ulcers
Ex; replicare, duoderm
Transparent film dressing?
Adhesive barrier that is gas permeable but blocks fluid
Allows wound visualization
Reduce friction
Used for Stage 1 pressure ulcers or IV sites
Ex; bioclusive, tegaderm
Hydrogel / Amorphous hydrogel dressing sheets?
Moist, cooling dressing
Best for burns, dry/dehydrated, or painful wounds
Helps rehydrate tissue
Ex; Solosite, Intrasite

Regrane?
For diabetic neuropathic foot ulcers
Used after debridement to promote healing
What are pharmacists expected to do?
Perform triage
Provide evidence based self care advice
Identify high risk patients
Refer early and appropriately
What are pharmacists NEVER expected to do?
Stage chronic wounds in detail
Select specialty dressings
Manage debridement plans