Exam 1 - Mental Health Terms
1/97
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
98 Terms
clinical epidemiology
a broad field that examines health and illness at the population level. Studies use traditional epidemiological methods and are conducted in groups usually defined by the illness or symptoms or by the diagnostic procedures or treatments given for the illness or symptoms.
Clinical epidemiology includes the following:
Studies of the natural history—what happens if there is no treatment and the problem is left to run its course—of an illness
Studies of diagnostic screening tests
Observational and experimental studies of interventions used to treat people with the illness or symptoms
cultural competence
that nurses adjust their practices to meet their patients’ cultural beliefs, practices, needs, and preferences.
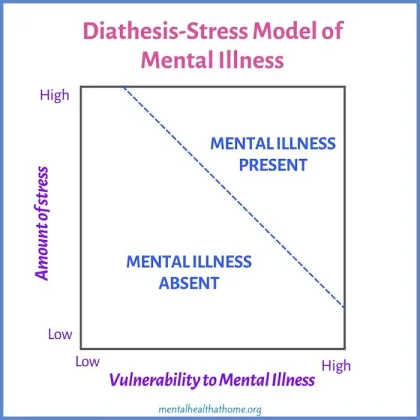
diathesis-stress model
In which diathesis represents biological predisposition, and stress represents environmental stress or trauma, is the most accepted explanation for mental illness.
Compare vulnerability to mental illness to the amount of stress (more stress + more vulnerability = more likelihood of disease)
epidemiology
the quantitative study of the distribution of mental disorders in human populations. Understanding this distribution helps identify high-risk groups and risk factors associated with illness onset, duration, and recurrence.
incidence
conveys information about the risk of contracting a disease. It refers to the number of new cases of mental disorders in a healthy population within a given period of time, usually annually
Mental health
a state of well-being in which each individual is able to realize his or her own potential, cope with the normal stresses of life, work productively, and make a contribution to the community
Mental illness
all psychiatric disorders that have definable diagnoses
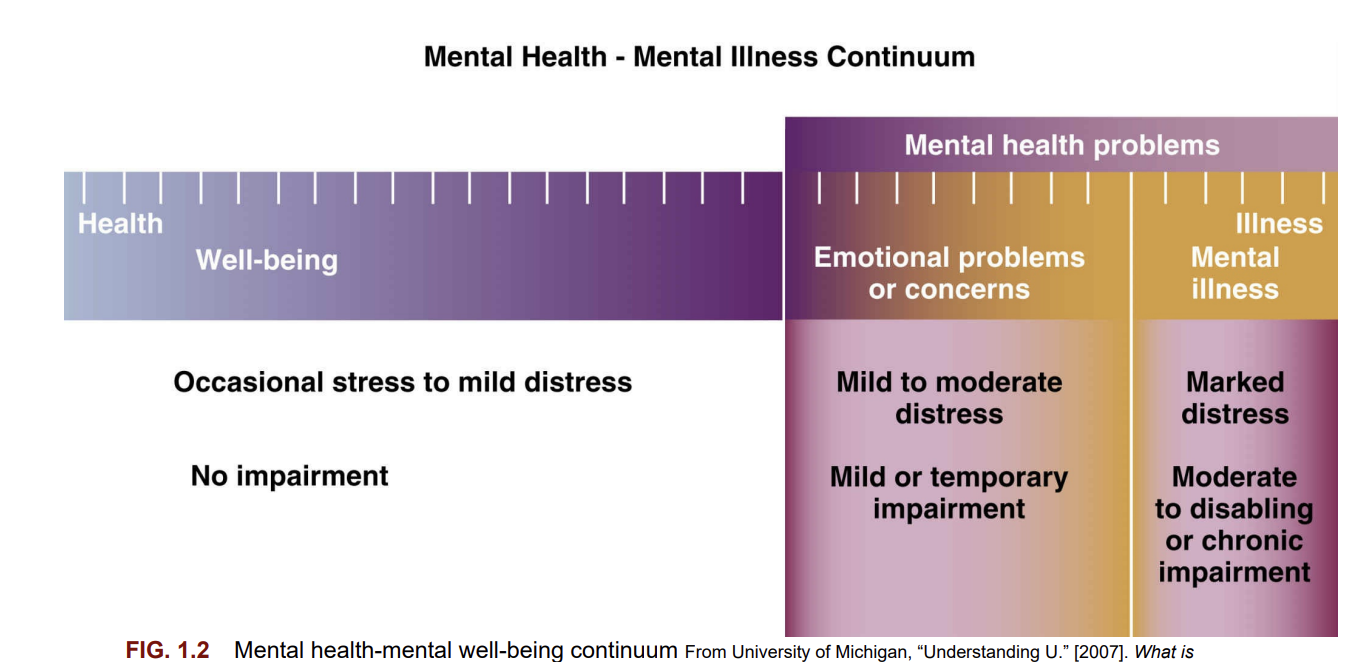
Mental Health Continuum
well-being (mild stress) to concerns/problems to illnesses
Resilience
the ability and capacity for people to secure the resources they need to support their well-being.
prevalence
the total number of cases, new and existing, in a given population during a specific period of time, regardless of when they became ill.
phenomena of concern
Phenomena of concern for psychiatric-mental health nurses include:
Promotion of optimal mental and physical health and well-being
Prevention of mental and behavioral distress and illness
Promotion of social inclusion of mentally and behaviorally fragile individuals
Co-occurring mental health and substance use disorders
Co-occurring mental health and physical disorders
Alterations in thinking, perceiving, communicating, and functioning related to psychological and physiological distress
Psychological and physiological distress resulting from physical, interpersonal, and/or environment trauma or neglect
Psychogenesis and individual vulnerability
Complex clinical presentations confounded by poverty and poor, inconsistent, or toxic environmental factors
Alterations in self-concept related to loss of physical organs and/or limbs, psychic trauma, developmental conflicts, or injury • Individual, family, or group isolation and difficulty with interpersonal relations
Self-harm and self-destructive behaviors including mutilation and suicide
Violent behavior including physical abuse, sexual abuse, and bullying
Low health literacy rates contributing to treatment non adherence
Freuds psychoanalytic theory
Id: at birth, totally unconscious and impulsive
Ego: he first few years of life as the child begins to interact with other, ego follows the reality principle, which says to the id, “You have to delay gratification for right now,” then sets a course of action.
Superego: develops between the ages of 3 and 5, represents the moral component of personality, the egos ideal
He believed experiences during the early stages of life determined individuals life time adjustment patterns and personality traits
Therapy: unstructured, talk therapy, uncover “truth” (unconscious thoughts), long term, 5x/week
Transference
unconscious feelings that the patient has toward a healthcare worker that were originally felt in childhood for a significant other
Countertransference
unconscious feelings that the healthcare worker has toward the patient
Psychodynamic therapy
Freud: the psychoanalytic model by using many of the tools of psychoanalysis such as free association, dream analysis, transference, and countertransference. However, the therapist has increased involvement and interacts with the patient more freely than in traditional psychoanalysis
The best candidates for psychodynamic therapy are relatively healthy and well-functioning individuals, sometimes referred to as the “worried well” who have a clear area of difficulty and are intelligent, psychologically minded, and well motivated for change.
Interpersonal therapy
Sullivan
effective short-term therapy. The assumption is that psychiatric disorders are influenced by interpersonal interactions and the social context. The goal of interpersonal therapy is to reduce or eliminate psychiatric symptoms (particularly depression) by improving interpersonal functioning and satisfaction with social relationships.
3 problems that respond well to this therapy:
Grief and loss: Complicated bereavement after death, divorce, or other loss 2.
Interpersonal disputes: Conflicts with a significant other
Role transition: Problematic change in life status or social or vocational role
Conditioning
pairing a behavior with a condition that reinforces or diminishes the behavior’s occurrence
classical conditioning
Pavlov
when a neutral stimulus (a bell) was repeatedly paired with another stimulus (food that triggered salivation), eventually the sound of the bell alone could elicit salivation in the dogs
Behavioral therapy
operant conditioning
Skinner
a method of learning that occurs through rewards and punishment for voluntary behavior. Behavioral responses are elicited through reinforcement, which causes a behavior to occur more frequently
Behavioral therapy
positive reinforcement
adding pleasant stimulus immediately after that behavior occurs (reward system)
negative reinforcement
removing an unpleasant stimulus immediately after that behavior occurs
punishment
absence of reinforcement, thus decreasing behavior by withholding rewards
Behavioral therapy
based on the assumption that changes in maladaptive behavior can occur without insight into the underlying cause. This approach works best when it is directed at specific problems and the goals are well defined. Behavioral therapy is effective in treating people with phobias, alcoholism, schizophrenia, and many other conditions
4 types: modeling, operant conditioning, systematic desensitization, and aversion therapy.
Modeling
the therapist provides a role model for specific identified behaviors, and the patient learns through imitation
Behavioral therapy
Systematic desensitization
behavior modification therapy that involves the development of behavior tasks customized to the patient’s specific fears; these tasks are presented to the patient while using learned relaxation techniques.
Aversion Therapy
used to treat behaviors such as alcoholism, paraphilic disorders, shoplifting, violent and aggressive behavior, and self-mutilation. Aversion therapy is the pairing of a negative stimulus with a specific target behavior, thereby suppressing the behavior.
Behavioral therapy
Biofeedback
form of behavioral therapy and is successfully used today, especially for controlling the body’s physiological response to stress and anxiety.
Behavioral therapy
cognitive-behavioral therapy (CBT)
Beck:
a structured, goal-oriented form of talk therapy that treats mental health issues by changing negative thought patterns and behaviors
automatic thoughts
Rapid, unthinking responses based on schemas (unique assumptions about themselves, others, and the world in general)
Maslows Hierachy of needs
Physiological needs, safety needs, love and belonging needs, esteem (related to competency, achievement, and esteem from others), self actualization (become everything one is capable of), self transcendence
defense mechanisms
ward off anxiety by preventing conscious awareness of threatening feelings.
Defense mechanisms share two common features: (1) they all (except suppression) operate on an unconscious level and (2) they deny, falsify, or distort reality to make it less threatening.
stigma
a mark of disgrace, shame, or social disapproval associated with a person's characteristics, behaviors, or circumstances, often leading to discrimination, exclusion, or negative stereotypes
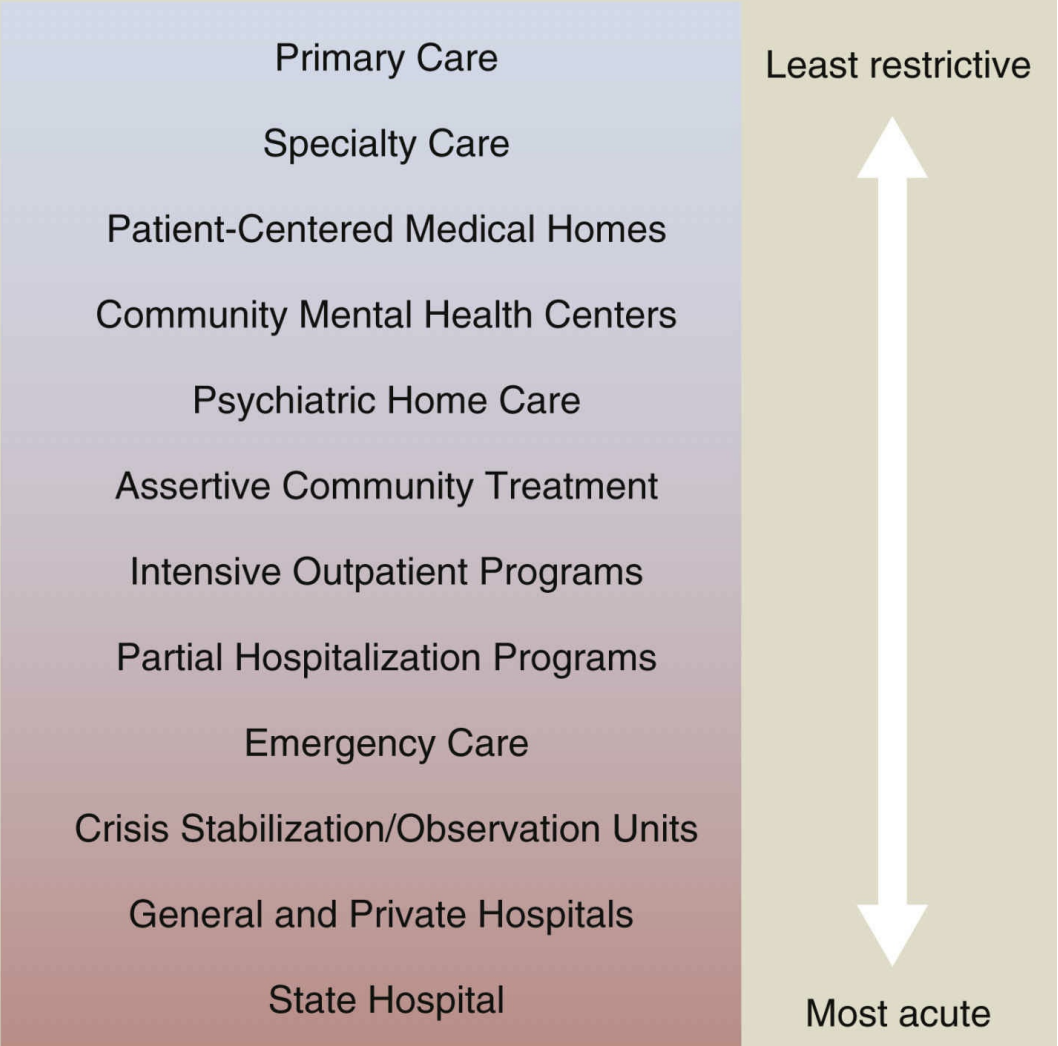
continuum of psychiatric-mental healthcare
from primary care checks to emergency care to hospitalization
decompensation
deterioration of mental health
Specialized psychiatric care providers
an educational background and experience in care of psychiatric problems and mental health. These providers include psychiatrists, psychiatric-mental health advanced practice registered nurses (nurse practitioners or clinical nurse specialists), psychologists, social workers, counselors, and other licensed therapists.
Patient-centered medical homes (PCMHs)
These health homes were developed in response to fragmented care that result in some services never being delivered while others are duplicated. The focus of care is patient-centered and provides access to physical health, behavioral health, and supportive community and social services.
5 key characteristics:
Patient centered care
Comprehensive care
Coordination of care
Improved access (not limited to mon-fri 9-5)
Systems approach
Assertive community treatment (ACT)
an intensive type of case management developed in the 1970s. This treatment was in response to the hard-to-engage, community-living needs of people with serious, persistent psychiatric symptoms.
In homes, agencies, hospitals, or clinicals, 24/7
Emergency care
goal: perform triage (determines severity) and stabilization (resolution of immediate crisis)
3 types
1. Comprehensive emergency service model is often affiliated with a full-service emergency department (ED) in a hospital or medical center setting. Typically, there is dedicated clinical space with specialty staffing. Psychiatric-mental health nurses, psychiatric technicians, mental health specialists, social workers, mental health counselors, and psychiatrists generally make up the multidisciplinary workforce. The concepts of triage and stabilization are incorporated into the individualized care plan for each patient.
2. Hospital-based consultant model utilizes the concepts of the comprehensive model by incorporating triage and stabilization. However, there is generally no dedicated clinical space or comprehensive separate staffing. Psychiatric clinical staff members are assigned to a specific hospital and are on-site or on-call, serving as part of the emergency department staff. Psychiatric clinicians manage emergency psychiatric evaluations as requested. Clinicians complete a “level of care” assessment, attempt to stabilize patients, and arrange for discharge or transfer. The emergency department staff maintain responsibility for all immediate care needs.
3. Mobile crisis team model is considered for stabilization in the field. The teams meet face to face with the person in crisis to assess and de-escalate the situation. While the teams vary in composition, psychiatric-mental health nurses, social workers, and counselors, in collaboration with a psychiatrist and/or an advanced practice nurse, often make up the care team.
Recovery
a process of change through which individuals improve their health and wellness, live a self-directed life, and strive to reach their full potential
elopement
leaving before being discharged (also referred to as being away without leave or AWOL)
Psychiatric-mental health registered nurses
Licensed registered nurses whose focus is on mental health and mental illness and who may or may not be certified in psychiatric-mental health nursing. The registered nurse is typically the only 24-hours-a-day, 7-days-a-week professional working in acute care. Among the responsibilities of the registered nurse are diagnosing and treating responses to psychiatric disorders, coordinating care, counseling, giving medication and evaluating responses, and providing education.
Psychiatric-mental health advanced practice registered nurses
Licensed registered nurses who are prepared at the master’s or doctoral level and hold specialty certification as either clinical nurse specialists or nurse practitioners. These nurses are qualified for clinical functions such as diagnosing psychiatric conditions, prescribing psychotropic medications and integrative therapy, and conducting psychotherapy. They are also involved in case management, consulting, education, and research.
Psychiatrists
Psychiatrists prescribe medication for psychiatric symptoms. They may also provide psychotherapy. As physicians, psychiatrists may be employed by the hospital or may hold practice privileges in the facility
Psychologists
In keeping with their doctoral or doctorate degree preparation, psychologists conduct psychological testing, provide consultation for the team, and offer direct services such as specialized individual, family, or marital therapies
Social workers
Basic level social workers help the patient prepare a support system that will promote mental health on discharge from the hospital. This includes contacts with day treatment centers, employers, sources of financial aid, and landlords. Licensed clinical social workers undergo training in individual, family, and group therapies.
Counselors
Counselors prepared in disciplines such as psychology, rehabilitation counseling, and addiction counseling may augment the treatment plan by co-leading groups, providing basic supportive counseling, or assisting in psychoeducational and recreational activities
Occupational, recreational, art, music, and dance therapists
Based on their specialist preparation, these therapists assist patients in gaining skills that help them cope more effectively, gain or retain employment, use leisure time to the benefit of their mental health, and express themselves in healthy ways.
Medical advanced practice nurses, medical doctors, and physician assistants
Medical professionals provide diagnoses and treatments on a consultation basis. Occasionally, a medical professional who is trained as an addiction specialist may play a more direct role on a unit that offers treatment for addictive disease.
Mental health workers (mental health specialists/psychiatric technicians)
Mental health workers, including nursing assistants, function under the direction and supervision of registered nurses. They provide assistance to patients in meeting basic needs and also help the community to remain supportive, safe, and healthy.
Pharmacists:
In view of the intricacies of prescribing, coordinating, and administering combinations of psychotropic and other medications, the consulting pharmacist can offer a valuable safeguard. Physicians and nurses collaborate with the pharmacist regarding new medications, which are proliferating at a steady rate.
Milieu
a word of French origin (mi “middle” + lieu “place”) and refers to surroundings and physical environment. In a therapeutic context, it refers to the overall environment and interactions within that environment.
Ethics
the study of philosophical beliefs about what is right or wrong in a society
bioethics: 5 basic ethical principles
the study of specific ethical questions that arise in healthcare. The five basic ethical principles important to bioethics are:
1. Beneficence: The duty to act to benefit or promote the good of others
2. Autonomy: Respecting the rights of others to make their own decisions
3. Justice: The duty to distribute resources or care equally, regardless of personal attributes
4. Fidelity (nonmaleficence): Maintaining loyalty and commitment to the patient and doing no wrong to the patient (
5. Veracity: The duty to communicate truthfully
ethical dilemma
when there is a conflict between two or more courses of action, each carrying favorable and unfavorable consequences
Informal admission
the least restrictive of all admissions. It is similar to any general hospital admission in which there is no formal application. The person does not pose a substantial threat of harm to self or others. Under this model, the normal caregiver-patient relationship exists, and the patient is free to stay or leave, even against medical advice.
Voluntary admissions
when patients apply in writing for admission to the facility. The person must understand the need for treatment and be willing to be admitted (if the person is <16, guardian may have authority to apply on the person’s behalf)
Involuntary commitment
a court-ordered admission to a facility without the patient’s consent
standards:
Mentally ill
Posing a danger to self or others
Gravely disabled (unable to provide for basic necessities such as food, clothing, and shelter)
In need of treatment, and the mental illness prevents help-seeking on a voluntary basis
writ of habeas corpus
means a “formal written order” to “free the person.” The writ of habeas corpus is the procedural mechanism used to challenge unlawful detention by the government. The hospital must immediately submit the document to the court. The court must then decide if the patient has been denied due process of law. The person must be detained before being charged.
least restrictive alternative doctrin
mandates that care providers must take the least drastic action to achieve a specific purpose
Emergency commitment
a temporary admission or emergency hospitalization. Emergency commitment is used (1) for people who are so confused they cannot make decisions on their own or (2) for people who are so ill they need emergency admission
Assisted outpatient treatment
also known as court-ordered outpatient treatment and more than 20 other names throughout the United States. This type of involuntary outpatient commitment arose in the 1990s when states began to pass legislation that permitted court-ordered outpatient treatment as an alternative to forced inpatient treatment.
Conditional release
requires outpatient treatment for a specified period to determine if the patient follows the medication regimen, can meet basic needs, and is able to reintegrate into the community
Unconditional release
The termination of a patient-institution relationship. This release may be court-ordered or administratively ordered by the institution’s officials
Patients rights
right to treatment
right to refuse treatment
Right to Informed Consent
Rights Regarding Psychiatric Advance Directives
Designation of preferred physician and therapists
Appointment of someone to make mental health treatment decisions
Preferences regarding medications to take or not take
Consent or lack of consent for electroconvulsive therapy
Consent or lack of consent for admission to a psychiatric facility
Preferred facilities and unacceptable facilities
Individuals who should not visit
Rights Regarding Restraint and Seclusion
Rights Regarding Confidentiality
Duty to protect/duty to warn/ Tarasoff law
Duty to warn: an obligation to warn third parties when they may be in danger from a patient
Duty to protect: When a therapist determines that a patient presents a serious danger of violence to another, the therapist has the duty to protect that other person. In fulfilling this duty, the therapist may be required to call and warn the intended victim, the victim’s family, or the police or to take whatever steps are reasonably necessary under the circumstances.
The duty to protect usually includes the following:
Assessing and predicting the patient’s danger of violence toward another
Identifying the specific persons being threatened
Taking appropriate action to protect the identified victims
Tort Law
When a person wrongfully harms another, the injured party (the plaintiff) can seek money for damages from the responsible party (the defendant). We call this wrongful harm a tort.
Intentional tort: are willful or intentional acts that violate another person’s rights or property. Examples of intentional torts include assault, battery, and false imprisonment.
Unintentional tort: Negligence, malpractice
5 elements: Duty, Breach of duty, Cause in fact, Proximate cause, Damages
Aggression
an action or behavior that results in a verbal or physical attack. Aggression tends to be used synonymously with violence. However, aggression is not always inappropriate and is sometimes necessary for self-protection
Anger
an emotional response to frustration of desires, a threat to one’s needs (emotional or physical), or a challenge. It is a normal emotion that can even be positive when it is expressed in a healthy way
Violence
always an objectionable act that involves intentional use of force that results in, or has the potential to result in, injury to another person.
Deescalation techiniques
Maintain the patient’s self-esteem and dignity
Maintain calmness (your own and the patient’s)
Assess the patient and the situation
Identify stressors and stress indicators
Respond as early as possible
Use a calm clear tone of voice
Invest time
Remain honest
Determine what the patient considers to be needed
Identify goals
Avoid invading personal space; in times of high anxiety, personal space increases
Avoid arguing
Give several clear options
Use genuineness and empathy
Be assertive (not aggressive)
Do not take chances; maintain personal safety
Restraints
defined as “any manual method, physical or mechanical device, material, or equipment that immobilizes or reduces the ability of a patient to move his or her arms, legs, body, or head freely”
Seclusions
the involuntary confinement of a patient alone in a room, or area from which the patient is physically prevented from leaving”
Rather, the goal of seclusion is safety of the patient and others. Seclusion is less restrictive than restraint and may be helpful in reducing sensory overstimulation.
still considered a type of restraint
Alternative to restraints
Comfort rooms: voluntary isolation to manage destress/anxiety
Trauma-based care: focuses on the patient’s past experiences of violence or trauma and on the role these experiences currently play in their lives.
6 principles
safety
trustworthiness/transparency
peer support
collaboration/mutuality
empowerment, voice, choice
cultural, historical, and gender issues accounted for
Validation therapy
Telling the patient that her babies have grown up and there is no home to return to is not only cruel but nontherapeutic and will result in increased agitation. It is often more helpful to reflect back to the patient the feelings behind her demand and to show understanding and concern for her worry.
Social vs therapeutic communication
A social relationship is primarily initiated for the purpose of friendship, socialization, enjoyment, or accomplishment of a task. Mutual needs are met during social interaction.
In a therapeutic relationship, the nurse maximizes communication skills, understanding of human behaviors, and personal strengths to enhance the patient’s growth. Patients more easily engage in the relationship when the clinician’s interactions address their concerns, respect patients as partners in decision making, and use straightforward language.
Values
abstract standards and represent an ideal, either positive or negative
Peplau’s model of nurse-patient relationship
1. Preorientation phase begins with preparing for your assignment. The chart is a rich source of information including mental and physical evaluation, progress notes, and patient orders. You will probably be required to research your patient’s condition, learn about prescribed medications, and understand laboratory results.
Another task before meeting your patient is recognizing your own thoughts and feelings regarding this first meeting.
2. Orientation phase can last for a few meetings or extend over a longer period. It is the first time the nurse and the patient meet and is the phase in which the nurse conducts the initial interview
Specific tasks: Introductions, Establish rapport, Specifying a contract (contract, either stated or written, contains the place, time, date, and duration of the meetings.), Explaining confidentiality,
3. Working phase.
Specific tasks for the nurse in this phase include:
Gathering further data
Identifying problem-solving skills and self-esteem
Providing education about the disorder
Promoting symptom management
Providing medication education
Evaluating progress
Patient education
4. Termination phase is the final, integral phase of the nurse-patient relationship. You discuss termination during the first interview and again during the working stage at appropriate times
Goals:
Summarizing the goals and objectives achieved in the relationship
Discussing ways for the patient to incorporate into daily life any new coping strategies learned
Reviewing situations that occurred during the nurse-patient relationship
Exchanging memories, which can help validate the experience for both nurse and patient and facilitate closure of that relationship
Part of the termination process is to discuss the patient’s plans for the future. Registered nurses generally reinforce those plans and emphasize understanding of medications and recognizing when symptoms are getting out of control. Self-help groups can also be encouraged.
contract
emphasizes the patient’s participation and responsibility because it shows that the nurse does something with the patient rather than for the patient. The contract, either stated or written, contains the place, time, date, and duration of the meetings. You should also discuss termination of the relationship
Empathy vs sympathy
Empathy occurs when the helping person attempts to understand the world from the patient’s perspective.
In empathy, we understand the feelings of others, and in sympathy, we feel pity or sorrow for others. Although these are considered nurturing human traits, they may not be particularly useful in a therapeutic relationship.
Clinical supervision
mentoring relationship characterized by feedback and evaluation. Typically, students experience a gradual increase in autonomy and responsibility.
Counseling
a supportive face-to-face process that helps individuals problem-solve, resolve personal conflicts, and feel supported.
therapeutic encounter
informal and not extensive such as when the nurse and patient meet for only a few sessions. Even though it is brief, the relationship may be substantial, useful, and important for the patient
therapeutic use of self.
distinct gifts—unique personality traits and talents—that we can learn to use creatively to form positive bonds with others. The use of these gifts to promote healing in others
the communication process
Stimulus. One person has a need to communicate with another for information, comfort, or advice.
Sender. The person sending the message initiates interpersonal contact.
Message. The message is the information sent or expressed to another. The clearest messages are those that are well-organized and expressed in a manner familiar to the receiver.
Channel. The message can be sent through a variety of channels, including auditory (hearing), visual (seeing), tactile (touch), olfactory (smell), or any combination of these.
Receiver. The person receiving the message then interprets the message and responds to the sender by providing feedback.
Feedback that validates the accuracy of the sender’s message is extremely important.
Complementary relationship
One participant has more control.
the inequality decreases as the patient recovers and as the student progresses and graduates. Complementary relationships also exist based on social status, age or developmental differences, gender differences, and educational differences.
Verbal communication
consists of all the words a person speaks
Nonverbal behaviors/communication
may be sending the real message through. The tone of voice, emphasis on certain words, and the manner in which a person paces speech are examples of nonverbal communication.
Better indicator for feeling than verbal
Content/process
The verbal message is sometimes referred to as the content of the message (what is said)
the nonverbal behavior is called the process of the message (nonverbal cues a person gives to substantiate or contradict the verbal message).
double-bind messages
They are characterized by two or more mutually contradictory messages given by a person in power (the content and process do not match)
Therapeutic communication techniques
Using silence
Active listening - nurses fully concentrate, understand, respond, and remember what the patient is saying verbally and nonverbally.
Clarifying techniques
Paraphrasing - you restate the basic content of a patient’s message in different, usually fewer, words
Prefacing statements with a phrase such as “I’m not sure I understand” or “You seem to be saying…” helps the nurse to understand the message in what may be a bewildering mass of details
Restating - an active listening strategy that helps the nurse to understand what the patient is saying. It also lets the patient know he is being heard. Restating differs from paraphrasing in that it involves repeating the same key words the patient has just spoken
Reflecting - Reflecting may take the form of a question or a simple statement that conveys the nurse’s observations of the patient when discussing sensitive issues
The use of a question in response to the patient’s question is another reflective technique
Exploring - A technique that enables the nurse to examine important ideas, experiences, or relationships more fully is exploring.
Open-ended statements “tell me more about..”, “describe…”, or “give me an example...”
Questions
Open-ended questions - encourage patients to share information about experiences, perceptions, or responses to a situation
No yes or no answers
Close-ended questions - used sparingly, can give you specific and needed information
Yes or no answers
Projective questions - usually start with a “what if” to help people articulate, explore, and identify thoughts and feelings
The miracle question - a goal-setting question that helps patients to see what the future would look like if a particular problem were to vanish. You can use the miracle question to identify goals that the patient may be motivated to pursue.
Nontherapeutic Communication Techniques
Excessive Questioning - asking multiple questions (particularly closed-ended) consecutively or rapidly—casts the nurse in the role of interrogator who demands information without respect for the patient’s willingness or readiness to respond
Giving Approval or Disapproval
Giving advice
Asking “why” questions
The Clinical Interview
Preparing
Pace - permitting the patient to set the pace of the interview, no matter how slow or halting the progress may be
Setting - establish safety
Seating
Assuming the same height, either both sitting or both standing.
Avoiding a face-to-face arrangement when possible; a 90- to 120-degree angle or side-by-side position may be less intense, and patient and nurse can look away from each other without discomfort.
Providing safety and psychological comfort in terms of exiting the room. Do not position the patient between the nurse and the door, nor should you position yourself in such a way that the patient feels trapped in the room.
Avoiding a desk barrier between the nurse and the patient.
Introduction - tell the patient who they are, what the purpose of the meeting is, and how long and at what time they will be meeting with the patient. Ask the patient how he or she would like to be addressed. This question conveys respect and gives the patient direct control over an important ego issue.
Initiating the interview
Start with one open-ended question
Tactics to avoid
Argue with, minimize, or challenge the patient.
Give false reassurance.
Interpret to the patient or speculate on the dynamics.
Question or probe patients about sensitive areas they do not wish to discuss.
Try to sell the patient on accepting treatment.
Participate in criticism of another nurse or any other staff member.
Helpful guidelines
Speak briefly.
When you do not know what to say, say nothing.
When in doubt, focus on feelings.
Avoid advice.
Avoid relying on questions.
Pay attention to nonverbal cues.
Keep the focus on the patient.
Attending Behaviors: The Foundation of Interviewing
Eye contact
Body language involves two elements: kinesics and proxemics.
Kinesics is associated with physical characteristics such as body movements and postures
Proxemics refers to the study of personal space and the significance of the physical distance between individuals
Different culture to culture
Intimate distance in the United States is up to 18 inches and is reserved for those we trust most and with whom we feel most safe.
Personal distance (18 to 40 inches) is for personal communications such as those with friends or colleagues.
Social distance (4 to 12 feet) applies to strangers or acquaintances, often in public places or formal social gatherings.
Public distance (12 feet or more) relates to public space (e.g., public speaking). In public space, one may hail another, and the parties may move about while communicating
Voice quality - encompasses voice loudness, pitch, rate, and fluency.
Speaking in soft and gentle tones is apt to encourage a person to share thoughts and feelings, whereas speaking in a rapid, high-pitched tone may convey anxiety and create it in the patient.
Clinical Supervision and Debriefing
Debriefing refers to a critical conversation and reflection regarding an experience that results in growth and learning. Debriefing supports essential learning along a continuum of “knowing what” to “knowing how” and “knowing why.”
Process recordings - written records of a segment of the nurse-patient session that reflect as closely as possible the verbal and nonverbal behaviors of both patient and nurse
Cultural filters
A form of cultural bias or cultural prejudice that determines what we pay attention to and what we ignore.
These cultural filters provide structure for our lives and help us interpret and interact with the world. However, these filters also unavoidably introduce various forms of bias into our communication, because they are bound to influence our personal, professional, familial, and sociological values and interpretations
Cognitive Distortions
irrational thoughts based on misinterpretation and false assumptions
Interpersonal Relationship in Nursing
Peplav: based on sullivan’s interpersonal theory:
4 levels of anxiety
mild: day-to-day sense of awareness
moderate: heightened sense of alertness
severe: interferes with critical thinking and perceptual field is diminished, nearly all behavior is aimed to decrease anxiety
panic: overwhelmed, results in paralysis or hyperactivity, individuals can not communicate, function, or follow directions
Nursing process for violence
Assessment: history of violence, subjective questions, objective data (hyperactivity, increasing tension, anxiety, anger)
Diagnosis: nursing diagnosis - symptom management, example harm to others/self
Outcome identification: short and long-term goals for nursing diagnosis
SMART (specific, measurable, achievable, realistic/relevant, time)
Planning: knowlege self response to anger
Implement
Evaluate: effectiveness of interventions, was the assessment and diagnosis accurate? were goals met? etc.
Stages of violence
Pre-assaultive - intervention: de-escalation techniques
Assaultive - intervention: medication, restraint, seclusion
seclusion, least restrictive - first
Post-assaultive - intervention: restraint, seclusion
plan reintegration: gradual, structured
Debrief/staff analysis: What went well? What could have gone better?
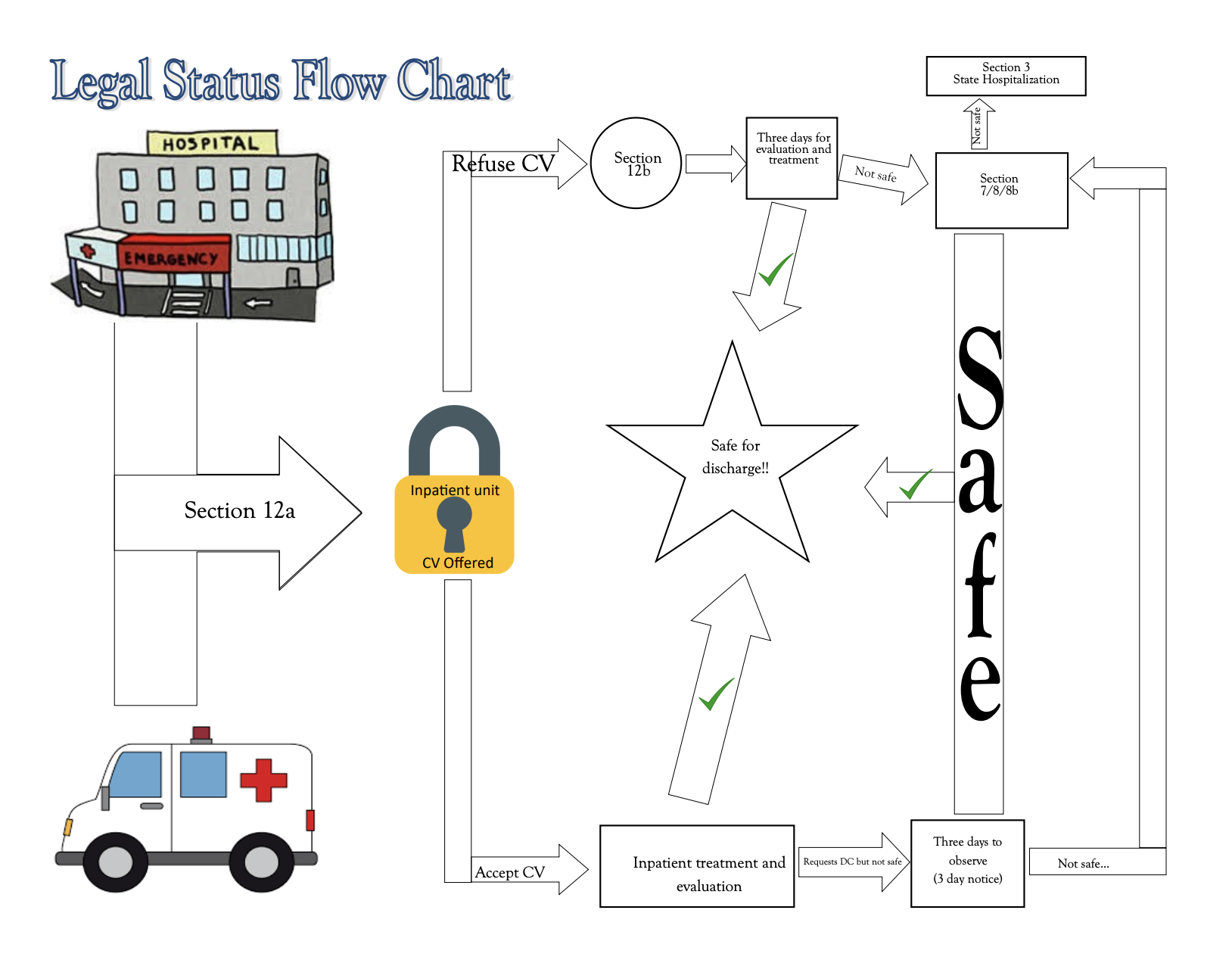
Sectioning (section 12a/12b, 7, 8/8b, 10, 11)
section 12a: transportation to hospital → section 12b: evaluation
If you sign a CV (conditional voluntary, section 10/11) (to sign, you must be oriented x3), you will be evaluated, and if ur “okay,” you are released.
If they feel you need to stay in the hospital, you can submit a 3-day notice (you want to be discharged in 3 days) → evaluation determines if you can leave
After 3 days, you are either released, or section 7, 8/8b will allow the hospital to hold you
If you do not sign the CV, you will be evaluated for 3 days and either hospitalized (section 7, 8/8b) or let go