Pathology - Chest/Abdomen (Unit 1-2)
1/93
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
94 Terms
CXRs are used to verify the proper placement of what internal devices?
Endotracheal tube
Central venous catheter
Swan-Ganz catheter
Transvenous cardiac pacemaker
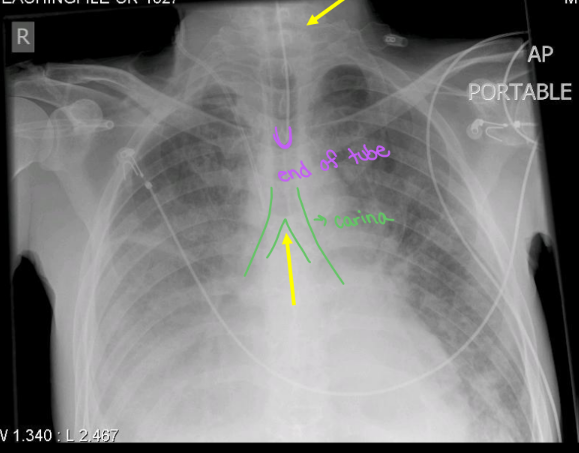
Placement and purpose of the Endotracheal Tube (ET):
Keeps airway open if obstruction or respiratory failure.
End of tube 5-7 cm above carina
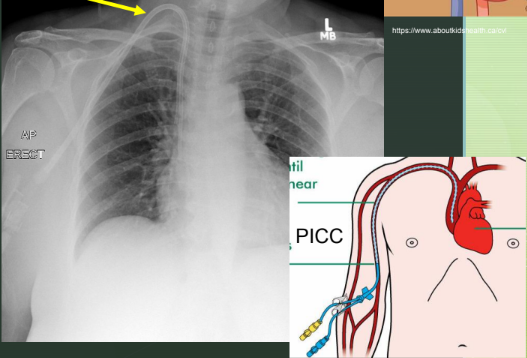
Placement and purpose for Central Venous Catheter:
Rapid infusion of fluids, nutrition, drugs, dialysis over a long period of time.
Measures central venous pressure (CVP)
Placement in internal jugular vein, subclavian vein, and common femoral vein.
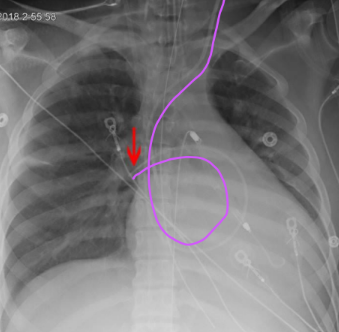
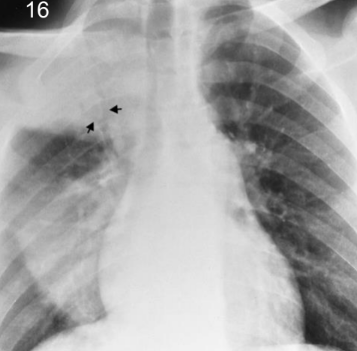
Placement and purpose for Swan-Ganz Catheter:
Monitors heart function and blood flow. Cardiac output and CVP
Positioned in R or L main pulmonary artery, with the tip not extending beyond the medial lung field
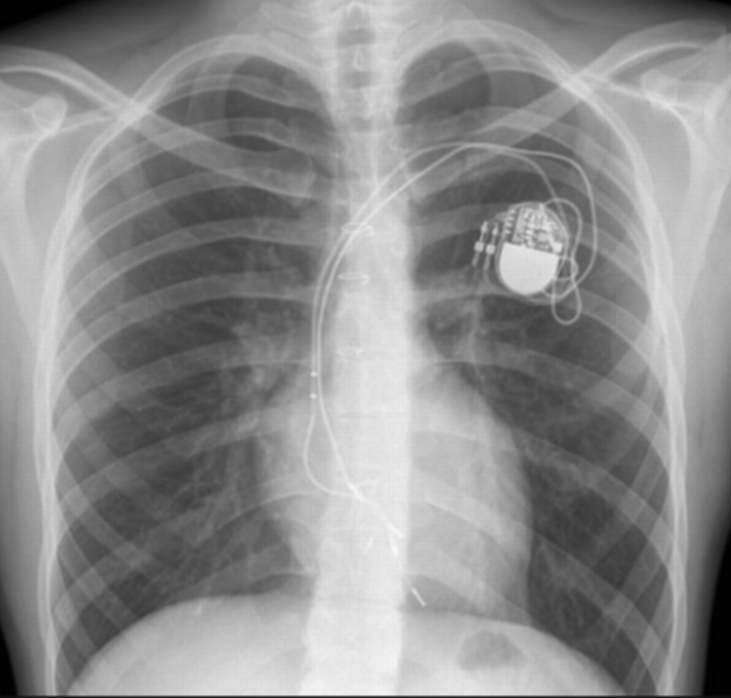
Placement and purpose for Transvenous Cardiac Pacemaker:
Maintain cardiac rhythm
Tip of pacemaker electrode should be positioned at the apex of right ventricle
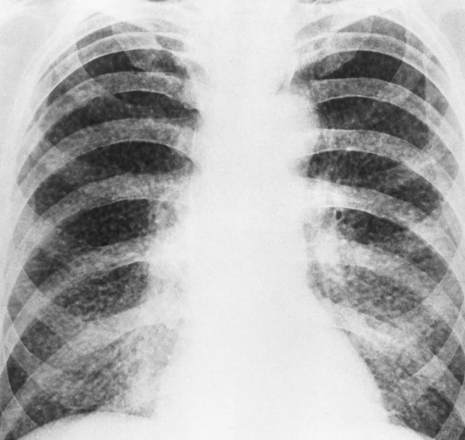
Cystic Fibrosis
Secretion of excessively viscous (thick) mucus causing severe damage to the lungs, digestive system, and other organs.
What is the typical life expectancy for individuals with cystic fibrosis?
30-40 years
Cystic Fibrosis: Additive or Destructive?
Additive condition - increase kVp
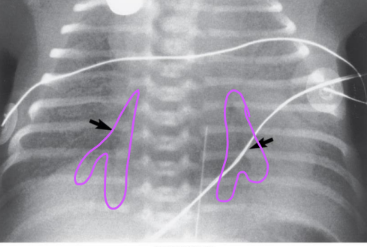
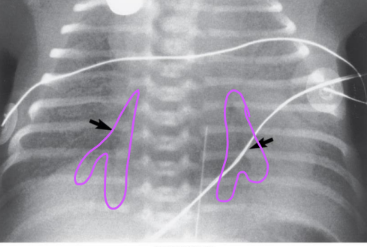
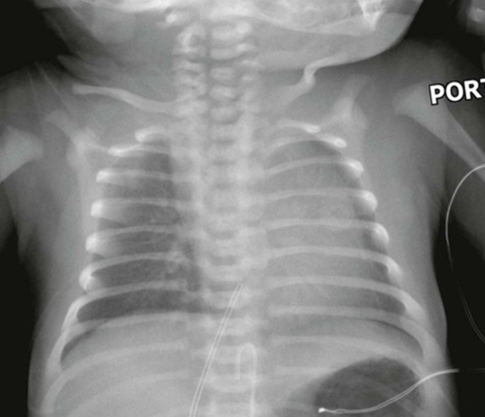
Hyaline Membrane Disease
Idiopathic respiratory distress syndrome is caused by lack of surfactant (lubricant) in immature lungs. In premature newborns.
Hyaline Membrane Disease: Additive or Destructive?
No exposure factor change necessary
Hyaline Membrane Disease looks like on XR
Air bronchogram (spiderweb air pocket)
COPD (Chronic Obstructive Pulmonary Disease)
Chronic obstruction of the airways leads to an ineffective exchange of respiratory gases and makes breathing difficult.
What are the two most common types of COPD?
Chronic bronchitis
Emphysema
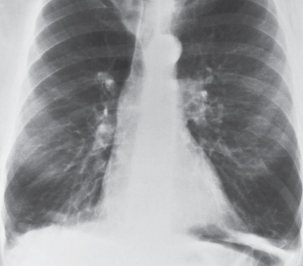
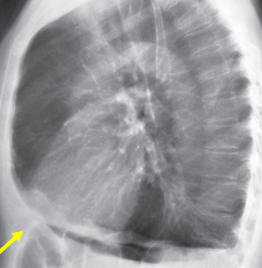
Emphysema
Distension of the distal air spaces as a result of the destruction of alveolar walls and obstruction of small airways.
Emphysema: Additive or Destructive?
Destructive - decrease mAs
Emphysema looks like on XR
Severe overinflation of lungs along with flattening and even a superiorly concave configuration of the hemidiaphragms.
Chronic Bronchitis
Excessive tracheobronchial mucus production leading to the obstruction of small airways.
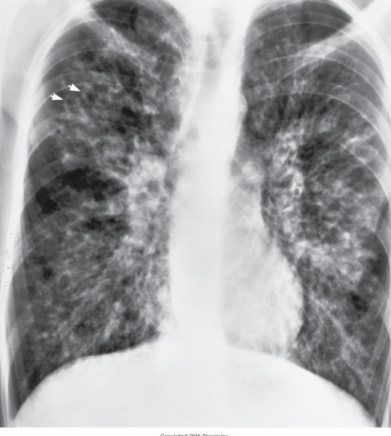
Tuberculosis (TB)
Lung disease caused by bacteria and spreads via droplets in the air; no longer prevalent in the US
Latent and Active

Active TB
Infectious; chest pain, SOB, coughing. Curable
Latent TB
No symptoms, not infectious, ticking time bomb
Active TB: Additive or Destructive?
Additive - increase kVp
Pneumoconiosis
Inhaled irritants retained permanently in the alveolar sacs causing irreversible damage.
Silicosis
Asbestosis
Anthracosis
Silicosis
Most common form of pneumoconiosis, caused by silica quartz dust in mining/sandblasting
Asbestosis
Pneumonconiosis caused by inhlation of asbestos in manufacturing.
Anthracosis
Pneumoconiosis caused by inhalation of anthracite (coal) dust.
Pneumoconiosis: Additive or Destructive?
No exposure factor change necessary
Pneumonia
Inflammation of the lung caused by bacteria and viruses
Viral - both sides of lungs
Bacterial - one side of lungs
What are the three types of pneumonia radiographic patterns?
Alveolar, or air-space, pneumonia
Bronchopneumonia
Interstitial pneumonia
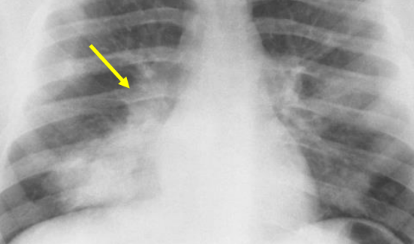
Alveolar Pneumonia
Homogenous consolidation of right lung with associated bronchograms. Bacterial. Inflammatory condition
Bronchopneumonia
Ill-defined consolidation at right base. Bacterial
Interstitial Pneumonia
Diffuse infiltrate; air space consolidation obscures heart border. Viral

Atelectasis
Complete or partial collapse of the entire lung caused by bronchial obstruction.
Atelectasis: Additive or Destructive?
Additive
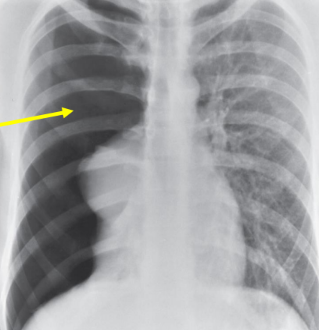
Pneumothorax
Air in the pleural cavity resulting in partial or complete collapse of the lungs.
What are the causes of a Pneumothorax?
Rupture of a subpleural bulla (air pockets)
Spontaneous event
Trauma
Iatrogenic causes
Pneumothorax: Additive or Destructive?
Destructive
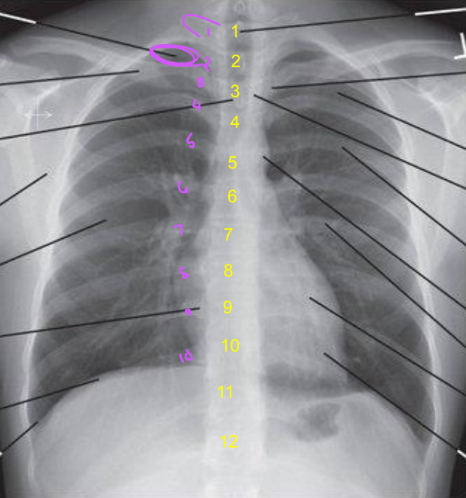
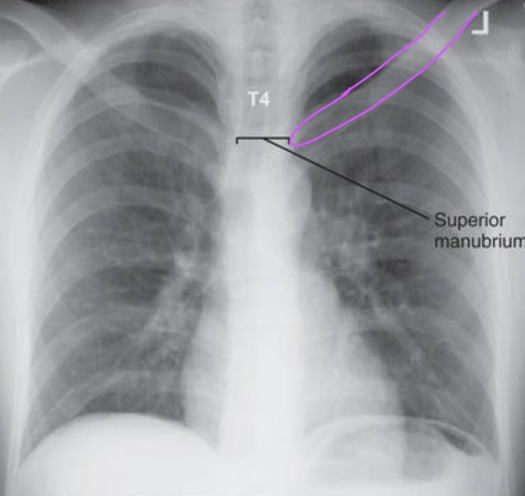
PA Chest: Image Criteria
Manubrium superimposed by T4
1” of apices above clavicles
PA Chest Tilted Forward/Anteriorly
Lungs and heart are foreshortened
Vertical clavicles
Manubrium at T5 or lower
More than 1” of apices
Ribs are more curved
Upper MCP was tilted toward IR
PA Chest Tilted Backwards/Posteriorly
Lungs and heart are foreshortened
Horizontal clavicles
Manubrium at T1-3
Less than 1” of the apices
Ribs are more horizontal
MCP titled away from IR
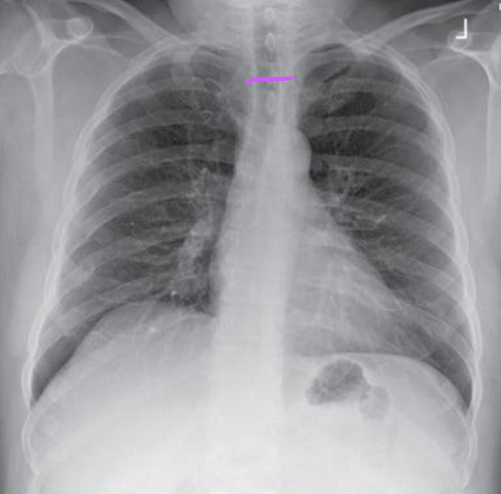
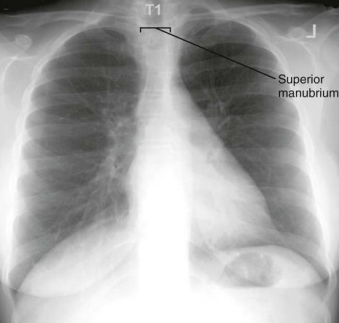
PA Chest: Is this Image Good?
Manubrium is at T1
Patient was tilted backwards. Bring pt towards IR.
Did not get all 10 ribs
Have patient do a deeper inspiration
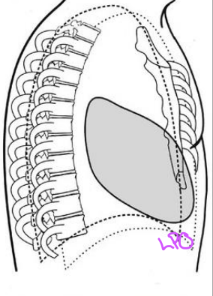
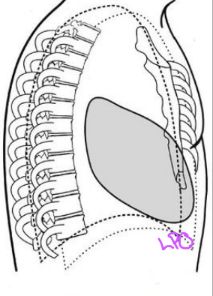
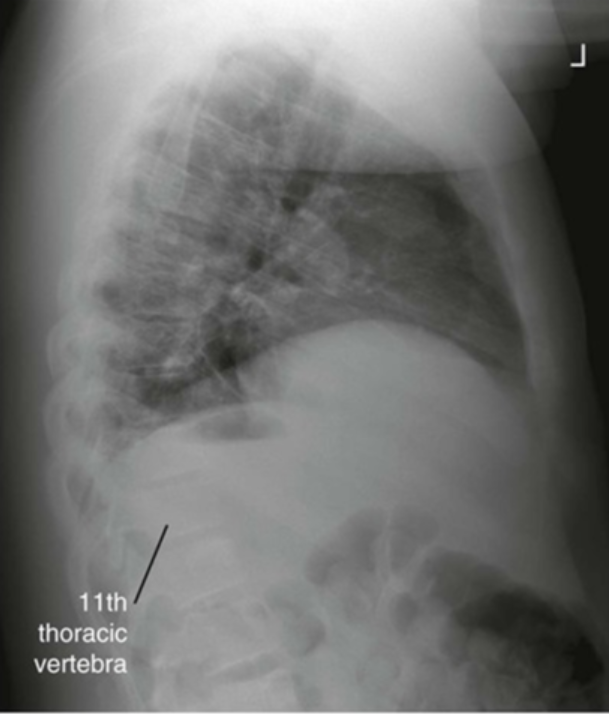
Distinguishing R and L lungs on Lateral Chest
Gastric bubble
Lung tissue
Heart Shadow
What position shifts the heart to superimpose the sternum anteriorly?
LPO
What position shifts the left lung toward the anterior direction?
LPO
What position demonstrates the left lung more anterior to sternum on image?
Describes an LPO position, but the left lung does not get demonstrated due to OID
What position shifts the heart posterior to the sternum?
LAO
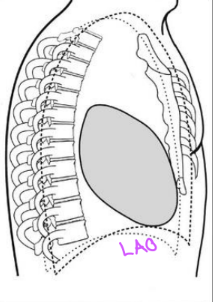
What position demonstrates the right lung more anterior to sternum on image?
LAO
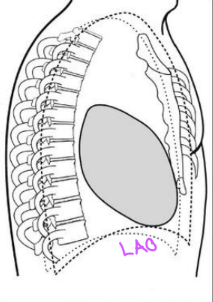
What position shifts the right lung more toward the anterior direction?
LAO
How much do ribs need to be separated on a lateral CXR for a correction to be necessary?
Greater than 0.5”
A left lateral chest xray demonstrates the right and left ribs separated about 0.25". what caused this and how should it be fixed?
Caused by rotation; however, no fix necessary because it is less than 0.5”.

Lateral Chest: Is this Image Good?
R and L ribs are separated >0.5” (span of finger)
Humeral soft tissue obscures anterior lung apices
Raise arms until humeri are vertical
Do not see any anterior lungs which means patient is in an LPO
Rotate patient’s right thorax anteriorly
Lateral Chest: Is this Image Good?
Need 10 ribs for good inspiration
Make the patient take a deeper inspiration and make sure to expose on second inspiration.
An AP CXR requires ______ angle to prevent clavicles from obscuring the apices.
± 5 degree caudad
CR perp. to sternum

AP Chest: Is this Image Good?
Poor inspiration
Patient needs to do a deeper inspiration
Clavicles are too vertical
Depress the shoulders

AP Chest: Is this Image Good?
<1” of apices
Posterior ribs are horizontal
CR was angled cephalically
Adjust so the angle is caudad
AP Chest: Is this Image Good?
Left clavicle is foreshortened
Left SC joint is farther from vertical column
Left side posterior ribs are longer than the right
Head and body are rotated to the left
Rotate left side away from the IR
Describe how the position of the SC joints can indicate the direction of rotation in a poorly positioned AP CXR
LPO - Left SC joint is farther from vertebral column. Right SC superimposed
RPO - Right SC joint is farther from vertebral column. Left SC superimposed
PA CXR SC Joints
RAO - Right SC joint is closer to midline than left
LAO - Left SC joint is closer to midline
If the left SC joint is demonstrated farther from the vertebral column than the right joint, the pt is rotated ____?
LPO/LAO
If the right SC joint is demonstrated farther from the vertebral column than the left joint, the pt is rotated ____?
RPO/RAO
Peritoneum
Double-walled sac that lines the abdominal cavity and covers organs (parietal and visceral).
Parietal Peritoneum
Along the abdominal wall
Visceral Peritoneum
Covers the organs
Peritoneal Cavity
Cavity contains serous fluid
Ascites
Abnormal accumulation of fluid in the peritoneal cavity of the abdomen
Displaces the bowel centrally

Ascites: Additive or Descructive?
Additive - increase kVp
Causes of ascites
Cirrhosis of the liver
Metastatic disease to the peritoneal cavity
May be treated with diuretics, drainage
Pneumoperitoneum
Free air in the peritoneal cavity
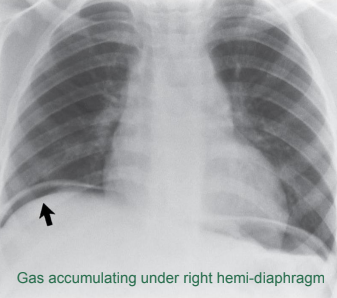
Causes of pneumoperitoneum
Perforation of a gas-containing viscus (intestine)
Pneumoperitoneum: Additive or destructive?
Destructive
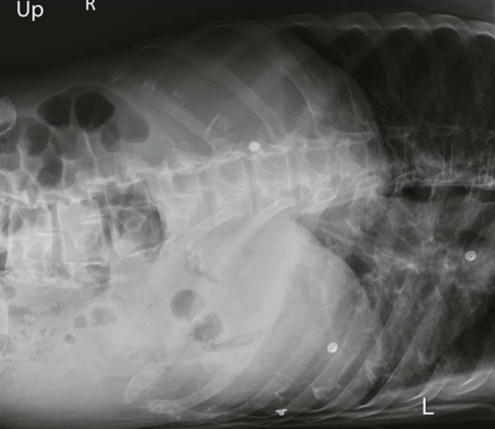
What should you do if the patient cannot stand for the abdominal XR and you need to see air-fluid levels?
Do a Left Lateral Decub
Peritonitis
Redness and swelling (inflammation) of the lining of the peritoneum.
What can typically cause Peritonitis?
An infection from a hole in the bowel or a burst appendix.
Dynamic or Mechanical Bowel Obstruction
Partial or complete blockage in the intestine due to adhesions or foreign body
Can happen anywhere in the intestinal tract, but common in small bowel
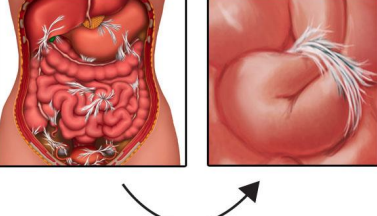
Fibrous adhesions
Fibrous band of tissue interrelates with the intestine, creating a blockage
Most common cause of mechanically based obstruction
Distended loops of air-filled small intestine
Fibrous Adhesions: Additive or Destructive?
Destructive
Ileus (Non-mechanical obstruction): Additive or Destructive?
Destructive
Ileus
Non-mechanical obstruction involving large amounts of air, often resolves within 1-3 days. Common for post-op patients.
Adynamic ileus
Occurs more often than mechanical bowel obstruction
Common disorder of intestinal motor activity
Fluid and gas do not progress normally

Factors that impede intestinal motility:
Neural
Hormonal
Metabolic
Causes of Adynamic ileus:
Peritonitis
Medications that decrease intestinal peristalsis
Electrolyte and metabolic disorders
Trauma
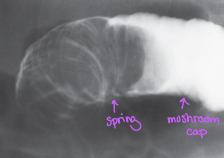
Intussusception
Telescoping of one part of the intestinal tract into another because of peristalsis
Common in children
Air-filled “coiled spring” appearance
Intussusception: Additive or Destructive?
Destructive
Volvulus
Twisting of a loop of intestine, which creates and obstruction
Bird’s beak appearance
Common sites: Cecum and Sigmoid
Ischemia and necrosis is a concern

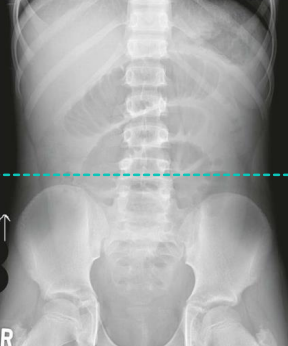
AP Abdomen: Image Criteria
T12 to pubic symphysis
L4 at center (iliac crest)
Psoas muscles

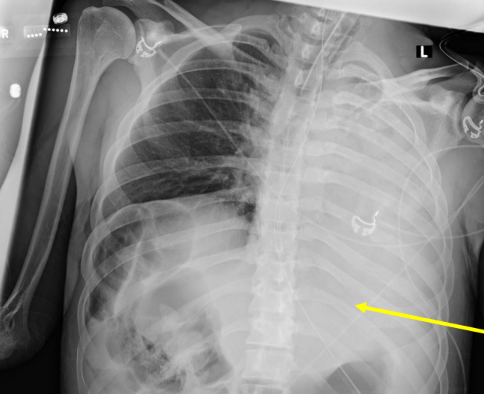
Where should a Nasogastric Tube end?
Tip should be visible at least 10 cm (4”) beyond the gastroesophageal junction. In LUQ.
What is the purpose of NG tubes?
Used for feeding or removal of gas/secretions by suction (decompression).
Patient should be upright for to ______ minutes before taking images to allow ______ to move away from the abdominal structures and rise to levels of diaphragms.
5-20 minutes
Air
Abdominal Breathing Instructions
First expiration
Full expiration: T8-9
Full inspiration: T12
The diaphragm can move as much as ___ inches from full inspiration to expiration.
4

KUB: Is this Image Good?
Not centered to iliac crests; missing pubic symphysis.
Do a bladder shot or center CR 1 inch lower
Upright Abdomen: Is this Image Good?
Domes of diaphragm not included
CR centered too low
Bring the CR higher - 2” above crests
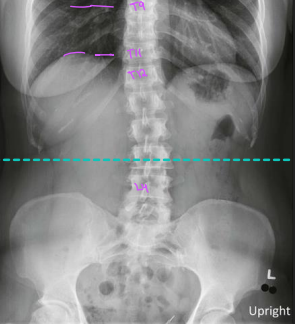
Upright Abdomen: Is this Image Good?
Diaphragm is at T11; full inspiration
Diaphragm should be at T9; full expiration
CR is good
Left Lateral Decub: Is this Image Good?
Left ribs are elongated indicating LPO position
Rotate right side back toward IR
CR is too high
Center CR 2” above crests
On abdomen XRs what does it look like when patient is improperly obliqued?
LPO - Left ribs elongated, left iliac wing is wider
Rotate right side back to IR
RPO - Right ribs elongated, right iliac wing is wider
Rotate left side back to IR