MSK growth injury & repair - ligament, tendons and bone
1/48
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
49 Terms
what are ligaments
dense bands of collagen that span a joint
Anchored to the bone at either end
Joint stability through range motion
Different portions ligament tensioned at different joint positions
what is the function of ligaments
provide stability and connect bone to bone
what type of collagen fibres do ligaments have
type 1
what are found within ligaments - why
fibroblasts - communication
sensory fibres for proprioception, stretch and sensory
Vessels (surface)
Crimping - allow stretch
why are ligaments different to tendons
lower % collagen
higher % proteoglycans and water
less organised collagen fibres
rounder fibroblasts
what is the most commonly injured ligament
ACL
lateral ligament in ankle
when does a ligament rupture
force exceeds strength of ligament
Expected
Unexpected (position/muscle)
Rate load
Complete vs incomplete
Stability of joint affected
Proprioception loss
how does ligament healing occur
haemorrhage
proliferative phase
remodelling

haemorrhage in ligament rupture
blood clot
resorbed
replaced with heavy cellular filtrate
hypertrophic vascular response
proliferative phase of ligament rupture
production of scar tissue
disorganised collagenous connective tissue
remodelling phase of ligament rupture
matrix becomes ligament life
differences in composition, architecture and function
when is conservative/non-operative treatment used for ligament injuries
partial rupture
no instability
poor surgery candidate
when are ligament injuries operated on
joint instability
expectation/functional demands e.g. athlete
compulsory - multiple ruptures
what is the function of tendons
Connect muscle to bone
allow flexibility
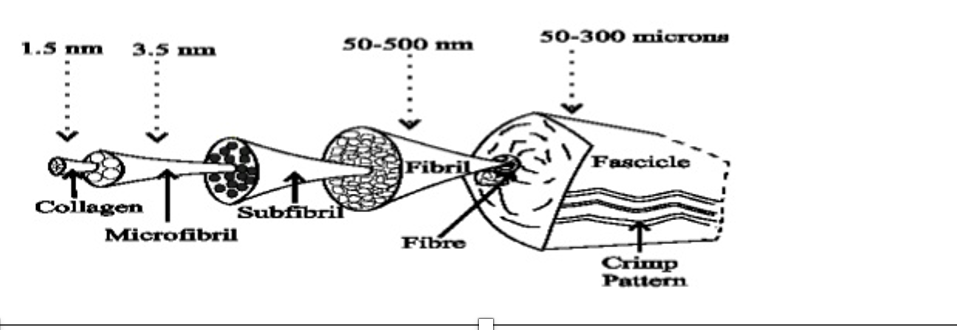
how are tendons arranged structurally
longitudinal arrangement of cells (tenocytes) and type 1 triple helix collagen fibres
- collagen = fascicles of long narrowing bundles
- collagen covered by endotenon
- fascicles covered by paratenon
- tendon covered by epitenon
blood supply to tendons
vinculim - fine network of blood vessels in paratenon
what are tendon sheaths
elongated bursa that wraps around a tendon
- thickenings form strong pulleys
what does immobility cause in tendons
reduced water content and glycosaminoglycan concentration and strength
types of tendon injuries
degeneration
inflammation
esenthesiopathy
traction apophysitis
avulsion +/- bone fragment
tear - intra substance = rupture
tear at musculotendinous junction
laceration/incision
crush
ischaemic
nodules
most commonly degenerated tendon
achilles
intrasubstance mucoid degeneration
achilles tendon degeneration symptoms
could be asymptomatic
swollen painful tender tendon
potential precursor to rupture
inflammation of tendon
tendonitis
what is de Quervain's tenovsynovitis + symptoms
tendons of extensor pollicis brevis and abductor pollicis longus through common tendon sheath at radial aspect of wrist
- swollen tender hot red joint
- positive Finklesteins test
what is ethesiopathy
inflammation at bone insertions
- muscle/tendon usually at muscle origin rather than tendon insertion e.g tennis elbow
- ligament - plantar fasciitis
example of traction apophysitis
Osgood Schlatter disease
what is Osgood Schlatter disease
Rupture of the growth plate at the tibial tuberosity from stress on patellar tendon - common in adolescent active boys
recurrent load, inflammation
what is avulsion +/- bone fragment
failure at insertion with load exceeding strength while muscle is contracting
- mallet finger is common
treatment of avulsion +/- bone fragment
conservative
stack splint - limited application due to retraction tendon
operative
- reattachment of tendon through bone
- fixation of bony fragment
mechanisms of tendon rupture
intrasubstance rupture
pushing off with weight bearing forefoot while extending knee joint e.g. sprint starts or jumping
unexpected dorsiflexion of ankle - slipping into hole
violent dorsiflexion of plantarflexed foot - fall from height
achilles tendon rupture test findings
positive Simmonds test
palpable tender gap
absent/limited active plantar flexion
what is musculotendinous junction tear
junction between muscles tendon tears often partial tear
•E.g. tear at the junction between the medial head of gastrocnemius and the Achilles tendon
when would you do non operative vs operative treatment in intrasubstance tendon rupture
conservative
- where ends can be opposed - mobilise, splint/cast
- where healing will occur - not intra-articular tendons
operative
- when high risk of re-rupture
- high functional demand patient
- ends cannot be opposed
common tendons that are lacerated and treatment of this
finger flexors - FDS, FDP
early surgical repair
long bone anatomy
diaphysis - shaft
epiphysis - on joint side of physis
metaphysis - flare at end of shaft
physis - growth plate
medullary canal

apophysis
where tendons/ligaments attach
what is a fracture
break in the structural continuity of bone
types of bone
cortical - diaphysis, less biologically active
cancellous - metaphysis, site of longitudinal growth at the physis, very biologically active
why do bones fail
high energy transfer in normal bones
repetitive stress in normal bones - stress fracture
low energy transfer in abnormal bones - osteoporosis, osteomalacia, metastatic tumour other bone disorders
fracture biology
•Mechanical and structural failure of bone
•Disruption of blood supply
•Regenerative process
•No scar
Four stages
what are the 4 stages of fracture healing
inflammation
soft callus
hard callus
bone remodelling
inflammation stage 1 of fracture healing
begins immediately
- haematoma and fibrin clot
- platelets, PMN's, neutrophils, monocytes and macrophages
- by-products of cell death - lysosomal enzymes
- fibroblasts
- mesenchyymal and osteprogenitor cells - transformed endothelial cells, osteogenic induction of cells from muscle and soft tissues
- angiogenesis - macrophages
factors affecting stage 1 of fracture healing - inflammation
NSAIDs
Loss of fracture haematoma
•Open fractures
•Surgery
Extensive soft tissue damage
•Leads to poor blood supply
soft callus stage 2 of fracture healing
begins when pain and swelling subsides
lasts until bony fragments are united by cartilage or fibrous tissue
some stability of fracture
angulation can still occur
continued increase in vascularity
stage 3 hard callus of fracture healing
conversion of cartilage to woven bone
typically long bone fracture
increased rigidity - obvious callus on imaging
bone remodelling stage 4 of fracture healing
conversion of woven bone to lamellar bone
medullary canal reconstituted
bone responds to loading characteristics - Wolffs law
delayed union vs non union
delayed union = failure to heal in expected time
non union = failure to heal
what cases delayed union
high energy injury
distraction - increased osteogenic jumping
instability
infection
steroids
immunosuppressant
NSAIDs
warfarin
ciprofloxacin
smoking
what causes non-union
failure of calcification fibrocartilage
instability - excessive osteoclasts
abundant callus formation
pain + tenderness
persistent fracture line
sclerosis
if there is delayed bone healing what do you need to do
consider alternative management
- different fixation
- dynamisation
- bone graft