9. PKPD of ARVs
1/46
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
47 Terms
Does PK or PD describe ADME?
PK: The study of how the body affects the drug
What is PD?
How the drug affects the body. e.g. drug concentration —> response?
What is PG (pharmacogenomics?)
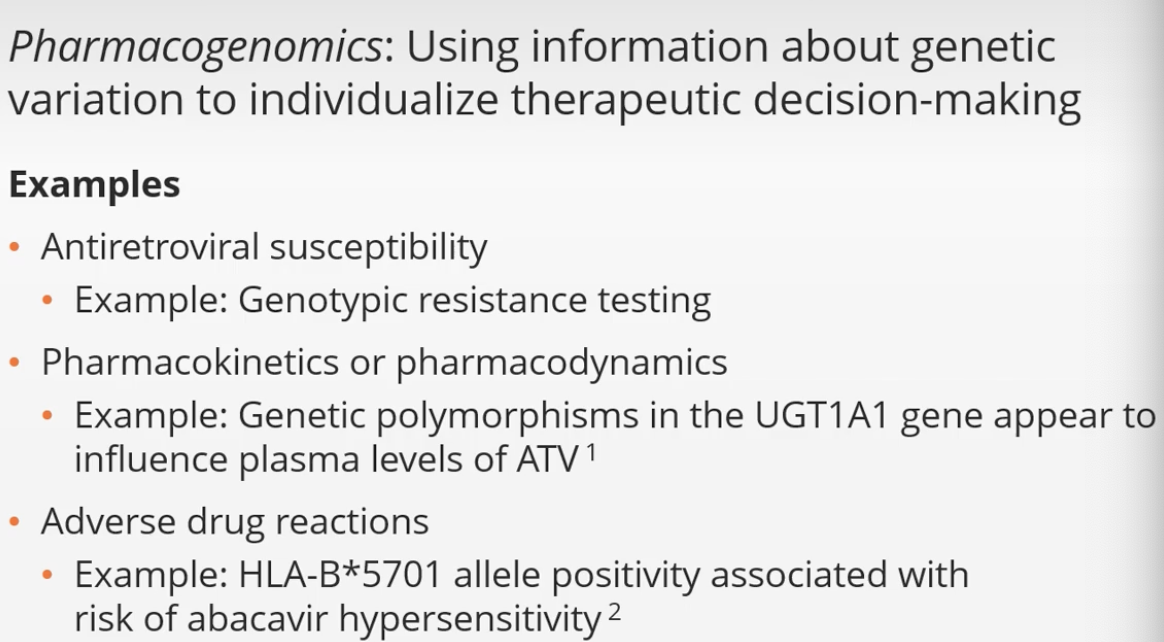
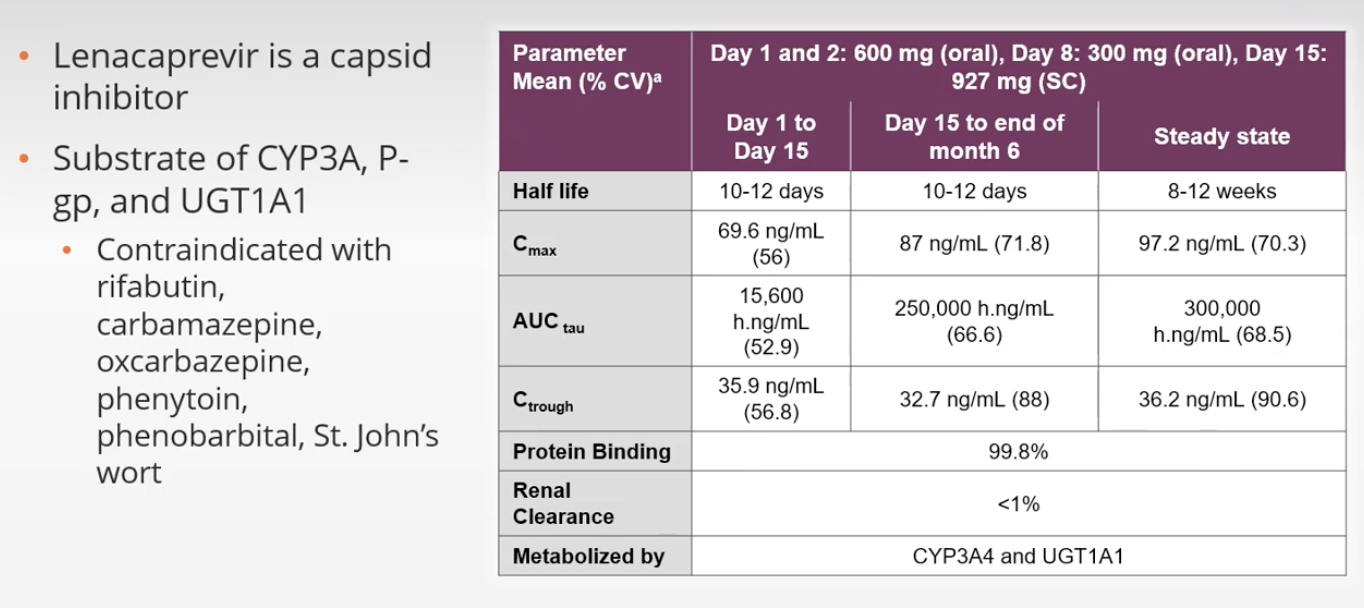
Polymorphisms in UGT1A1 gene appear to influence plasma levels of what ARV drug?
Atazanavir
What ARVs are the only IVs?
Zidovudine (AZT/ZDV) and Ibalizumab (IBA)
What are the only ARV available as SQ?
Enfurvitide (ENF/T-20), Lenacapavir (LEN)
What ARVs are available as IM?
LA RPV/CAB gluteal Q1-2M
What factors affect drug absorption?
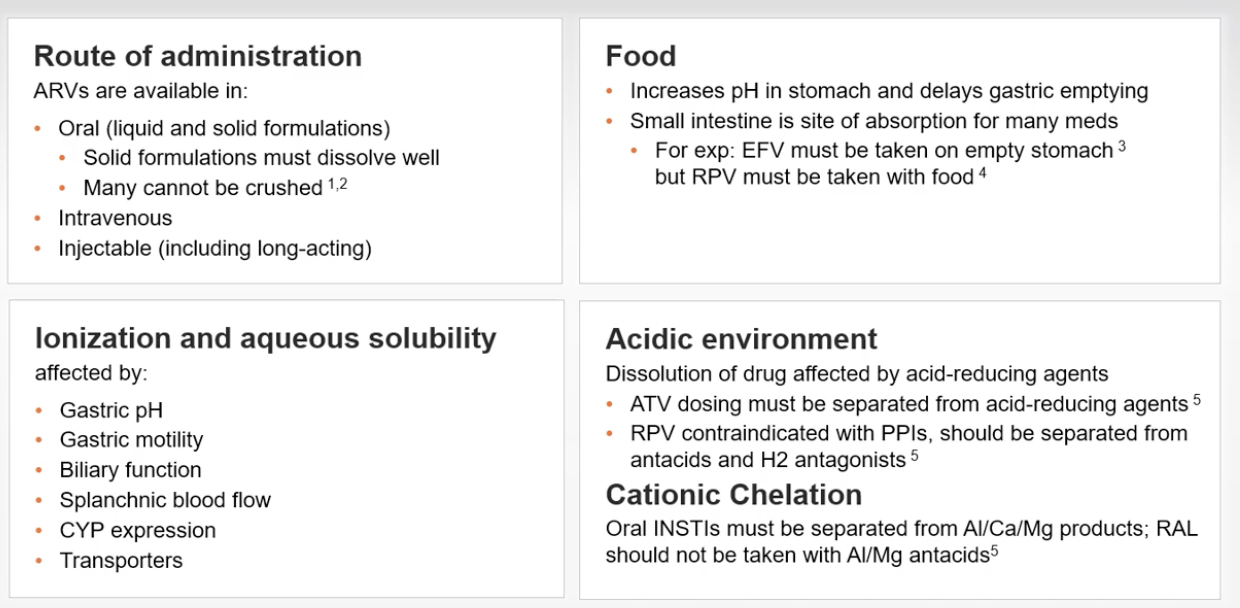
What is the effect of food on gastric pH?
Increases pH in stomach (lowers acid) immediately upon ingestion, acting as a buffer that makes the stomach contents less acidic (e.g., rising from pH 1 to over 4.5). This effect is temporary, as the meal subsequently stimulates gastric acid secretion, which eventually lowers the pH back to highly acidic levels over the next 3-4 hours
It also delays gastric emptying
What ARV(s) must be taken on an EMPTY stomach? and why?
Efavirenz (EFV) (high fat increases absorption —> toxicities)
What ARV(s) must be taken WITH FOOD?
NNRTI: RPV Rilpivirine (H2RAs 12 hours before or 4 hours after / Antacids 4 hours before or 2 hours after RPV. PPIs CId) (500+ calories, fat)
PI: ATV/b, DRV/b
INSTI: EVG/b
If RPV absorption is reduced by antacids (i.e. it needs acidic environment), then why does taking it with a meal help absorption? I thought meals initially alkalinize gastric pH?
Rilpivirine (RPV) absorption is indeed highly dependent on an acidic environment (low pH) to dissolve properly, and taking it with a meal helps because it relies on the secondary drop in gastric pH after the initial rise from eating a meal. That significant drop in pH later on, is what facilitates RPV absorption and dissolution.
What ARVs are either CId or must be separated from antacids?
Rilpivirine (RPV) - Separate from H2RAs/antacids. NO PPIS AT ALL. (TAKE WITH FOOD)
ATV - Separate from H2RAs/antacids/PPIs. Needs highly acidic environment
What ARVs must be separated from Cations?
[Mg+/Al+/Ca+/Fe+]
Oral INSTIs (they chelate to these)
RAL completely CId with any Al+/Mg + products (Calcium ok with caveats)
Per DHHS, Cation supplements/laxatives must be taken 2 hours after INSTIs or 6 hours before INSTIs
OR alternatively, INSTIs and cation supplements can be taken simultaneously with food.
This is because food inhibits the chelation process in the stomach
RAL completely CId with any Al/Mg products/supplements. Calcium carbonate antacids (tums) MAY be taken with RAL under what circumstances?
BID RAL is okay with calcium carbonate antacids
RAL 400mg BID (yes)
RAL 1200mg QD (no)
Which ARVs must be taken with regards to food and/or PPIs?
Efavirenz EFV - EMPTY stomach
Rilpivirine (RPV) - WITH FOOD (500cal or more) Separate from H2RAs/antacids. NO PPIS AT ALL.
ATV - SEPARATE from acid-reducing agents
ORAL INSTIs: Separate from cations (Al/Ca/Mg) products, RAL CId with Al/Mg products
Which one: Kaletra tablets or solution needs to be taken with food?
Oral solution requires food for proper absorption. Tablets can be taken with/without food.
ARV tablets/capsules you cannot crush or open?
Kaletra tablets: Crushing tablets significantly reduces exposure to both components by around 50% vs. swallowing whole. Should be given in solutions.
Proteins in the blood: Albumin binds ____ drugs. Alpha 1 Glycoprotein binds _____ drugs.
Albumin binds ACIDIC drugs
A1GP binds BASIC drugs
ARV Drugs that have this property may improve neurocognitive HIV deficits?
Drugs with better CNS penetration
What is an HIV “sanctuary site”?
A compartmentalized area where HIV can undergo viral replication with higher potential to select for RAMs due to suboptimal drug penetration into that specific site. Such as male/female genital track and CNS.
What score categorizes ARVs by CNS penetration?
“CPE” scores
CNS Penetration-Effectiveness Score
Rates ARVs 1(low CNS) to 4 (high CNS)
What ARVs have high CPE score of 4?
AZT, NVP, IND/r, DTG
Other than Liver, where else are CYP enzymes found?
INSTESTINES
also, to lesser extent, in smooth endoplasmic reticulum of cells throughout the body
Ritonovir and Cobi inhibit which CYP?
CYP3A4
Which ARVs is COBI FDA approved to boost?
EVG/ATV/DRV
Which is more selective to CYP3A4 and thus has less potential for off-target DDIs? Cobi vs. RTV?
COBI
Do both COBI and RTV have anti-HIV activity?
NO. only RTV. and 100mg booster dose is considered subtherapeutic.
What PK parameter do RTV/Cobi primarily enhance, and how is this beneficial?
Primarily enhance TROUGH levels of ARVs which reduces the risk of selection of RAMs
Also:
Minimizes need for food requirements and
reduces DDIs with inducers of CYP3A4.
reduced dosing frequency
increased forgiveness with missing doses (increased barrier to resistance)
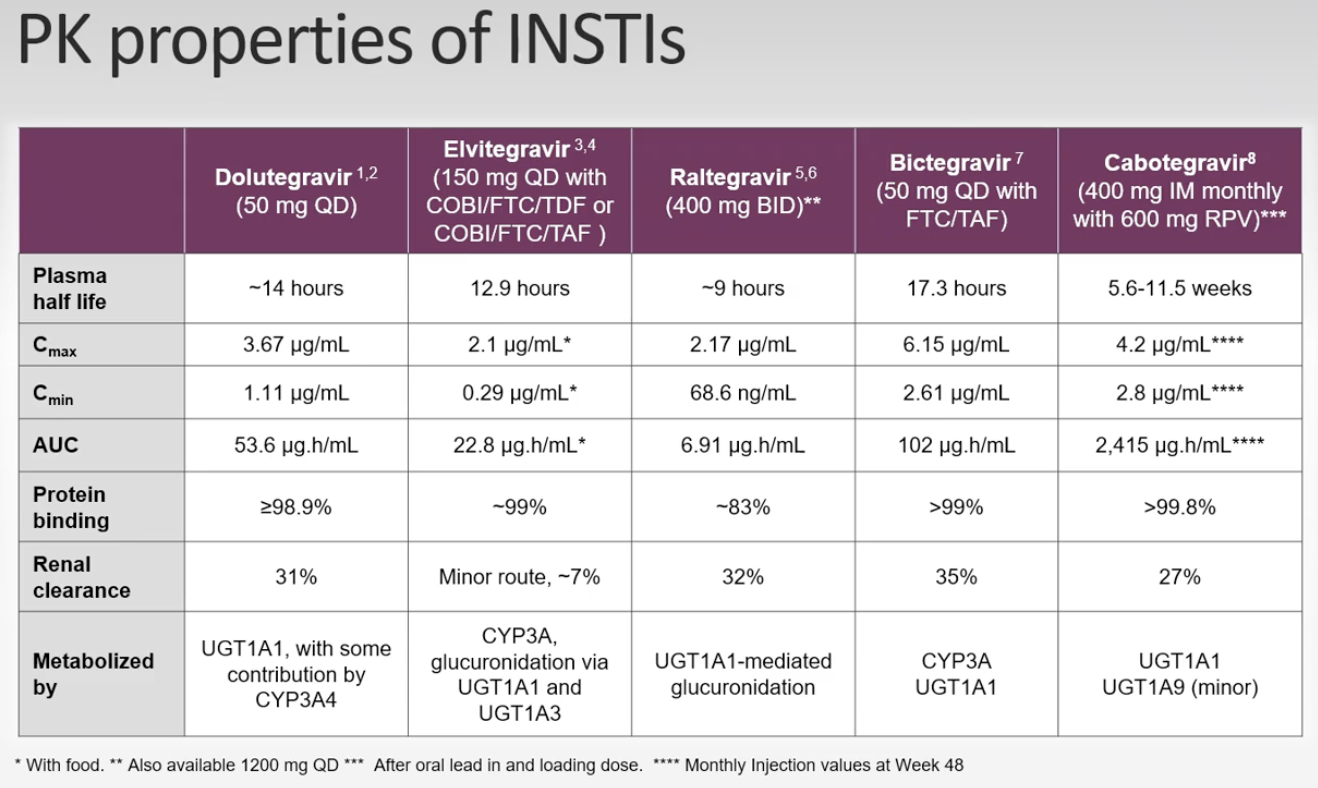
How are INSTIs metabolized?

What is P-gp?
a cellular protein pump involved in transporting molecules in/out of the cell. found extensively in the intestine. PIs are major P-gp substates.
overexpression of Pgp may result in lower ARV concentration.
Ritonovir is a potent P-gp inhibitor
Substrates for P-gp
All PWH should have SCr monitored AT LEAST _____
every 6 months.
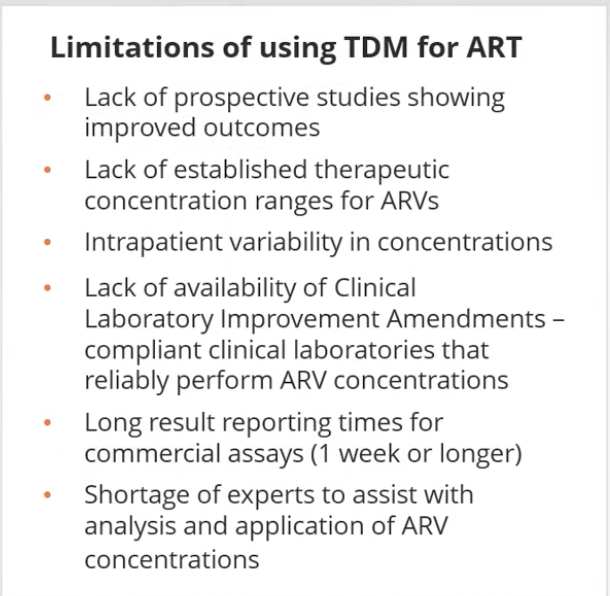
Some experts advocate the use of TDM to monitor ART. What are the limitations of routinely using TDM for ART?
Therapeutic Drug Monitoring
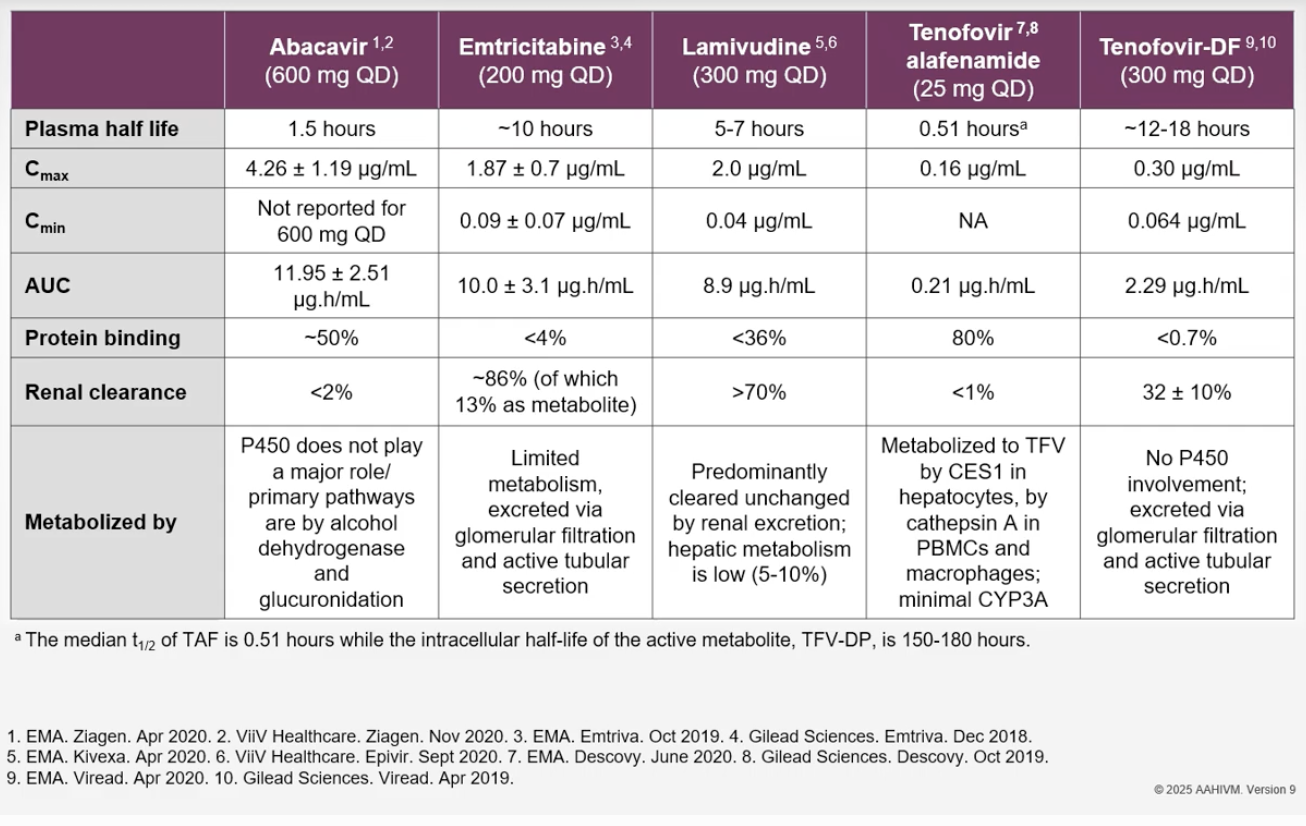
Does TAF or TDF have longer half life?
In plasma, TDF is much LONGER, 12 hrs vs. 30 minutes
TAF has a SHORT plasma half life of 30 minutes, because it all goes into the cell. It has an intracellular half life of active metabolite TFV-DP is 150-180 hours.
PK Table of NRTIs
PK properties of NNRTIs
Which ARVs are inducers of CYP3A4?
Efavirenz, Etravirine, Nevirapine
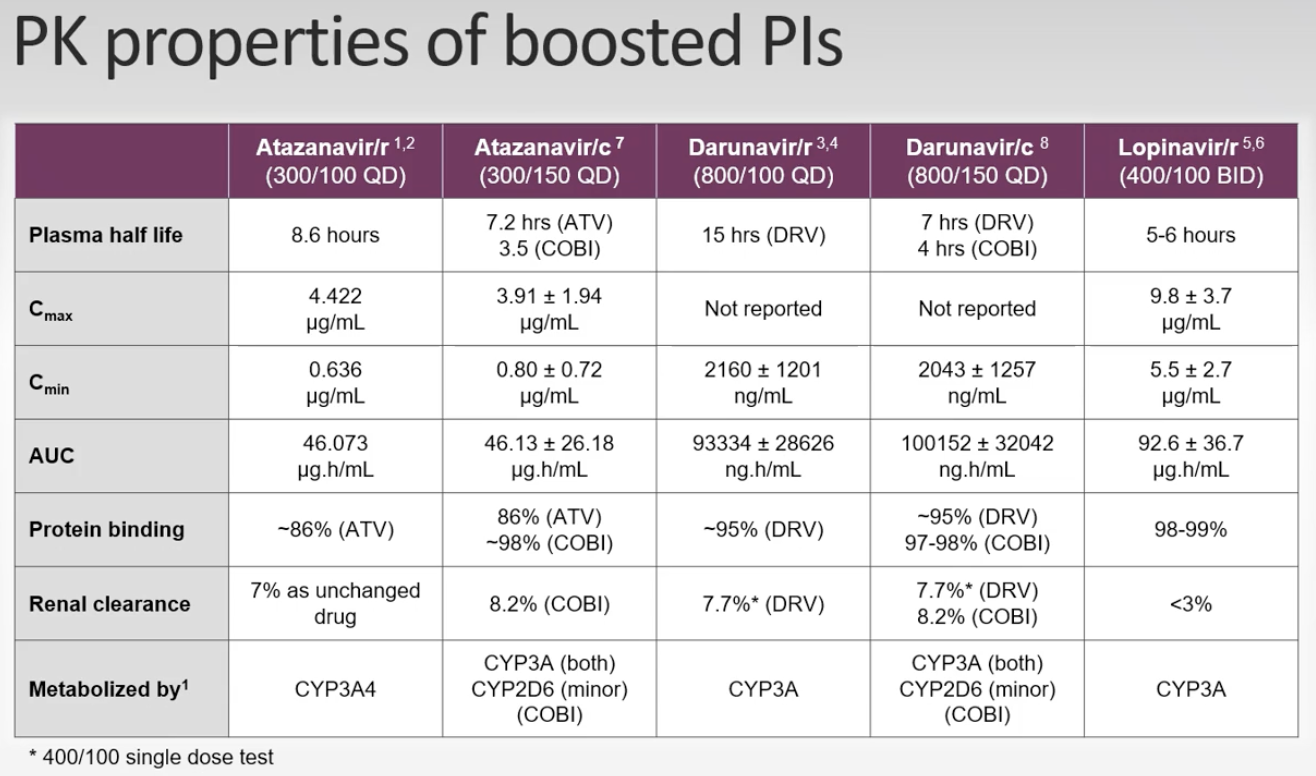
PK table PIs
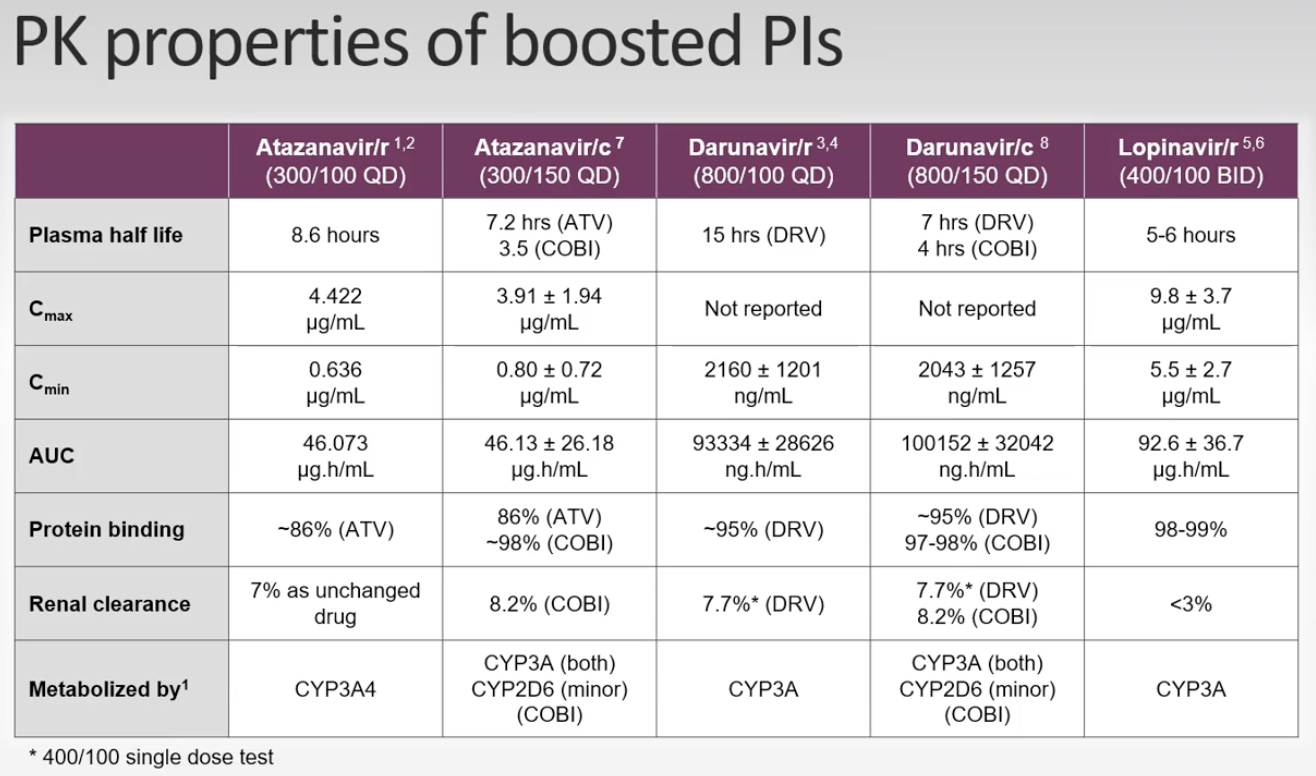
Numerous drug interactions occur with which class of ART? and why?
PIs because they are CYP3A4 substrates.
INSTI PK Table
How is RAL dosed?
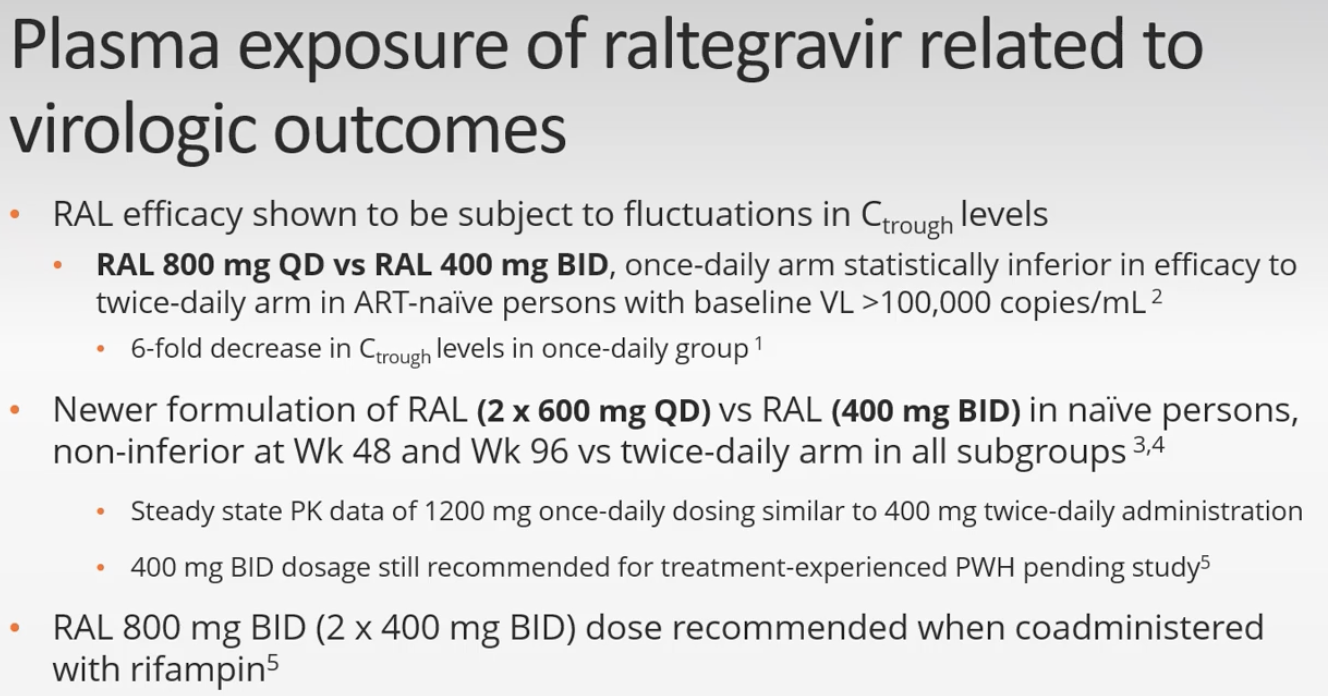
When RAL given with rifampin, what does must you use?
RAL 800mg BID
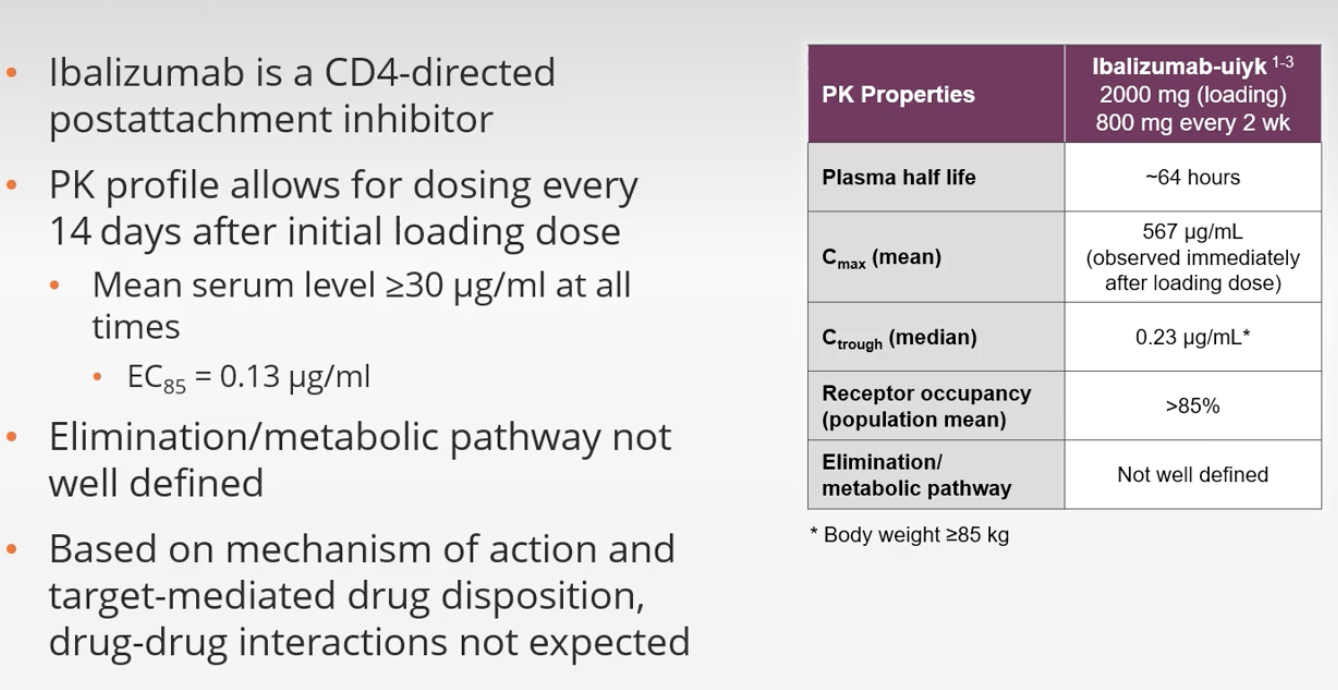
IBA PK TABLE
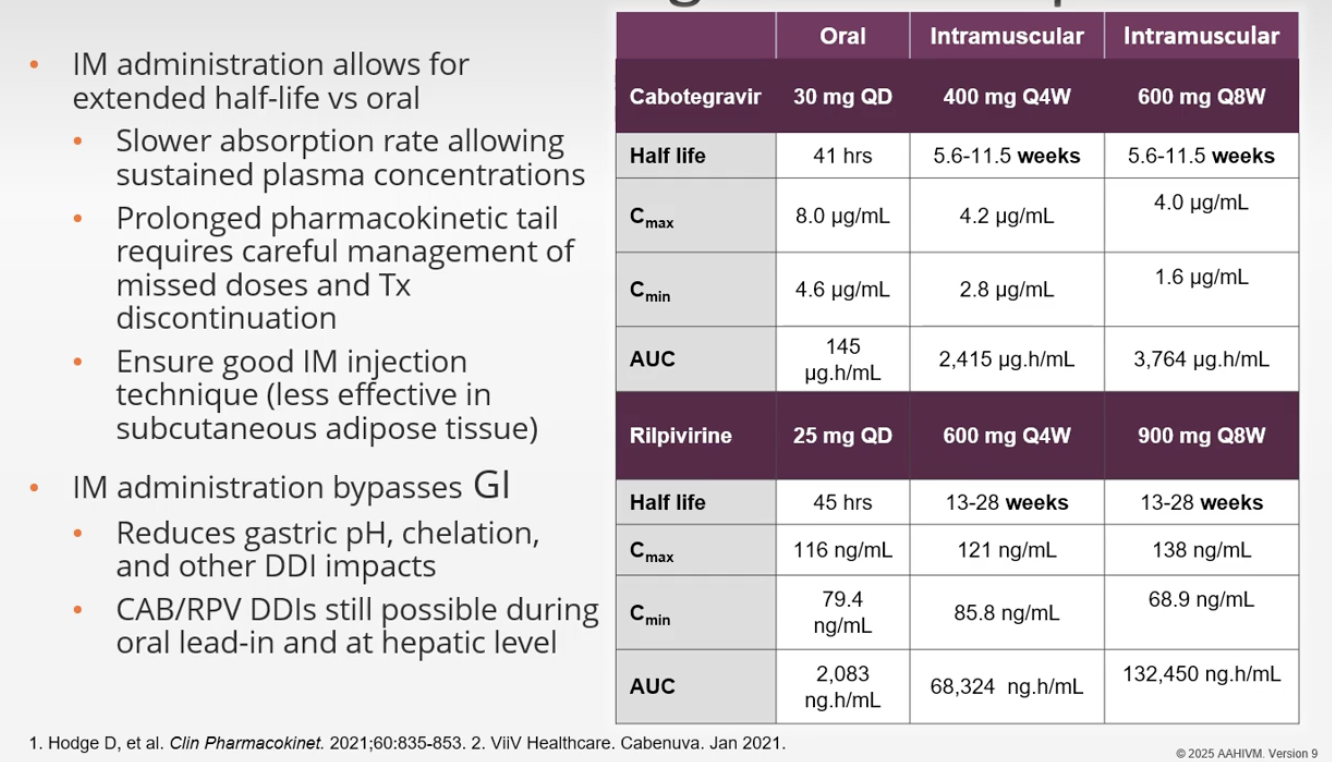
LA CAB/RPV PK TABLE
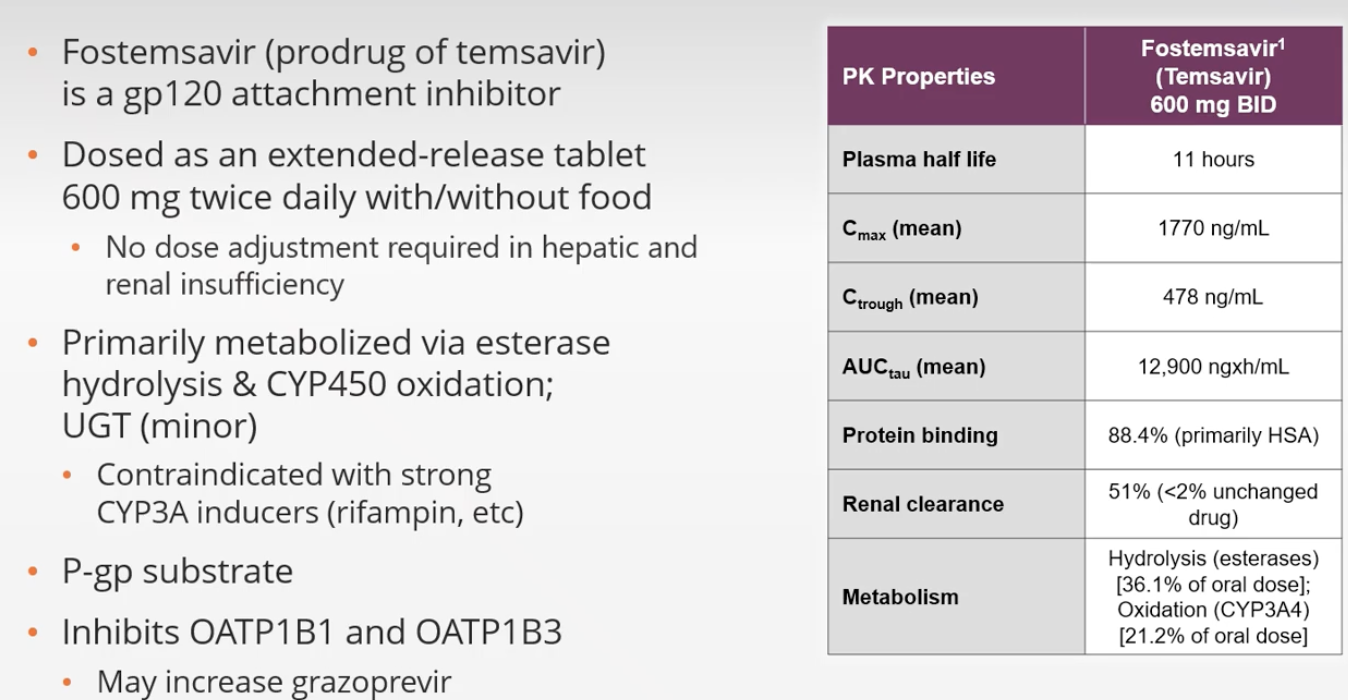
PK FOSTEMSAVIR TABLE
Temsavir primarily metabolized by esterases
CId with rifampin
PK TABLE LENACAPAVIR
Q6M SQ