PHR 948 - Block 4: Tuberculosis
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
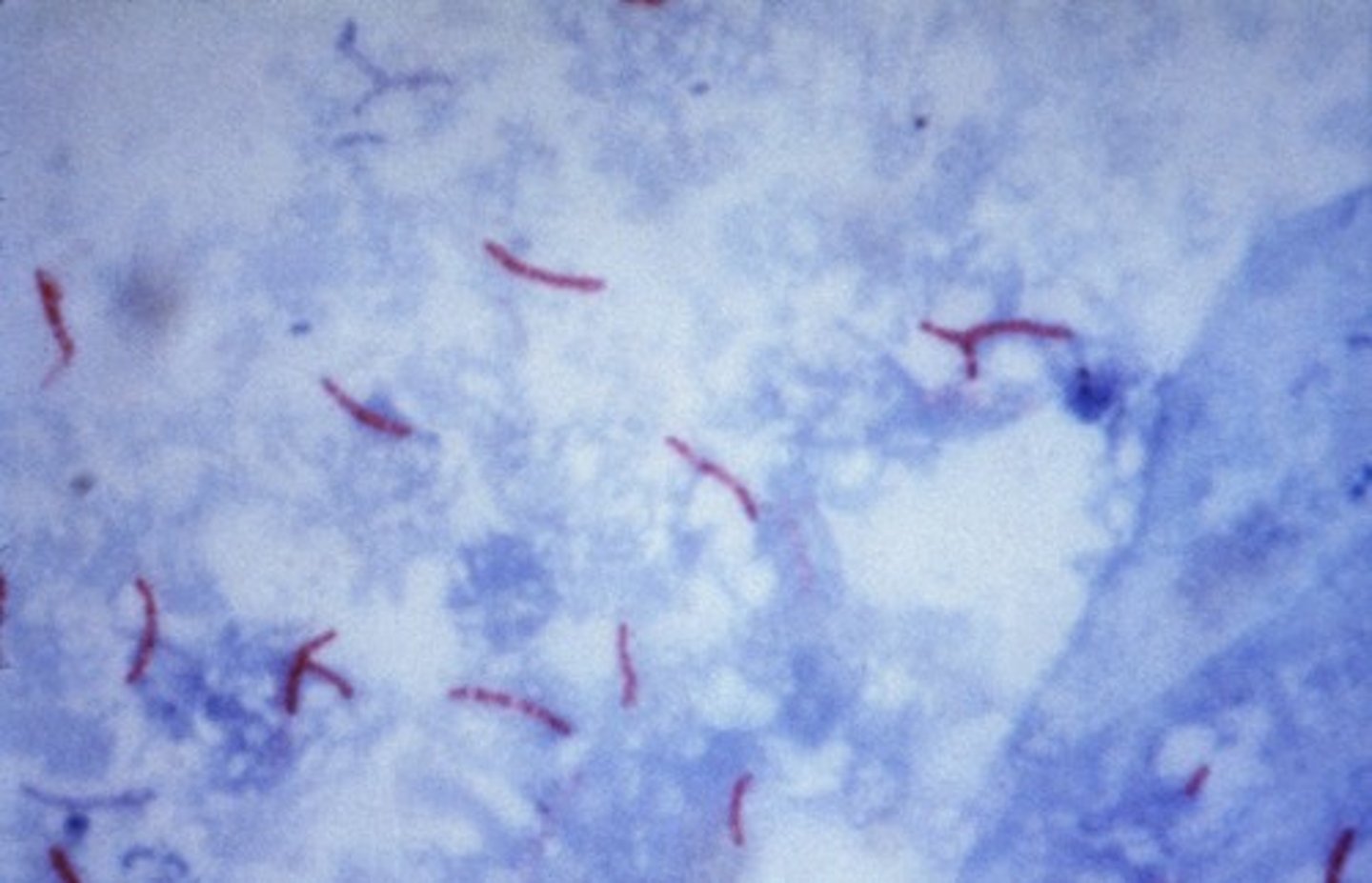
mycobacterium tuberculosis
causative agent of tuberculosis
- acid-fast, obligate intracellular aerobic bacteria
- very slow growing
- only grows in humans
- horizontal transmission via respiratory droplets
tuberculosis (TB)
- typically causes pneumonia
- can be extrapulmonary
- mortality rate: 5%
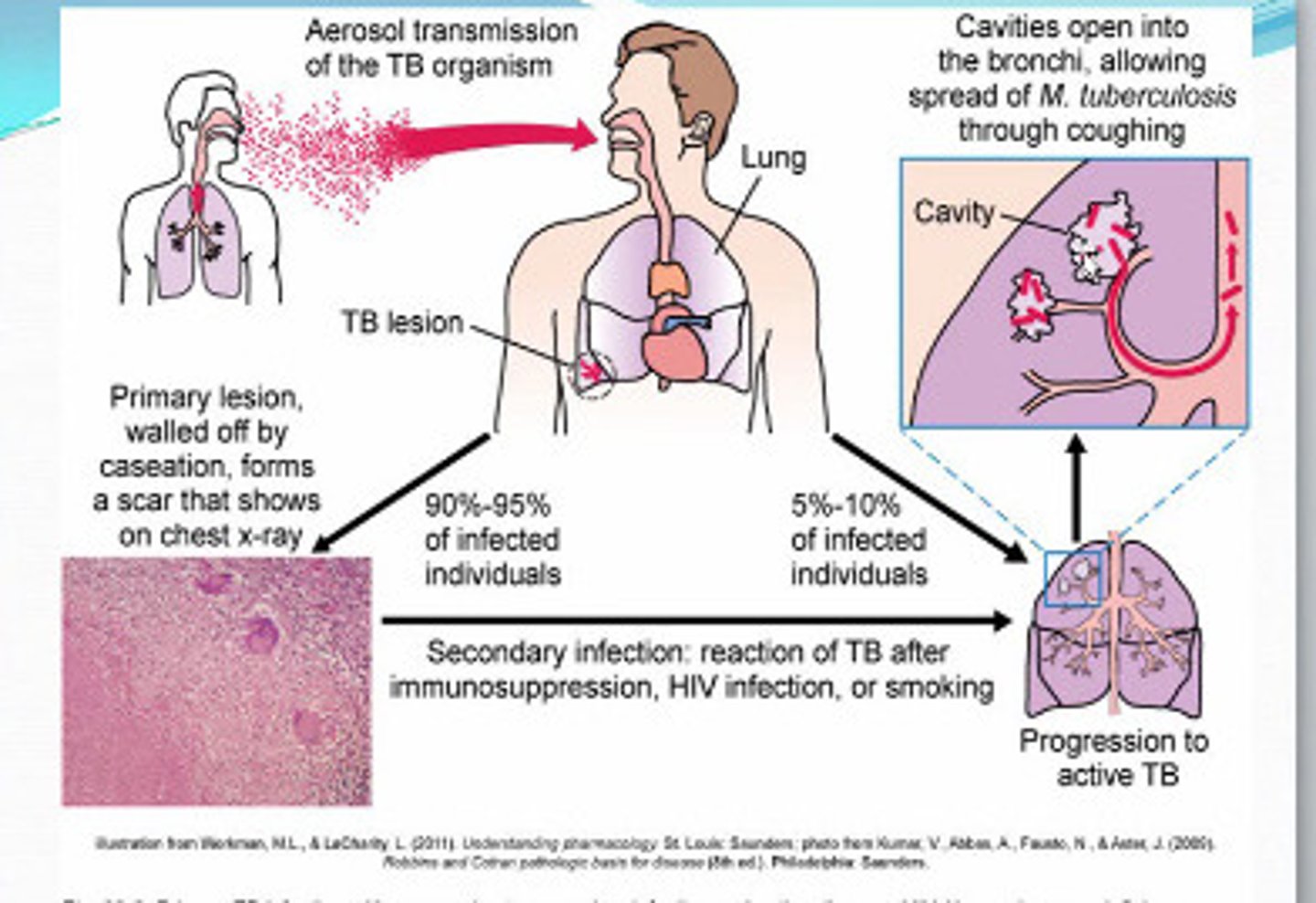
TB transmission
- spread by airborne droplet nuclei
- transmission affected by: infectiousness of patient, environmental conditions, and duration of exposure
- most people who are exposed do not become infected
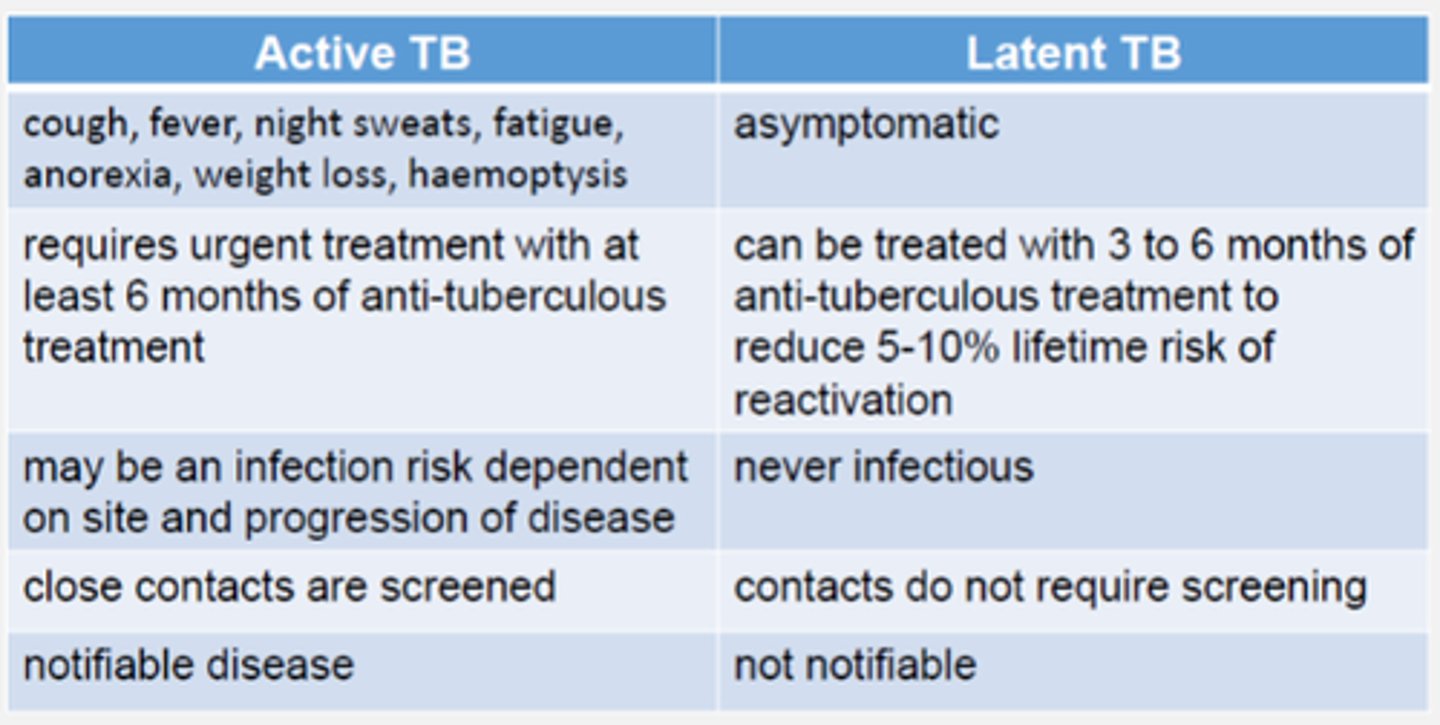
latent TB (LTBI)
inactive TB infection without symptoms
- asymptomatic = non-infectious
- bacteria can survive and remain dormant, but viable, for years
progression to active TB
- soon after infection: small number
- during lifetime: 5-10% of untreated LTBI
- 10% of people with HIV + untreated LTBI per year
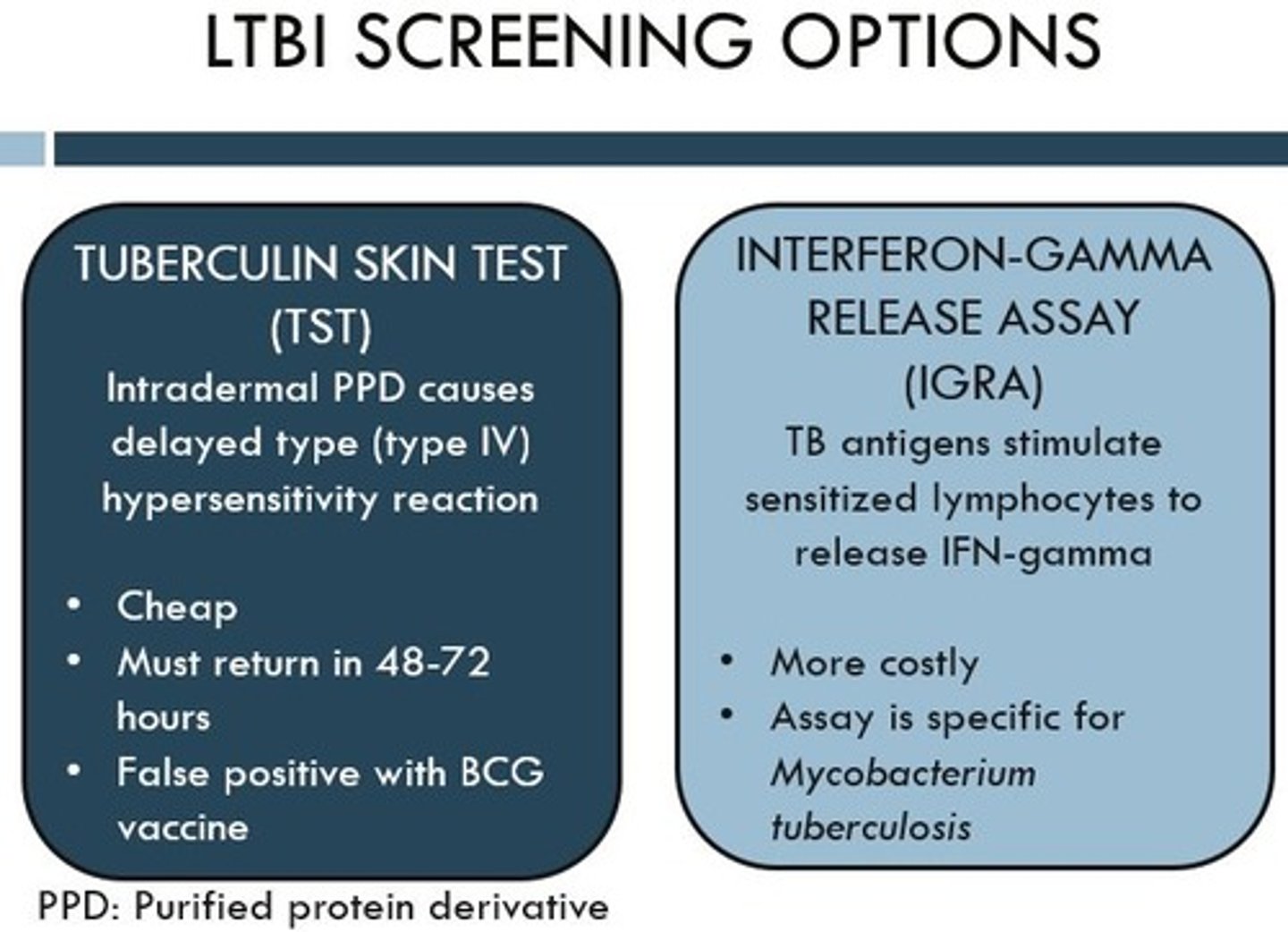
LTBI diagnosis
1. tuberculin skin test (TST)
- delayed hypersensitivity to purified protein derivative tuberculin
- intradermal injection, then read results in 48-72 hours
- false negatives seen in immunosuppressed pts, false positives seen in pts that received BCG or exposed to other mycobacteria
2. interferon-gamma release assay (IGRA)
- measured IFNγ released by T cells in response to TB antigens
- more specific, only one visit required
- fast negatives seen in kids <5, HIV infection + low CD4
- preferred test
active TB
Infected, symptomatic, and contagious
- symptoms: weight loss, fatigue, productive cough, fever, night sweats
- lab tests: some WBC elevation, lymphocyte predominance
- chest xray: patchy/ nodular infiltrates in upper lobes, cavitation
factors increasing risk for infectiousness
- coughing
- undergoing cough-inducing or aerosol-generating procedure
- chest cavitation on xray
- positive acid-fast bacilli )AFB) sputum smear
- inadequate TB treatment
suspected active TB
- if suspected, obtain: acid-fast bacilli smear/ stain, culture, and susceptibility testing
- put pt in respiratory isolation
- pt is considered noninfectious when they meet all 3 criteria:
> receiving effective therapy
> clinical improvement
> negative results for 3 consecutive sputum AFB smears (on different days)
TB treatment overview
- must use a combination of drugs
- 4 drug regiment is most common for active TB
- intensive phase for x2 months, susceptibility testing done, then additional 4-7 months in some patients
- many ADEs, drug interactions, and counseling points
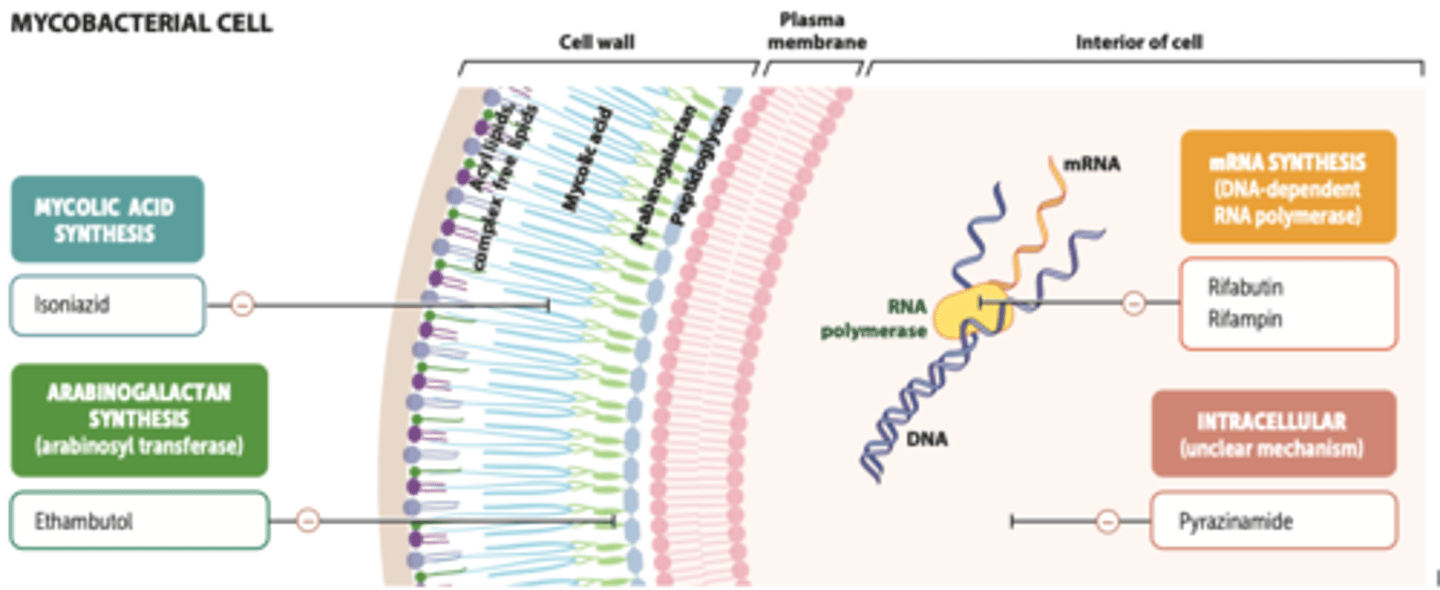
antituberculosis drugs
first-line
- isoniazid (INH): cell wall synthesis
- rifampin (RIF): RNA transcription
- pyrazinamide (PZA): lowers pH
- ethambutol (EMB): cell wall synthesis
- rifapentine (RPT)
- rifabutin (RBT)
- moxifloxacin (FQ): DNA replication
second line
- streptomycin (SM)
- cycloserine
- kanamycin
- P-aminosalicylic acid
- ethionamide
- amikacin (AGL): protein translation
- capreomycin
- levofloxacin
last line
- bedaquiline
- pretomanid
- linezolid
isoniazid (INH)
- MOA: inhibits synthesis of mycolic acids in the cell wall
- advantages: relatively nontoxic, easy to give, inexpensive
- PK: good CSF and tissue penetration, prolonged t1/2 in renal and hepatic failure
- toxicity: hepatotoxicity (NO alcohol), peripheral neuropathy (interferes w pyridoxine metabolism)
> supplement B6 in high risk pts
- DDI: CYP450 inhibitor, warfarin, carbamazepine, phenytoin, cycloserine; aluminum salts
> caution acetaminophen (hepatotoxicity)
rifampin (RIF)
- MOA: binds to bacterial RNA polymerase, inhibiting transcription
- advantages: rapidly bactericidal for TB, relatively nontoxic, easily administered
- PK: oral bioavailability >90%, good penetration into cells/tissues, poor CNS penetration
- counseling: discoloration of urine, tears, and other bodily fluids
- toxicity: GI disturbances, hepatitis, skin rash, thrombocytopenia, cholestatic jaundice
- DDI: potent inducer of CYP450s, steroids, methadone, warfarin, -azoles, estrogens
- alternatives: rifapentine, rifabutin
rifapentine and rifabutin
alternatives to rifampin
rifapentene
- used to be once weekly, now used daily
- once weekly for LTBI
- similar toxicities and DDIs to rifampin
rifabutin
- less potent hepatic enzyme inducer
- good for HIV+ patients
pyrazinamide (PZA)
- MOA: converted to pyrazinoic acid by TB = lowers pH of environment
- advantages: highly effective in first few months when inflammation is present
- PK: large Vd, good CSF penetration, adjust dose in renal impairment
- warnings: CI in severe hepatic impairment, caution in elevated LFTs/ history of alcoholism, caution in combo with other hepatotoxic drugs
- toxicity: hepatic injury, hyperuricemia, skin rash, GI upset
- DDI: small increase in isoniazid levels, combo with rifampin = severe liver toxicity
ethambutol (EMB)
- MOA: inhibits arabinosyl transferase, impairing mycobacterial cell wall synthesis
- PK: adjust dose in renal impairment
- toxicity: retrobulbar neuritis (frequent and serious)
> signs: blurred vision, central scotomata, R-G color blindness; report any visual changes
> dose and duration dependent
- DDI: aluminum salts decrease absorption
bedaquiline
last line TB therapy
- MOA: diarylquinoline antimycobacterial = inhibits mycobacterial ATP synthase
- PK: CYP3A4 metabolism
- toxicity: increase of mortality (unrelated to TB), QT prolongation, hepatotoxicity, anorexia, nausea, arthralgia
- limited data in HIV+ people
pretomanid
last line TB therapy
- MOA: nitroimidazooaxazine antimycobacterial prodrug
> activated by TB to inhibit mycolic acid biosynthesis (respiratory poison)
- toxicity: hepatotoxicity, QT prolongation, testicular atrophy
- DDI: CYP3A4 inducers, linezolid (myelosuppression, neuropathies, lactic acidosis)
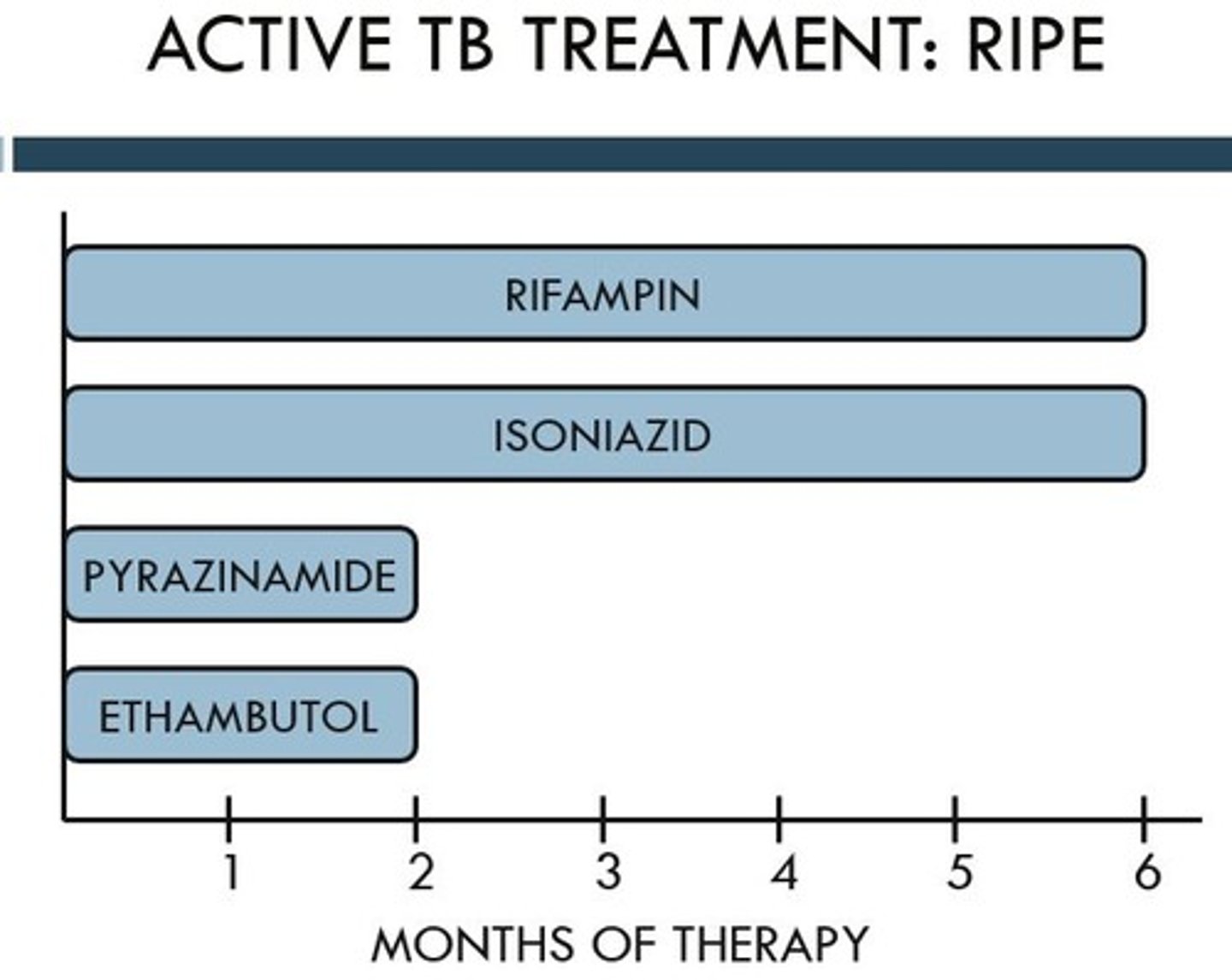
active TB treatment
intensive phase: 2 months
- RIPE: RIF + INH + PZA + EMB
- frequency options: daily, 5x week, or 3x week
- can drop EMB if susceptible to other 3
continuation phase: 4-7 months
- INH + RIF
- frequency options: daily, 5x week, 3x week, or 2x week
extend to 7 months if:
> initial chest xray shows a cavitary lesion AND (+) culture at 2 months
> only RIF + INH + EMB was used in initial phase
use clinical judgement to extend to 7 months if:
> initial chest xray shows a cavitary lesion OR (+) culture at 2 months
treatment monitoring
1. sputum for AFB smear and culture
- smear daily until out of isolation
- AFB and culture initially, then every month until 2 are negative
2. drug susceptibility test
- initially, then once if culture (+) after 3 months of treatment
3. lab testing
- renal function, AST, ALY, bilirubin, platelet count
- baseline, then only if abnormal or symptoms develop
4. if on EMB for >2 months
- visual acuity and color vision monthly
5. chest xray
- initially, then again in 2 months if culture (+)
6. monthly evaluation to assess adherence and identify ADEs
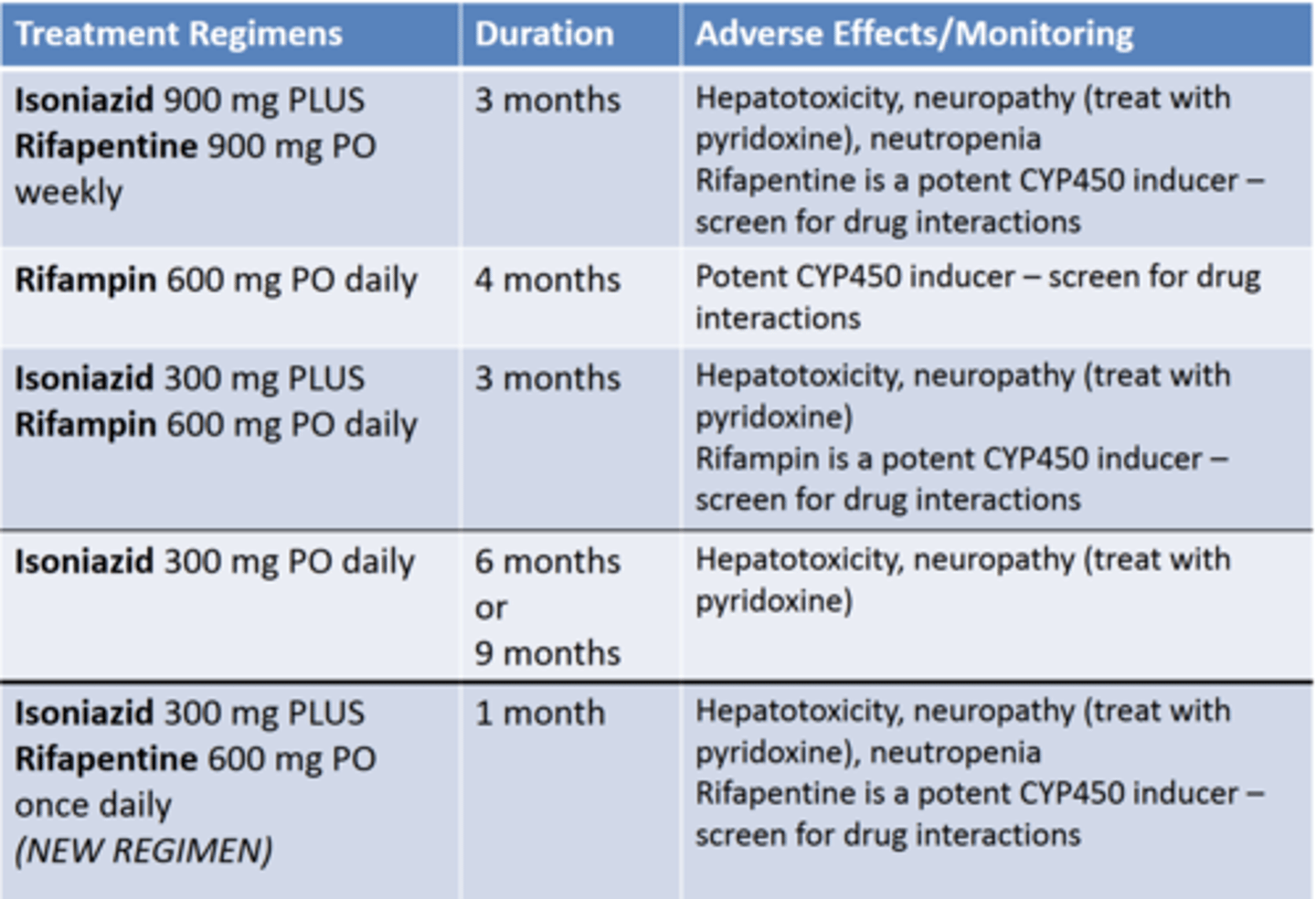
LTBI treatment
treat ALL patients diagnosed with LTBI
preferred regimens
1. INH weekly + RPT weekly x12 weeks
- directly observed or self administered
- 3+ years old
- okay for HIV+ as long as DDIs are addressed
- high pill burden
2. RIF/RBT daily x16 weeks
- no evidence in HIV+
- many DDIs
3. INH daily + RIF daily x12 weeks
- conditional recommendation
alternative regiments
1. INH daily or twice weekly (DOT) x26 weeks
- strong recommendation for HIV-
- conditional recommendation for HIV+
2. INH daily or twice weekly (DOT) x38 weeks
- conditional recommendation
drug resistance risk factors
risk factors
- prior TB therapy
- failed treatment/ relapsed
- high resistance areas
- homeless, institutionalized, IVDU, HIV (+)
- known exposure to patient infected with drug resistant TB
drug resistant TB regimen
INH resistance
- RIF + PZA + EMB x6-9 months
- could sub SM for EMB
INH + RIF resistance
- consult specialist
- give 4+ susceptible drugs
RIF resistance
- 6 month regimen (BPaL pr BPaLM)
- bedaquiline, pretomanid, linezolid, moxifloxacin
- lots of monitoring
INH + RIF + FQ + AGL resistance
- cure rates low, treatment outcomes bad, no guidelines
treatment failure
positive cultures after 4 months of treatment in patients for whom medication ingestion was ensured
mitigate:
- add at least 3 new drugs to exisiting regimen
> FQ, ethionamide, and injectable
- retest for drug resistance
- one single new drug should never be added