Oral Pathology Exam 2
1/259
Earn XP
Description and Tags
Physical & Chemical Injuries, Melanocytic Lesions, Oral Manifestations of Systemic Disease
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
260 Terms
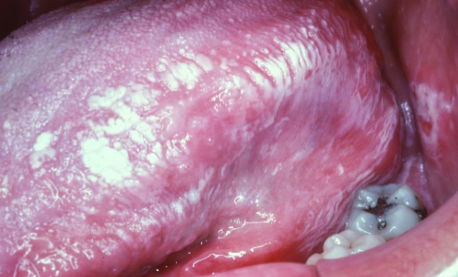
irregular white keratotic plaque, due to chewing
chronic mucosal chewing : morsicatio mucosae oris
biting on buccal mucosa (cheek)
morsicatio buccarum
biting on the lateral border of the tongue
morsicatio linguarum
biting on labial mucosa
morsicatio labiorum

morsicatio linguarum

morsicatio buccarum
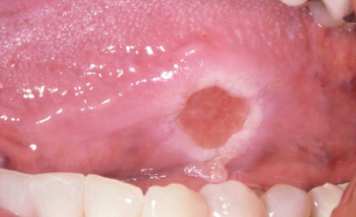
deep, chronic ulceration due to repetitive trauma causing damage to muscle; very slow resolution (months to years); more common in adults; usually found on the tongue over buccal mucosa and lips
traumatic ulcerative granuloma with stromal eosinophilia (TUGSE)
clinically similar to squamous cell carcinoma, MUST do biopsy for any lesion that is >2 weeks!
traumatic ulcerative granuloma with stromal eosinophilia
TX for TUGSE
incisional biopsy and remove cause of trauma

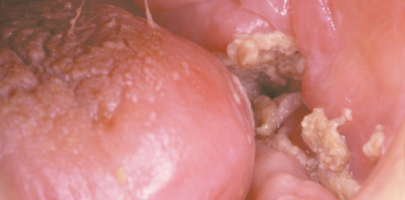
tumor-like hyperplasia of fibrous tissue that develops with the flange of an ill-fitting denture; single or multiple folds along the alveolar ridge
epulis fissuratum
TX for epulis fissuratum
reline/ adjust denture; surgical removal of tissue

placing aspirin tablet or powder next to toothache
chemical burn
characteristics of chemical burn
low pH, pseudomembrane that can be rubbed off, takes a few days to heal after chemical is removed, no scar formation

chemical burn
formocresole necrosis

chemical burn
phenol burn

chemical burn
phenol peel

chemical burn
hydrogen peroxide burn
contact with hot beverages and food
thermal burn
contact with electricity
electrical burn
characteristics of electrical and thermal burns
zones of erythema, ulceration, necrotic epithelium at periphery

burn
pizza burn

burn
smoke steam burn

burn
electrical burn

burn
pipe stem burn
topical allergic reaction; generalized or localized; may burn or be painful; goes away if product causing irritation is not used/ removed
contact stomatitis
most common flavoring agent of contact stomatitis
cinnamon
examples of products that cause contact stomatitis
mouth wash, tooth-paste, candy, gum

begins a few day to weeks after chemo begins; ulcerations and sloughing of the epithelium; common on the lips, tongue, and gingiva; resolves slowly within weeks after TX
chemotherapy mucositis
oral side effects of radiation therapy (frequency = to or > than 90%)
xerostomia, hypogeusia (loss of taste), trismus (restricted mouth opening due to muscle spasms)

radiation therapy induced
radiation mucositis

radiation therapy induced
radiation dermatitis

radiation therapy induced
radiation caries

radiation therapy induced
candidiasis

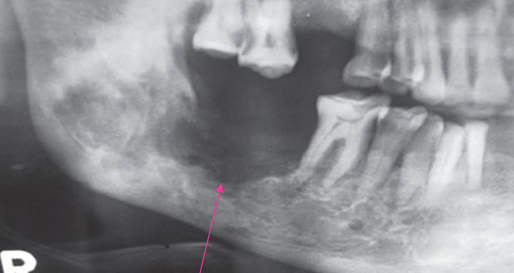
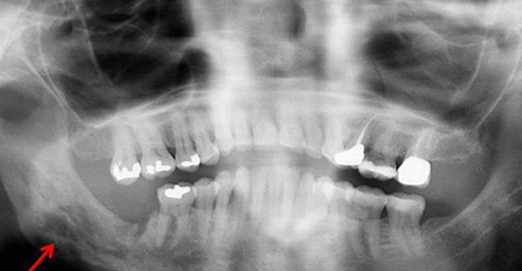
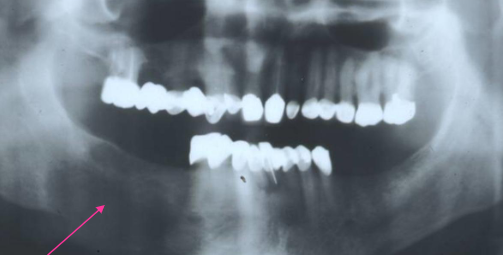
radiation therapy induced exposed non vital bone that persists for more than 3 months in absence of neoplastic disease; occurs in < 5% of patients; most arise secondary to local trauma (ext), but some are spontaneous
osteoradionecrosis
what is the main factor for development of osteoradionecrosis
radiation dose > 60 Gy
what is the more common site of osteoradionecrosis
24x more common in mandible
what is the timeframe for the development of osteoradionecrosis
occurs 4 months to 3 years after radiotherapy; pts can be susceptible forever but likelihood is less over time
to reduce the risk of osteoradionecrosis, dental tx should occur __
before radiation begins; ideally with a healing time of a minimum of 3 wks
dental tx is __ during radiation therapy unless NECESSARY
contraindicated
after radiation therapy, there is a __ window where dental tx can be performed
4 month

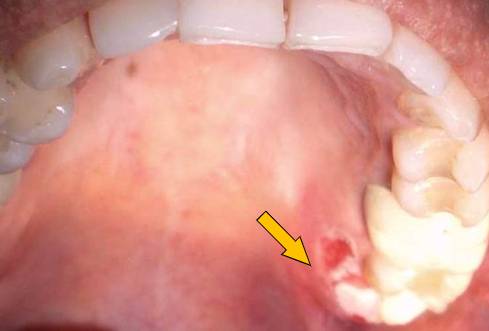
manifestation of osteoradionecrosis
fistula
manifestation of osteoradionecrosis
exposed bone

manifestation of osteoradionecrosis
moth-eaten ill-defined radiolucency
BRONJ (2003)
bisphosphonate related osteonecrosis of the jaw
ARONJ (2011)
antiresorptive related osteonecrosis of the jaw
MRONJ (2014)
medication related osteonecrosis of the jaw

current or previous tx with antiresorptive medication, exposed bone in MF region for longer than 8 wks, no hx of radiation therapy
required characteristics for diagnosis of MRONJ
poorly defined RL borders
osteoradionecrosis
poorly defined RL borders
MRONJ
poorly defined RL borders
metastatic disease

poorly defined RL borders
osteomyelitis
occurs at the site of anesthetic injection; necrosis/ ischemia from epinephrine; erythema, pain, ulceration; usually occurs on the hard palate; heals within 1-2 wks
anesthesia necrosis

minute hemorrhage (1-2 mm) in skin, mucosa, serosa; multiple red/ purple spots, do not blanch with pressure; due to injuries, accidents, excessive coughing, vomiting
petechiae

slightly larger than 1-2 mm (max 1cm); single or multiple red or purple spots; do not blanch with pressure; due to vascular problems, platelet disorders, vit C deficiency
purpura
any accumulation over 2 cm
ecchymosis

accumulation of blood within tissue producing a mass
hematoma

amalgam traumatically introduced into mucosa; steel gray/ blue/ black macule; last indefinitely and may enlarge over time; no TX necessary but excision of very dark lesions may be warranted to rule out melanoma
amalgam tattoo (localized argyrosis)

becoming more common; hyaluronic acid (juvederm) or poly-lactic acid (sculptra); usually asymptomatic though pts may complain of a “bump”; some cases can have an allergic reaction; brusing, erythema, itching
oral lesions associated with cosmetic fillers
from solder, old paint, battery factories, porcelain glaze, candle wicks; black marginal gingivitis
lead poisoning (plumbism)
from medications/ makeup; diffuse gray discoloration of skin and membranes; gray marginal gingiva
silver poisoning (argyria)
from medications; “mad hatter” curing pelts in hats (1800s)
mercury poisoning (acrodynia)

from lead poisoning (plumbism)
Burton’s line
burton line, plumbism
lead
acrodynia, erythism, pink disease
mercury
argyria
silver
mees lines, black foot disease
arsenic
methemoglobinemia
bismuth
chrysiasis
gold
dead necrotic bone that is separated from remaining bone
sequestrum

most arise from lingual surface of the mandible adjacent to molars along mylohyoid ridge; linear ulceration, pain varies; TX = surgical removal
spontaneous sequestration
the sheath of new bon that forms around a sequestrum (new viable bone surrounding dead bone)
involucrum

dome shaped, faintly radiopaque lesions; arising from maxillary sinus; accumulation of inflammatory exudate; TX depends if lesion is symptomatic
antral pseudocyst

from air forced into subcutaneous or fascia spaces (e.g. blowing an instrument or glass, prolonged extraction while using a handpiece); rapid onset within an hour; facial swelling and erythema, pain dysphagia, dysphonia, vision difficulties, mild fever; TX = AB if infection, most regress spontaneously within 5 days
cervicofacial emphysema
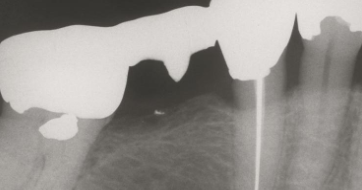
30% show amalgam particles on xray
localized argyrosis
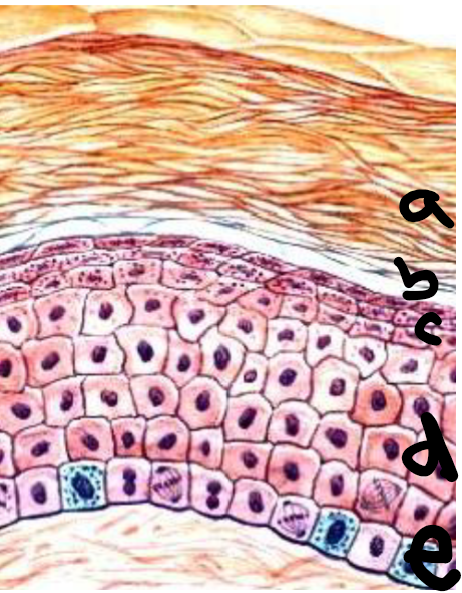
a
stratum corneum
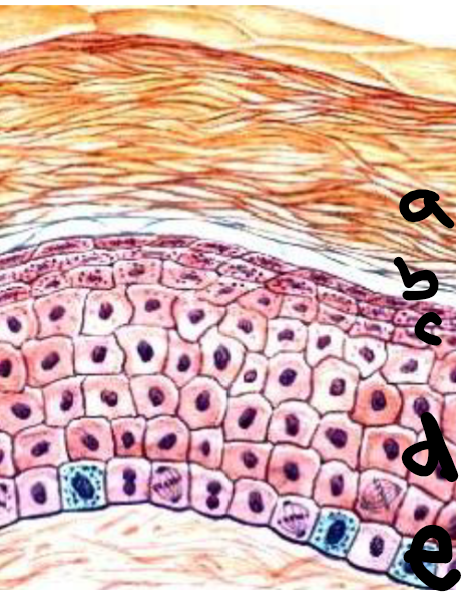
b
stratum lucidum
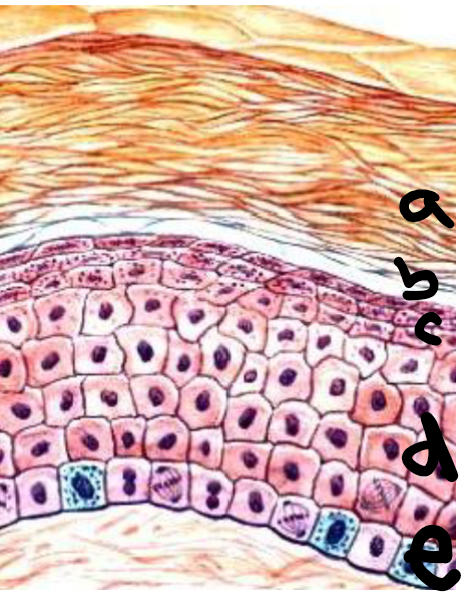
c
stratum granulosum
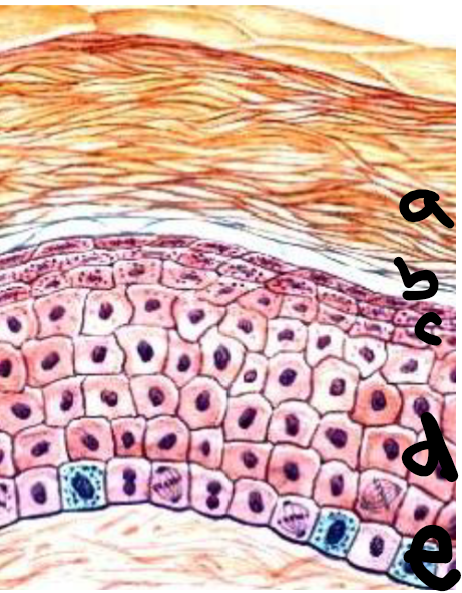
d
stratum spinosum
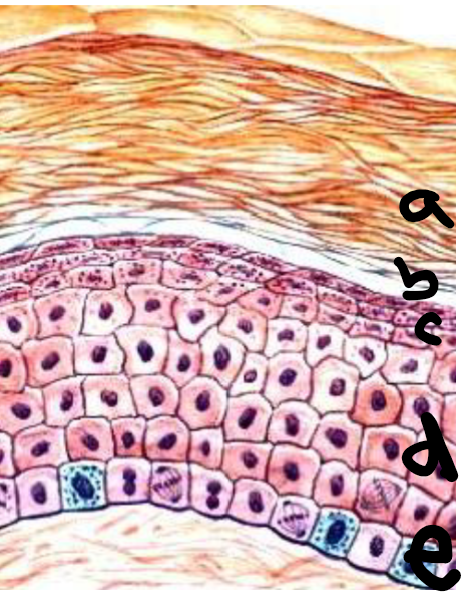
e
stratum basale

clinically, a brown macule on face/arms/back that gets darker with UV light and is a benign increased in melanin deposition
ephelis (freckles)
If your patient comes in with ephelis, should you prescribe tx?
No tx required
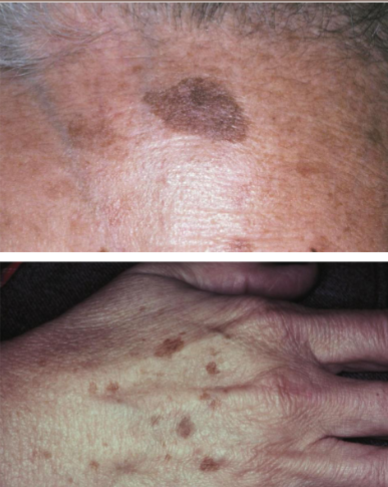
A uniform demarcated brown color, may have irregular outline. Results in an increase in melanocytes, are benign brown macules. No color change with UV light
actinic lentigo (age spots, liver spots)
What treatment does actinic lentigo call for?
no tx

rare, benign acquired dark melanosis of mucosa (reactive process) most commonly on the buccal mucosa. Solitary, asymptomatic, grows fast within weeks and is usually caused by trauma (like a toothbrush)
Melanoacanthoma
Tx required of Melanoacanthoma
disappears when insult is removed
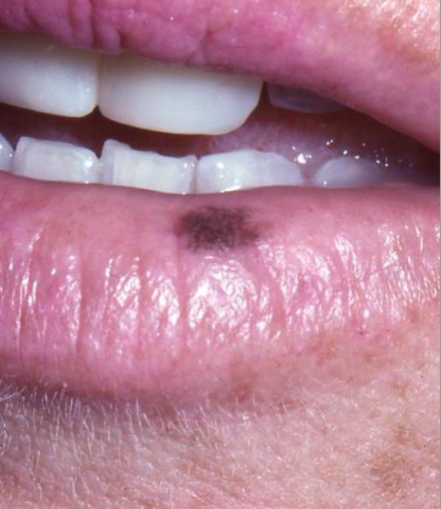
Uniform brown pigmentation, oval w/ well demarcated borders. Most common on the lower lip vermillion, buccal mucosa, gingiva, palate. Will be a benign increase in melanin deposits
melanotic macule
Cause of melanotic macule?
developmental

Acquired melanotic nevus - “common mole”

Congenital melanocytic nevus “birth mark”

developed during childhood and YA, located on the skin above the waist and intraorally on the hard palate or gingiva, but can occur anywhere
Acquired melanocytic nevus
What condition is classified on histopathological appearance: junctional, compound, intradermal/intramucosal, blue nevus
acquired melanocytic nevus
What happens to 2-3% of large congenital nevus?
transforms into malignant melanoma

most common on trunk and extremities, 15% in head and neck
congenital melanocytic nevus

melanoma arising in a congenital nevus

treatment for melanocytic nevus
excise for aesthetics & definitive diagnosis. Follow-up. Can use dermabrasion, chemical peel, cryotherapy, or surgery
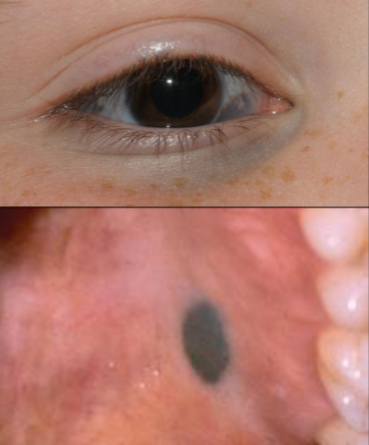
Appears as a macular or dome-shaped, blue or blue-black lesion smaller than 1 cm in diameter usually in childhood or YA and females.
blue nevus
nevus of ota
conjunctiva
oral lesions of blue nevus are found
almost always on the palate

blue nevus

amalgam tattoo