q5: basics of obturation
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
endontic success is dependent on…
adequate instrumentation, disinfection, and obturation of the root canal system
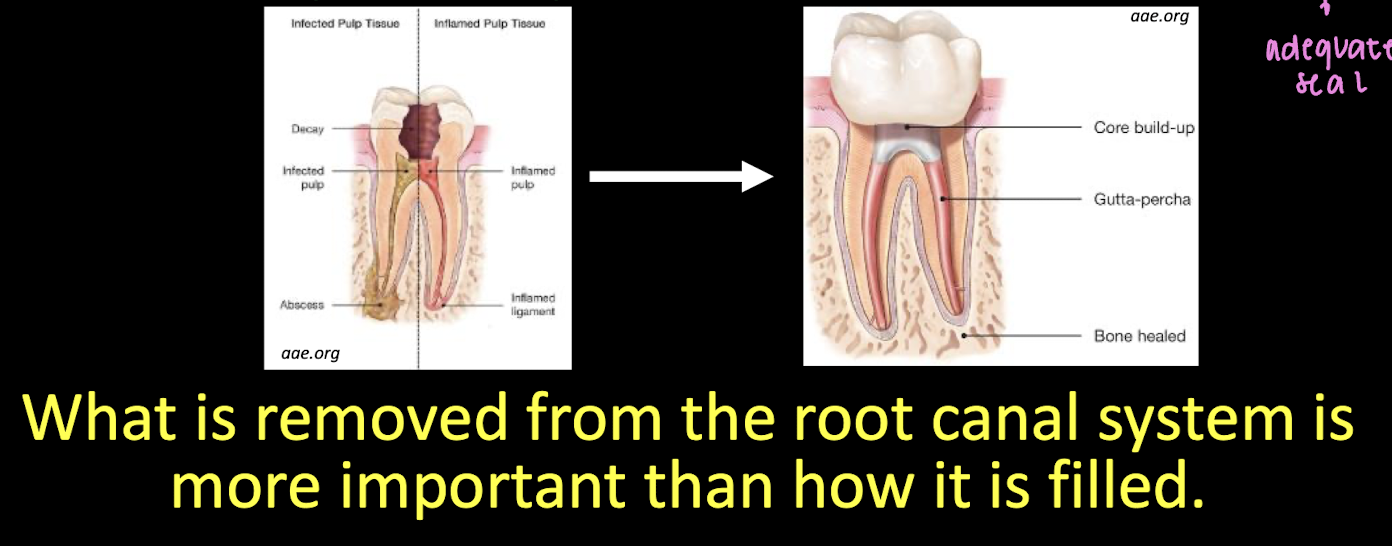
objective of obturation
create a watertight seal along the length of the root canal system from the orifice to the apical foramen
obturation prevents leakage of microorganisms and their biproducts into the root canal system from a _________ direction and leakage of periapical tissue fluids into the root canal system from an ______ direction
coronal; apical
t for f: obturation seals within the root canal system any irritants that are NOT fully removed during cleaning and shaping
t
obturation seal allows for _________ and _________ of apical periodontitis
prevention and healing
why obturate (3)
prevention and healing of apical periodontitis
periapical lesions may heal after root canal debridement without obturation
if bacteria are eliminated prior to obturation, PA lesions heal regardless of quality of obturation
if bacteria remain prior to obturation, healing is related to the quality of obturation
t or f: how the root canal system is filled is more important than what is removed
f
obturation depends on… (5)
pulpal and periapical dx
radiographic presentation
signs and symptoms
degree and difficulty
pt management issues ‘logistical concerns
in predoc endo clinic, most cases are completed in ___ vist(s)
>1 due to logistical concerns (clinician experience level)
when can you obturate in the case of a vital pulp
can do in 1 visit
when can you obturate is the pulp is swelling and unable to dry
takes 2 visitis
what necrotic diagnoses are included in obturation timing decisions
Asymptomatic apical periodontitis
Symptomatic apical periodontitis
Chronic apical abscess
why might you choose multiple visits instead of single-visit obturation
to allow antimicrobial effect of intracanal medicament.
does multiple-visit treatment improve prognosis compared to single-visit
no evidence of improved prognosis
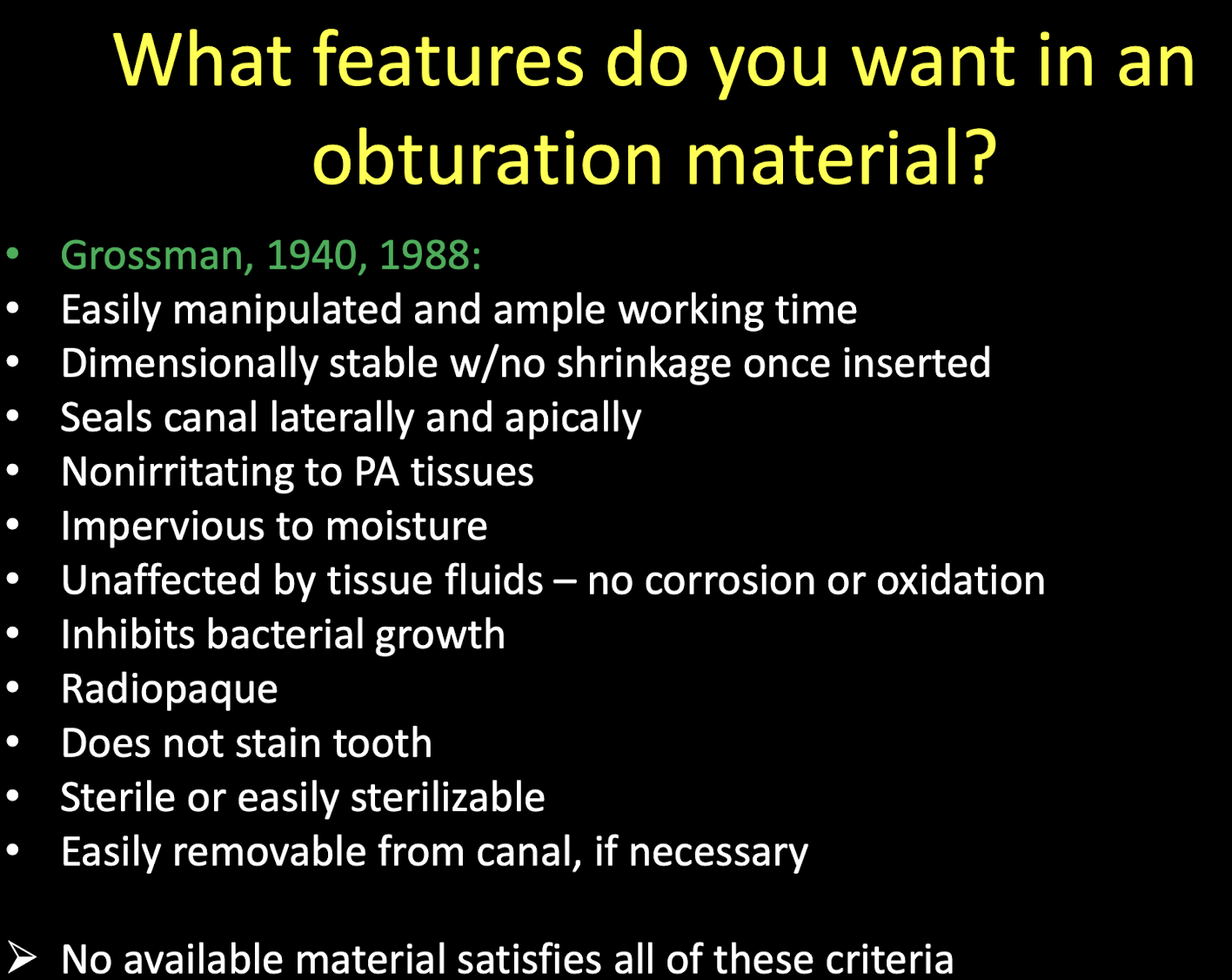
what features do you want in an obturation material (11)
easily manipulated and ample working time
dimensionally stable w no skrinkage once inserted
seals canal laterally and apically
non-irritating to PA tissues
impervious to moisture
unaffected by tissue fluids- no corrosion or oxidation
inhibits bacterial growth
radiopaque
does not stain tooth
sterile or easily sterilizable
easily removable from canal, if necessary
when thinking of features that you want in an obturation material, what single material do you think of
no available material that satifies all these criteria
what do we obturate w
gutta-percha
sealer
gutta percha is a core material that…
occupies the bulk of the space
sealer must be used w gutta-percha for adequate…
seal
most popular obturation material
gutta percha
composition of commercial gutta percha
~20% gutta-percha
65% zinc oxide
10% radiopacifiers
5% plasticizers
gutta percha bond
1,4 trans-polyisoprene (rubber)
2 different forms/phases of gutta percha
alpha
beta
beta form/phase of gutta percha
soild, compactable
alpha form/phase of gutta percha
pliable flowable, tacky
how does gutta percha transition between its alpha and beta phase
alpha: when heated
beta: when cooled
advantages of gutta percha (5)
plasticity
easy of manipulation
minimal toxicity
radiopaque
removable w heat or solvent
disadvantages of gutta percha (2)
does not bond to dentin
shrinks on cooling
taper of gutta percha
.04
.02

sizing consistency w .04 taper gutta percha
laser cut, so they are consistent tip size
sizing consistency w .02 taper gutta percha
these are hand-rolled so there is some variation within the ISO size
colors of gutta perch match _____
files:
15= white
20=yellow
25=red
30=blue
35=green
40=black
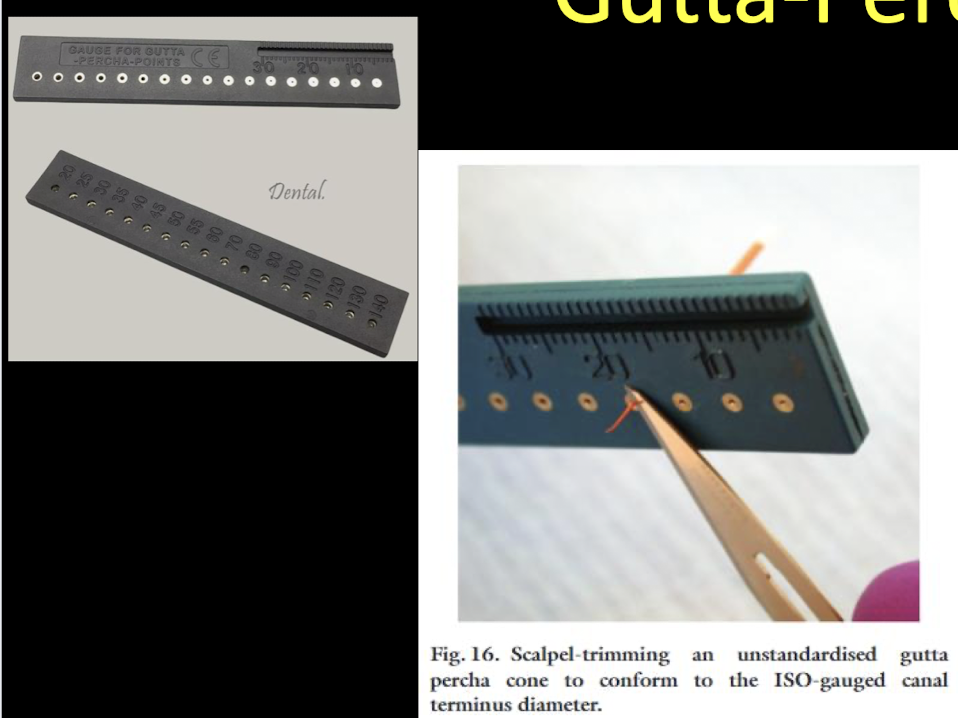
what is gutta-gauge used for
to trim the tip to the ISO size usually for the .02 taper → using a smaller cone size, putting it into the number side and cutting the opposite side w a blade, spoon, etc)
sealer creates _______
seal
sealer serves as a filler between ____________ and ____________
gutta percha and canal irregularities
sealer serves as a _________ in seating gutta-percha during obturation
lubricant
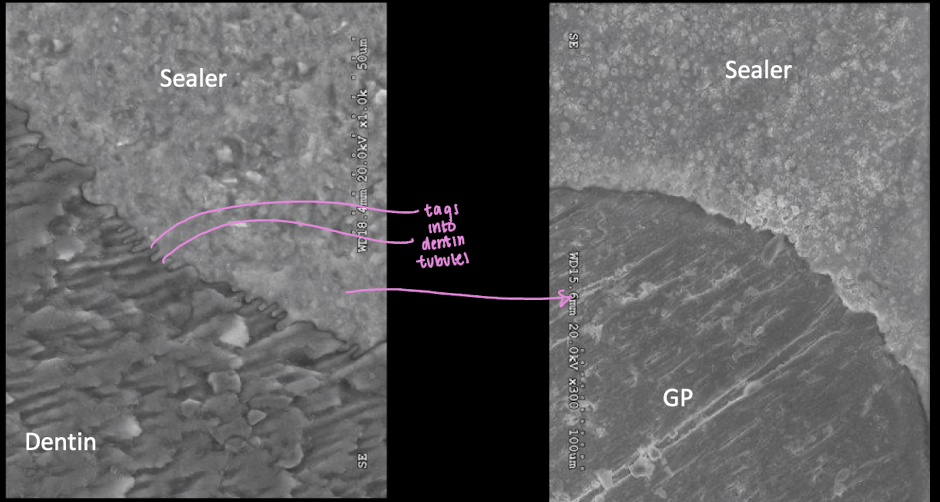
sealer can flow into _________
dentinal tubules
desired properties of sealer (10)
biocompatible
seals well- hermetic seal
adhesive- between it and canal wall
radiopaque
non-shrinking
non-staining
set slowly
soluble in solvents, but not tissue fluid
bacteriostatic/cidal
powder particles should be v fine to allow mixing easily w liquid
5 types of sealer
zinc oxide eugenol (ZOE)
calcium hydroxide
glass ionomer
resin
bioceramic
what type of sealer will we be using
bioceramic
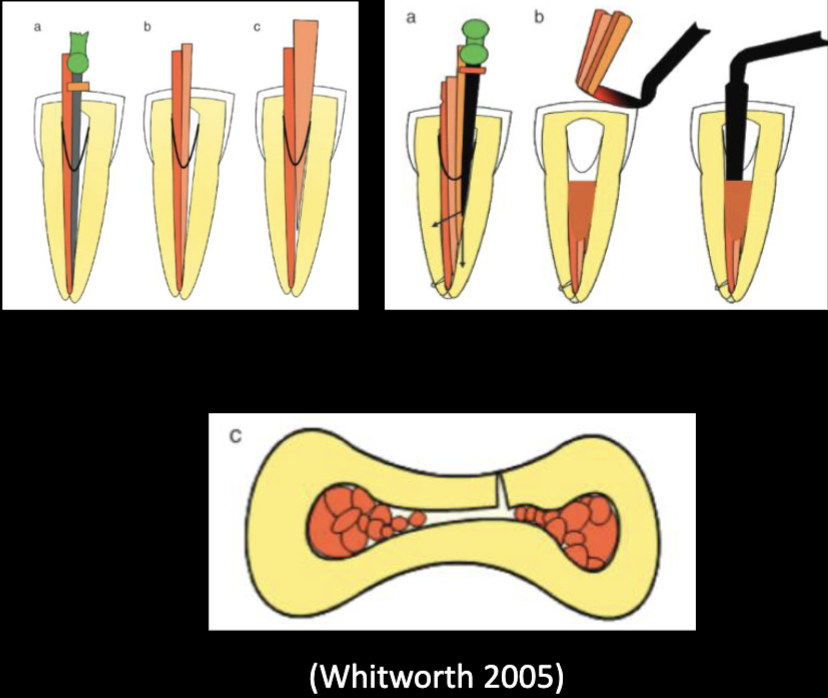
advantages of lateral condensation (6)
can be used in wide variety cases
does NOT require specialized equipment
track record of clinical success → well-documented efficacy
safe and simple to learn for novice clinicians- widely taught and used
less technique sensitive than some techniques
predictable length control → less likely to overfill
good length control
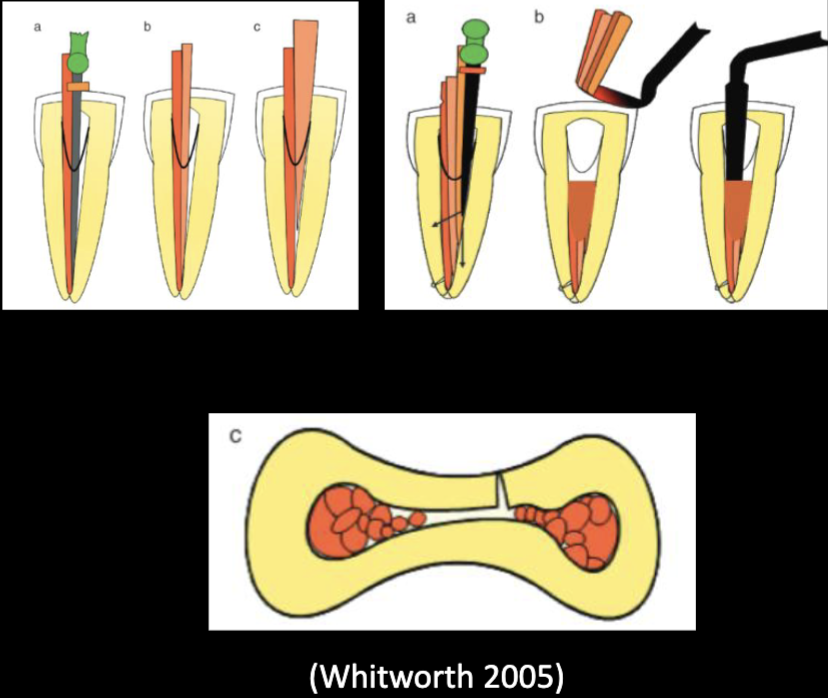
disadvantages of lateral condensation
requires more time than some techniques
challenging to use in some clinical cases (just like hard cases)
does NOT fill canal irregularities, voids, spreader tract
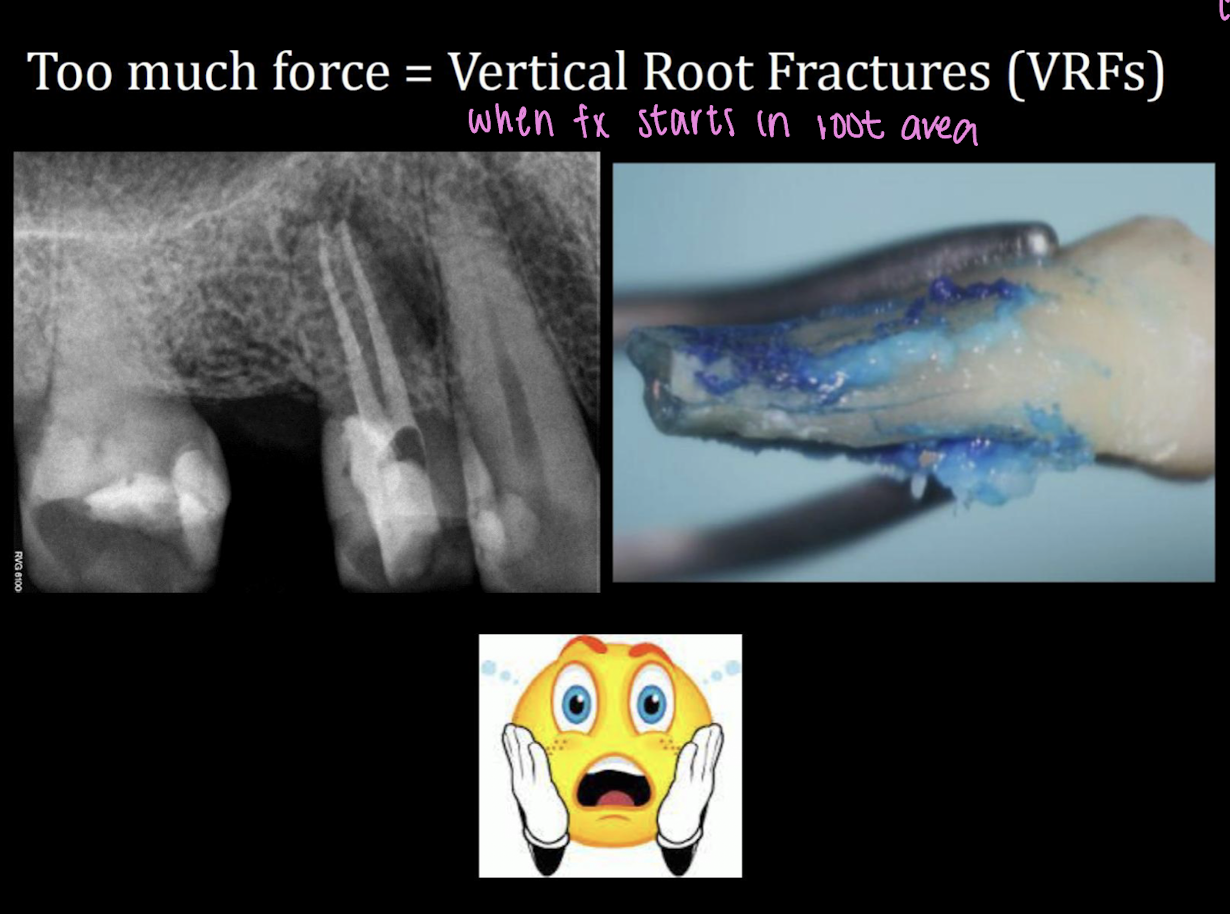
risk of vertical root fracture → w finger spreader if too much force is applied

used for cold lateral condensation
finger spreader

5-7 condenser/plugger is used to
condense gutta percha after searing

heated plugger is used to
sear GP
ZOE sealer requires mixing ______ and ______
powder and liquid

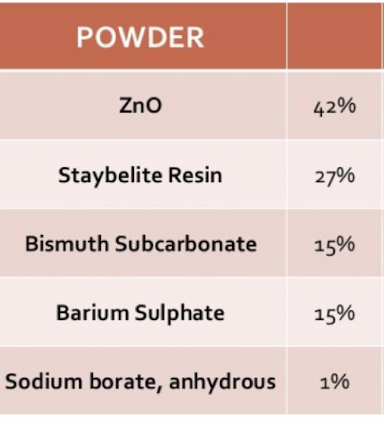
components that make-up powder in ZOE sealer (5)
ZnO
staybelite resin
bismuth subcarbonate
barium sulphate
sodium borate, anhydrous
component that makes-up liquid in ZOE sealer
eugenol
setting time for ZOE sealer vs in canal
2 hour set time
within root canal 10-30 min → moisture of dentin
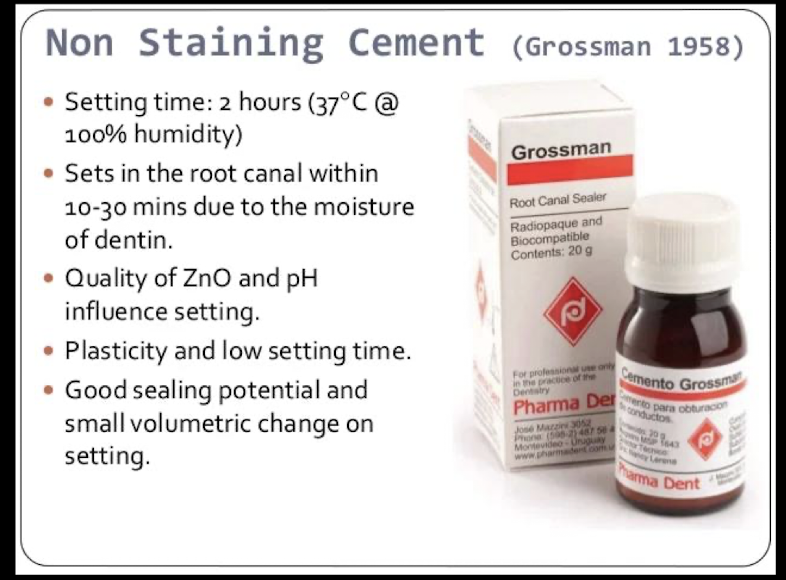
quality of _________ influences the setting of ZOE sealer
ZnO and pH
properties of ZOE sealer (4)
plasticity
low setting time
good sealing potential
small volumetric change on setting
recommended condensation forces w finger spread in canal
<2.5 lb
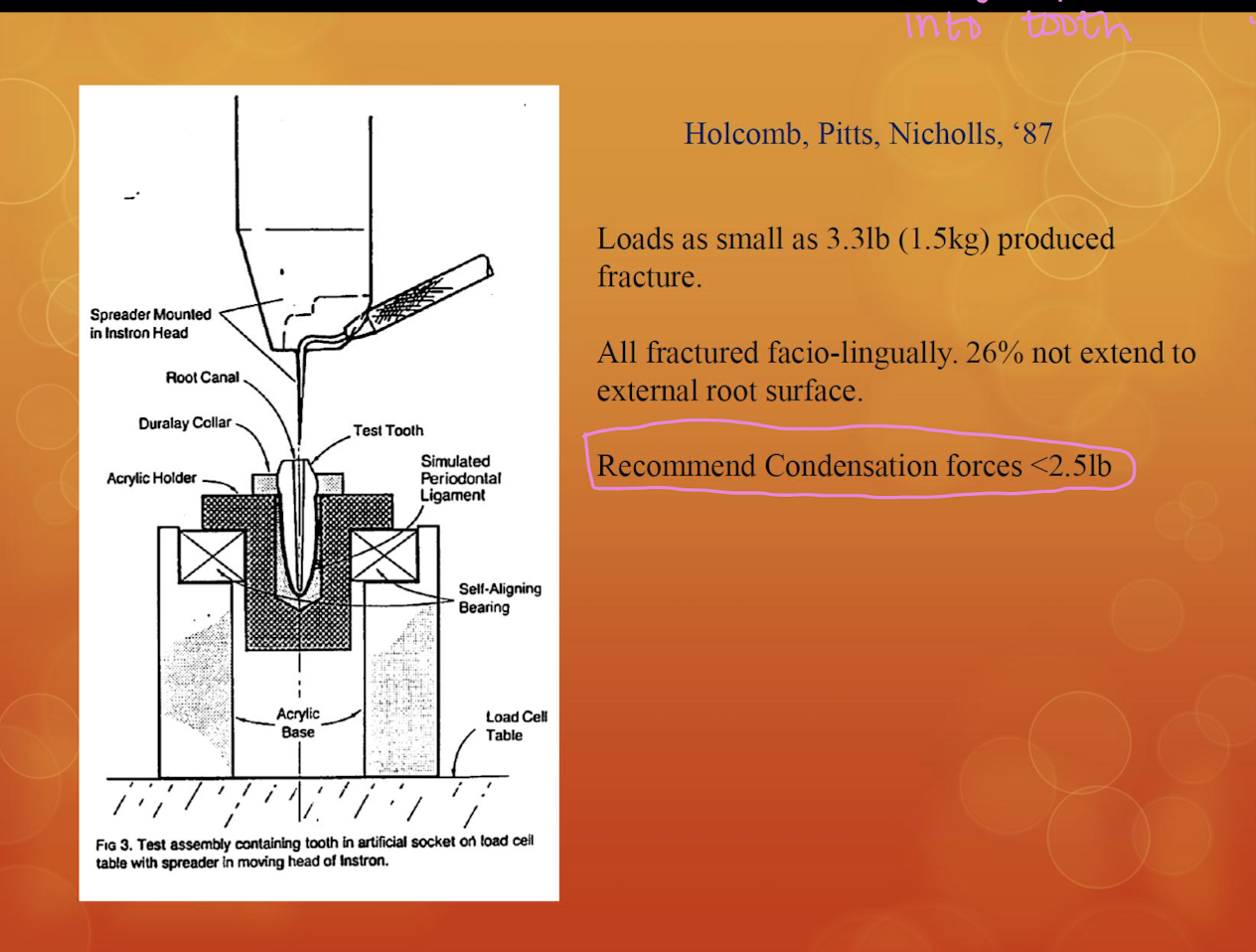
loads as small as _____ lbs produced fracture
3.3 lbs
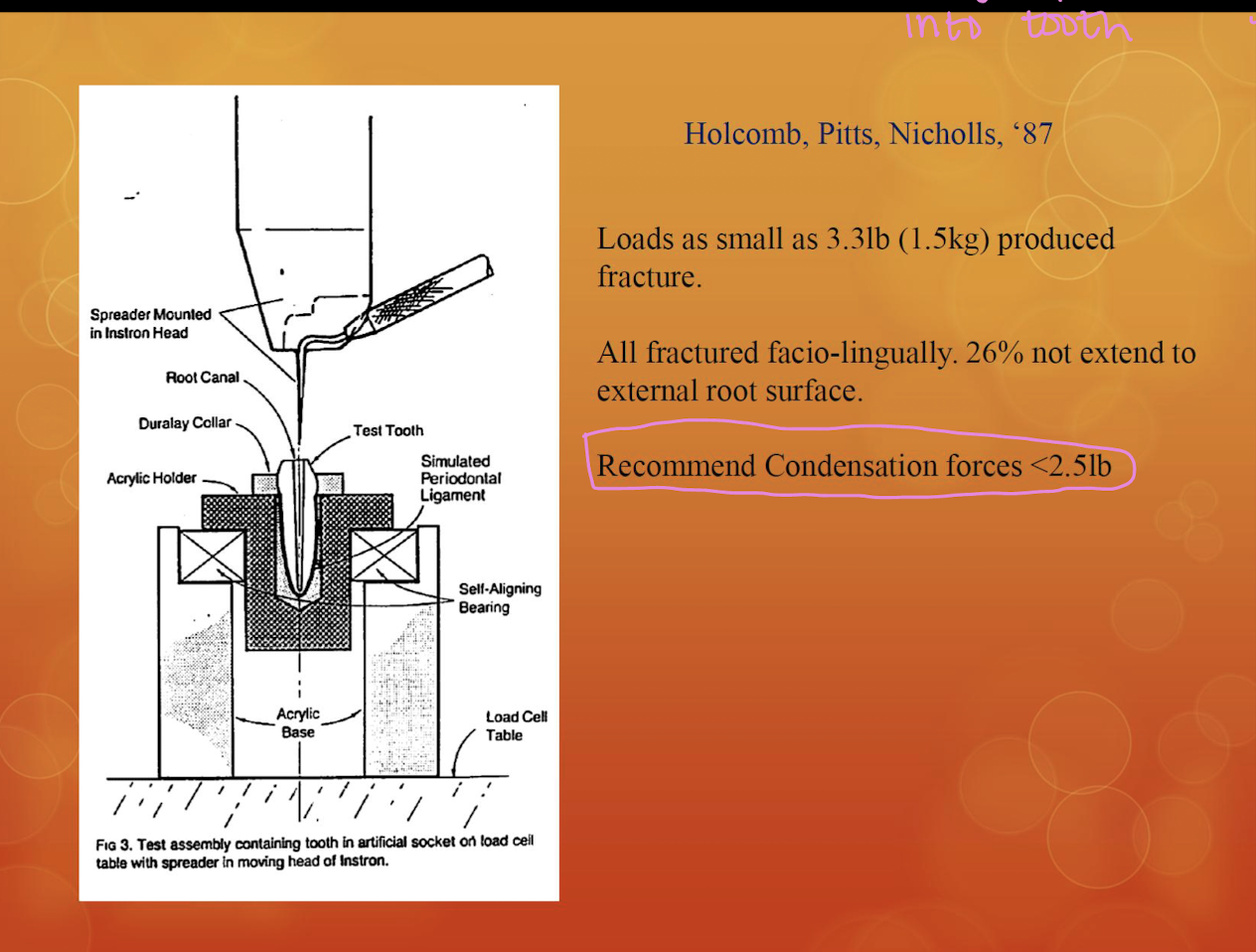
too much force applied w finger spreader, a tooth is likely to undergo
vertical root fractures
advantages of ZOE based sealers
long history of clinical use and well documented success
good flow
antibacterial
disadvantages of ZOE based sealers
stain (earlier formula)
shrinkage
cytotoxicity
solubility
advantages of resin-based epoxy methacrylate sealer
good adhesion
flow
hydrophillic
disadvantages of resin-based epoxy methacrylate sealer
polymerization shrinkage
cytotoxicity
advantages of calcium hydroxide-containing sealers
antibacterial
biocompatible
osteogenic
disadvantages of calcium hydroxide-containing sealers
high solubility
poor adhesion and seal
advantages of silicon-based sealers
dimensionally stable
slight expansion (.03%)
moisture-resistant
low solubility
thixotropic
biocompatible
disadvantages of silicon-based sealers
lack of flow
shorter working time
not antibacterial
properties of bioceramic sealers (3)
inorganic, non-metallic, biocompatible
bioceramic sealers are based off _____________ that has shown to be very biocompatible and _______________ manufactured as a single paste system
mineral trioxide silicate (MTA) calcium silicate; calcium silicate based sealer
endosequence of bioceramic sealer contains:
zirconium oxide
calcium silicates
calcium phosphate monobasic
calcium hydroxide filler
filler
thickening agents
key features according to brassler, of bioceramic sealer
biocompatible and osteogenic
non-resorbable
chemical bond of sealer to dentin
chemical bond of sealer to BC and GP points
less expensive than carrier technique
highly antibacterial (+12 pH upon setting)
can be used as an intra-canal medicament
highn radiopacity
hydrophillic
hydroxyapetite producing
user friendly
smaller particle size
no/zero shrinkage
bioceramic sealer kills ____________ within 2 min of contact
enterococcus faecalis
working time for bioceramic sealer
30 min
setting time for bioceramic sealer
3-4 hrs
particle size of bioceramic sealer
.2-.4 um
bioceramic sealers and MTA are both…
bioceramics → they are similar
_______________ is a refined bioceramic which has a much smaller particle size and a much better viscosity
endosequence BC sealer
endosequence BC sealer is a ___ generation bioceramic
2nd
MTA is a ___ generation
1st
bioceramic sealer is a medical grade bioceramic based off the properties of…
MTA that is Portland cement w the heavy metals removed
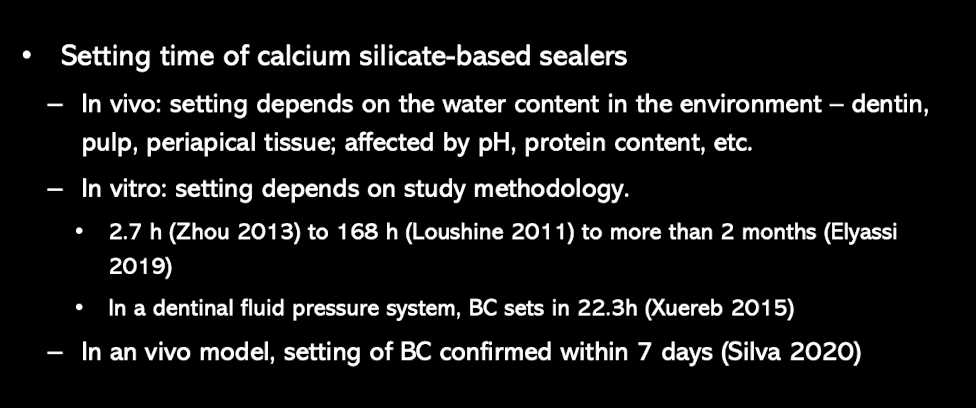
setting time of calcium silicate sealers
can depend on water content in the environment but confirmed to be 7 days
bioceramic sealers _________ and ________ allow it to create an interface between the sealer, gutta percha, and dentin
viscosity; small particle size
advantages of bioceramic sealers
hydrophilic
good sealing ability
adequate working time
dimensionally stable
bacteriostatis/bactericidal
biocompatible
_______ (min/max) volume of gutta percha does NOT seal, whereas the _____ (min/max) of sealer seals
max; min
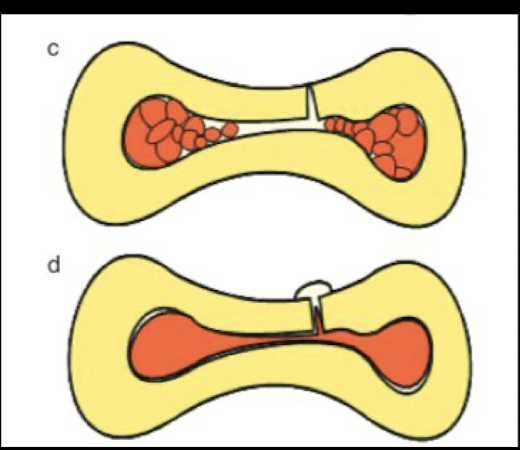
which is showing cold lateral condensation vs warm vertical condensation
C: cold
D: warm
advantages of single cone obturation
time efficient
no special equipment needed
good length control
disadvantages of single cone obturation
considered inappropriate when used w traditional sealers
more voids and leaking in large/oval canals
advantages of single cone obturation w bioceramic sealer-based obturation
time efficient
no special equipment needed
good length control
dimensionally stability prevents the formation of voids and gaps after the sealer sets
disadvantages of single cone obturation w bioceramic sealer-based obturation
more voids and leaking in large/oval canals
in the single cone obturation w bioceramic sealer-based obturation technique, gutta percha is used as a delivery tool to help generate….
hydraulic pressure to distribute the sealer (we do NOT do this technique)

9 steps of modified single cone w BC sealer obturation technique
MAF radiograph
dry canal w paper point
select matching WOG GP
confirm tug-back
master cone RG
apply sealer w sterile K file CCW → 1 size smaller than MAF and short of WL
“butter” master cone and seat to WL
apply accessory cones as needed for large/oval canals → if using .02 taper GP for modified lateral condensation
sear GP off within 1 mm facial of CEJ or at orifice in multi rooted teeth
what is an alternative to this step in the modified single cone w BC sealer obturation technique
“apply sealer w sterile K file CCW → 1 size smaller than MAF and short of WL”
coat sterile GP w sealer, place 2 mm short of WL to coat canal walls
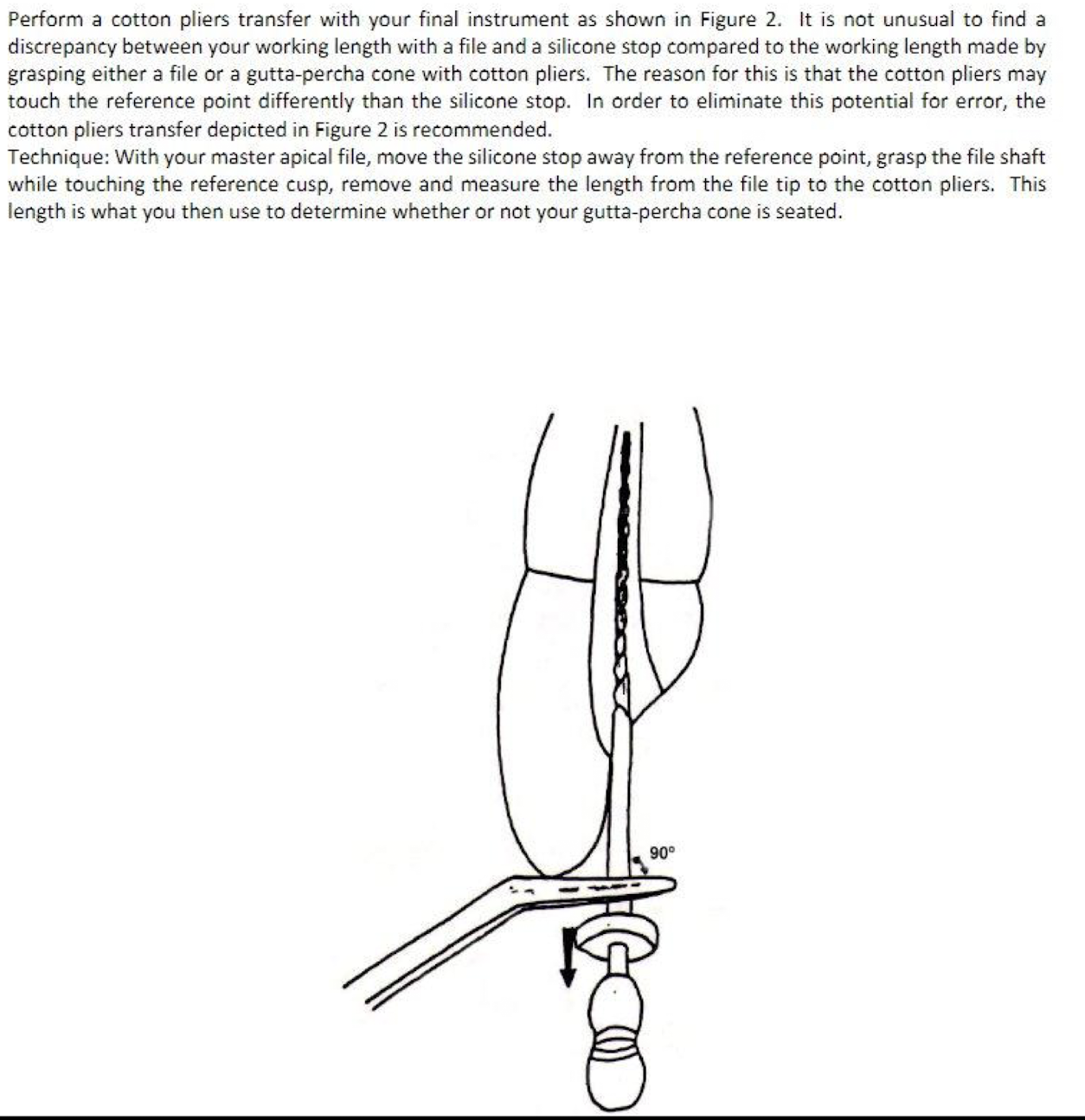
what should you use to eliminate the discrepancies between your working length w a file + silicone stop compared to the WL made by grasping either a file or GP cone w cotton pliers
w MAF, move silicone stop away from reference point → grasp the file shaft while touching the reference cusp → remove and measure the length from the file tip to the cotton pliers → use this length to determine whether GP is seated
initial condensation radiograph has what
master cone GP
sealer
accessory if needed