The kidney
1/24
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
25 Terms
Briefly explain the two functions of the kidney
excretion - removal of nitrogenous waste from the body
osmoregulation - the control of the water potential inside the body by maintaining water and solute conc.
Explain how nitrogenous waste is taken to the kidney for excretion
Proteins are broken down into amino acids which are transported to the liver where most are distributed around the body to build new proteins in cells. the excess is deaminated in the liver by removing the amino group and converting it to urea. It is then taken to kidney for excretion.
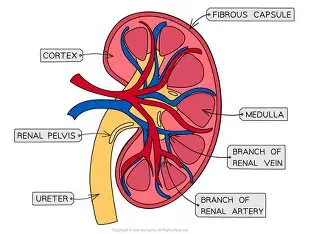
Explain the structure of the kidney
Draw and label the fine structure of the kidney nephron and what is a nephron
A nephron is an individual filtering unit

Explain ways to identify microscope slides of the cortex and medulla
cortex
glomerulus - lots of vessels
Bowmans capsule - large white curved
PCT - cuboidal cells
Medulla
No glomerulus or Bowmans
loop of Henle and collecting duct - lots of small circles
Where does ultrafiltration take place and how is it adapted for fast diffusion and how the filtrate is made
Bowman’s capsule and glomerulus
Its adapted for fast diffusion by
a high blood pressure - high hydrostatic pressure to counteract the water potential from lost of solutes in blood. This is done by: Efferent arteriole has a smaller diameter and lumen compared to afferent arteriole so the blood builds up in glomerulus and there is higher blood pressure. Also its under heart control - ventricular systole
Basement membrane of collagen and glycoproteins act as a molecular filter - selectively permeable
Capillaries have fenestrae which are pores in a thin walled endothelium one cell thick wall
podocytes - squamous epithelium cells that wrap around the capillary to lower diffusion pathway and the slits are filtration slits
Stages of ultrafilitration
fenestrae
basement membrane
podocyte filtrate gaps
bowmans capsule
This forms the fitrate of small mols like glucose, urea, ions, water, salts and amino acids
Explain what is selective reabsorption, where is it done and what are the PCTs adaptations and process
Selective reabsorption takes place in the kidney proximal covulated tubule of the the nephron. It is the reabsorption of useful products from the filtrate including
glucose and amino acids - by FD (co-transport with sodium (two for glucose and one for amino acid)) and sometimes secondary active transport - energy from diffusion of sodium ions down electrochemical gradient provides energy
ions - active transport or co-transport or FD
sodium - actively transported from cytoplasm of PCT into blood which means lower conc. grad. in the cytoplasm so diffuse via FD into cytoplasm with co-transport with glucose
water - osmosis
diffusion - some proteins and urea
ADAPTATIONS and process
The PCT includes columnar epithelium cells which have cilia that provide a large SA:V for absorption
they also have lots of mitochondria in their lumen for active transport
they also have basal channels in the strong basement membrane that have a large SA:V and concentrate a build up of mols to create conc. grad.
Tight junctions between cells of protein complexes prevent diffusion back of between mols.
Vasa recta vessels are close for short diffusion pathway and maintain conc. grad by taking away proteins
What will happen if glucose levels are too high in the blood
It means that there may not be enough transport proteins to reabsorb all glucose so it may be lost as urine
This is due to
type 2 diabetes - damage to insulin receptors
type 1 diabetes - lack of insulin from pancreas
How is water reabsorbed differently in parts of the nephron
The PCT (most of the water reabsorbed) and loop of Henle absorb the same amount of water no matter the conditions of the body but the collecting duct and DCT are selectively dependent on bodily needs
Explain the process of reabsorption of water in The Loop of Henle
In the ascending limb ions like CL and Na are pumped out by active transport to create a low WP grad. and due to impermeable walls no water leaves to maintain WP in the medulla intertitular fluid .
This means that when water flows down the desending limb water leaves via osmosis due to permeable walls down WP gradient as their is a low WP in medulla. - no ions leave.
This means at the hair pin there is a concentration gradient built up so FD out of loop
The vasa recta is close to loop of Henle and maintains low WP by moving water along
The low WP in medulla benefits DCT and collecting duct as more water can be removed based on ADH needs too and a concentrated urine is passed into pelvis and ureter.
Explain how nitrogenous waste is dealt with in different organisms
Reptiles, birds and insects produce uric acid that is highly concentrated and low toxic as they need to conserve water they they have no excess water
fish can excrete ammonia straight into the water as no need to store
plants convert ammonia with a-keto glutamate to make glutamine which can be used to transaminate into any amino acids so no need for excretion.
Why is kidney failure a problem and how does it occur and give some treatments for them
It is a problem because if you can’t remove excess nitrogenous urea then it can build up and be toxic by compromising reactions
Causes
Diabetes - high levels of glucose in blood can cause proteins like albumin to force into filtrate which can damage glomerulus or cause linking of proteins - glomerulosclerosis
high blood pressure - can damage glomerulus which causes ultrafiltration issues and excessive loss of nutrients - low blood pressure pills
inherited issues eg. Alports disease - kidney transplant
K+ is needed for transmission of nervous impulses and is actively transported into all cells; concentrations of K+ that are too high or too low can disrupt nervous transmission. Control can be dietary (reducing or increasing K+ intake), or by taking drugs to reduce or increase reabsorption of K+.
Excessive loss of Ca2+ can lead to a reduction of calcium in bones and cause brittle bone disease (osteoporosis). Reduced loss of Ca2+ can lead to problems with hormonal production and the deposition of calcium salts in tissues such as the retina (can lead to blindness), muscle (leading to pain on contraction), and joints (pain during movement).
injury - surgery
High protein increases urea levels which can be converted to uric acid; this can crystallise and form kidney stones which can tear and damage tissues leading to bleeding. which can cause loss of proteins too
infection - antibiotics
autoimmune disease
What is dialysis and explain one of the types
It filters the blood like a kidney
Haemodialysis - using a machine to artificially filter the blood - need to come into hospital 2/3 times a week for hours
Blood is taken from the arteriovenous vein and passes to a dialyzer.
Here the blood is filtered through a artificial membrane into dialysis fluid where the conc. of solutes is controlled to change the amount of water and solutes removed.
The filtered clean blood then goes back to arteriovenous vein.
Explain another type of dialysis
petironeal dialysis
This is where a the blood is filtered through the petironeal membrane (selcetively permeable) into a cavity - petrioneal space until equilibrium is reached and cavity must be emptied.
List some advantages and disadvantages of the two dialysis
ADVANTAGES Effective removal of waste products | Schedule flexibility, easier to travel |
Care given by trained professionals | Few risks of dialysis-associated cramps |
Regular contact with other patients | Clinic visits limited to 1-2x a month |
Rapid correction of electrolyte imbalances | Patient and/or family involved in care |
No equipment to store at home | No need for needles or vascular access |
Treatment usually occurs only three times a week | Steady state therapy, gentler ultrafiltration |
Disadvantages | |
Vascular access surgery required | Permanent external catheter; “body-image” problems |
Use of large needles | No “off” days |
Schedule inflexibility | Risk of peritonitis |
Must travel to center three times a week | Risk of weight gain from dialysate |
Cramping with ultrafiltration | Must store dialysis equipment and supplies at home |
Risk of bacteremia (with tunneled catheter) | Need for self-monitoring of care |
what are kidney transplants and explain the types and differences
The kidney transplant is implanting a kidney from a live or deceased donor into a recipient that has the same blood group and antigens to reduce the risk of rejection by the immune system
Explain some advantages and disadvantages of live vs dead kidney donors
Living +
Shorter waiting time
Less risk of rejection
Shorter time between removal of kidney from donor and transplant into recipient
Donor makes an informed decision
Lasts longer (20+ years)
living -
Shorter waiting time
Less risk of rejection
Shorter time between removal of kidney from donor and transplant into recipient
Donor makes an informed decision
Lasts longer (20+ years)
Dead +
No need for dialysis
Feel healthier
Have more energy
Be able to work, travel and do other activities
Deceased donors not harmed by surgery
dead -
Long waiting time
Pain following surgery
Could reject the kidney
Need to take immunosuppressive drugs for the rest of your life
Increased risk of infection
Only lasts 10 to 15 years
What is osmoregulation, why does it need to be maintained
Osmoregulation is a homeostatic process to maintain osmosis to maintain enzyme and metabolites rate of metabolism by controlling WP
why could the water potential falls
sweating
lots of salt intake
lack of water intake
What is the full process of osmoregulation
For reduced WP in blood
Osmoreceptors in the hypothalamus detect reduced WP
Secretory granules in the hypothalamus carry along axons ADH - antidiuretic hormone (dilutes dilute things) to the pituitary gland (posterior lobe).
It is then secreted into blood and travels to kidneys
It binds to membrane receptors on DCT or collecting duct
adenyl cyclase catalyses cyclic AMP production as a secondary messanger.
These two hormones cause vesicles containing aquaporins (intrinsic proteins that allow movement of water through pores) to incorporate with membrane of DCT or collecting duct and cause a series of transmission duct pathways to allow their pores enable water to be reabsorbed into medulla and vasa recta down WP
This creates concentrated urine
Exact opposite for higher WP
Done
What is homeostasis and what needs to be controlled within the body
Homeostasis is the maintenance of a constant internal environment in contrast to the external environment to protect the cells and keep metabolism rate stable
Factors that need to be controlled-
body temperature
pH
Water potential
Hormone levels
Waste products - eg. Nitrogenous waste
What is negative feedback and explain how this is used to maintain homeostasis
It’s a change in the system to reverse a change caused by the environment
It’s starts at a set point and then an input change in system causes the receptor to detect this change and via sensory neurons send a message to the co-ordinatior to give the effector a response - usually a hormone to counteract change.
What examples are there of negative feedback
Glucose - if levels are too high insulin converts glucose to glycogen and glucagon coverts it back to glucose if levels are too low
temp - too low and respiration rate increases to generate energy for heat and vessels constrict to prevent loss of heat. for too high - dilate
What is positive feedback
Where the effector causes a change that doesn’t counteract but changes it more. The stimulus for this change is also affected by this effector to complete the loop