medical imaging pathologies
1/175
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
176 Terms
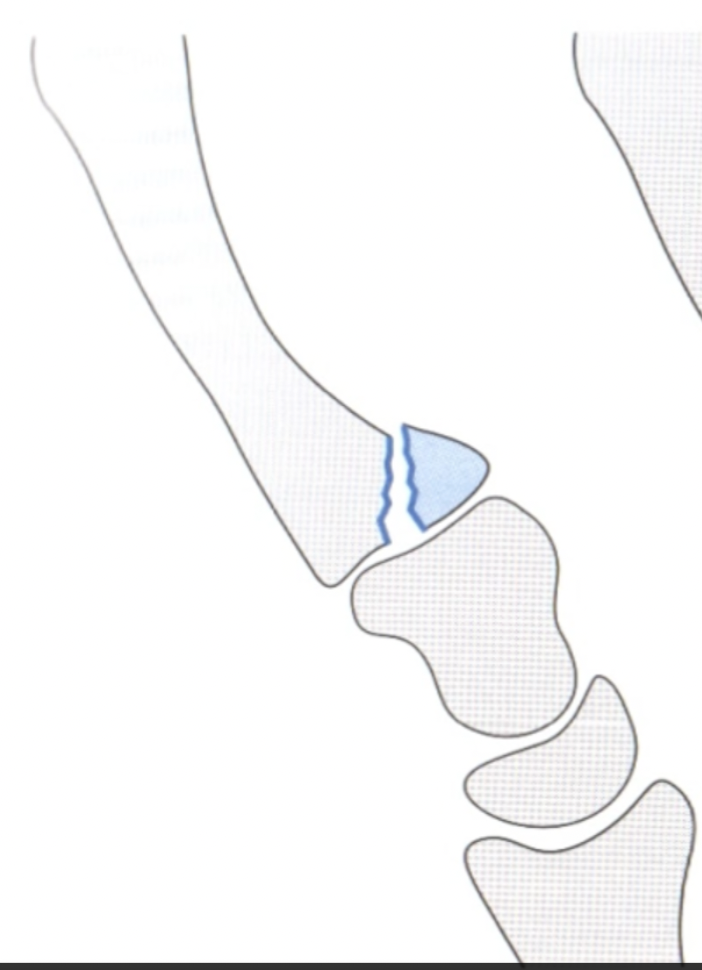
Bennet
Oblique avulsion# of metacarpal base
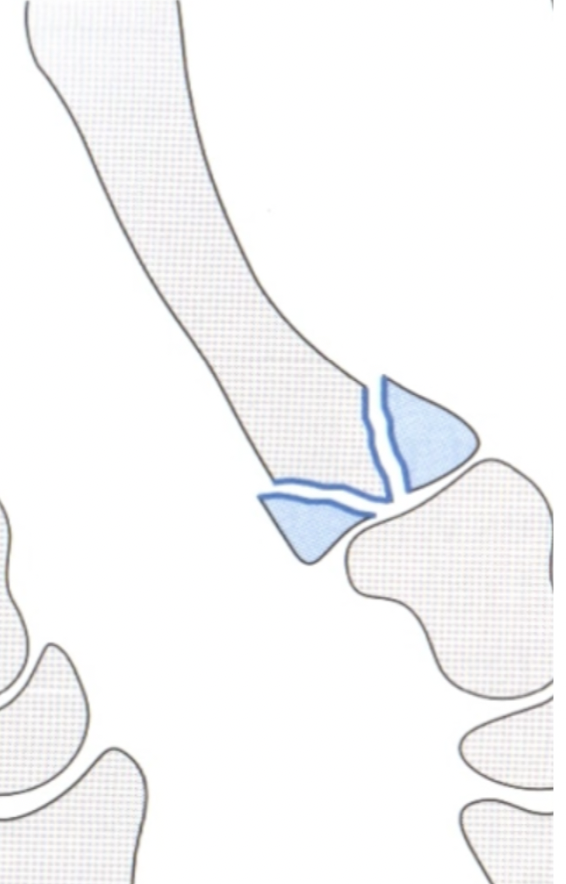
Rolando
Y shaped or comminuted # of metacarpal base
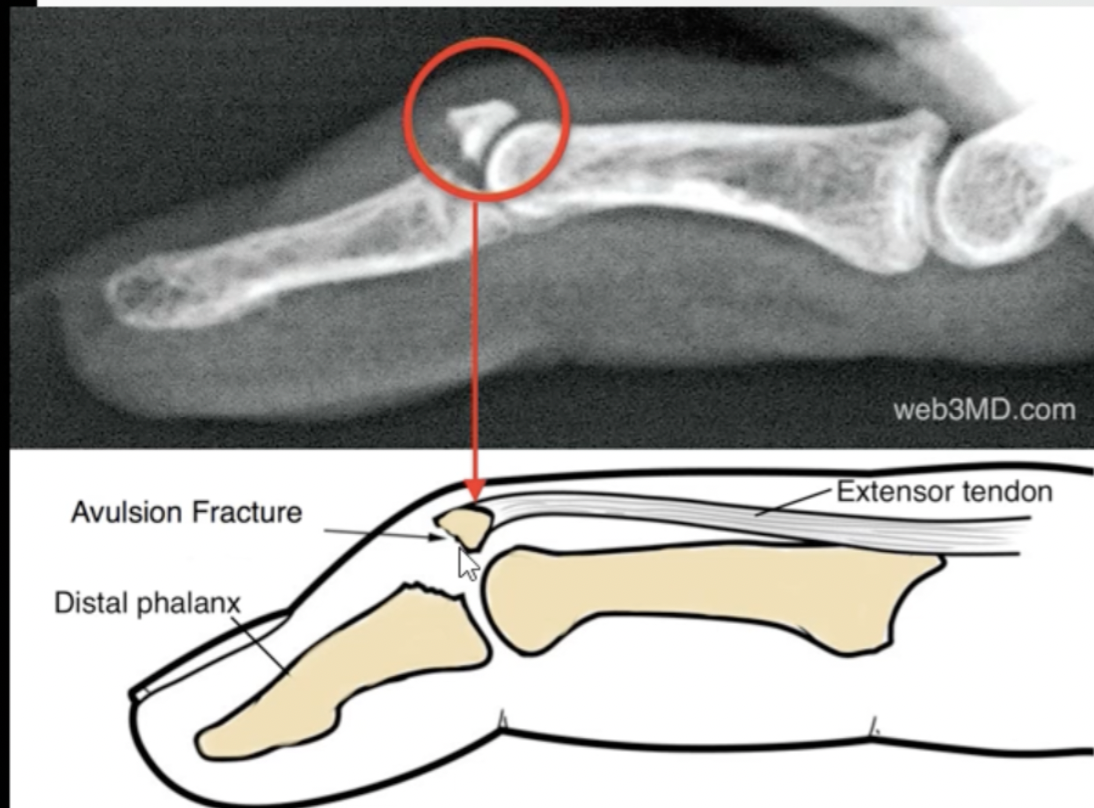
Mallet finger
distal phalanx
small bone fragment pulled away by the tendon
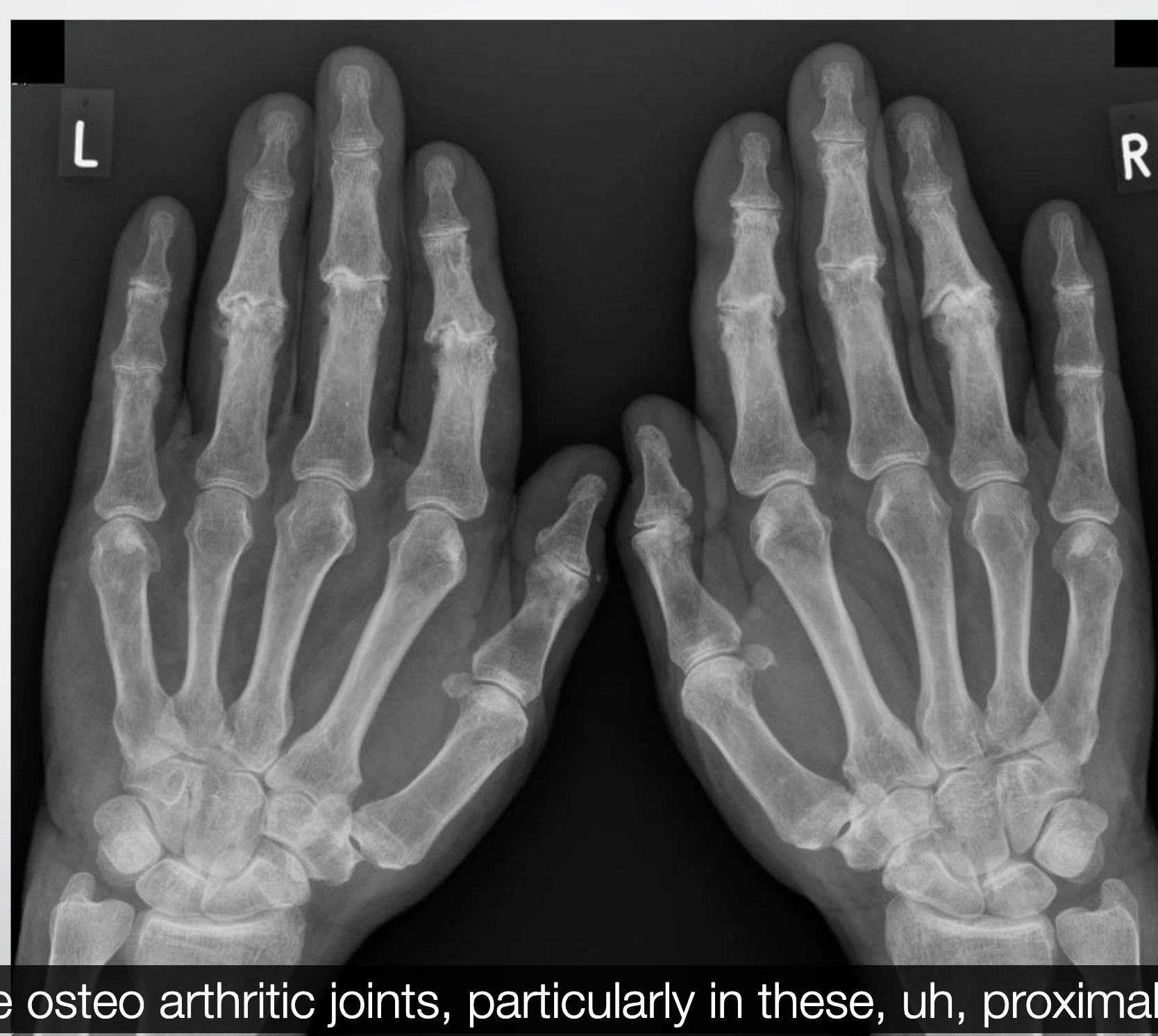
Osteoarthritis
Soft tissue swelling
Sclerotic margins
Joint space loss
Bony cysts
Bony spurs
boxers fracture
A boxer's fracture is a break in the neck of the 5th metacarpal

joint replacements in fingers

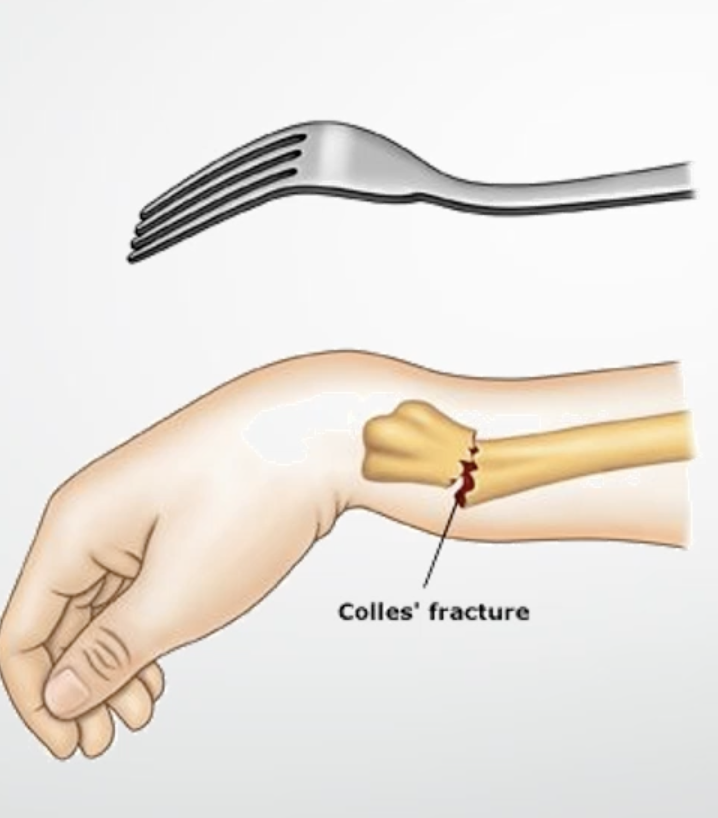
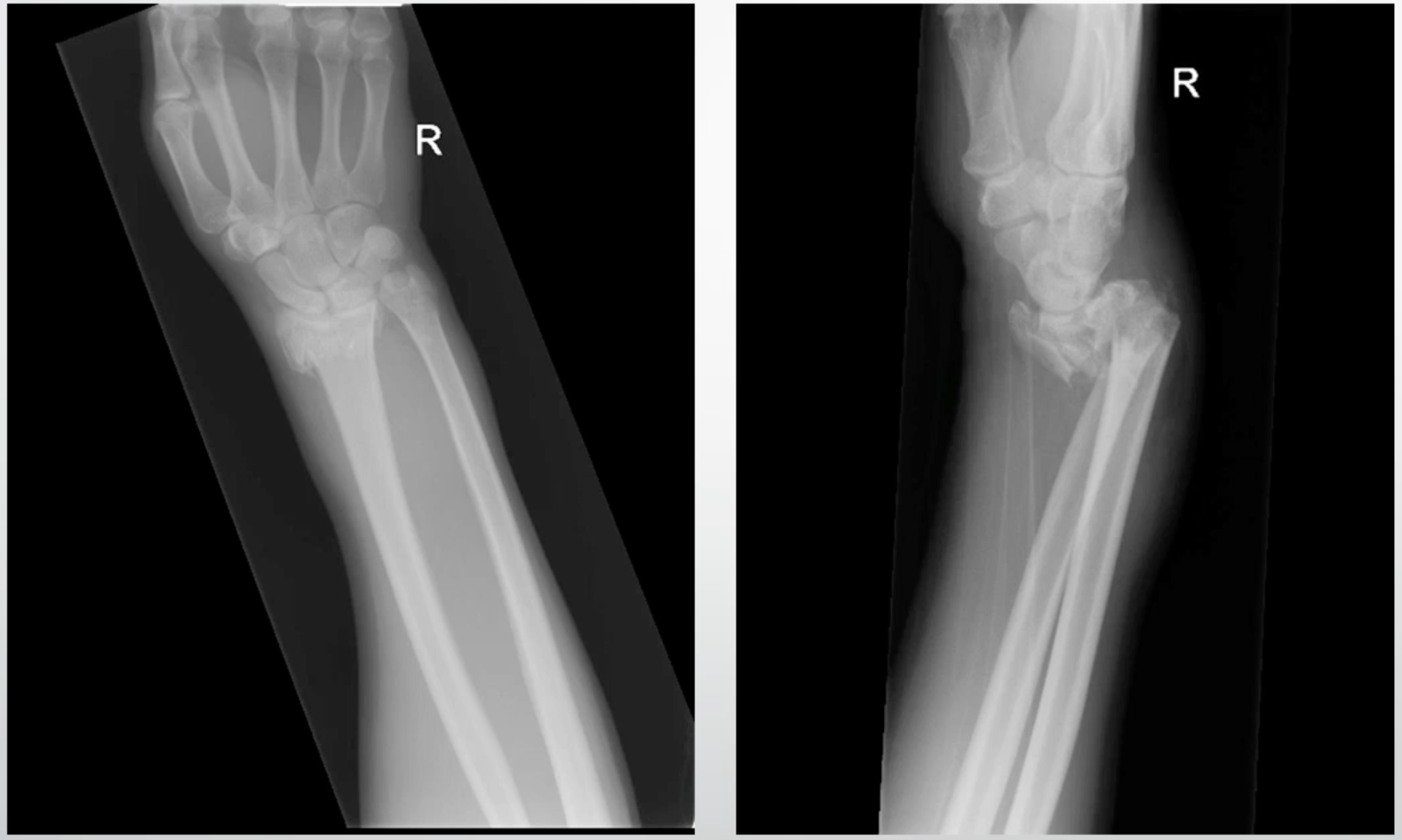
colles fracture
radius tilts posteriorly when its fractured
Smiths fracture
radius tilts anteriorly when fractured
Scaphoid interpretation
Accounts for more than 60% # of the wrist
3 locations
Distal pole
Waist
Proximal pole
Major blood supply through distal pole

Galeazzi
Distal radius + dislocation distal radioulnar joint

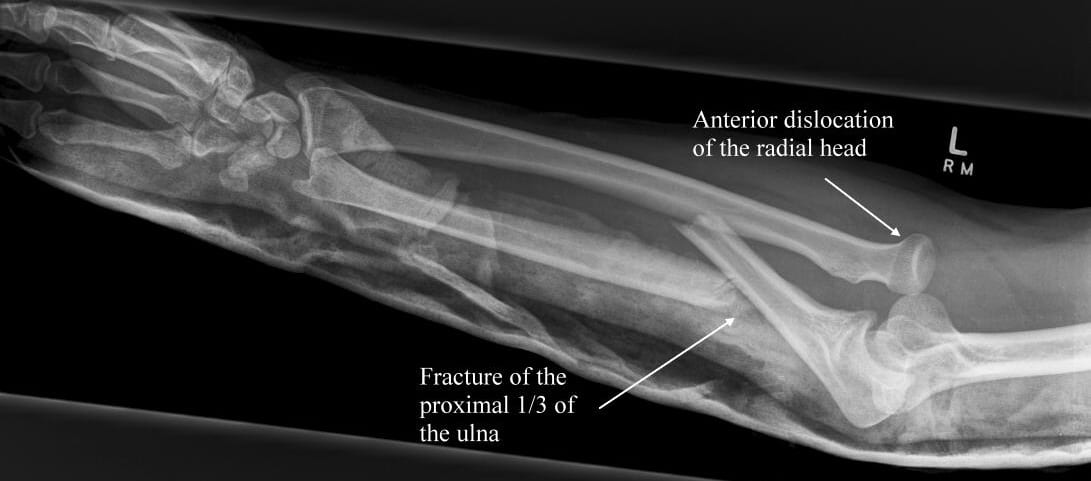
Monteggia
# proximal ulna + dislocation of the radial head
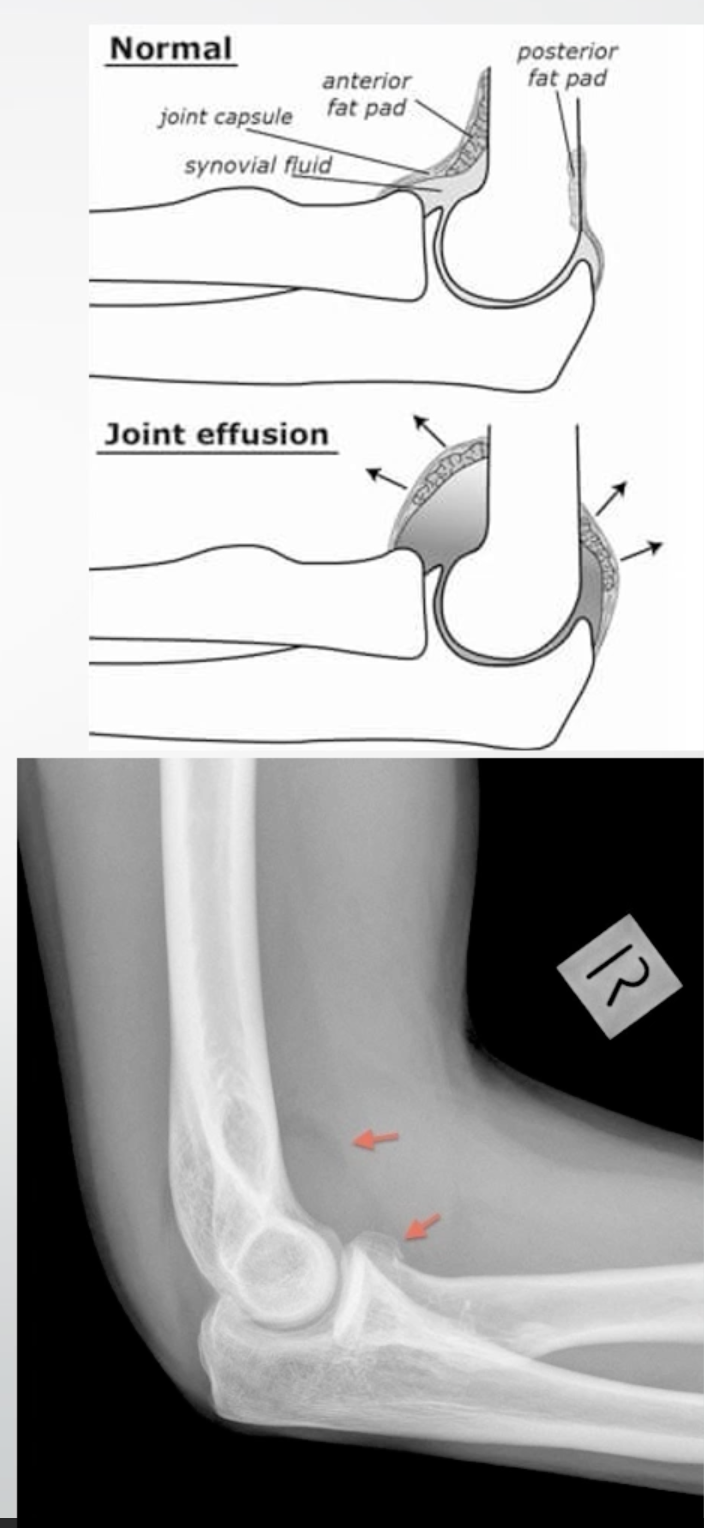
Sail sign
Raised anterior and/or posterior fat pad on an elbow radiograph
Indicates joint effusion, possible fracture
Mason classification - radial head fractures
Type I - no displacement
Type II - displaced # with separation
Type III - comminuted
Type IV - with elbow dislocation
mason classification
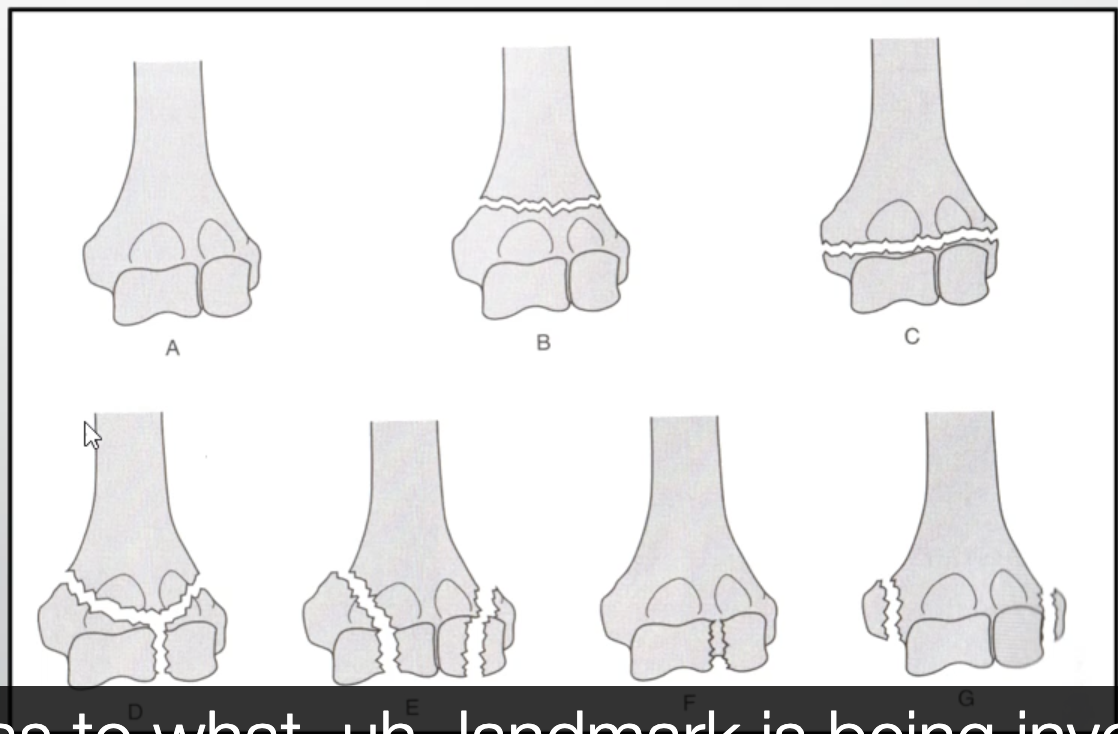
distal humerus fractures
FOOSH with flexed elbow
B supracondylar
C transcondylar
D intercondylar
E condylar
F articular
G epicondylar
Olecranon fractures
Fall onto flexed elbow or forceful contraction of triceps
Mayo classification
I, II, and III - level of displacement
A and B - non communited/ communited
Post reduction - dislocations
Patient is numbed and the arm is manipulated to put the shoulder back into its socket
Puts head of humerus back into glenoid fossa
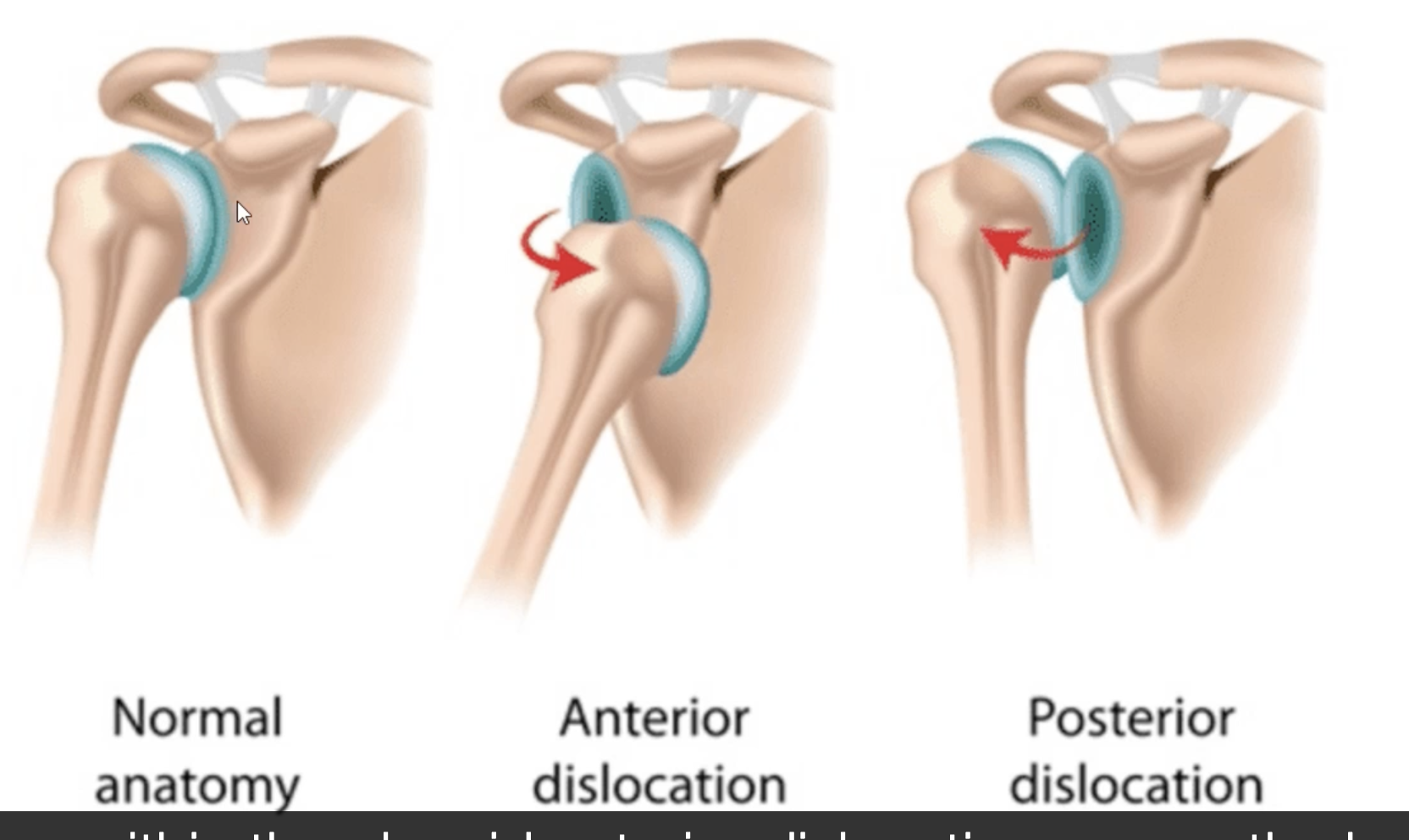
Types of shoulder dislocations
Anterior or posterior dislocations
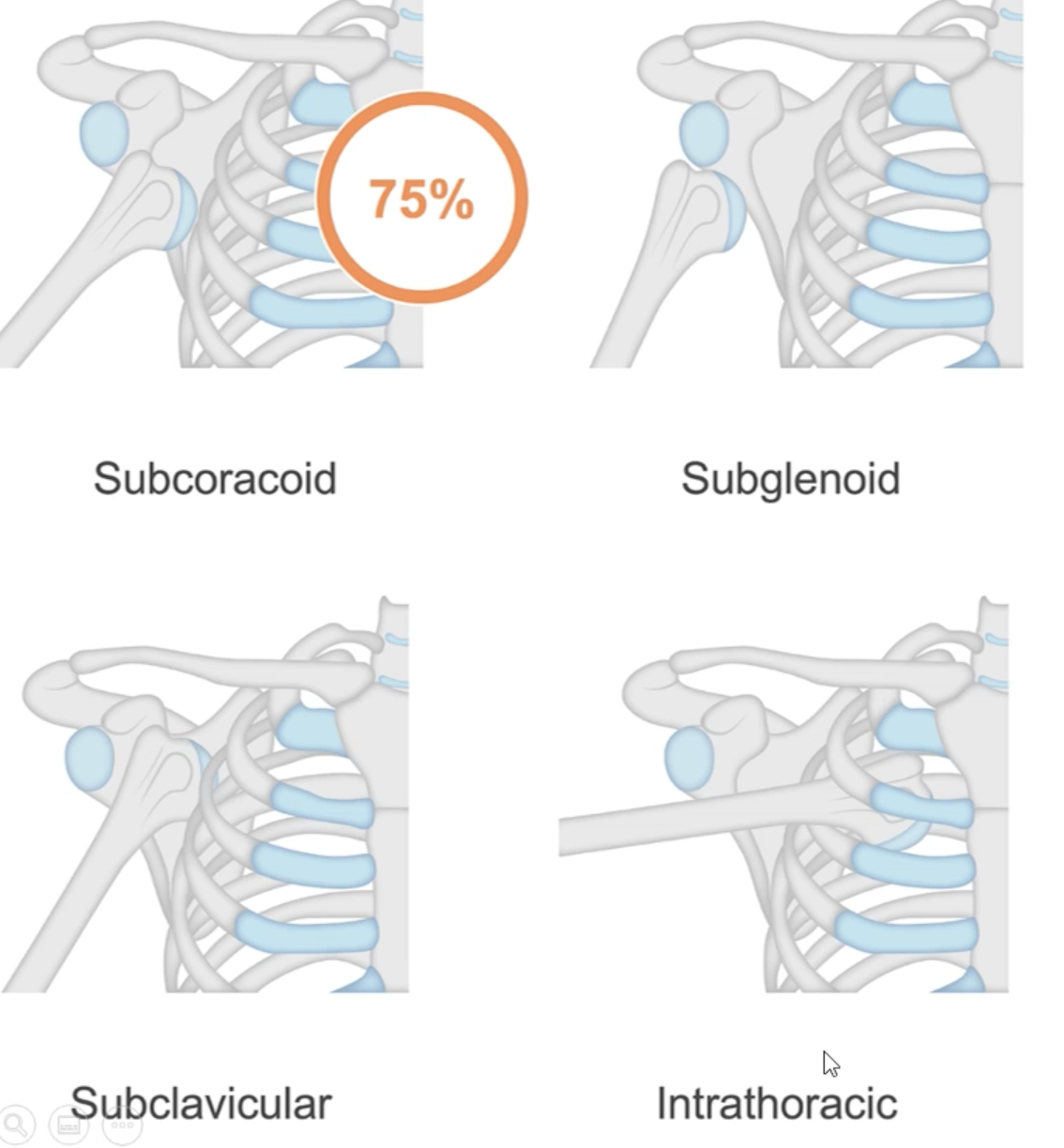
Anterior dislocation examples
Classified based on where the humeral head moves to
Subcoracoid
Subglenoid
Sub clavicular
Intrathoracic - rare
Anterior medial and inferior
Anterior more common than posterior
Posterior dislocation - shoulder
Less common, overuse injury
On exam: adduction and internal rotation (sling position)
Humeral head behind glenoid fossa

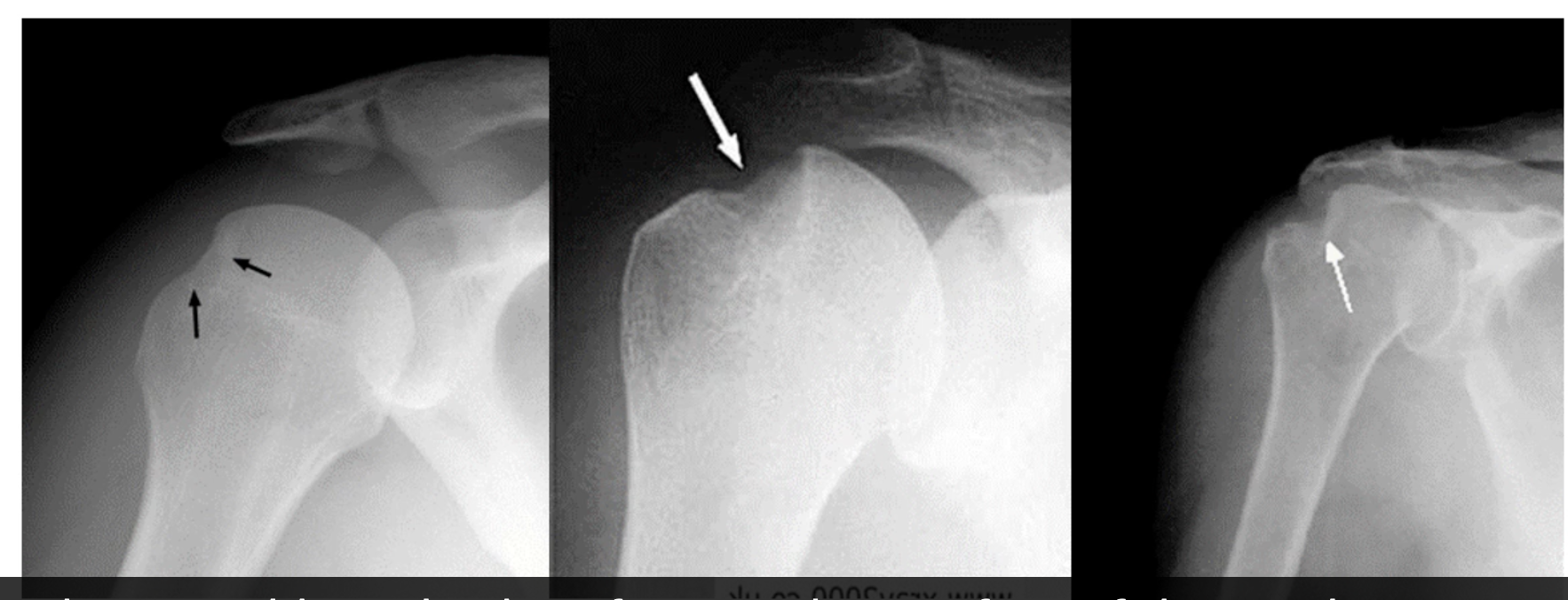
Hills-sachs lesion
Common post-anterior dislocations
Often the result of an anterior dislocation
Caused by humeral head strikes inferior glenoid
Divot seen on superior posterior lateral aspect of humeral head
Reverse hills-sachs lesion
Occur after posterior dislocation
Divot in anterior aspect of humeral head
Bankart lesion
Damage to inferior glenoid after anterior dislocation

Neck of humerus fracture
Communuted - multiple fragments
The humeral head is moving medially and superiorly

Scapula fracture

clavicle fracture
Communuted distal one third of clavicle
Clavicle moved superiorly and distal part moved inferiorly
Shoulder impingement
Compression of supraspinatus tendon, subacromial bursa and long head of biceps tendon
Due to decreased space under the coraco-acromial arch
Sub acromial spurs which can cause impingement particularly in older people
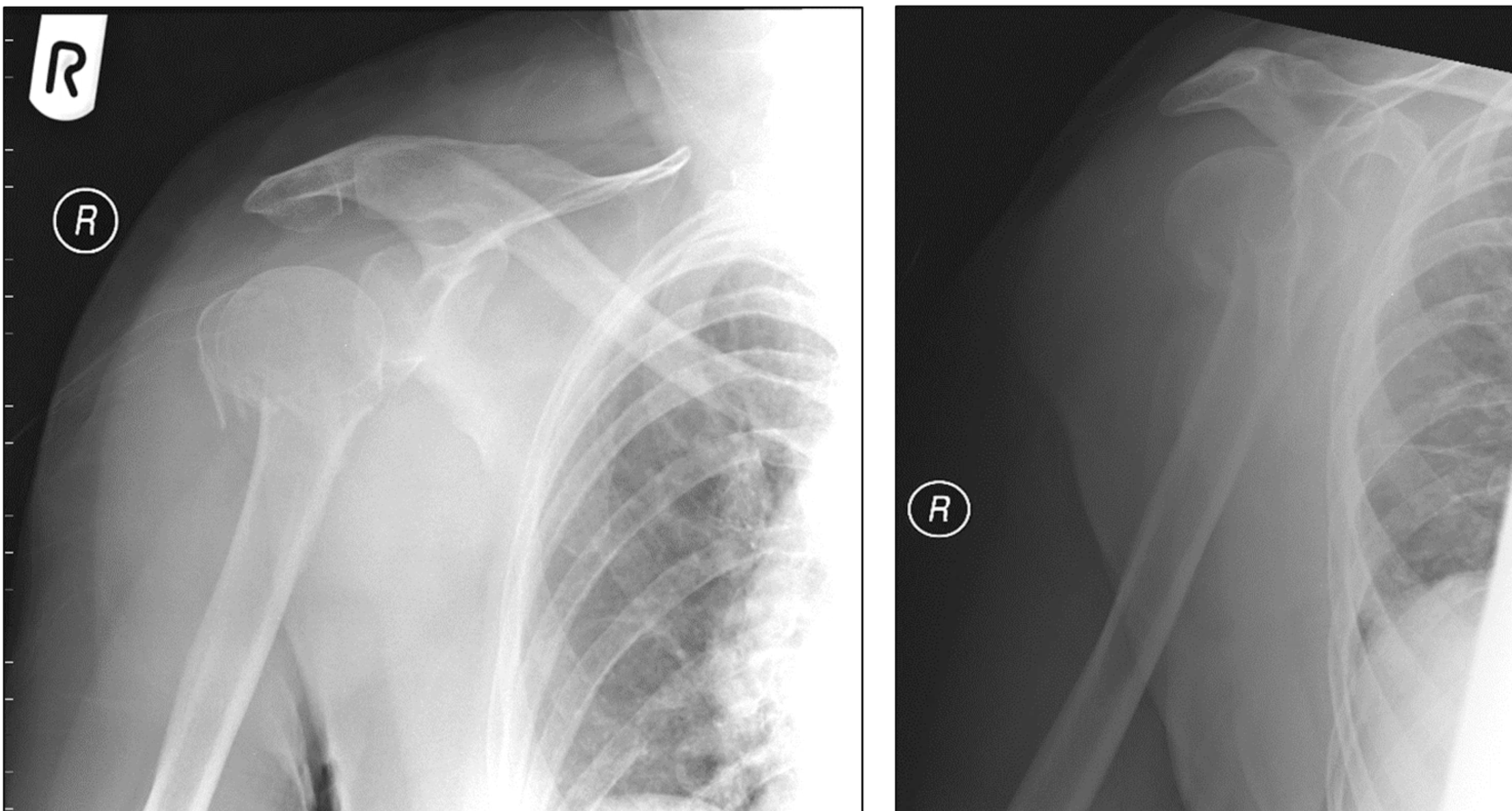
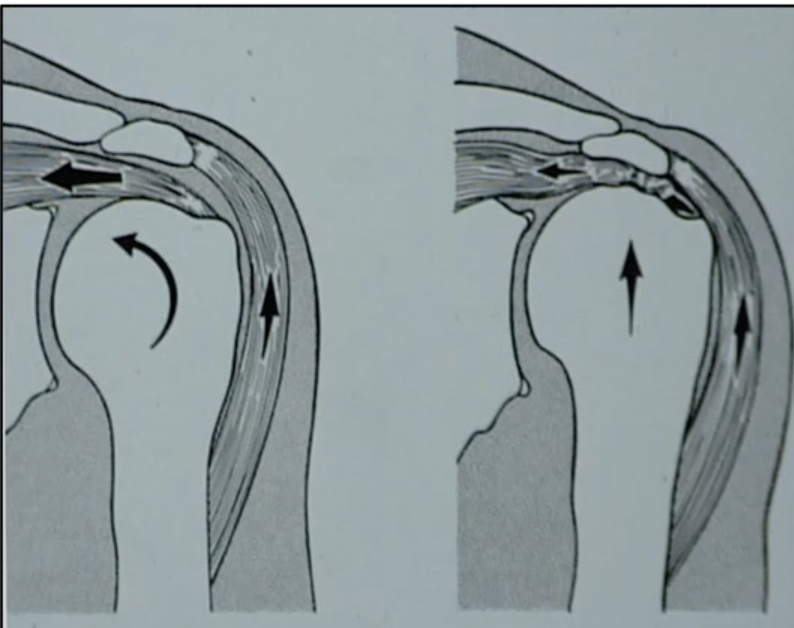
Rotator cuff tear/degeneration
Humeral head moves superiorly due to:
Weakening of rotator cuff pull medially
Deltoid pull superiorly
Calcific tendonitis
Deposits of calcium in tendons of rotator cuff
Pain and reduced ROM
Supraspinatus common

Osteoarthritis shoulder

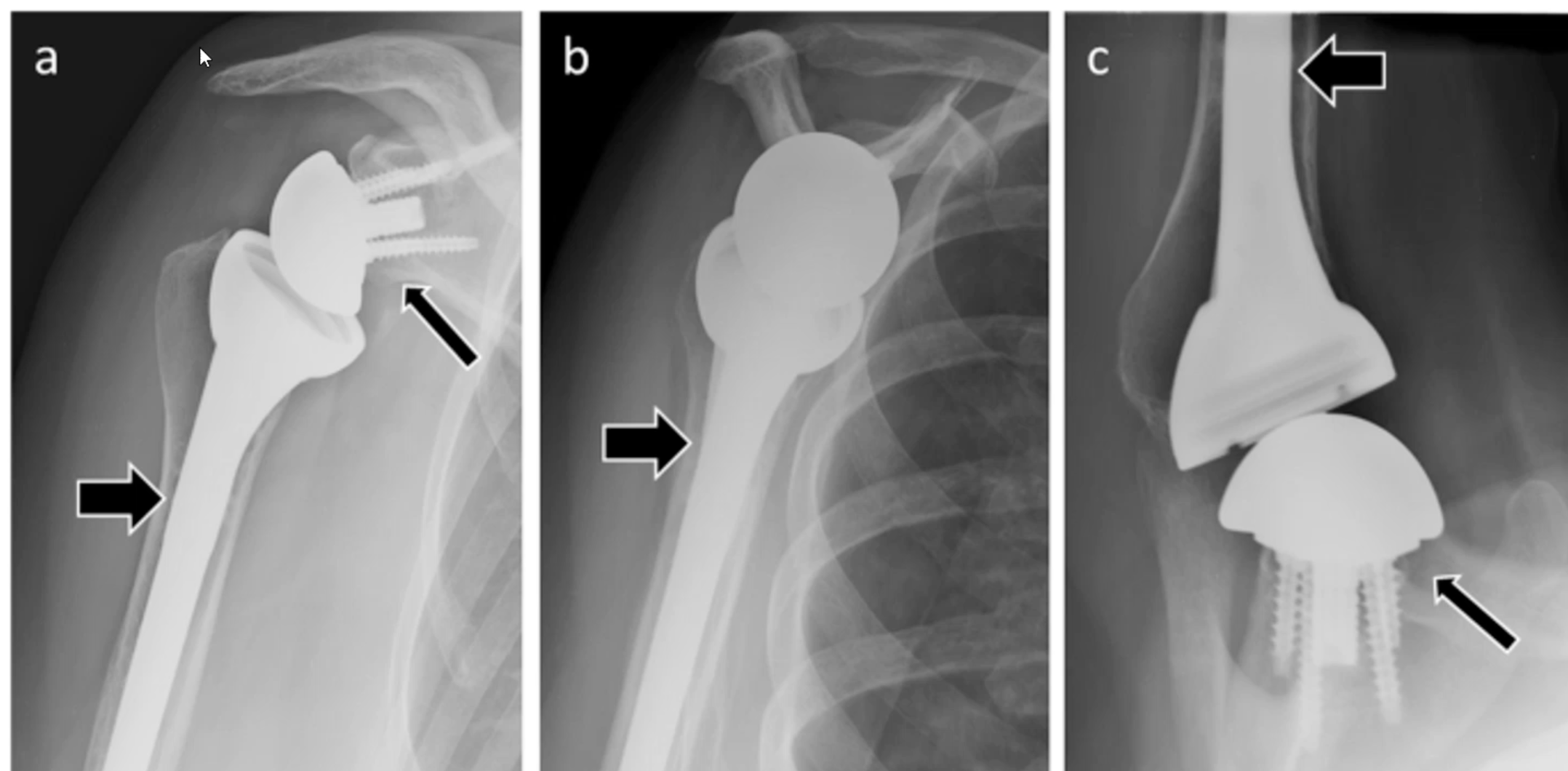
Shoulder replacement
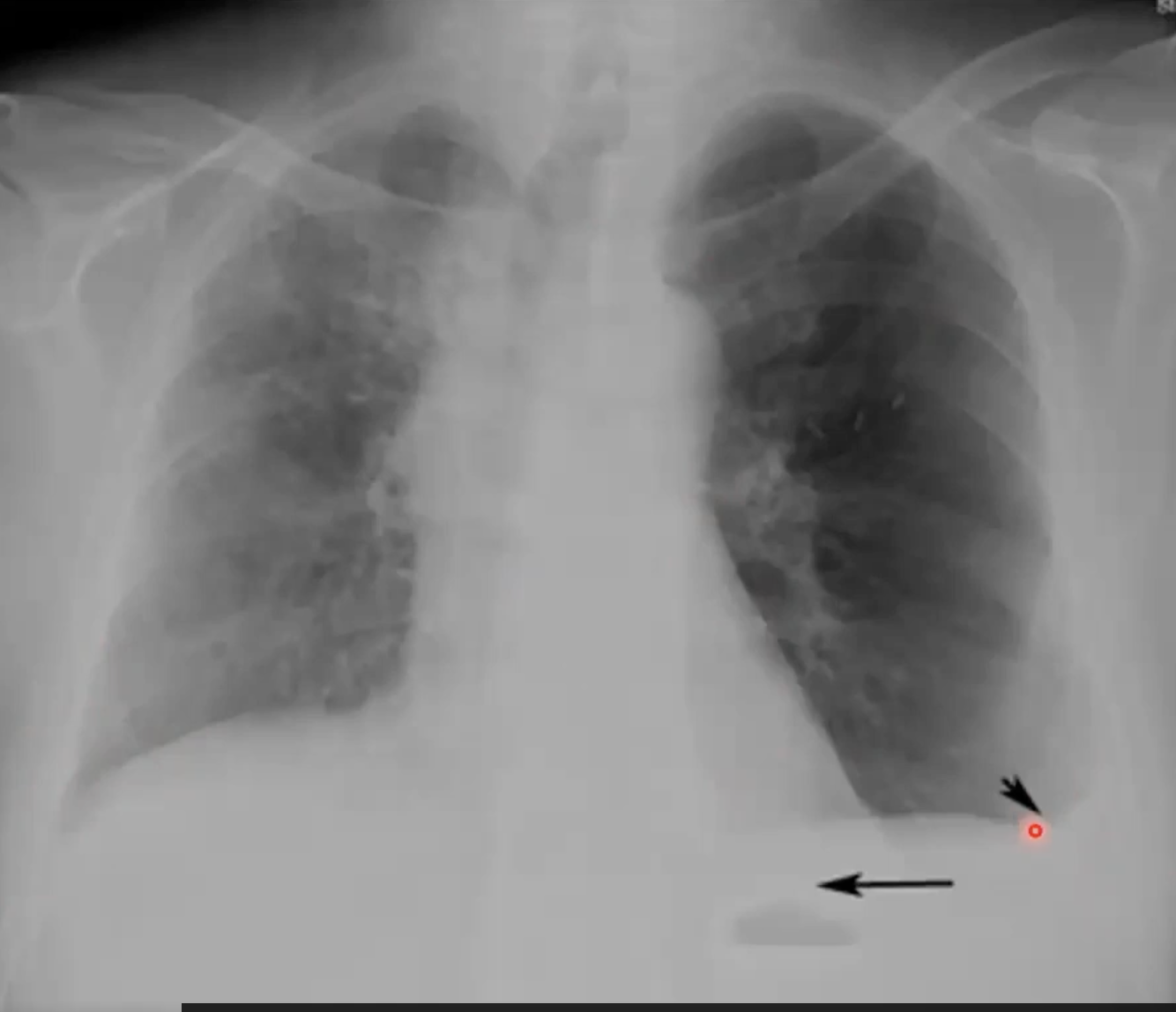
Pleural effusion can be seen as costophrenic angles are not sharp
When laying on the effected side you can see the fluid pooling at the bottom of the image with pleural effusion
Bones and soft tissue
Trace all the bones carefully (including the spine)
Looking for:
Fractures
Radiolucent or radiopaque areas
Dislocations
Destructive lesions
Assess for any unexpected soft tissue swelling
Airways/assessment of quality
Assess the quality of the image overall from a technical point of view
Assess the airways from the trachea down to the left and the right bronchus
Ensure the trachea is straight with no narrow points
The carina should never be wider than 100 degrees
Cardiac
Assess the cardiac border and ensure it is not obstructed
Assess the mediastinum, taking into account all structures that make up the mediastinum
Ensure the cardiac position is sound
Ensure the arch and upper mediastinum is not widened
Diaphragm
Ensure the diaphragm has a smooth border
The right hemidiaphragm is generally higher than the left due to the liver
Look for gas under the diaphragm - common on the left side because that is where stomach is (gastric bubble)
On right side is liver so shouldn’t be any air
Effusion/ extra thoracic
Assess for any effusions by checking costophrenic angles
Assess for any extra thoracic soft tissue issues/air where it shouldn’t be
Fields/fissures/foreign bodies
Check symmetry
Compare each zone for changes in density and volume
Start at the apex and working inferior and ensure the edges of the lungs are consistent
Evaluate the fissures for any unexpected changes in position
Check position for all FB that include lines or previously inserted surgical clips/layers
Good to see lung markings behind the heart
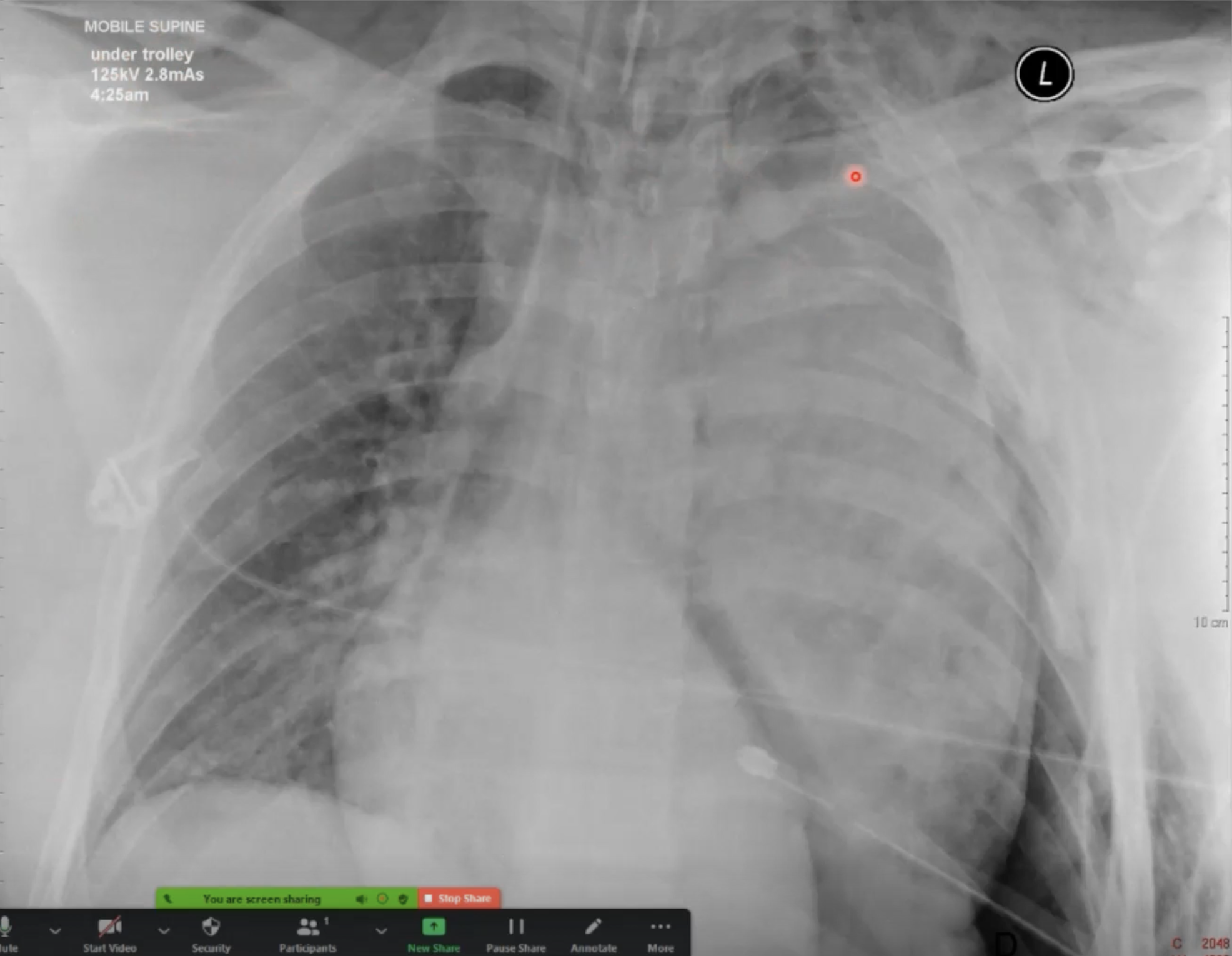
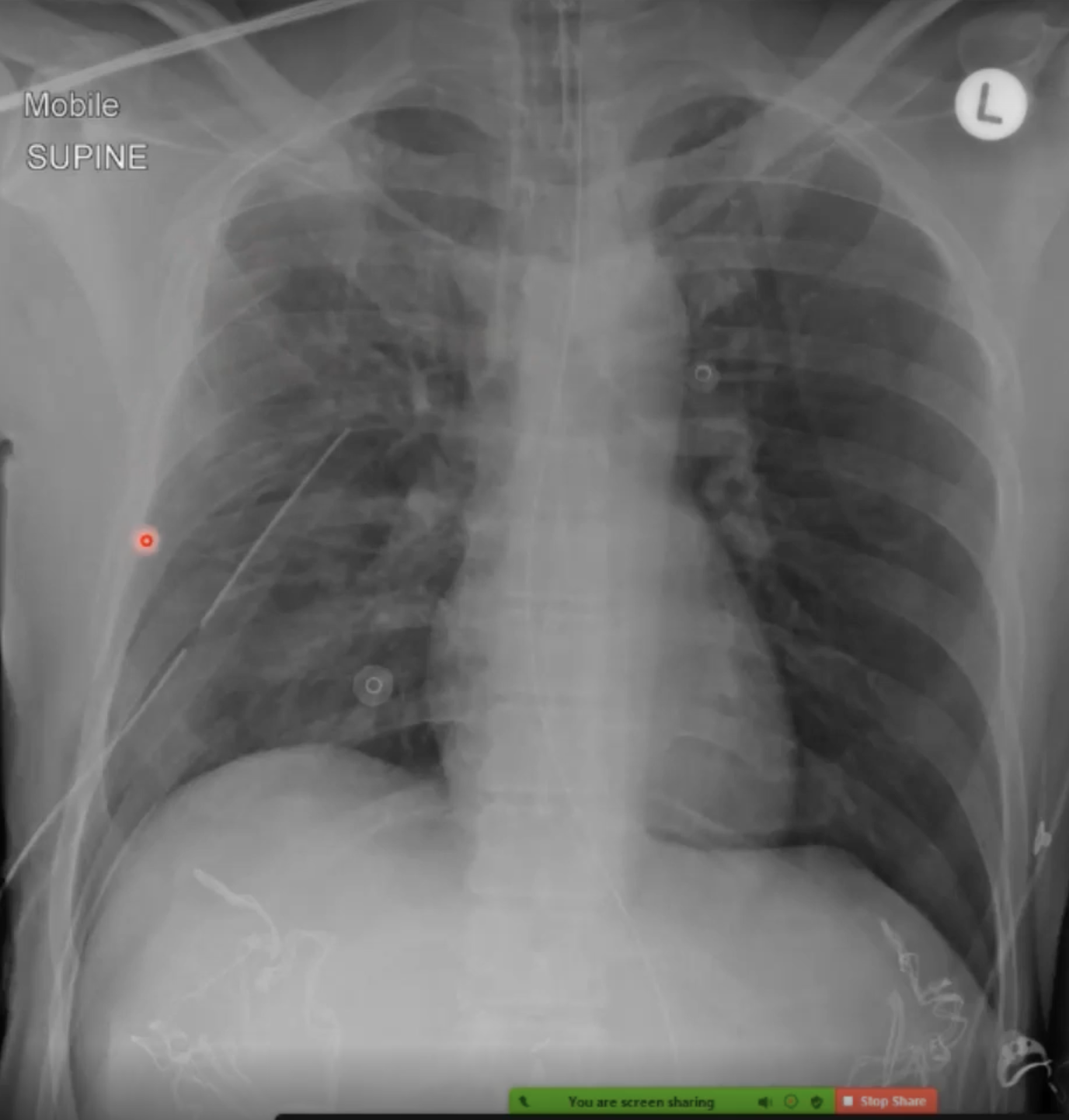
Iatrogenic devices
An xray cannot determine that a device is in the right place. Only in the wrong place
Clinical correlation is essential
Nasogastric tubes etc - need other things to determine it is in correct place

what devices are seen
Two clips holding two ECG lines
Through the trachea is the ETT
Metal wires in the chest which are sternal wires
Tube down from jugular vein into heart - CVC, swan ganz catheter
extrarathoracic devices
Breast implants
Attachments
pleural devices
Thoracostomy tube
Pigtail catheter
Tracheal and oesophageal devices
Nasogastric tube
Endotracheal tube
Tracheostomy tube
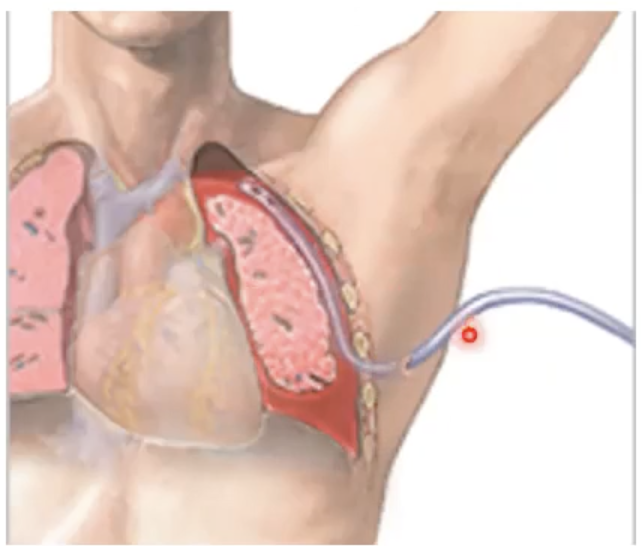
intravascular devices
CVC
PICC
Cardiac devices
Pacemakers
Cardiac prosthetic valve
Orthopaedic devices
Sternal wiring
vertebroplasty
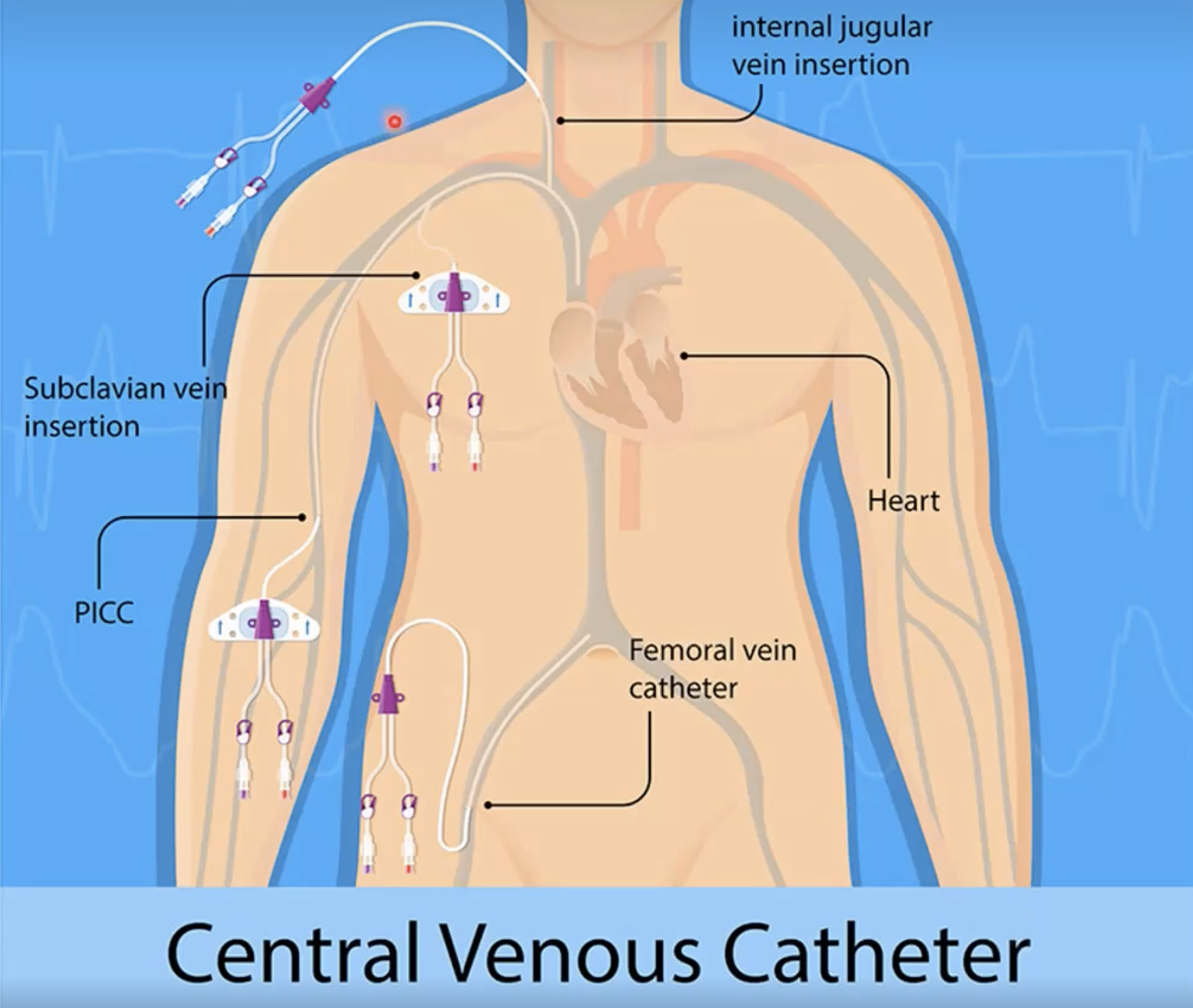
Can either go through the internal jugular vein into the heart or through the subclavian vein
If near the elbow it is a PICC line
Can also go through the femoral vein
Breast implants
Saline silicone
Many types
Unilateral or bilateral
Increased ST density
May extend beyond boundaries of the chest wall
May have well defined contours
Have an increased soft tissue density
Artefacts on chest images
Tubing and external ports
Sheets, pillows, clothing
ECG electrodes and leads
External pacemaker-defibrillator
Should be removed prior to imaging where possible
Should be included with interpretation
Thoracostomy tube use
Used for drainage of the pleural space
Air (pneumothorax)
Fluid (pleural effusion)
Pus (emphysema)
Thoracostomy tube structure
Flexible plastic tube
End and side holes
Attached to receptacle/water trap
Inserted under local antithesis
Flexible tube
Incision into a safe area of the thoracic cage
Tube passed through hole into pleural space
Stitched in
Thoracostomy tube complications
Haemorrhage
Infection
Rupture of lung tissue, liver, spleen, diaphragm
Re-expansion pulmonary oedema
Thoracostomy tube why image?
Check position - radio-opaque stripe, tube within pleural cavity
Look for complications - tip of tube not abutting the mediastinum, parenchyma or a fissure
Nasogastric (NG) tubes uses
Feeding
Drug administration
Imaging (contrast)
Aspiration of stomach contents
NG tubes structure
Single lumen rubber tube
Flaccid with guide wire insert for positioning
Narrow/wide
NG tube insertion
Usually inserted unguided
Guidewire for manipulation
Through nose (or mouth) down oesophagus, into stomach (or further)
Taped down
NG tube complications
Enters skull vault
Misplacement eg. Coiled up in throat/bronchus/too short/long
Rupture of pleura
NG tubes - why image
Ideally, should see entry point and able to track all the way down:
Positioning/rotation
Exposure
Leave wire in
Narrow/wide bore
Guide wire
Travels centrally down oesophagus
Tip past level of diaphragm
Aim is to have it be 10cm to the oesophageal junction
Endotracheal tube indications for
Assisted ventilation
Isolate trachea to permit control of airway
Prevents gastric distension
Direct route for suctioning
Administrations via ETT
endotracheal tube evaluation
Assessed on frontal chest radiograph
The carina should be projected over t5-t7
The desired position should be 5+/-2cm above the carina
In children, the trachea is shorter and desired position is 1.5cm above carina
When carina not visualised (due to technical factors) ideal position is the middle third of the trachea (T2-T4 level)
endotracheal tube issues
Most common malposition: tip in right main bronchus
Overinflation f the right lung and collapse of the left lung
Tube in larynx or pharynx
Damage vocal cords
Aspiration
Tracheostomy indications for
Airway obstruction at or above the level of the larynx
Resp failure requiring long term intubation
Paralysis of muscles that affect swallowing or respiration
Tracheostomy evaluation
Assessed on the frontal chest radiograph
Tip half way between the stoma and the carina
Above t3
Tip placement not affected by flexion or extension
Width of tube above 2/3rd width of trachea
complications
Subcutaneous emphysema
Pneumomediastinum
Pneumothorax
Tracheal stenosis
Chest trauma CXR role
What is the circulatory status
What is the respiratory status
Is there a tension in the pneumothorax
Is there a pericardial tamponade
Widened mediastinal/abnormal mediastinal contours important indicator of mediastinal haemorrhage
Injury to: in chest traumas
Pleural manifestation of trauma
Thoracic cage
Aorta and great vessels
Heart and pericardium
Pulmonary parenchyma
Chest xray is always the primary image taken in response to trauma
Pleural manifestations of trauma
Pneumothorax
Haemothorax/pleural effusion
Hemopneumothorax
Associated collapse/atelectasis
Passive relaxation/collapse - passive removal of alveolar air by simple pneumothorax, diaphragmatic dysfunction or hypoventilation
Compressive collapse - extrinsic intrathoracic compression by air, fluid, mass
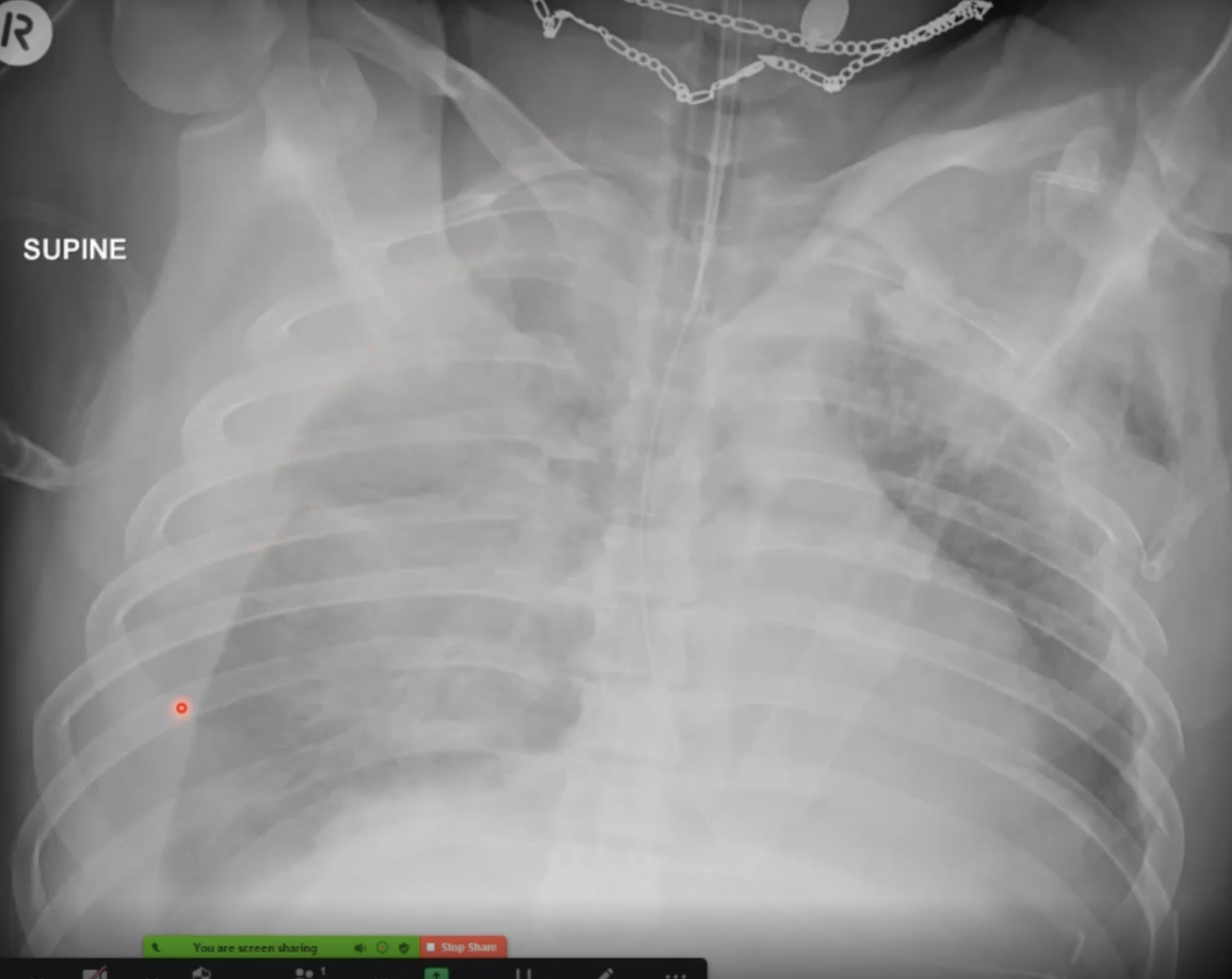
Multiple rib fractures, pneumothorax on the left side
Intercostal tube draining
Trachea is pushed to the right
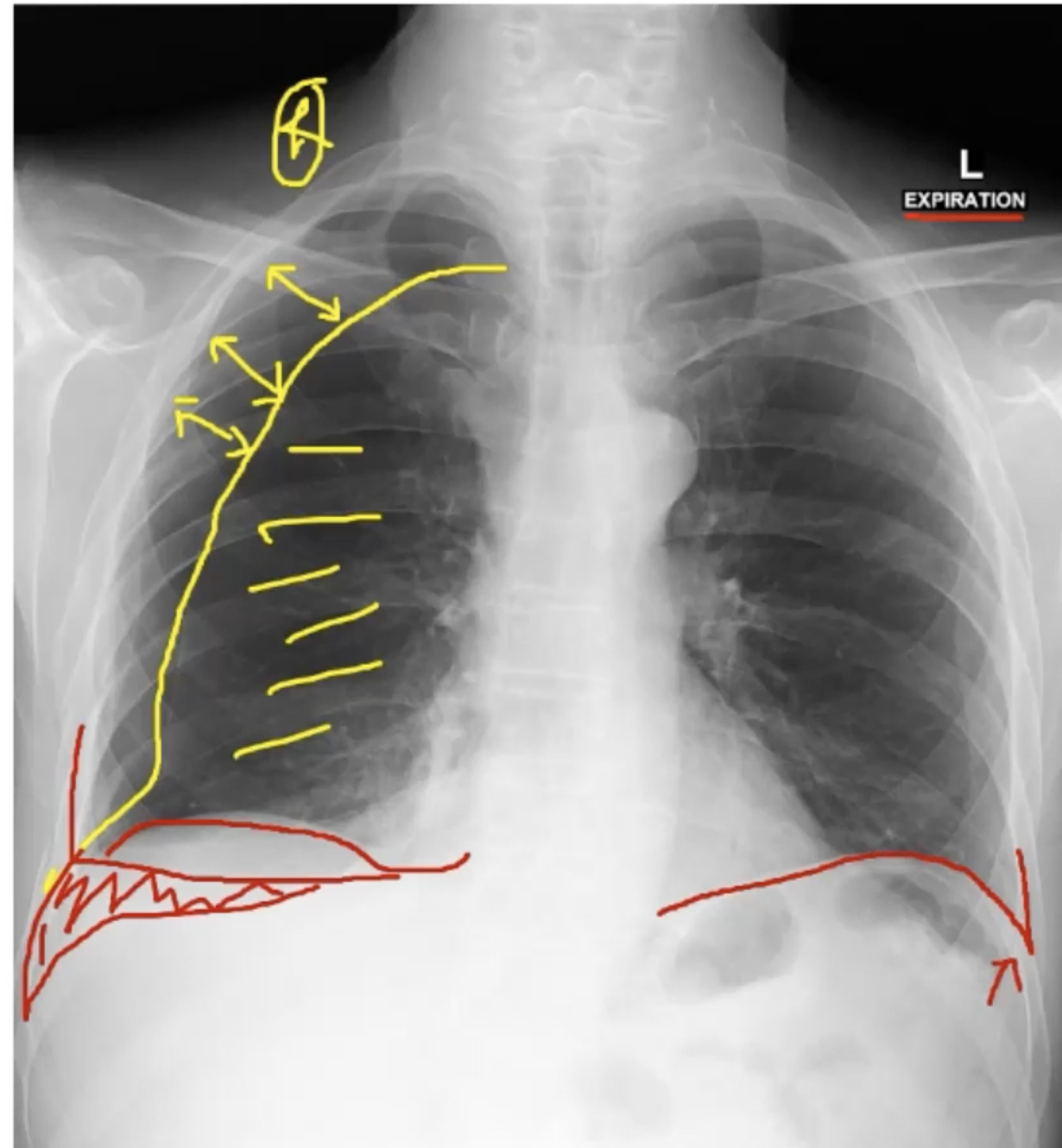
Pneumothorax
Presence of gas (Air) in the pleural space
Mechanism: injury to the lung, either by trauma or iatrogenic cause resulting in air leaking into the pleural space
Spine pneumothorax
Deep sulcus sign - abnormally prominent/deep costophrenic angle
Uneven lung density - affected lung may appear abnormally translucent
Subcutaneous emphysema - associated with rib fractures
Tube on right side - right sided pathology
Rib fractures on right side
Costophrenic angle is high and the edge goes too deep - pneumothorax
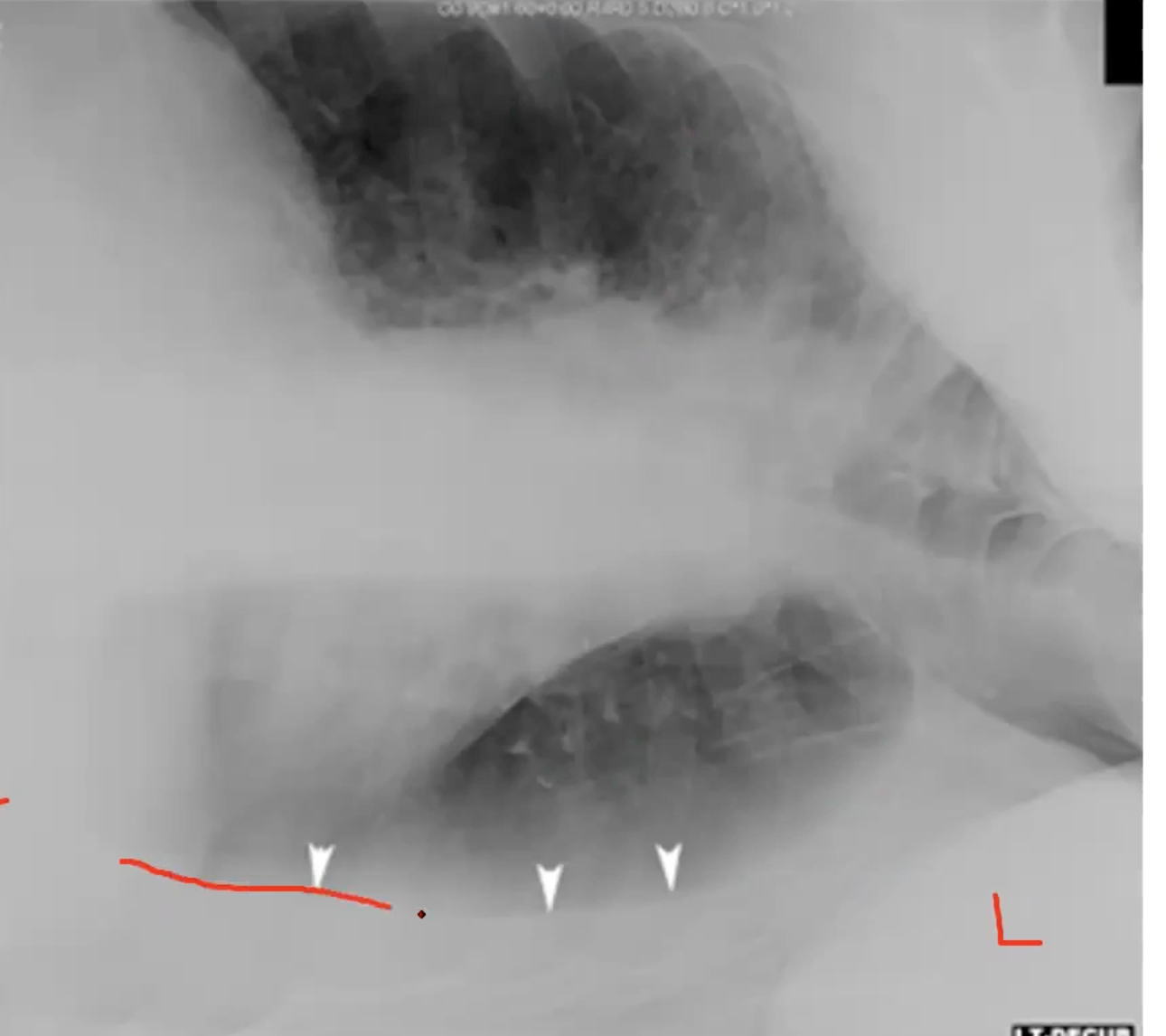
Haemothorax
Presence of blood in the chest, term used to define pleural effusion due to accumulation of blood
Mechanism
Injury to the lung from penetrating or blunt trauma
Can occur without trauma = spontaneous haemothorax (malignancy, vascular rupture etc.)
Radiographic appearances
Similar to pleural effusion
Step in the right pleural line
Outside of the line is all white
This means there is a rupture of the pleura where the blood is getting into the lungs
Pleural effusion
Fluid collection in the space between the parietal and visceral pleural layers
Often results in pulmonary oedema, often of cardiogenic or non cardiogenic, often bilateral
Cardiogenic pulmonary oedema - result of L HF or mitral valve disease
Non-cariogenic - renal failure, infection (pneumonia, TB), surgery, malignancies, RA, liver failure, and malnutrition
What type of fluid can accumulate in pleural space?
Transudate
Exudate
Pus
Blood
Chyle
Cholesterol
Urine
Transudate fluid in lungs
due to hydrostatic pressure changes in CHF, cirrhosis and hypoalbuminemia
Exudate fluid in lungs
due to inflammation of pleura such as malignancy, rheumatoid arthritis etc.
Pus in the lungs
emphysema from infection
Blood in lungs
trauma
Chyle in the lungs
from rupture of thoracic duct
Urine in lungs
urinothorax in hydronephrosis
Radiographic appearances of pleural effusion
Erect position = pleura fluid gravitates to the lowest part of the thorax
Homogenous opacification, generally same density as cardiac shadow
Loss of outline of diaphragm
No visual pulmonary or bronchiole marking
Concave upper border with highest level in axilla
Initially fluid accumulates in posterior of lung then lateral costophrenic space
As fluid collection grows in size, underlying lung decreases in size and retracts towards the hilum
With larger effusion, there is a mediastinal shift to the other side
Rib fractures with too high costophrenic angle - pooling fluid
Pneumothorax
Both of these result in hemopneumothorax
Thoracic cage injuries
Rib fractures
Flail chest
Sternal fractures
Rib fractures
Common
Limited clinical significance
Oblique rib projections
Medicolegal refferals
CXR to include
Pneumothorax
Haemothorax
Pneumohemothorax
Increasing number of broken ribs leads to increased trauma = increased incidence of intrathoracic trauma
Considerable force required to break ribs 1 2 and 3 - rare
Mainly in the middle that rib fractures do
Ribs 10, 11, 12 indicate possible liver, spleen, and kidney injury
Non-addental injury - in paediatrics
Flail chest
Traumatic costochondral segment separated from chest wall
Fracture of two or more contiguous ribs in two or more places
Classic paradoxical movement in relation to the rest of the chest wall
High association with other injuries
Radiographic findings of flail chest
Multiple rib fractures
Costochondral separation may be demonstrated
Pulmonary contusion/laceration
Sternal fractures
Typically result of car accident
Frequency increases with age
Not demonstrated on PA or AP CXR
Difficult to identify on a lateral CXR
Require dedicated projections
Simple sternal fracture is typically benign - wont cause intrathoracic trauma
Indicates significance of chest trauma
Associated with sudden deceleration of forces: aortic or great vessel injury
chronic chest pathologies
Consolidation
Pneumonia
Pulmonary oedema
Bronchiectasis
Atelectasis
Chronic obstructive pulmonary disease
Subcutaneous emphysema
Carcinoma/pulmonary metastasis
Consolidation
Refers to the alveoli/bronchioles being filled with fluid or some other material (eg. Inflammatory cells, tissues)
consolidation causes
infection = pneumonia
Fluid = pulmonary oedema
consoliation symptoms
SOB
Cough
Fever
Fatigue
Chest pain
consolidation on radiograph
Opacification
Loss of cardiac silhouette

consolidation
Pneumonia
Infection within the lung causing an inflammatory response of the alveolar tissue
Etiological
Viral, fungal, or aspiration
Acquisition
Hospital or community-acquired
Spread of infection
Bronchopneumonia, lobar pneumoni
pneumonia radiographically
Opacification
Patchy (isolated nodules) or confluent (merged)

pneumonia
Pulmonary oedema
Abnormal accumulation of fluid in the lungs
Cardiogenic (ie. CCF) and non cardiogenic - caused from the heart or not caused from the heart