PD - Older adult & Disabled patient
1/99
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
100 Terms
"Demographic imperative"
for societies worldwide to maximize not only life span but also "health span", so that older adults maintain full function as long as possible
Elements of ideal geriatric primary care include:
- Assessment of functional status
- Frequent medication review
- Careful evaluation of benefits
- Benefits and burdens of any new test or treatment
- Frequent assessment of goals of care and prognosis
The most important geriatric syndromes in primary care:
- Falls
- Urinary incontinence
- Frailty
- Cognitive impairment
Primary aging
changes in physiologic reserves overtime that are independent of changes from disease
can lead to the development of multiple impairments such as decline in overall functional capacity, morbidity, and mortality
Alterations in primary aging tends to have the most impact during periods of stress:
Exposure to fluctuating temperatures - decreased vasoconstriction and sweat production (impaired response to heat)
Dehydration - decline in thirst (delayed recovery)
Shock - drop in maximum cardiac output, left ventricular filling and maximum heart rate
Blood Pressure Changes
- Systolic BP tends to rise
- Aorta and large arteries become less distensible (atherosclerosis) leading to a greater rise of systolic
- Diastolic tends to stop rising around the ages of 50-59
- Develop orthostatic hypotension
Heart rate/rhythm changes
resting heart rate unchanged, more likely to have abnormal heart rhythms
remain unchanged
as you age, respiratory rate and temperature usually ______
Skin, Nails and Hair changes
- Skin loses turgor/elasticity
- Dermis is less vascular (thin, fragile)
- Actinic purpura
- Nails may yellow and thicken
- Scalp hair looses pigment (gray)
- Hair loss, the number and diameter decreases
- Hair loss on body (trunk, pubic area)
Eyes and visual acuity changes
- Fat surrounding eyes may atrophy
- Pupils become smaller
- Fewer lacrimal secretions (dry eyes)
- Presbyopia
- Visual acuity diminishes rapidly after 70 yrs of age
- Increased risk for cataracts, glaucoma and macular degeneration
Presbyopia
age related farsightedness
Hearing changes
- Hearing acuity declines with age
- Early loss of high-pitched sounds
- Gradual loss of middle and lower range sounds
- Presbycusis (more evident after the age of 50)
Mouth, Teeth, and Lymph node changes
- Decreased salivary secretions and loss of taste
- Teeth may wear down or fall out due to periodontal disease
- Without teeth, lower portion of face looks small and sunken, with accentuated "purse-string" wrinkles radiating from mouth
- Angular cheilitis
- Cervical lymph nodes become less palpable but, submandibular glands become easier to feel

Angular cheilitis
maceration of the skin at the corners of the mouth

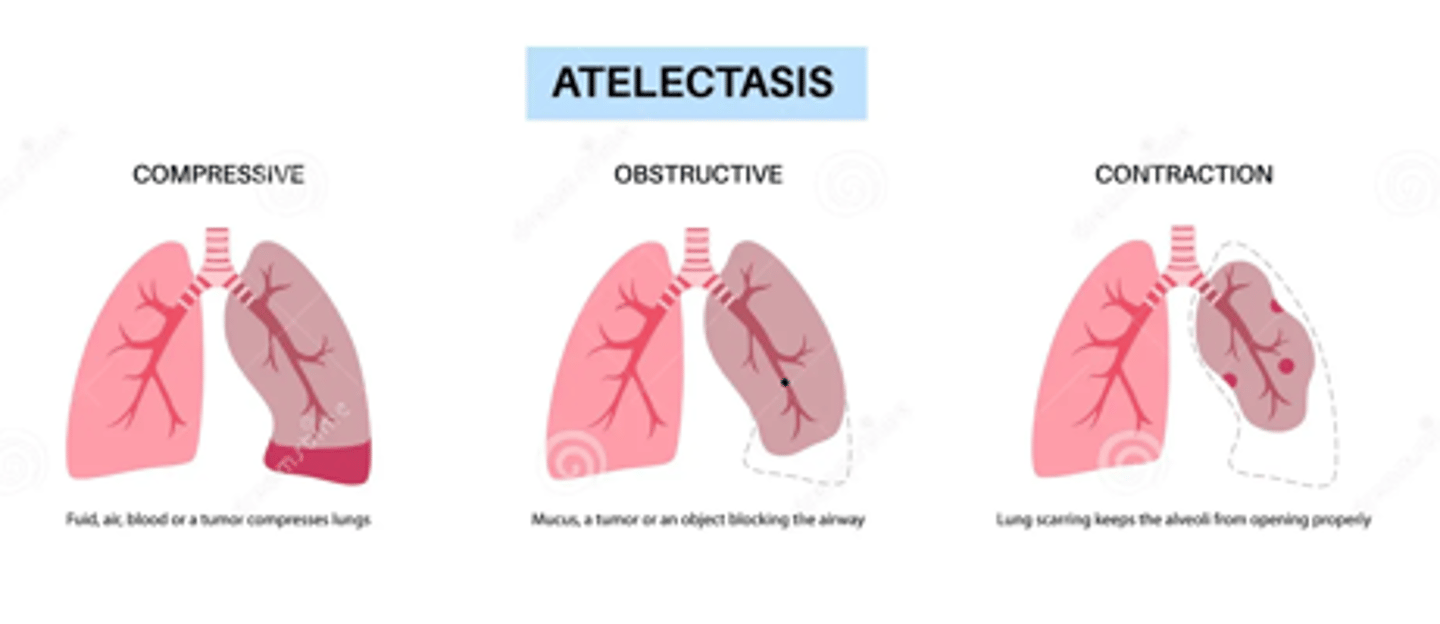
Thorax and Lung changes
- Loss of lung capacity
- Altered gas exchange
- Increase in closing volumes of small airways, predisposed to atelectasis and risk of pneumonia
- Diaphragmatic strength declines
- Mild decrease in arterial pO2 but O2 saturation normally remains above 90%
- Skeletal change, accentuate dorsal curve of the thoracic spine (kyphosis)
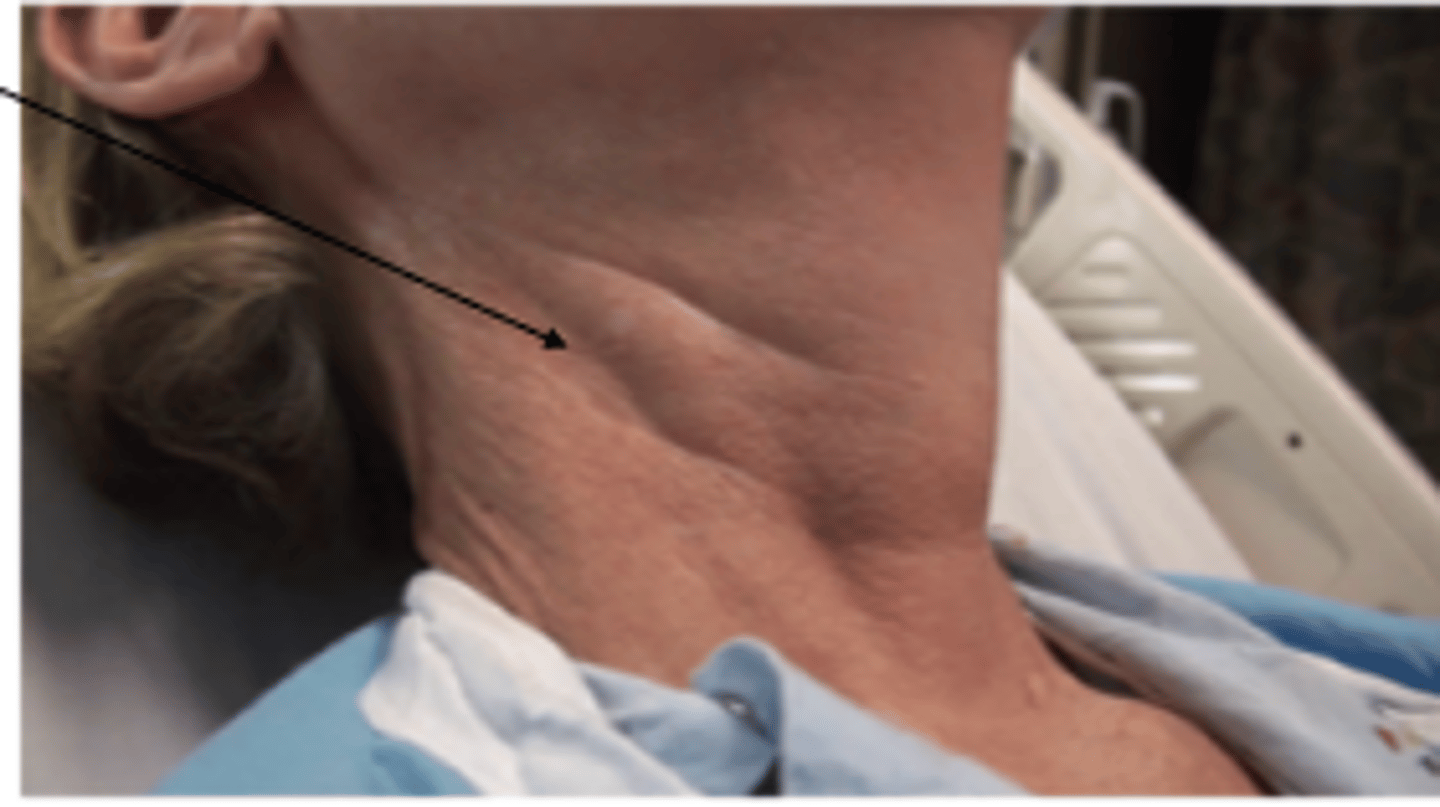
Neck changes
pulsatile mass due to kinking or buckling of the carotid artery low in the neck, caution not to mistake for carotid aneurysm which is true dilation of the artery!
systolic bruits heard in carotid artery/arteries indicate stenosis from atherosclerotic plaque (vs usually innocent in younger patients)
Cardiac output changes:
- modest drop in resting heart rate, but cardiac output in maintained due to increase in stroke volume
- significant drop in maximum heart rate during exercise
- increased myocardial stiffness and hypertrophy more notably in the left ventricle
- decreased early diastolic filling → diastolic dysfunction → greater dependence on atrial contraction
decreased ventricular filling
risk of heart failure increases with loss of atrial contraction and onset of atrial fibrillation due to ____________
Is S3 a normal heart sound to hear in the elderly? what about S4?
No, auscultating S3 strongly suggests heart failure from volume overload of the LV or valvular heart disease in the older adult
S4 in rarely normal, may suggest decreased ventricular compliance and impaired ventricular filling
Cardiac murmurs heard in the elderly:
Aortic Stenosis - fibrotic changes thicken the bases of the aortic cusps, calcifications follow and result in audible vibrations
Mitral Regurgitation - calcifications of mitral valve annulus
Peripheral Vascular System changes
peripheral arteries tend to lengthen, become tortuous, firmer, and less resilient
increased arterial stiffness, decreased endothelial function
Females - Breast and Axillae changes
Glandular tissues of breast atrophy, breasts are smaller more flaccid, more pendulous
Axillary hair diminishes
gynecomastia
elderly males may develop _______ due to obesity or hormonal changes
Abdomen changes
- muscles weaken
- decreased activity of lipoprotein lipase
- fat accumulation in lower abdomen and near the hips
- manifestation of acute abdomen may be blunted due to less severe complaint of pain (diminished or absent guarding and rebound tenderness - peritoneal inflammation)
Female genitourinary system changes
- estrogen falls, resulting in symptoms such as hot flashes, palpitations, chills, anxiety, sleep disruption, and mood changes
- ovarian function usually declines during fifth decade
- vagina narrows and shortens, mucosa becomes thin, pale and dry
- within 10 years after menopause, ovaries no longer palpable
Male genitourinary system changes
- penis decreases in size and testicles drop in the scrotum
- sexual interest remains intact, but intercourse frequently declines after age 75
Urinary incontinence
decreased innervation and contractility of the detrusor muscle and loss of bladder capacity, urinary flow rate, and ability to inhibit voiding
Benign Prostatic Hyperplasia (BPH)
benign growth of cells within the prostate gland, patient will report symptoms such as urinary hesitancy, dribbling and incomplete emptying
Musculoskeletal system changes
loss of bone mass, increased risk for fracture
- especially in women after menopause
- bone density scan (DEXA) to diagnose osteoporosis
Sarcopenia
loss of lean body mass and strength with aging
Mental Status Changes
- retrieve and process data more slowly, ability to perform complex tasks may diminish
- early Alzheimer disease vs. "benign senescent forgetfulness"
- more susceptible to delirium
what could be contributing to changes in mood of elderly patients?
death of friends, retirement, decreased income, social isolation
Motor system changes
- move and react slower, skeletal muscles decrease in bulk
- signs of muscle atrophy (hands, arms, legs)
- essential tremors (benign, faster, stop at rest, no muscle rigidity)
Position and Vibratory Sense/Reflexes:
- lose some or all vibratory sense in feet and ankles
- decreased reflexes → gag, knee, ankle etc.
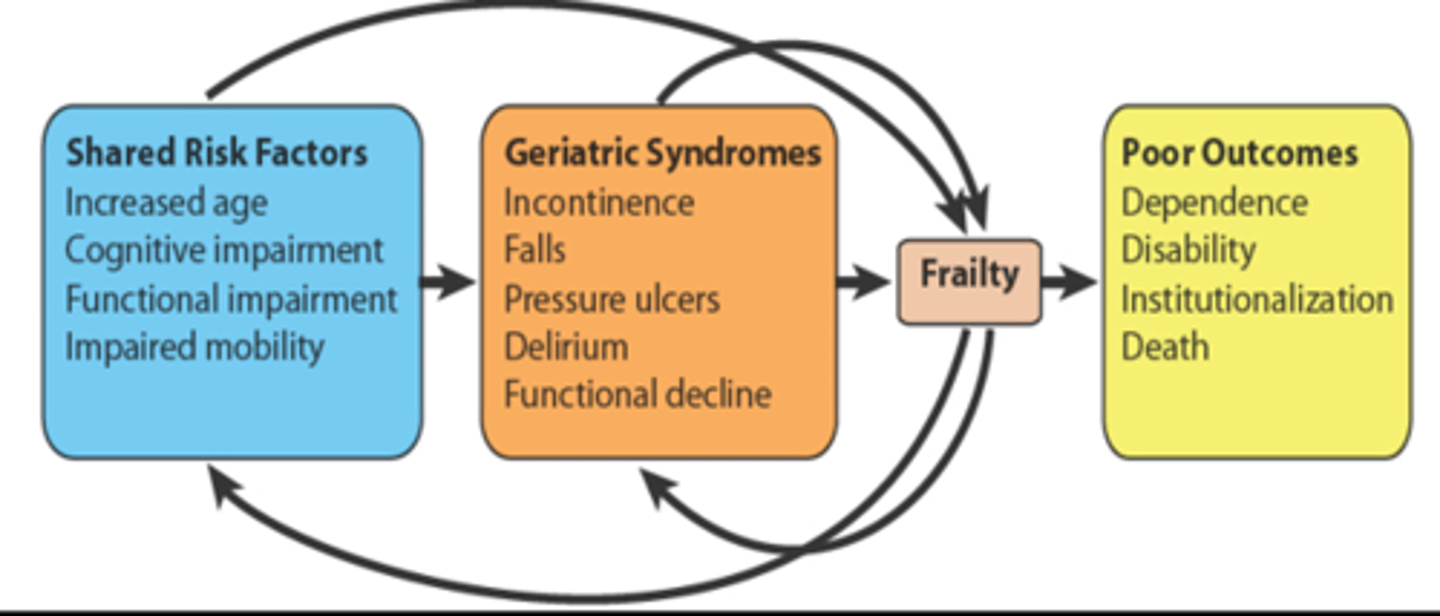
Recognizing geriatric syndrome:
multifactorial condition of identifiable situation - specific stressors & underlying age-related risk factors:
- incontinence
- falls
- pressure ulcers
- delirium
- functional decline
Interaction between geriatric syndromes & age-related risk factors can result in poor outcomes
Importance of addressing cultural dimensions of aging
culture shapes beliefs about aging, medications, health care proxies, end of life decisions
alcohol recommendation
recommend limit of 2 drinks in one day or 7 drinks in a week
clues of alcohol consumption: memory loss, depression, neglect of hygiene/appearance etc.
true, only 30-40% of elderly meet recommended guidelines for daily intake of fruit and vegetables
t/f prevalence of under nutrition increases with age
ADLs (activities of daily living): 6 basic self-care abilities
Bathing
Dressing
Toileting
Transferring
Continence
Feeding
IADLs (instrumental activities of daily living): higher level functions
Using the telephone
Shopping
Preparing food
Housekeeping
Laundry
Transportation
Taking medicine
Managing money
Level of Assistance
- Independent
- Needs some assistance
- Total assistance (dependence)
what is polypharmacy and why should it be avoided?
suboptimal prescribing, concurrent use of multiple drugs, inappropriate use and nonadherence
major cause of morbidity!! try to keep the number of drugs to a minimum
Medication Management
- perform a thorough medication history (name, dose, frequency & patient's explanation of reason for taking each drug)
- review all bottles, including OTC and herbal supplements
- new medication dosing: "start low and go slow"
- assess medication for drug interactions
- avoid polypharmacy
true
t/f medications are the single most common modifiable risk factor associated with falls
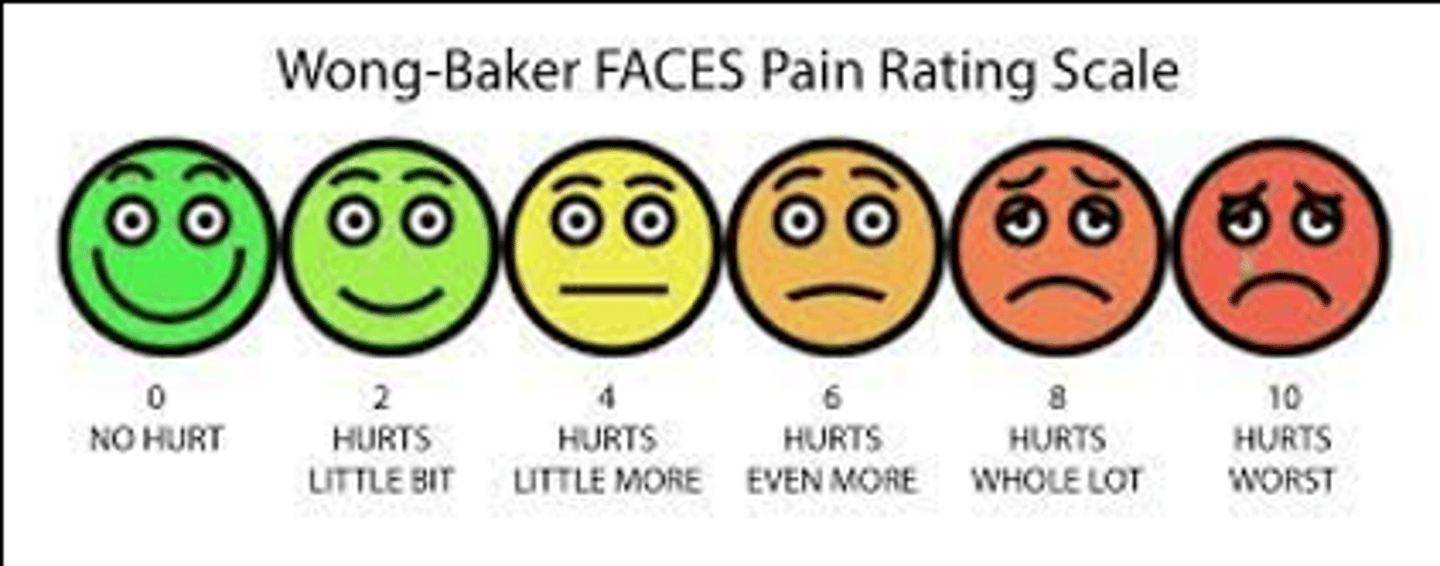
Assessment of Pain - Acute & persistent pain
- Address each visit
- Onset (distinct vs > 3 months)
- Pathology
- Duration
- Causes
- Analgesic history (effectiveness, satisfaction)
- Quantitative assessment: Standard pain scale (FACES pain scale)
Advance care planning
providing information, clarifying the patient's preferences and identifying the surrogate decision makers
Advance directives
includes DNR, DNI, do not hospitalize, do not provide artificial hydration or nutrition, do not administer antibiotics
Health care proxy, durable power of attorney (DPOA)
person who makes decisions reflecting patient's wishes
Palliative care
alleviation of pain and suffering and the promotion of optimal quality of life across all phases of treatment, including curative interventions and rehabilitation (advanced or terminal illnesses)
Assessing Functional Status
- ability to perform tasks and fulfill social roles associated w/ daily living
- baseline for making interventions and identifying geriatric syndrome
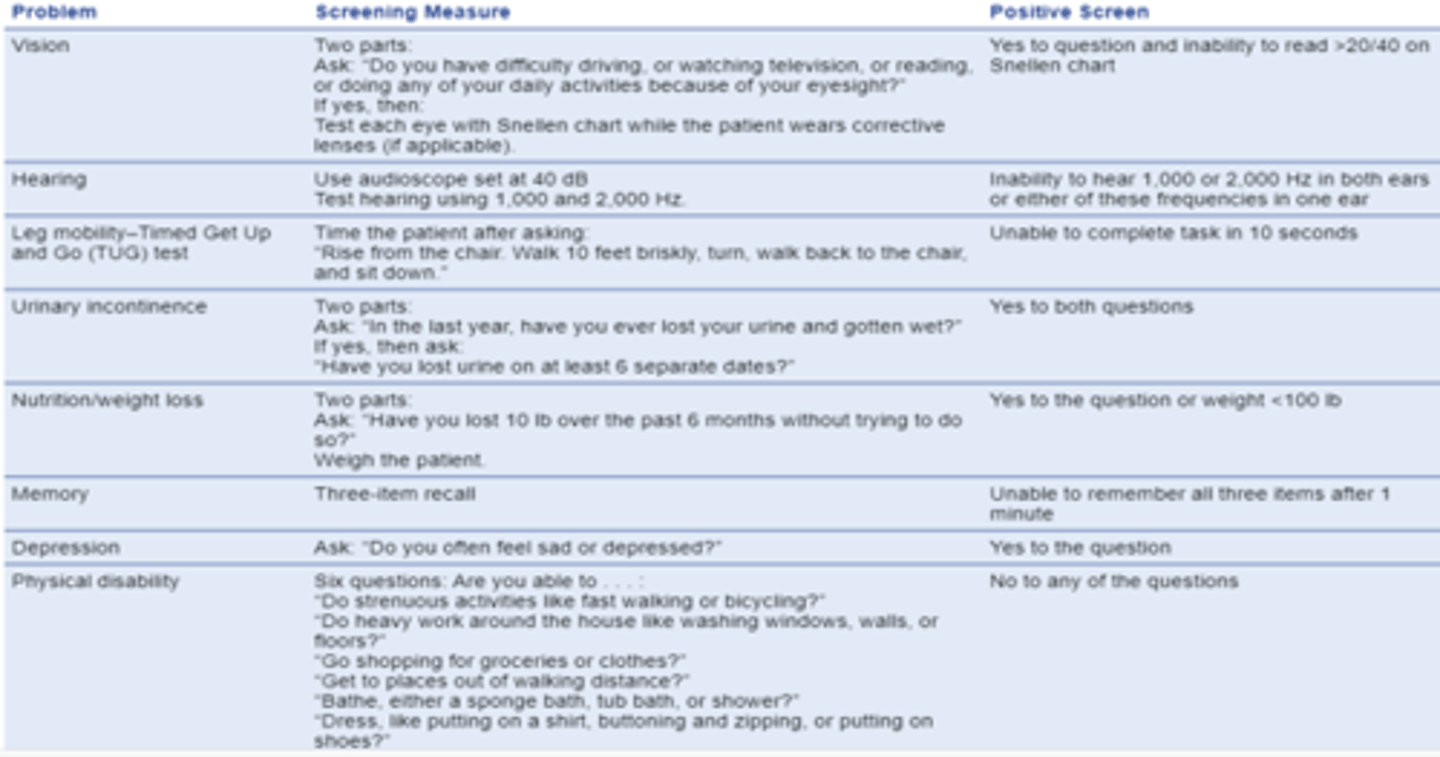
- 10 minute Geriatric Screener
10 minute geriatric screener
includes vision, hearing, incontinence, nutrition, memory, depression, leg mobility (timed get up & go test), and physical disability.
target blood pressure
recommendation for >60 yrs: <150/90 (80 years and older 140-150/70-80)
orthostatic hypotension
defined as the drop in systolic of >20 mmHg or diastolic of >10 mmHg within 3 minutes of standing
true
t/f apical heart rate allows for better detection of arrhythmias compared to radial pulse
Overall Physical Exam of the Older Adult:
- Assessing Functional Status (10 min geriatric screener)
- Vital Signs (BP, HR, RR, Temp, Height, Weight, BMI)
- General Survey
- Skin
- Snellen chart (visual acuity), eyelids, bony orbit, pupillary constriction, ophthalmic exam
- Ears (whisper or audio scope)
- Mouth/teeth
- Neck (thyroid & lymph exam)
- Thorax/Lungs
- Cardiovascular system
- Peripheral Vascular System
- Abdomen
- Breasts and Axillae
- GU
- MSK
- Nervous System
General Survey
observing gait, posture changes (kyphosis), involuntary movements, nutrition, flat effect (depression, Parkinson disease, Alzheimer disease), and hygiene
Skin Exam
- Physiologic changes (thinning, loss of turgor, dry, flaky, rough)
- Interosseous atrophy (space between metacarpals)
- Actinic purpura
- Pressure ulcers in bed bound patients
- Hair and scalp
- Nails

Actinic Keratoses
sun damage, pre cancerous, superficial flattened patches covered by a dry scale (crusty) often found on hands, ears, lips, neck and shoulders

Seborrheic keratoses
barnacles of old age, benign raised yellowish lesions that feel greasy and velvety, or warty, often found on head, back, or neck

Senile ptosis
both eyelids drooping due to old age, caused by weakening, relaxation, increased weight
Entropion
lower lid eyelashes directed toward the eye
Extropian
sagging and outward turning of lower eyelid and eyelashes
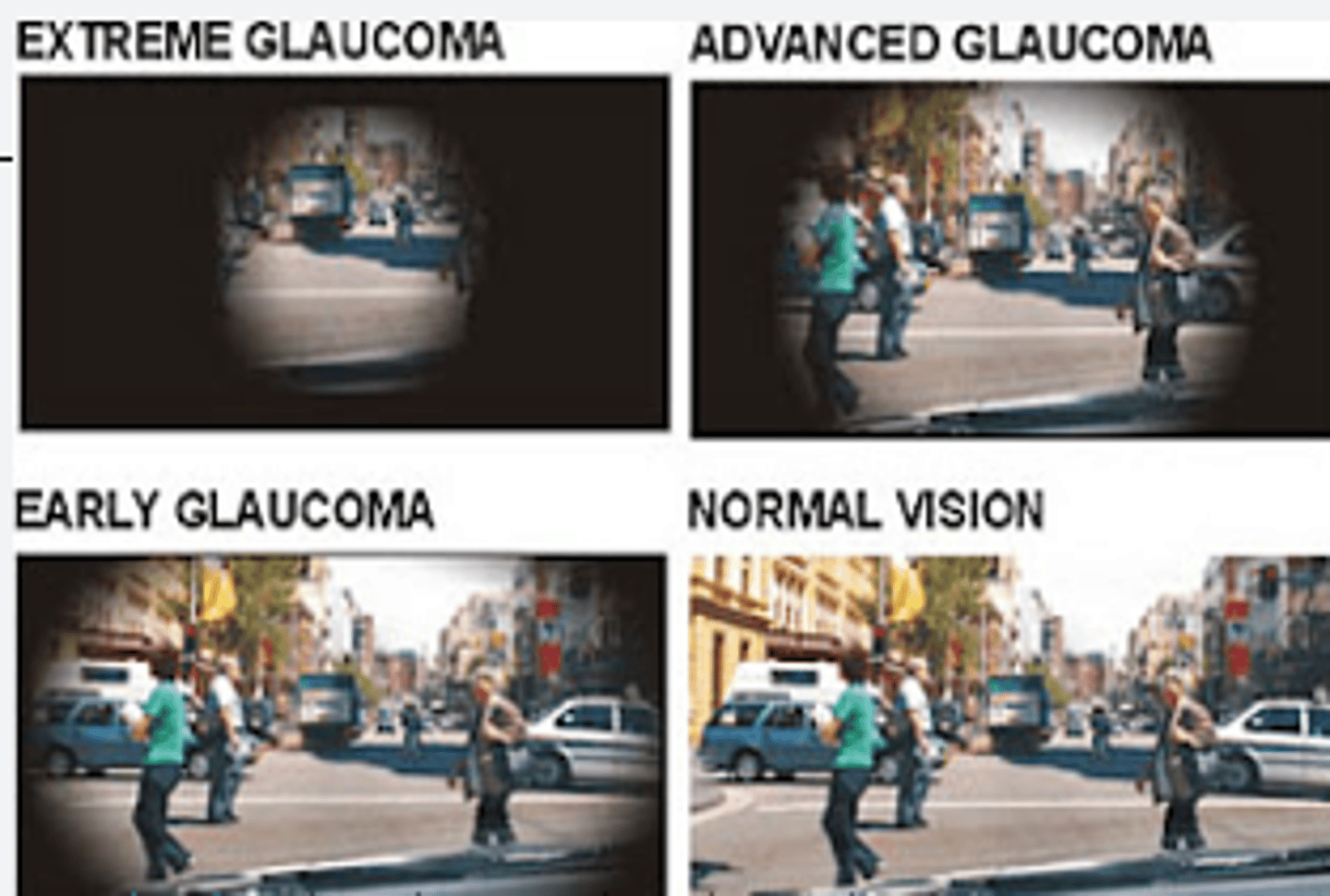
Glaucoma
increased intraocular pressure, loss of peripheral vision, disc cupping
Cataracts
opacity of eye lens
Macular degeneration
atrophy of cells in central macular region of retina
Ear exam
whisper test or audio scope, inspect canals for cerumen
Mouth/Teeth exam
examine oral cavity for odor, appearance of gingival mucosa, carries, adequacy of saliva, inspect for lesion. remove dentures!
Neck exam
thyroid and lymph node exam
Thorax/Lung exam
observe for subtle signs of change in pulmonary function
increased AP diameter, purse-lipped breathing, dyspnea w/ talking = COPD
Cardiovascular Exam
- JVP inspection and palpate carotid upstrokes, auscultate for bruits
- PMI, S1, S2, S3, S4
- Cardiac murmurs
Mitral regurgitation
most common murmur in older adults, harsh holosystolic murmur at the apex, radiating to the axilla
Peripheral Vascular System Exam
diminished or absent pulses seen in PAD - confirm diagnosis with Ankle-Brachial Index (ABI)
Abdomen Exam
assess for bruits (aortic, renal, iliac, femoral), masses, aortic pulsations, width of the aorta
Ascites
abdominal accumulation of fluid in peritoneal cavity (liver disease, cancer)
Atherosclerosis
plaque, cholesterol buildup to inner lining of artery (thickening/hardening)
Abdominal Aortic Aneurysm
swelling/enlargement of aorta
Breast and Axillae Exam
- Inspect nipples
- Atrophy, glandular tissues replace with fat, flaccid, pendulous breasts
- Males may develop gynecomastia
- Palpate for lumps or masses in older adults
- Ducts more easily palpable
- Mammogram?
Mammogram Recommendation
USPSTF recommends every 2 years for women 50-74 years old
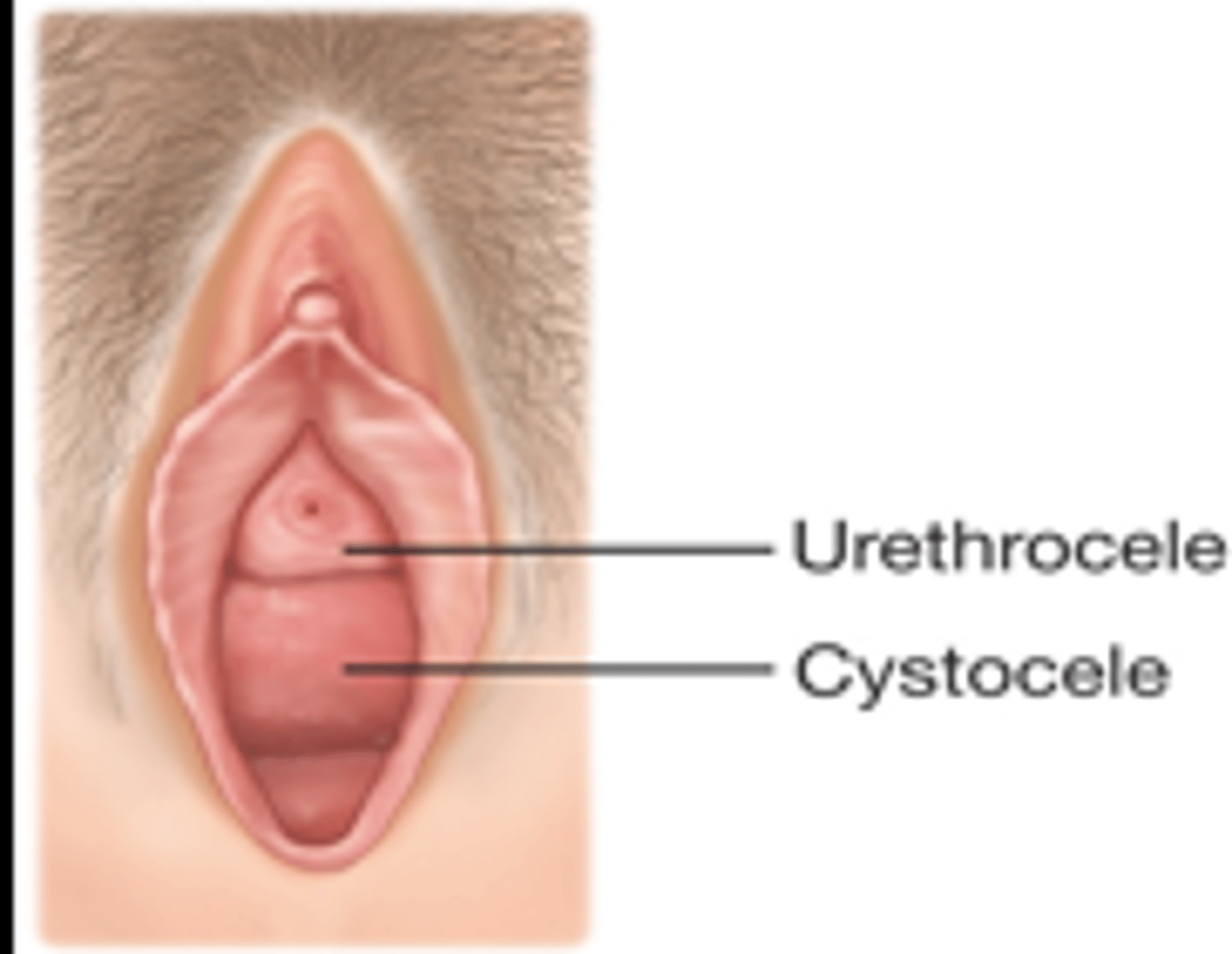
Female genitalia exam
raise head of table, caution with arthritis/spinal deformities while placing in lithotomy position
inspect for labial masses/ulcers, vulvar atrophy/erythema, prolapse (urethrocele, cystocele), rectovaginal exam
Male genitalia exam
inspect penis, scrotum, testes, epididymis, implant, rectal tone, rectal masses, enlarged prostate
Leg mobility - "Time to Get up and Go" or TUG Test
tests for gait and balance, and risk for falling
asking patient to get up from a chair, walk 10 feet, turn and walk back to the chair and sit back down
Nervous System Exam
- 10 minute geriatric screener assess memory and affect
- Gait, balance and stride characteristics
- Examine for TRAP
TRAP
Tremor
Rigidity
Akinesia
Postural instability
(commonly seen in Parkinson disease)
Causes of transient incontinence - DIAPPERS
Delirium
Infection (UTI)
Atrophic urethritis or vaginitis
Pharmaceuticals (diuretics, anticholinergics, CCB, opioids, sedatives, alcohol)
Psychological disorders (depression)
Excessive urine output (heart failure, uncontrolled DM)
Restricted mobility (hip fracture environmental barriers, restraints)
Stool impaction
Benefits of Exercise in Older Patients
- Decrease all-cause mortality (HTN, DM, colorectal/breast cancer, cardiac events)
- Improve cognitive function
- Improve physical function (gait speed, balance, performance of ADLs)
- Fall prevention
Exercise recommendation
150 minutes of moderate-intensity aerobic activity every week + muscle strengthening activities 2+ days a week = promotes healthy aging
Immunization recommendations
COVID - one or more doses of updated
Influenza inactivated or influenza recombinant - one dose annually
Tetanus, diphtheria, pertussis - 1 dose Tdap, then Td or Tdap booster every 10 years
Zoster recombinant (RZV) - 2 doses
Lung Cancer Screening
50-80 years old need screening IF 20 pack yr hx or current smoker or quit within the last 15 years
Low dose CT of lungs
Detecting the 3 D's
delirium, dementia, depression
Delirium
an acute brain dysfunction or confused state characterized by sudden onset, fluctuating course, inattention and at times alteration of consciousness, it can be reversed
screen at risk patients using confusion assessment method (CAM)
Dementia
an acquired condition characterized by a decline in memory & cognitive ability that interfere with activities of daily living
most common types: Alzheimer disease, Lewy body dementia, frontotemporal dementia, vascular dementia
Depression
mental disorder that presents with depressed mood, loss of interest of pleasure, feeling of guilt or low self-worth, disturbed sleep or appetite, low energy and poor concentration
screening: patient health questionnaire (PHQ) and geriatric depression scale
Elder Mistreatment & Abuse
-abuse, neglect, exploitation, abandonment
- increased prevalence among older adults w/ depression & dementia
- highly undetected
- no valid, reliable screening tools
- careful history & high index of suspicion are important!
Approach to a Disable Patient:
- affirm impression of history with attention to the patient's ability to follow commands and perform functional tasks
- "improvise" examination techniques, as many patients are severely limited by their underlying disability
- allow for additional time and utilize appropriate instruments
Examples of Disabilities:
Mobility impairments - can affect ability to move or control limbs
Sensory impairments - can affect ability to hear or see
Cognitive impairments - can affect ability to think, reason or process information
Communication impairments - can affect ability to communicate effectively
Clinical pearls to keep in mind when examining patients with disabilities:
Communication
Positioning
Sensory consideration
Flexibility
Transfer methods
- Cradle
- Stand and Pivot
- Two-person (pivot, side-to-side, dependent)
- Patient lifts (Hoyer, Sara)
- Slide Board transfer

Transfer guidelines - Lifter
- Allow the patient to direct transfer
- Do not overestimate ability to lift
- Not all non-ambulatory people need assistance
- Keep back straight, bend at knees and lift with legs
- Be aware of jewelry, clothing, tubing or equipment which might catch
Exam of the hospitalized patient
- Adjust approach to the examination
- Identify areas that should be assessed at the beginning (review chart, what are they here for?)
- Principles for condensing or expanding parts of physical exam depend on the patient condition/alertness/cooperation
Perform an evaluation of the lower extremity on all hospitalized patients!