Di Imaging I - Exam 2 (PEAR + RA)
1/111
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
112 Terms
Seropositive vs Seronegative arthropathies refer to the presence/absence of
rheumatoid factor (RF)
What is always a differential dx
infection
When the cause of an enthesophyte is degenerative it is known as
osteophyte
When the cause of an enthresophyte is inflammation it is known as
syndesmophyte
Seronegatives (for RF) (PEAR)
psoriatic arthritis
enteropathic arthritis
ankylosing spondylitis
reactive arthritis
The vowels in PEAR are ______ of each other and the consonants in PEAR are ______ of each other
radiographic mimics
AE (vowels) vs PR (consonants) in PEAR locations
AE = axial skeleton
PR = appendicular/peripheral skeleton
PEAR have a positive finding in blood (sero) tests, what is it
HLA-B27
HLA-B27 and seropositive/negative are just tests for
possibility
What is the most common seronegative spondyloarthropathy
ankylosing spondylitis (fusion)
Ankylosing spondylitis (Marie-Strumpell/Bechterew disease) MC occurs in what population
young males (15-35 yo)
(over call males, under call females)
Ankylosing spondylitis characteristics
synovial proliferation → pannus
erosions, bony proliferation/sclerosis, fusion
bilateral and symmetrical
Where is MC the first site of AS
sacroiliac joints (sacroilitis)
AS also likes the ____ joints causing limited chest expansion
costovertebral joints
Serological studies for AS
+HLA-B27 (in 90% of pts)
+ESR
-RF
-ANA
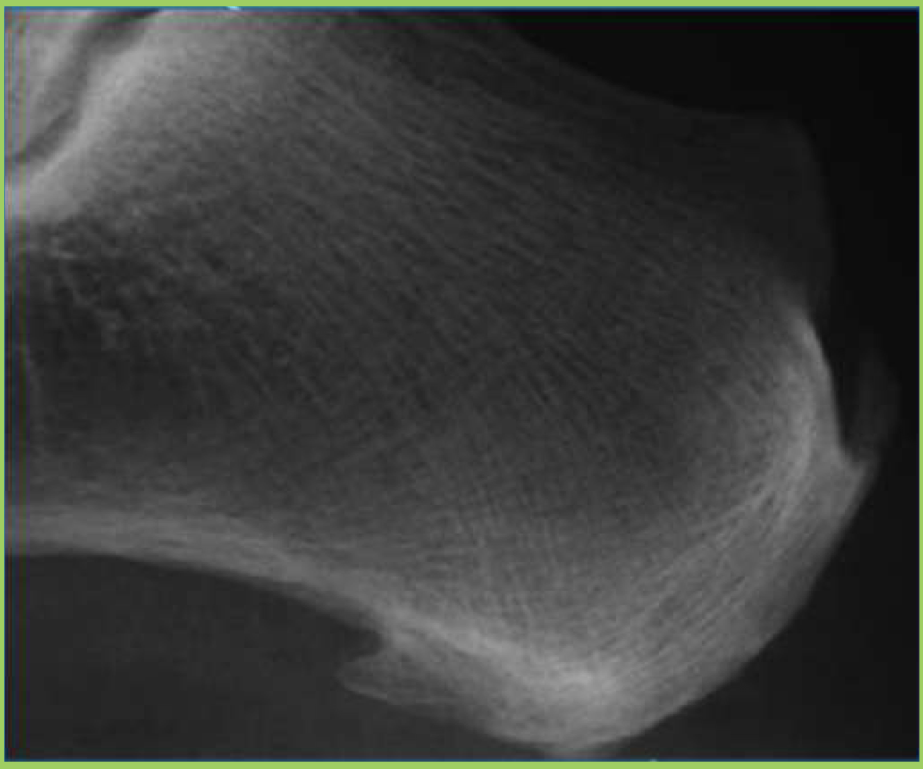
What two things are found on this image
achilles tendon enthesophyte
plantaraponerosis enthesophyte
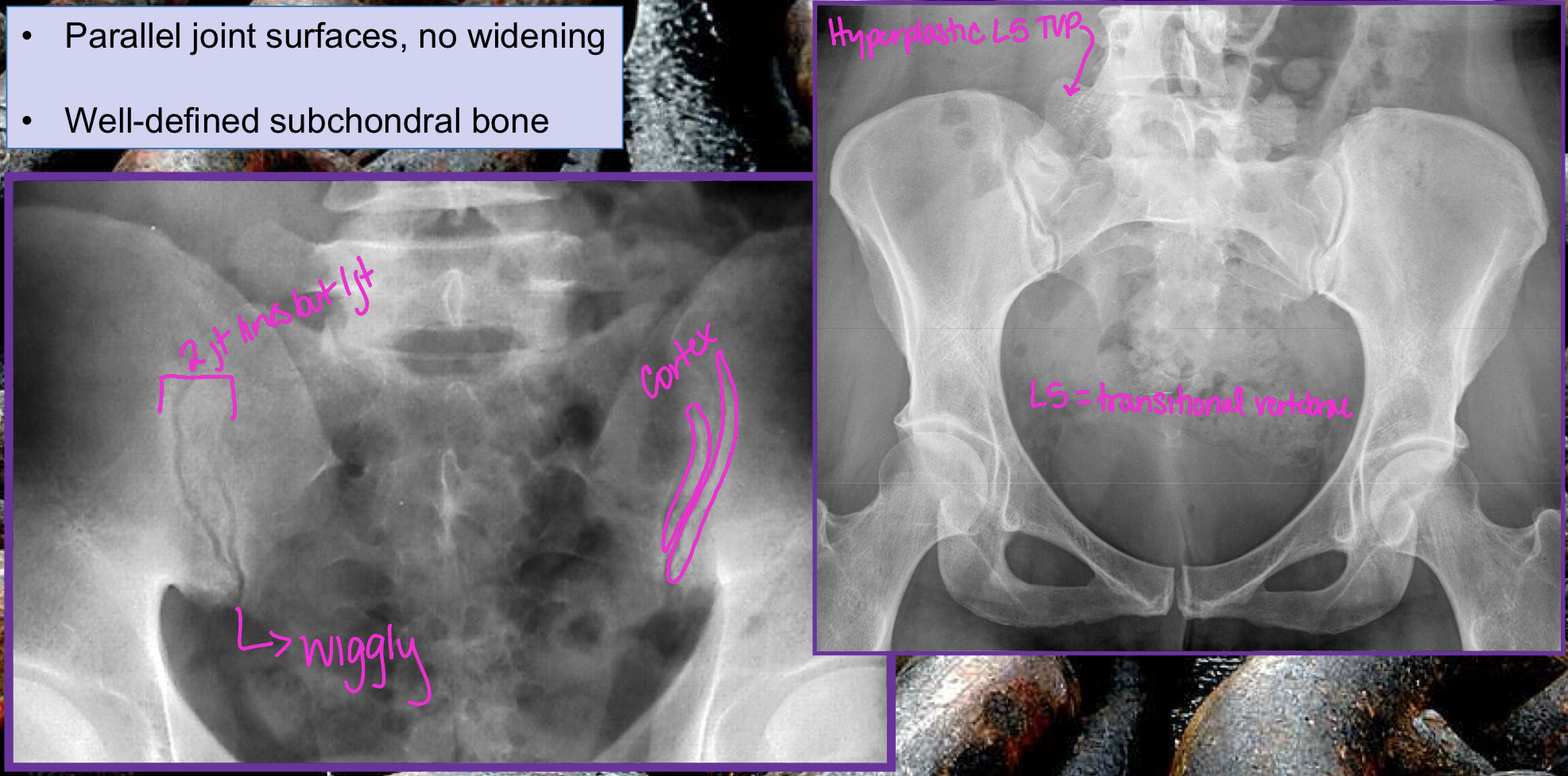
Normal SI joints
Why is MRI not great for looking at cortical bone
it holds onto its protons
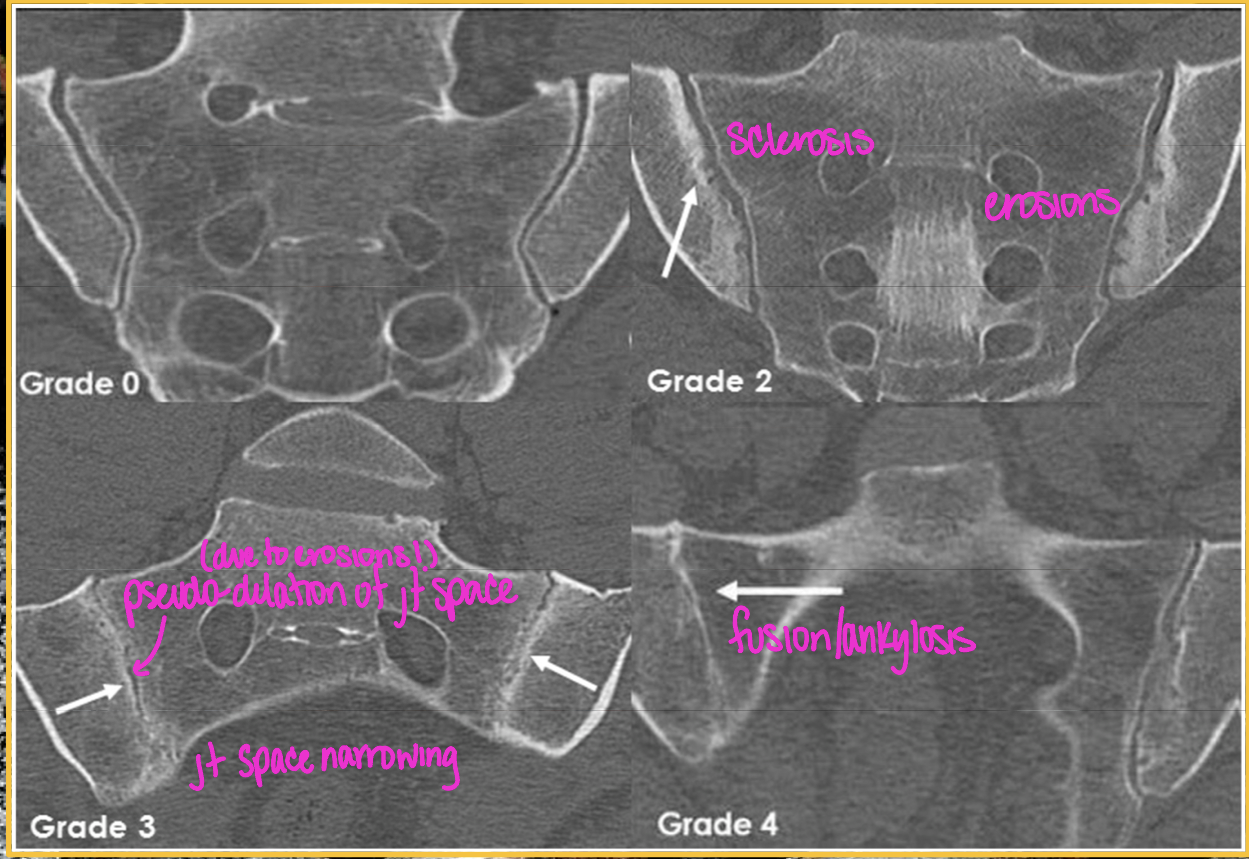
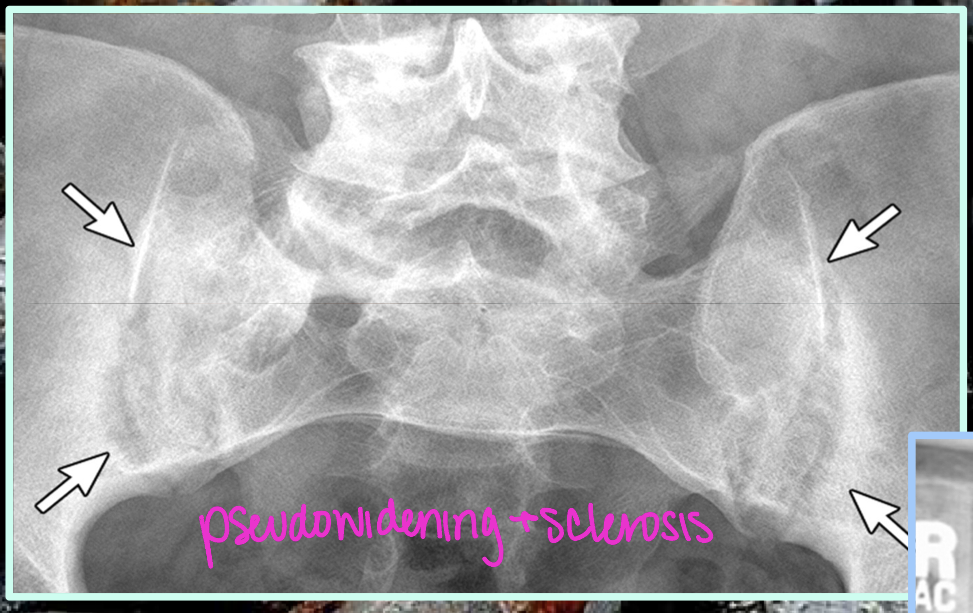
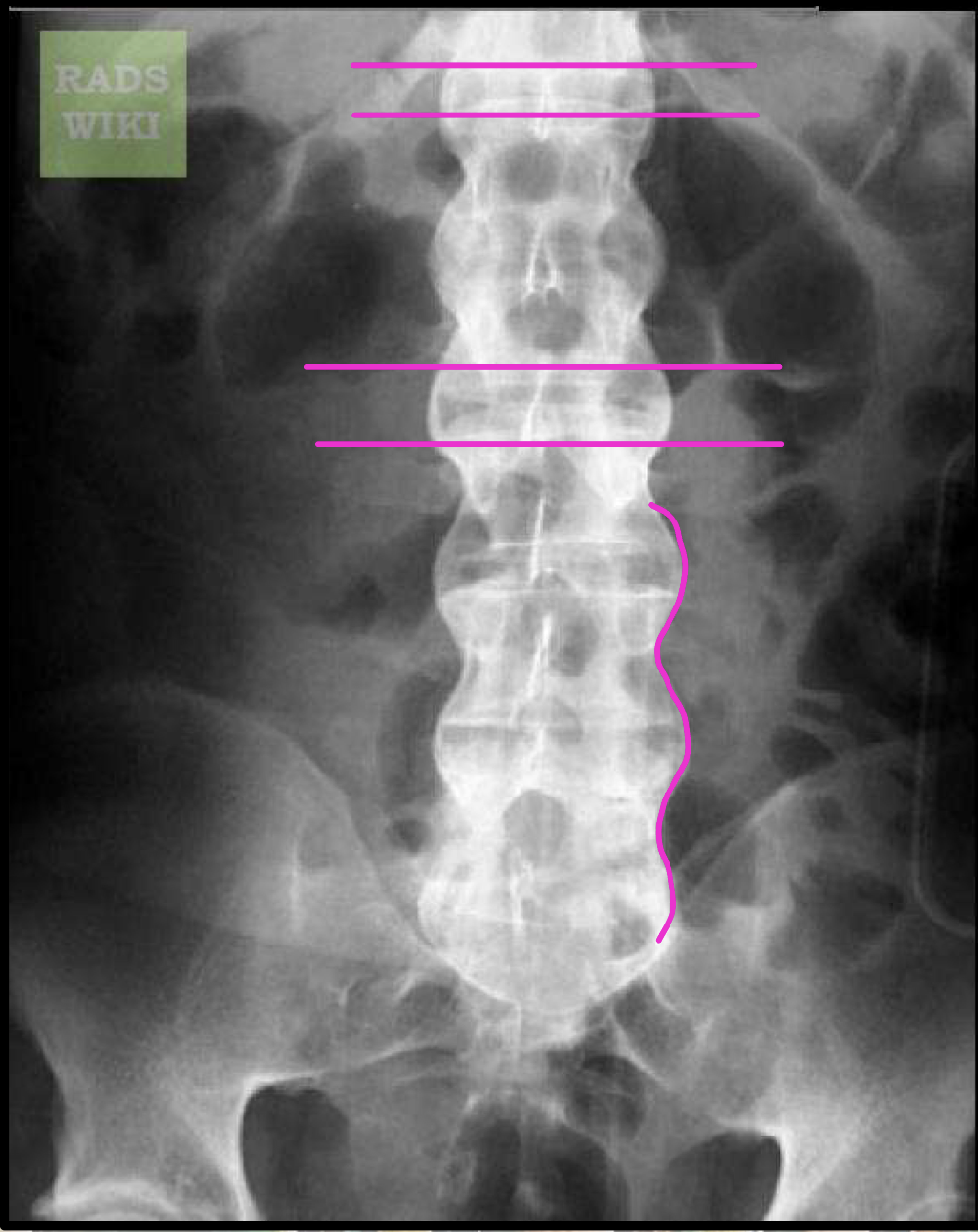
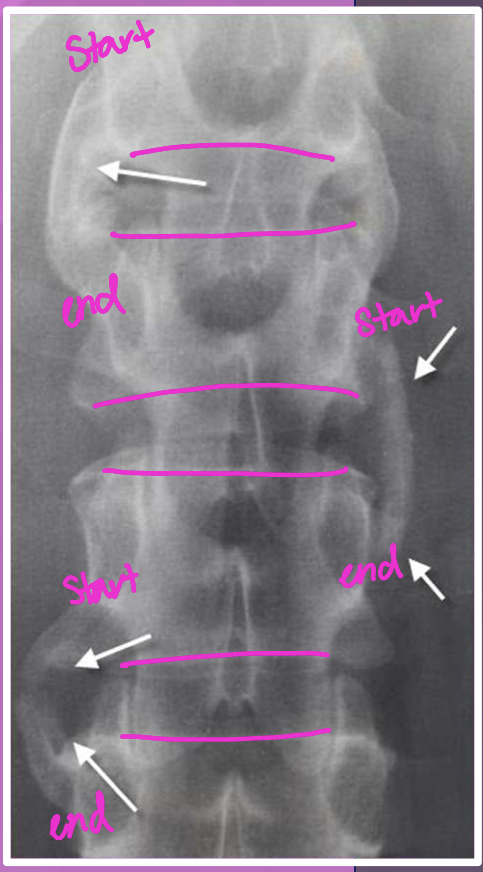
AS Sacroilitis grading
0 - normal SI joint width + sharp joint margins
1 - suspicious
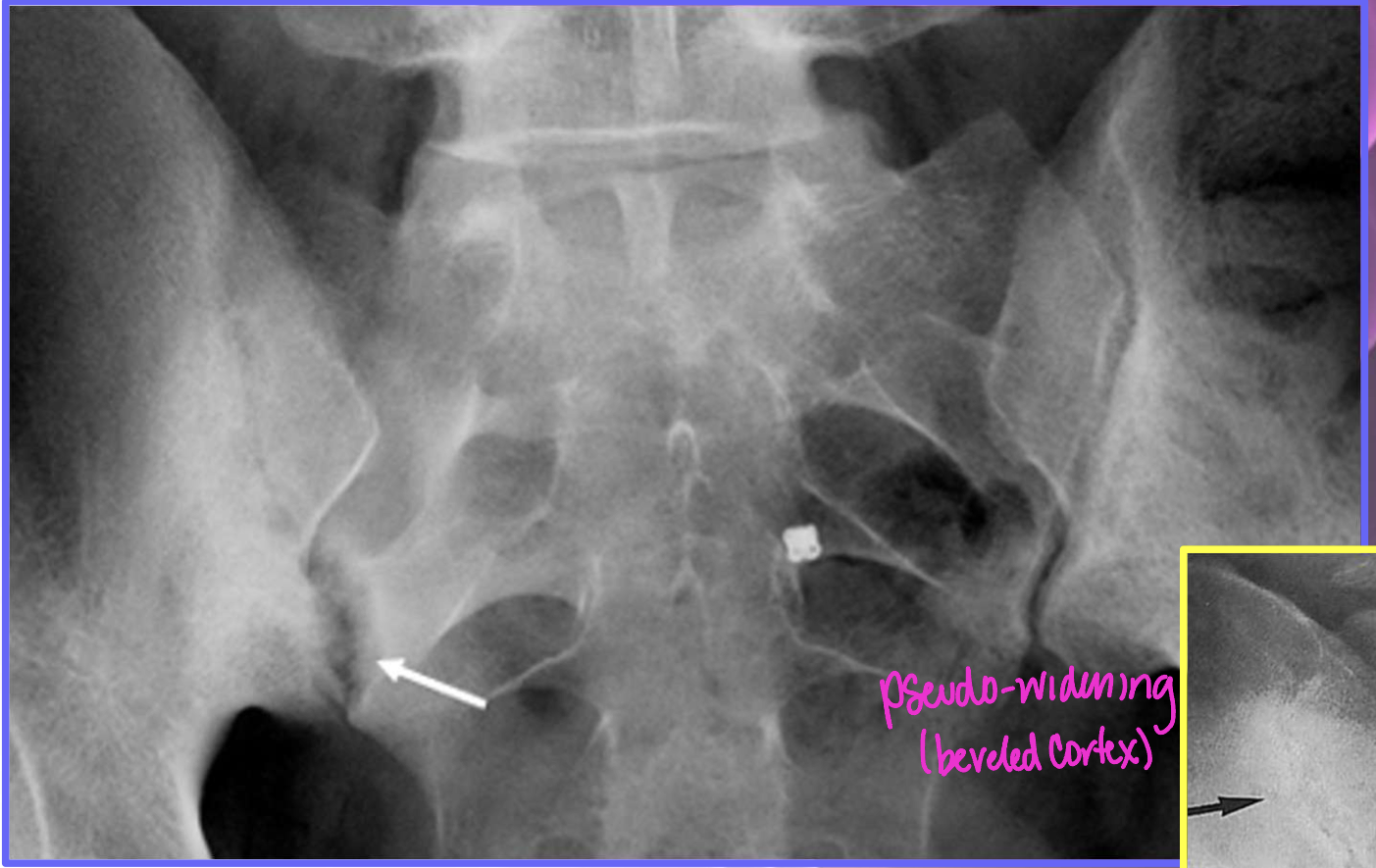
2 - sclerosis, some erosions
3 - severe erosions, pseudo-dilation of joint space, partial ankylosis
4 - complete ankylosis
We can see JSN and subchondral sclerosis in OA, which feature of AS is not seen in OA
erosions!!
With AS, don’t forget to
review prior imaging
(well-defined SI joints, 5yrs later poorly defined SI joints, 10yrs later ankylosis)
AS spinal findings are not enough to dx, what additional information/imaging do you need to be able to diagnosis AS
erosions of SI

What three DDx could you give this patient
OPLL
AH
OA/DDD
AS typical order of events (early to later findings)
corner erosions (Romanus lesions)
reactive sclerosis (shiny corner sign)
loss of anterior concavity (vertebrae squaring)
thin, marginal syndesmophytes (bamboo sign)
interspinous ligament ossification (dagger sign)
z-joint/facet capsular ossification (railroad track sign)
dagger sign + railroad track sign = trolley track sign
ischial enthesopathy (whiskering)
endplate destruction (andersson lesion)
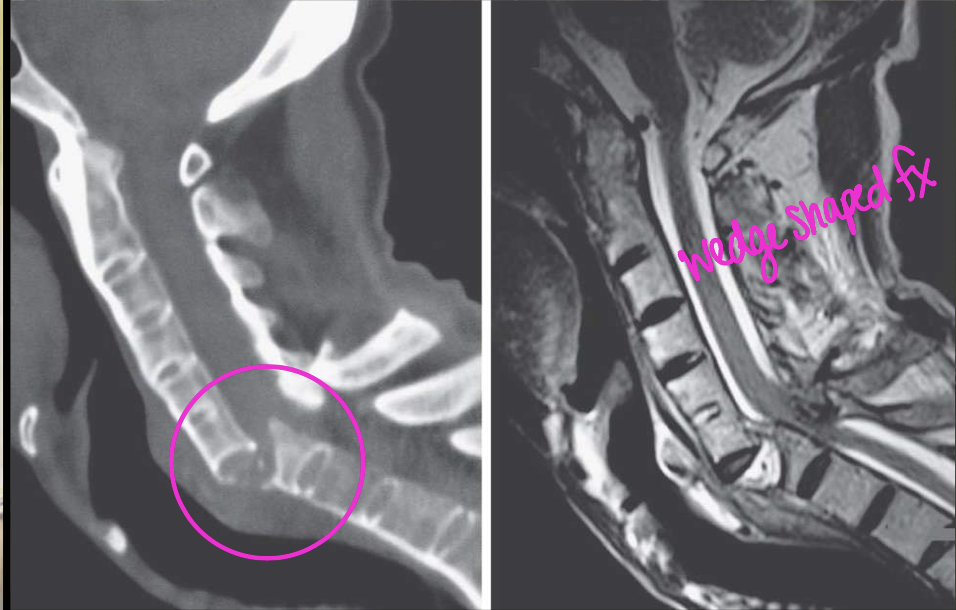
spinal fracture (carrot stick fracture)
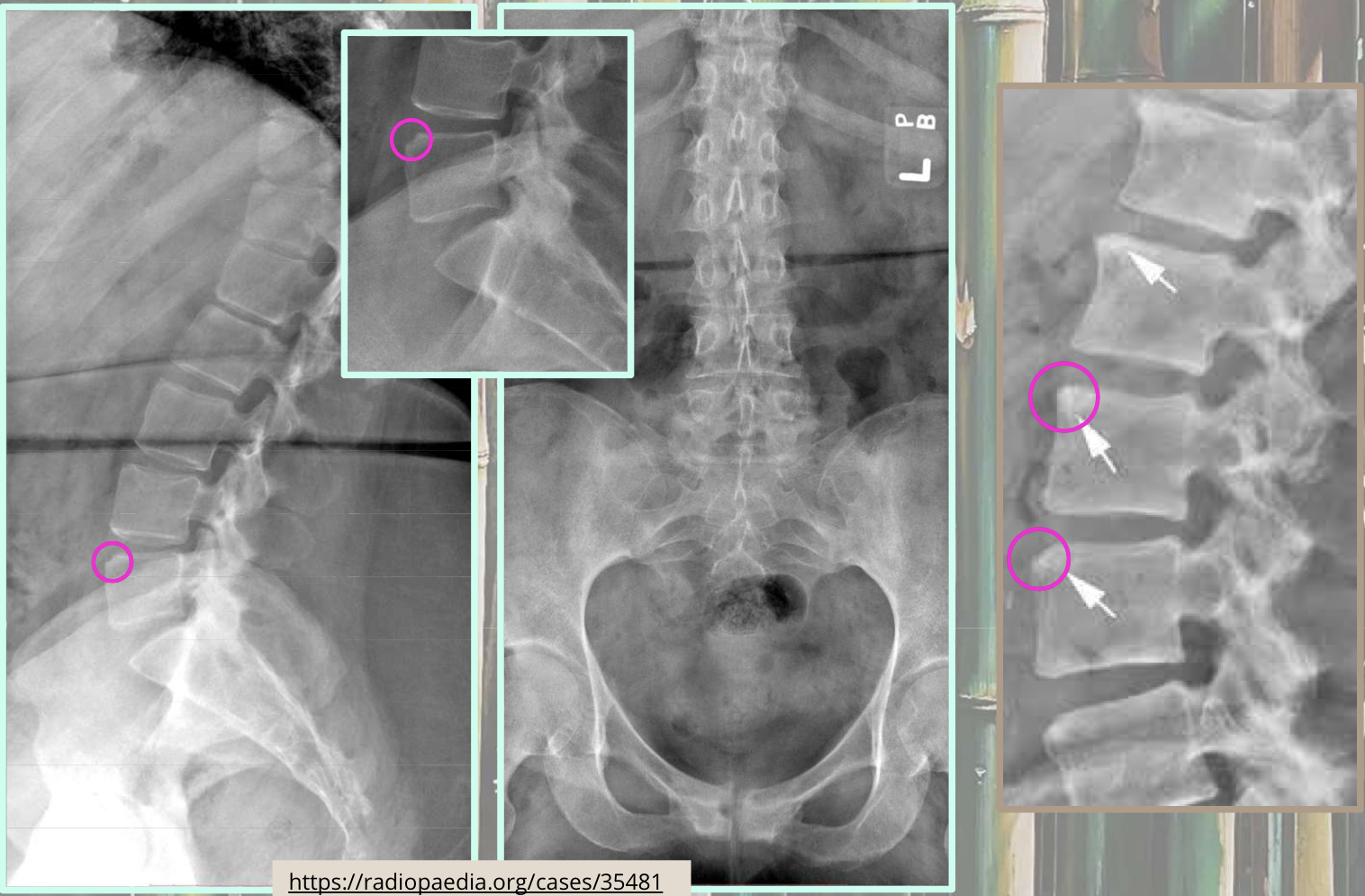
What two findings of AS are found in this image
Corner erosions (Romanus lesions)
Reactive sclerosis (shiny corner)

What two findings of AS are found in this image
Loss of anterior concavity (vertebrae squaring)
Reactive sclerosis (shiny corner)
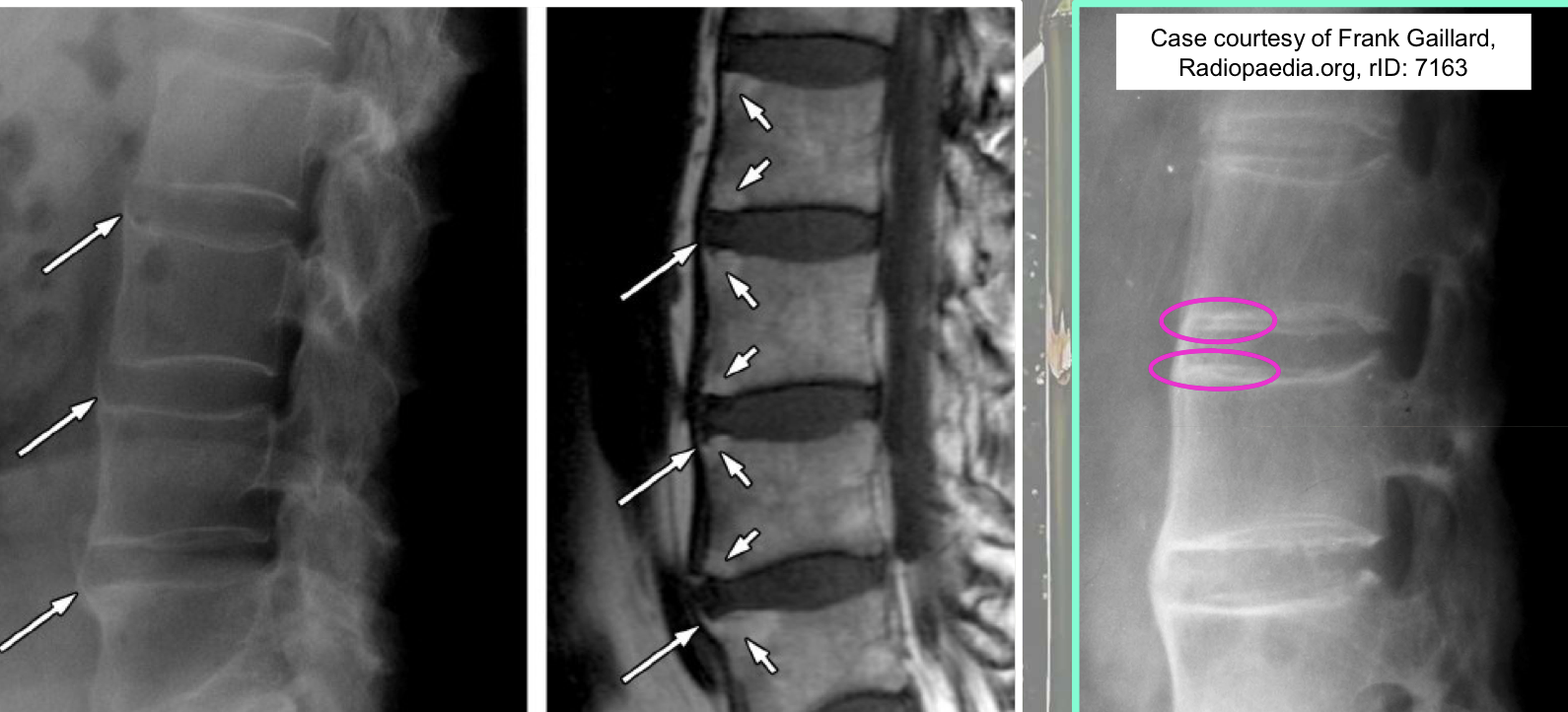
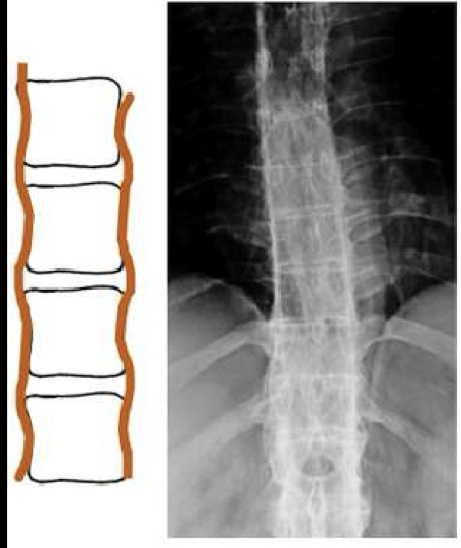
What finding of AS is found in this image
symmetrical, thin, marginal syndesmophytes (bamboo sign)
gracile/fragile
Where should you be looking every time you think the disease could be AS
SI joints
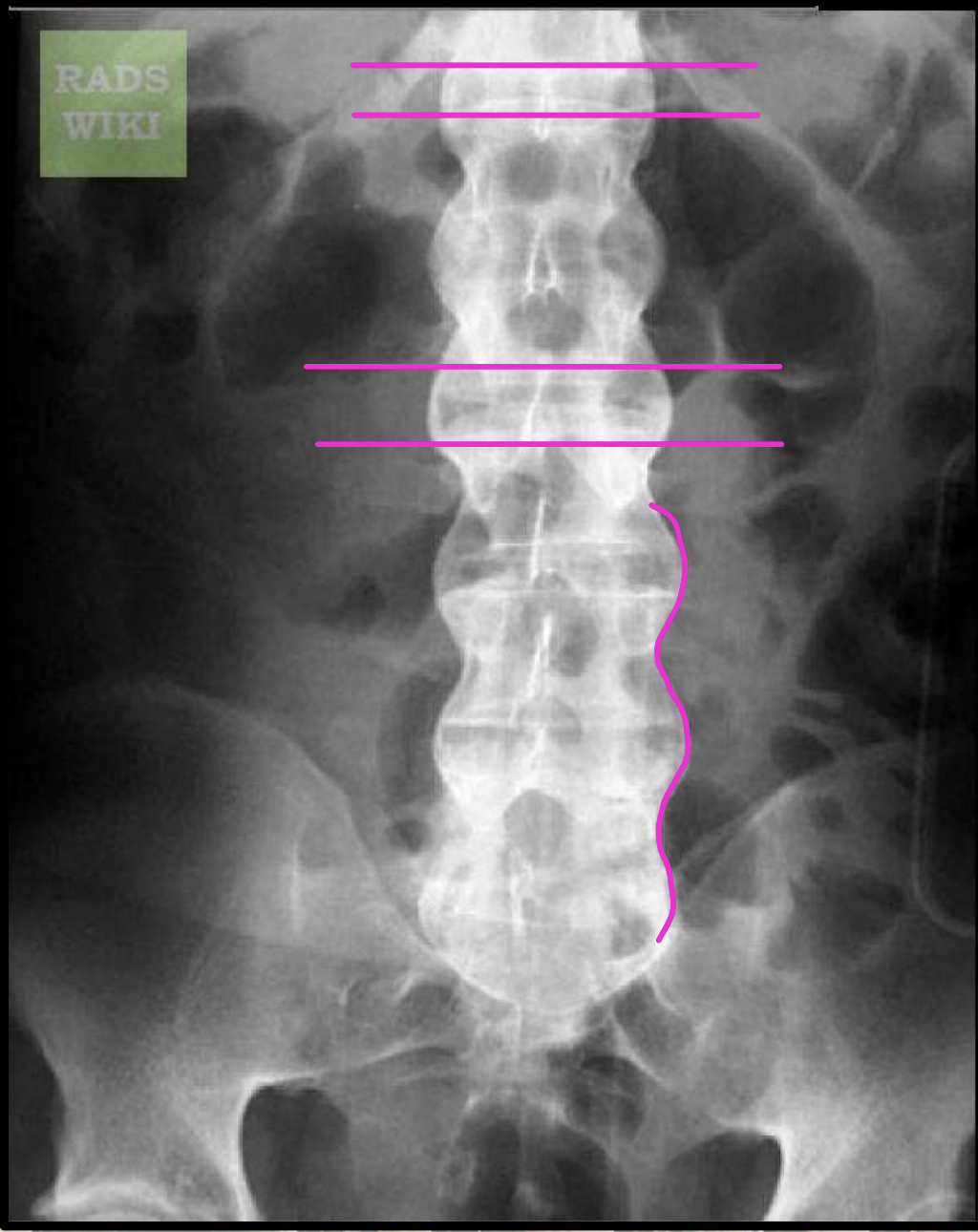
What finding of AS is found in this image
Interspinous ligament ossification (Dagger sign)
What finding of AS is found in this image
Z-joint/facet capsular ossification (Railroad track sign)
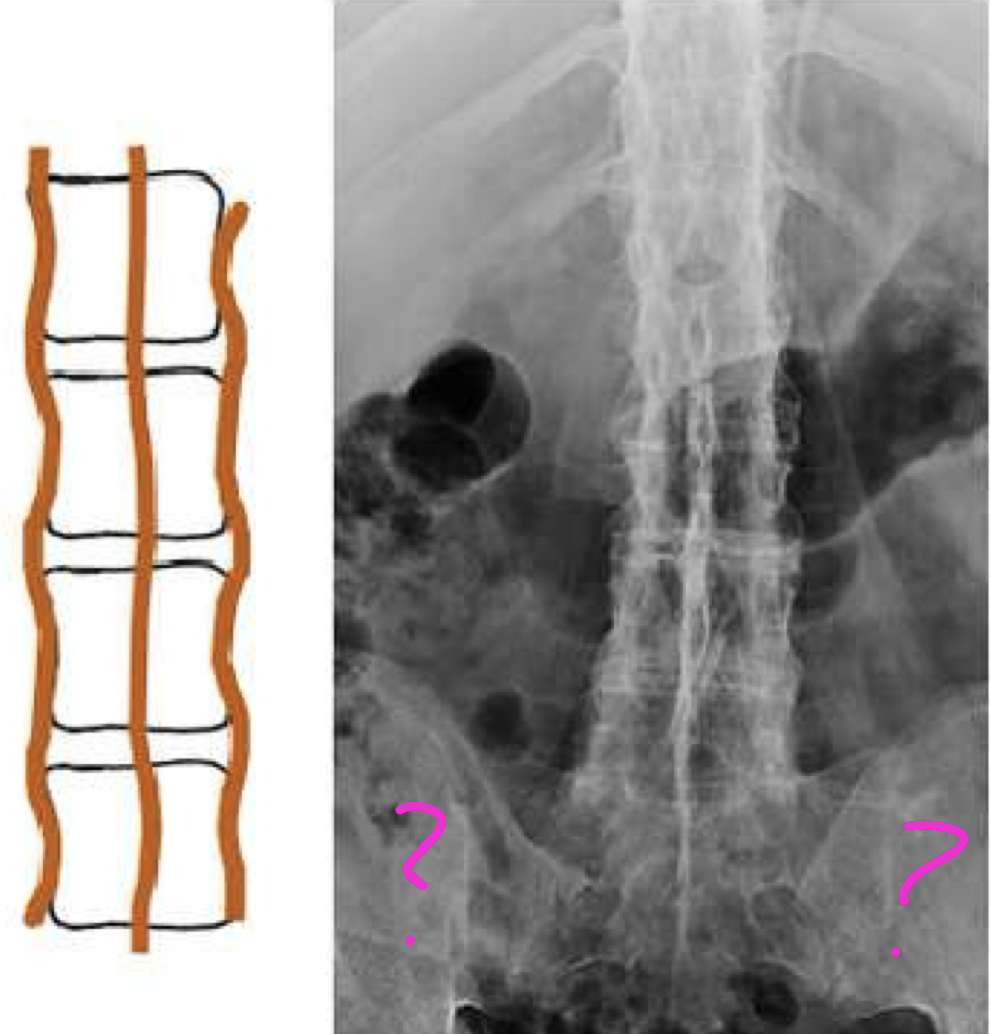
Dagger sign + Railroad track sign =
Trolley track sign
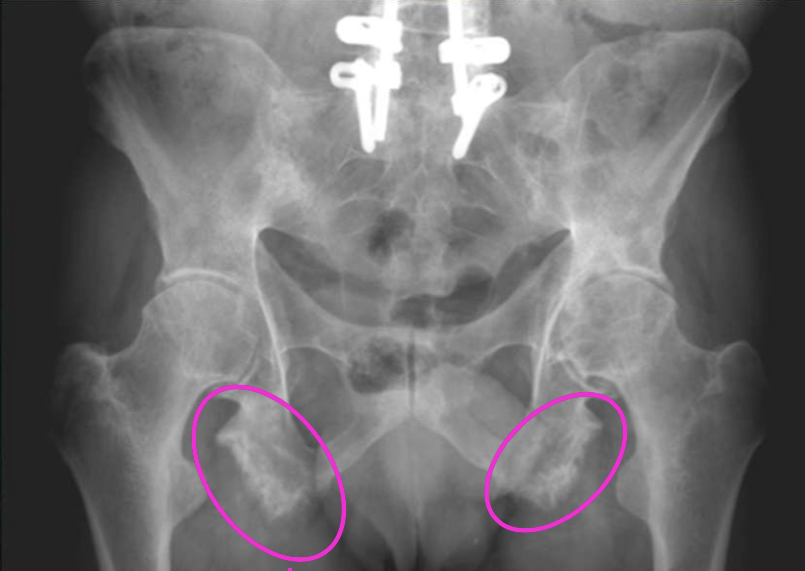
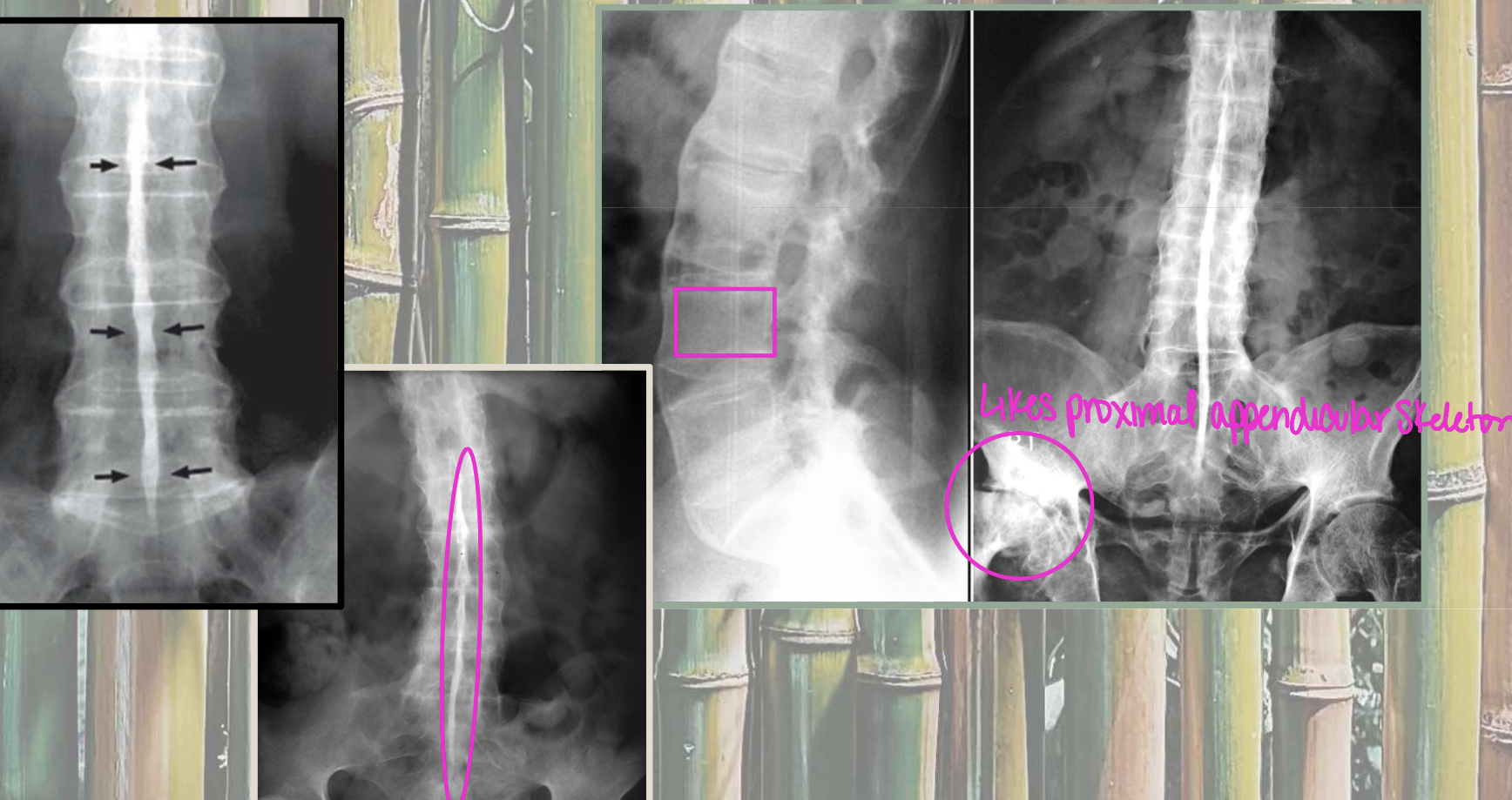
What finding of AS is found in this image
Ischial enthesopathy (Whiskering)
Ischial enthesopathy (Whiskering) could be found in AH as well, how would you ddx
via SI joints
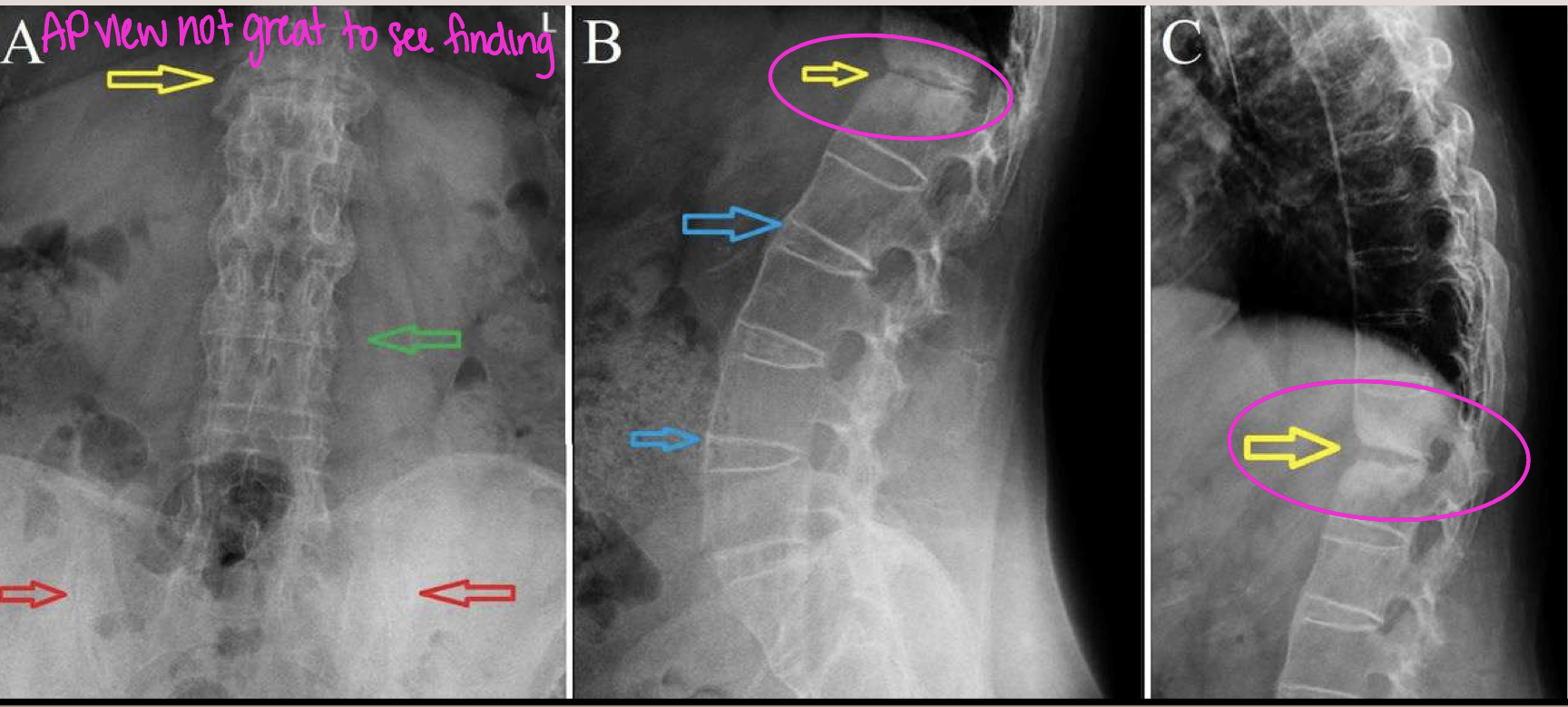
What finding of AS is found in this image
Endplate destruction (Andersson lesion)
causes loss of mobility and ability to shock absorb
Andersson lesion is also known as
rheumatic spondylodiscitis
What finding of AS is found in this image
Spinal fracture (Carrot/Chalk stick fracture)
IVDs hold vertebrae together still but can’t withhold forces
Erosive conditions with SI involvement
PEAR (AS 100%)
Osteomyelitis/septic arthritis/infection
Non-erosive conditions with SI involvement
OA
Osteitis Condensans Ilii (OCI)
compaction/condensation of cortical bone
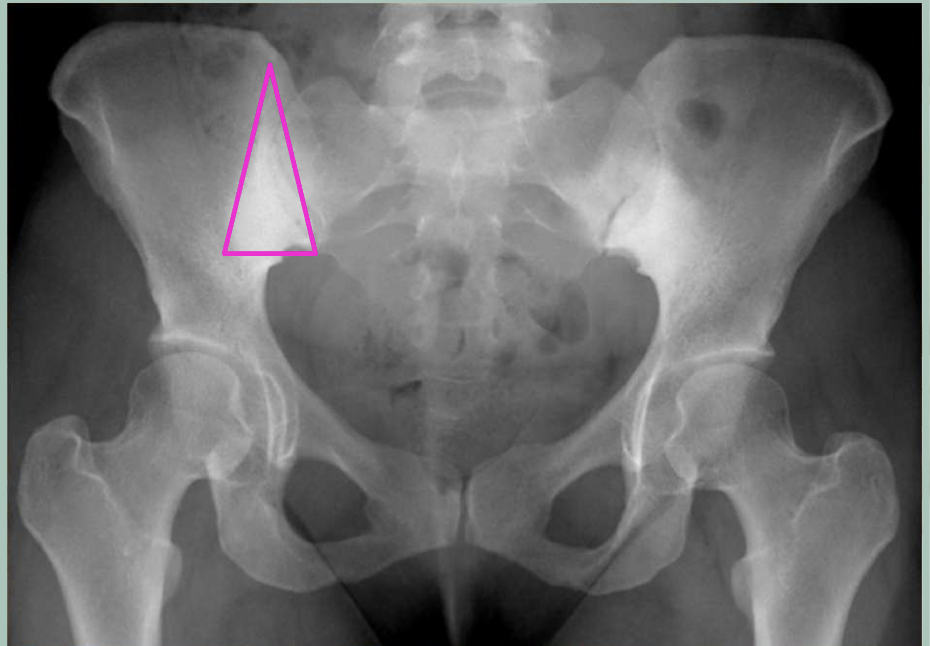
Osteitis Condensans Ilii (OCI)
sclerosis at inferior SI joint (Iliac side of joint ONLY)
NO erosions
triangular shape
What population is OCI most common in
postpartum females
(joint laxity, add sclerosis to increase stability)
Enteropathic arthritis
inflammatory spondyloarthropathy associated with inflammatory bowel disease (IBD)
In enteropathic arthritis, it is self-limiting but symptoms worsen with
flare-up of bowel disease
Enteropathic arthritis symptoms in the axial skeleton
morning stiffness
independent of GI symptoms
MC in Crohn’s disease
Enteropathic arthritis - when do symptoms show up in appendicular/peripheral skeleton
may precede intestinal involvement but usually at the same time as bowel disease
could show up as late as 10yrs after IBD diagnosis
Two types of peripheral enteropathic arthritis
1 - pauciarticular <5 joints
2 - polyarticular >5 joints
Where does peripheral enteropathic arthritis occur
heel - achilles and plantar fascia
knee - tibial tuberosity and patella
ischial tuberosities
Bowel resection for treatment of enteropathic arthritis may halt the peripheral arthropathy, but not the
axial arthropathy
Psoriatic arthritis
chronic disease of the joints and entheses
Upper extremity = hand
Erosive!!!!
Psoriatic arthritis (PsA) characteristics
soft tissue edema
asymmetrical JSN (MC DIP)
peripheral erosions w/periostitis (mouse ears)
central erosions (pencil in cup)
ankylosis and deformity
NORMAL bone density
unilateral/bilateral asymmetrical SI erosions
asymmetrical, thick, bulky, non-marginal syndesmophytes
Psoriasis (derm) _____ the onset of psoriatic arthritis
precedes (before)
Psoriatic arthritis occurs in what population
no sex discrimination
30-50 onset
may be linked to: HTN, T2DM, cardiovascular events
Why is RA a differential diagnosis for PsA
b/c they both have inflammatory markers

Psoriatic arthritis commonly starts as dramatic effects in
one joint
i.e. erosions that shorten digits (Dactylitis/ Sausage digits)

Differentials of OA, PsA and RH
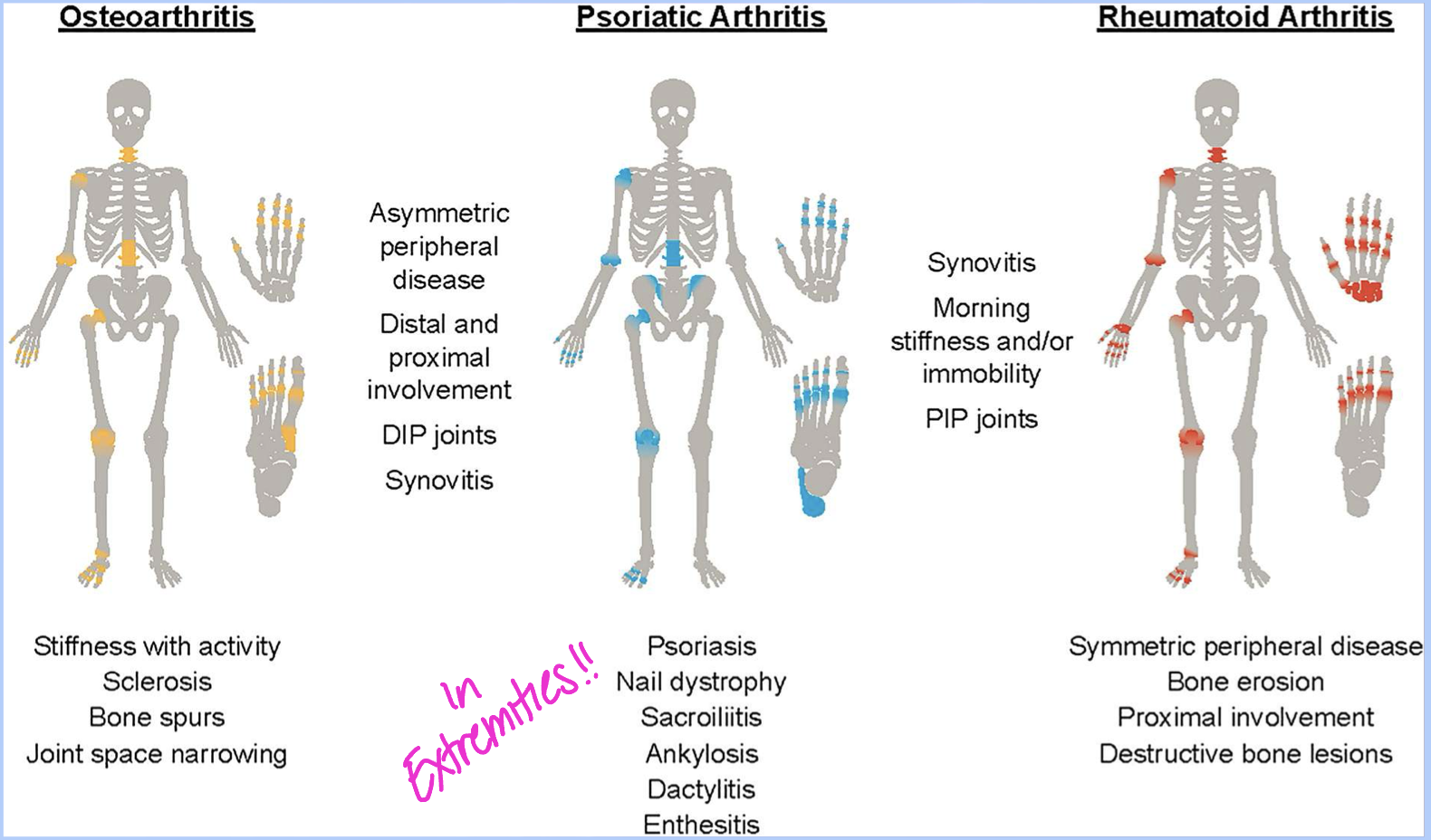
Proliferative synovitis results in
pannus
Psoriatic arthritis mimics of RA (rheumatoid)
JSN
soft tissue edema
marginal erosions at bare areas
ankylosis and deformity
Bare area
are in synovial capsule that is not covered by hyaline cartilage
Psoriatic arthritis distinctions from RA
AIP (acro-osteolysis)
Normal bone density
central erosions (pencil in cup)
asymmetrical - usually involves all joints of ONE digit (ray pattern)
New bone formation (sclerosis) is a key bone change that can be seen in Psa but NOT
RA
The surface of the bone erosion and proliferation in PsA may have a _______ appearance
fluffy (calcium may go into soft tissue)
What two findings of PsA are found in this image
periostitis (mouse ears) - lifts periosteum
soft tissue edema - leaves bone density alone
How are the erosions mentioned in the question beforehand different from RA
In RA… don’t lift periosteum, decrease bone density, goes wherever it wants

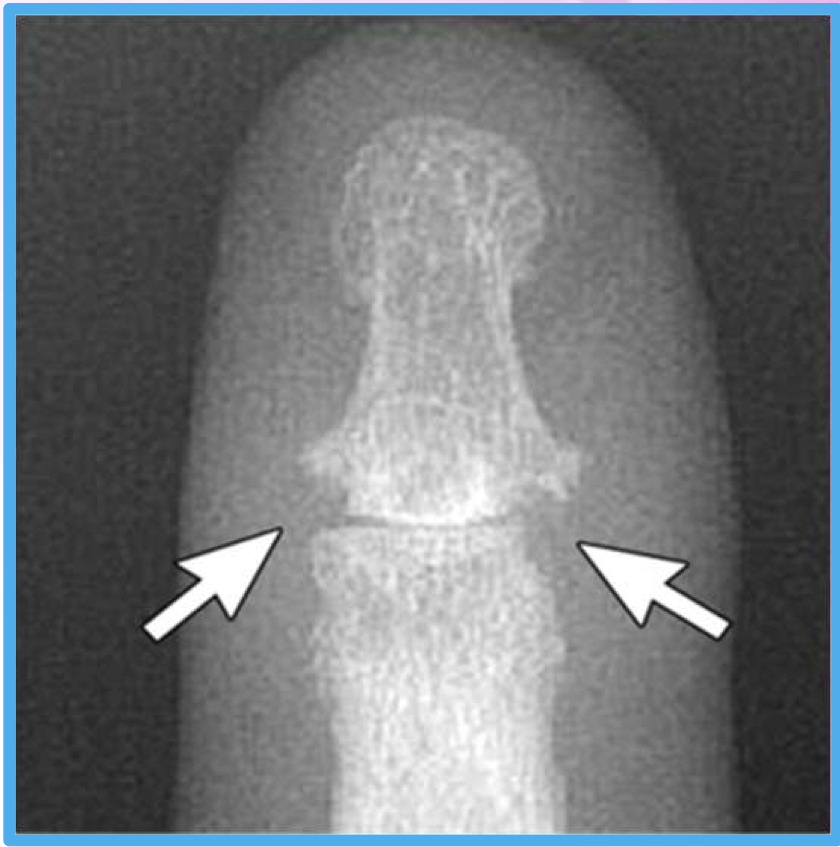
What finding of PsA is found in this image
central lesions (pencil in cup)

What finding of PsA is found in this image
Shortened digit (erosions)
Erosive OA (gull-wing erosions) typically occurs in what population
post-menopause females

What type of characterisitcs of PsA are found in this image
soft tissue edema
nail pitting
JSN + central erosions (pencil in cup)
periostitis (lifted periosteum - mouse ears)
Psoriatic arthritis mimics of Enteropathic arthritis
erosions, sclerosis, possible anylosis, syndesmophytes
Psoriatic arthritis distinctions from Enteropathic arthritis
unilateral or bilateral
asymmetrical
thick, bulky nonmarginal syndesmophytes
AS and Enteropathic arthritis syndesmophyte characteristics
symmetrical, thin, gracile/fragile marginal
PsA and Reactive arthritis syndesmophyte characteristics
asymmetrical, thick, bulky nonmarginal (above and below endplates)
Why is this image’s dx NOT Osteitis Condensans Ilii (OCI)
b/c erosions
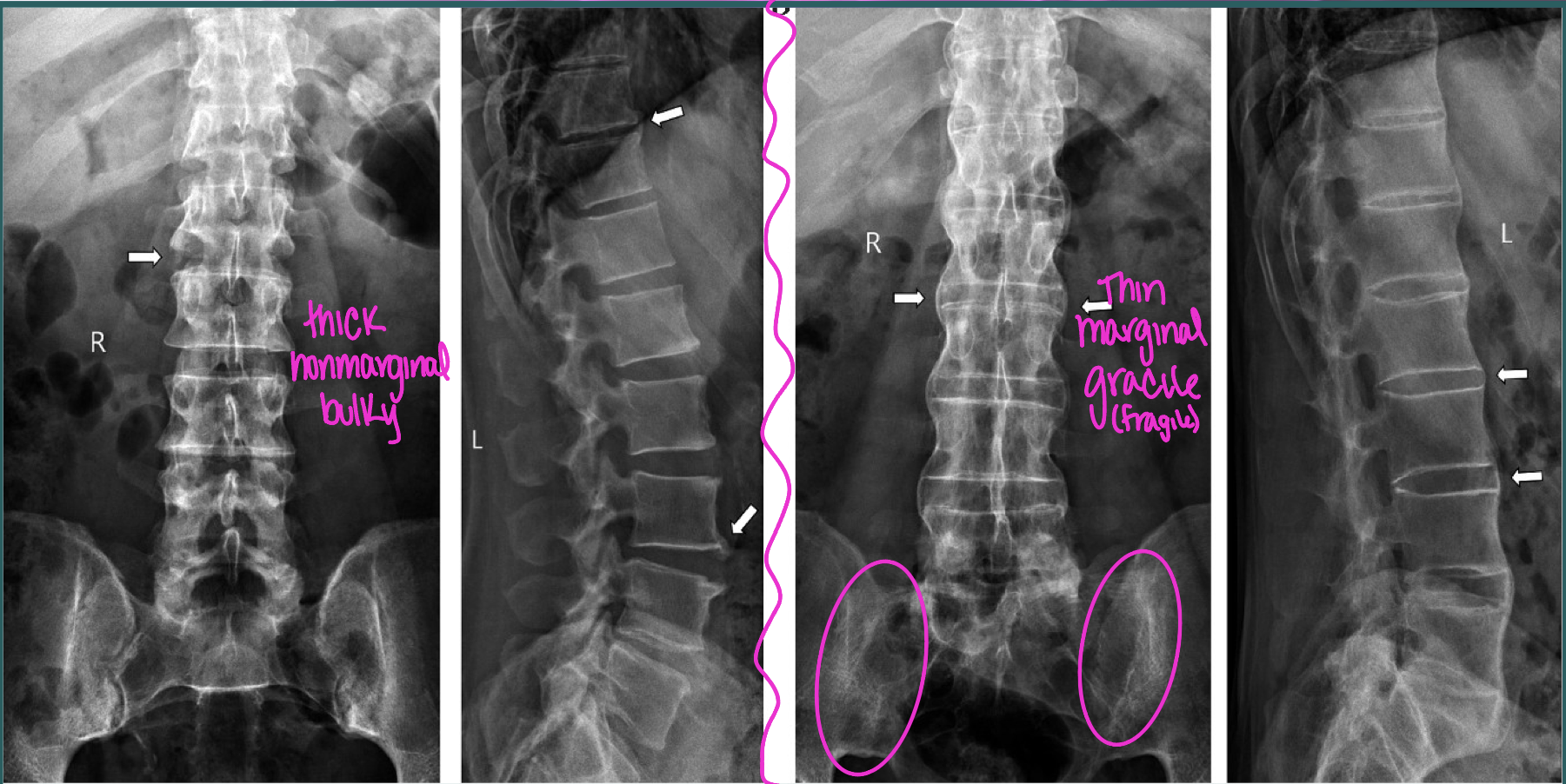
What are the two dx of these images (left vs right)
Left = PsA
Right = AS
Reactive Arthritis (ReA)
autoimmune condition caused by GI or GU infection (2-4 wks after)
shigella, salmonella, campylobacter
asymmetric oligoarthritis
dactylitis (sausage digit)
lower extremity = Achilles insertion (weight bearing)
Classic triad of Reactive arthritis
Noninfectious urethritis, Arthrtits, Conjunctivits
(can’t see, can’t pee, can’t climb a tree)
What population does ReA occur in
males
What two diseases are primarily associated with weight bearing joints
OA + Reactive arthritis
Reactive arthritis looks like PsA, but just not
as extreme
Reactive arthritis mimics of PsA
JSN
soft tissue edema
normal bone density
periostitis (mouse ears)
asymmetrical, thick, bulky nonmarginal syndesmophytes
Reactive arthritis distinctions from PsA
MC in lower extremity
no nail pitting
central erosions (pencil in cup) not common
Lover’s heel (ReA)
describes predominance of the plantar and calcaneal insertions
Spondyloarthritis often beginning in young people with symptoms starting
before age 45
Rheumatoid arthritis is primarily a
bone density ROBBING disease (don’t even need erosions present to dx)
RA symptoms
stiffness in morning (jelling phenomenon) - OA mimic!
in PIP and MCP (Haygarth) joints
osteopenia!!!
Rheumatoid Arthritis Diagnosis checklist
morning stiffness for at least 6 wks
pain on joint motion for at least 6 wks
swelling of at least 1 joint for at least 6 wks
swelling in at lest 1 other joint for more than 6 wks
bilateral symmetrical joint swelling
subcutaneous nodules
DDx from RA and OA
OA - asymmetrical JSN in weight bearing
RA - symmetrical JSN in non-weight bearing
Distribution of RA in hand joints
MCP = Haygarth, IF nodes
PIP = Bouchard, IF nodes
Ulnar aspect of wrist
All soft tissue hand nodes
MCP = Haygarth nodes (CPPD + RA)
DIP = Heberden nodes (OA)
PIP = Bouchard nodes (OA + RA)
RA likes to FIRST impact synovial joints at bare areas causing
pannus and decreased bone density
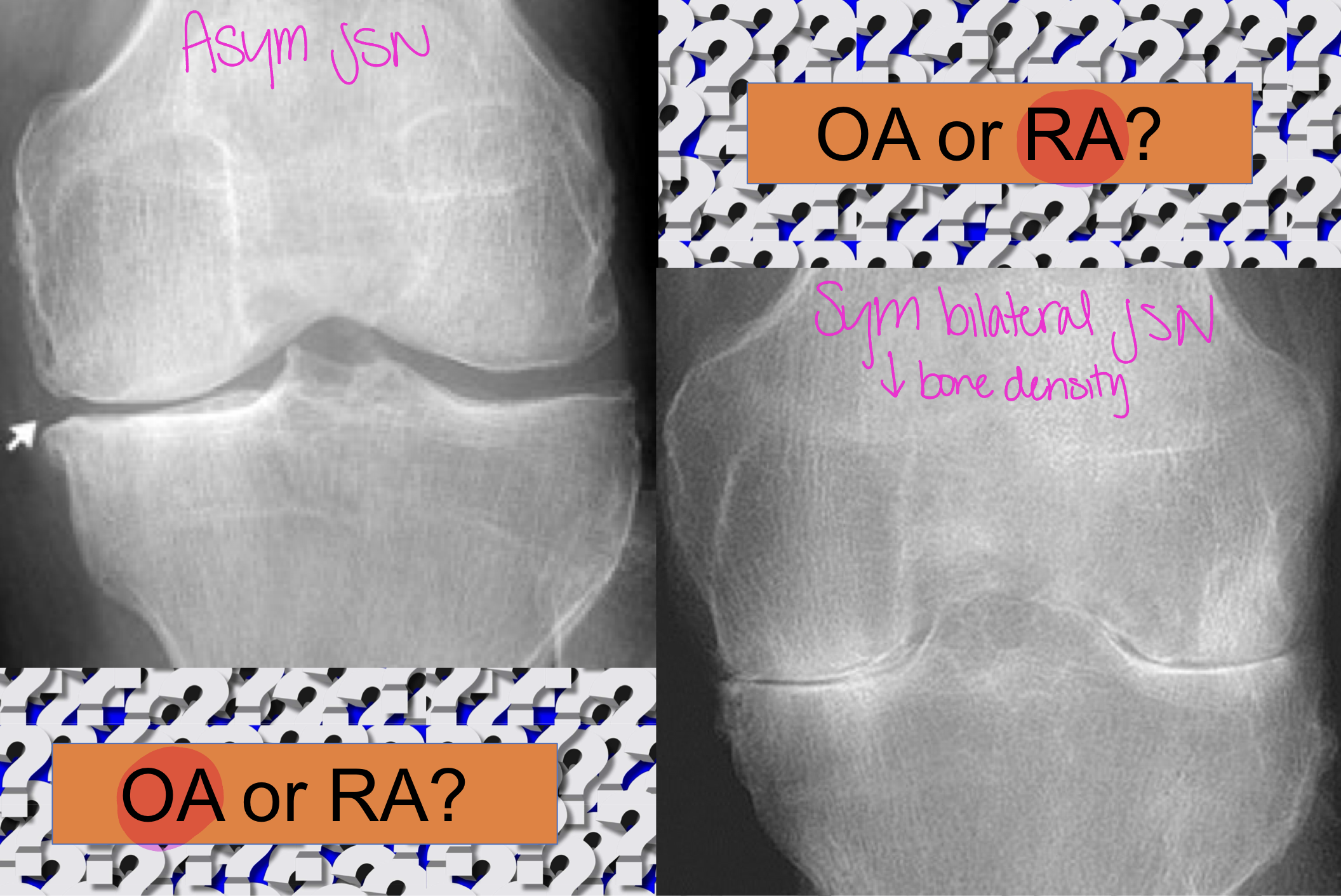
OA or RA (left vs right)
Left - OA
Right - RA

OA or RA (left vs right)
Left - OA
Right - RA
Rheumatoid arthritis
multisystem (systemic) disease
pts with higher RF levels tend to have a more severe disease
inflammatory hyperplastic synovitis (pannus)
Rheumatoid arthritis occurs in what population
20-60 females
>60 no sex discrimination
Proliferating pannus in RA erodes cartilage and releases ______ and can cause
chondrolytic collagenase enzymes
subchondral cysts (pannus intrusion)
Associated terms with RA
arthritis mutilans - severe joint deformity
Baker’s cyst - enlargement of gastrognemius bursa (trauma → inflam)
Felty’s syndrome - leukopenia, splenomegaly, RA
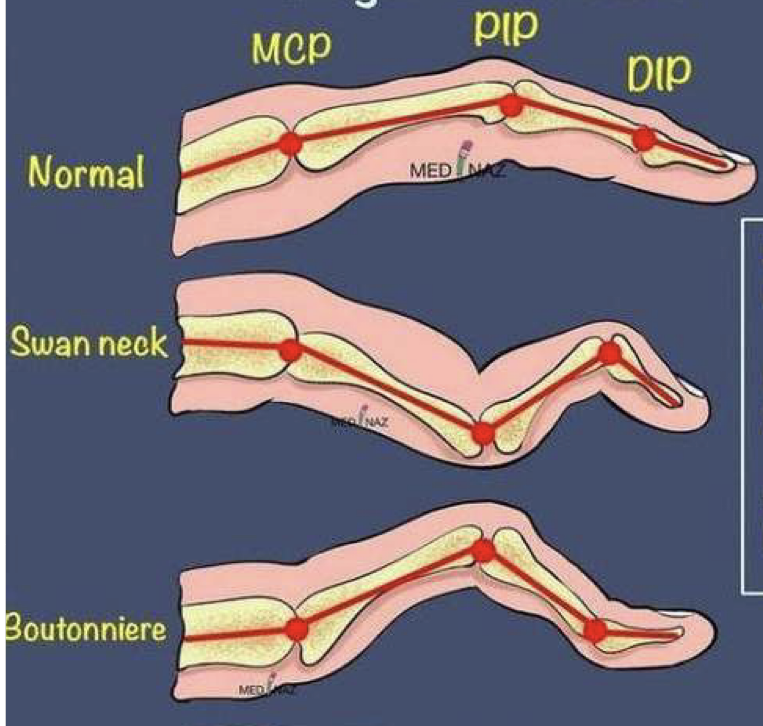
Rheumatoid arthritis finger deformities
Boutonniere deformity - PIP flexion and DIP extension
Swan neck deformity - PIP extension and DIP flexion
Radiographic features of RA
marginal erosion - “rate bites”
loss of intra-articular cortex adjacent to capsular insertion (b/c pannus)
dot-dash appearance
Hyperplastic synovitis (pannus) cannot be seen on x-ray well, what other modalities should you use
MRI + CT
Radiographic findings in RA (early to late)
periarticular soft tissue swelling
juxta-articular osteopenia (density loss on bare areas)
symmetrical JSN
erosions (beginning in bare areas)
subchondral cysts
joint deformity due to connective tissue laxity/disruption
secondary OA, possible ankylosis

What finding of RA is found in this image
rat bite marginal erosions

What two findings of RA are found in this image
symmetrical JSN
marginal erosions