Superficial Fungal Infections
1/8
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
9 Terms
Recognize the pharmacologic category, dosage form (topical or oral), and Rx vs OTC status of antifungals used for superficial fungal infections
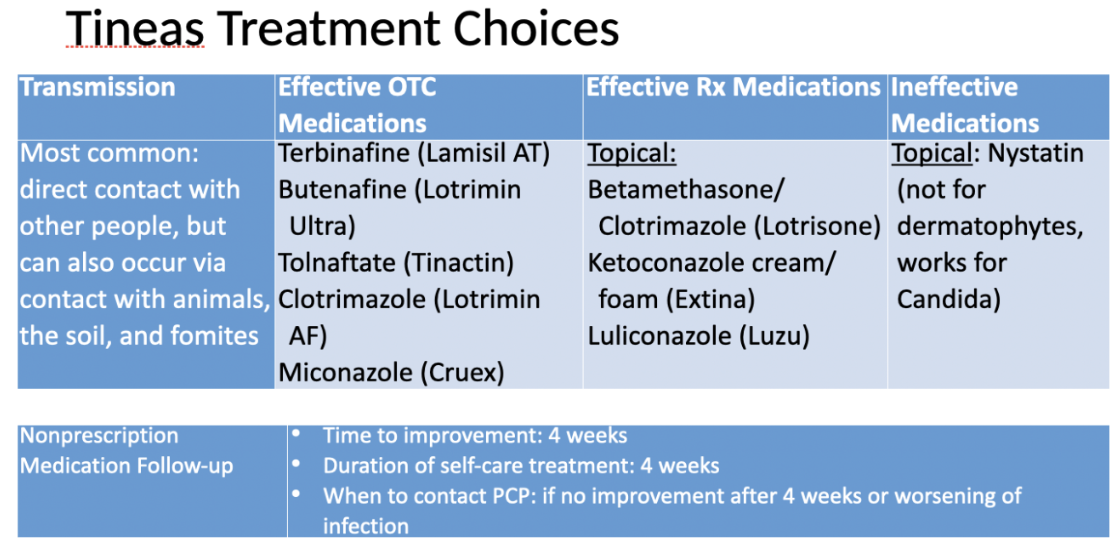
OTC Antifungal Agents - Topical
Tolnaftate
Aerosol powder 1%, aerosol solution 1%, cream 1%, gel 1%, powder 1%, solution 1%
Indecylenic acid
Clontrimazole
Cream 1%, lotion 1%, ointment 1%, solution 1%
Ketoconazole (also available in prescription by oral)
Micronazole
Aerosol powder 2%, aerosol solution 2%, cream 2%, ointment 2%, powder 2%, solution 2%
Terbinafine (also available in prescription by oral)
Cream 1%
Butenafine
Cream 1%
Forms
Creams, lotions
Ointments
Solution
Foam, shampoo
Powder, aerosol spray or powder
Gel
Suspension
Rx antifungal agents
Oral
Fluconazole
Itraconazole
Terbinafine
Griseofulvin
Narrow spectrum, ADE/toxicity/DDI
Topical
Ciclopirox
Nystatin
Athlete’s Foot (Tinea Pedis)
Nonpharm (athletes foot)
Avoid tight fitting or enclosed shoes for long periods of time
Wear protective/shower shoes in public showers
Cleanse the skin daily with soap and water, and thoroughly pat dry including between toes
Wear socks that don’t hold moisture/are moisture-wicking
Do not share towels, clothing, or other personal articles with family members, especially when an infection is present
Launder contaminated towels and clothing in hot water to prevent spreading the infection
Use of Antifungal agents in athlete’s foot
Some locations are harder to penetrate/reach/cure and may require oral therapy and/or longer treatment times
Topical agents are considered first line therapy for infections of the skin
Topical products are available in different formulations for different reasons
Powders do not work well for treatment but may be used for prevention (like in shoes)
creams/gels work best are are used mostly
Ointments are best for scaly or weeping areas
Solutions are easier for hairy areas
Topical treatment duration = 4 weeks
Can cure by 2 weeks; some require 4-6w
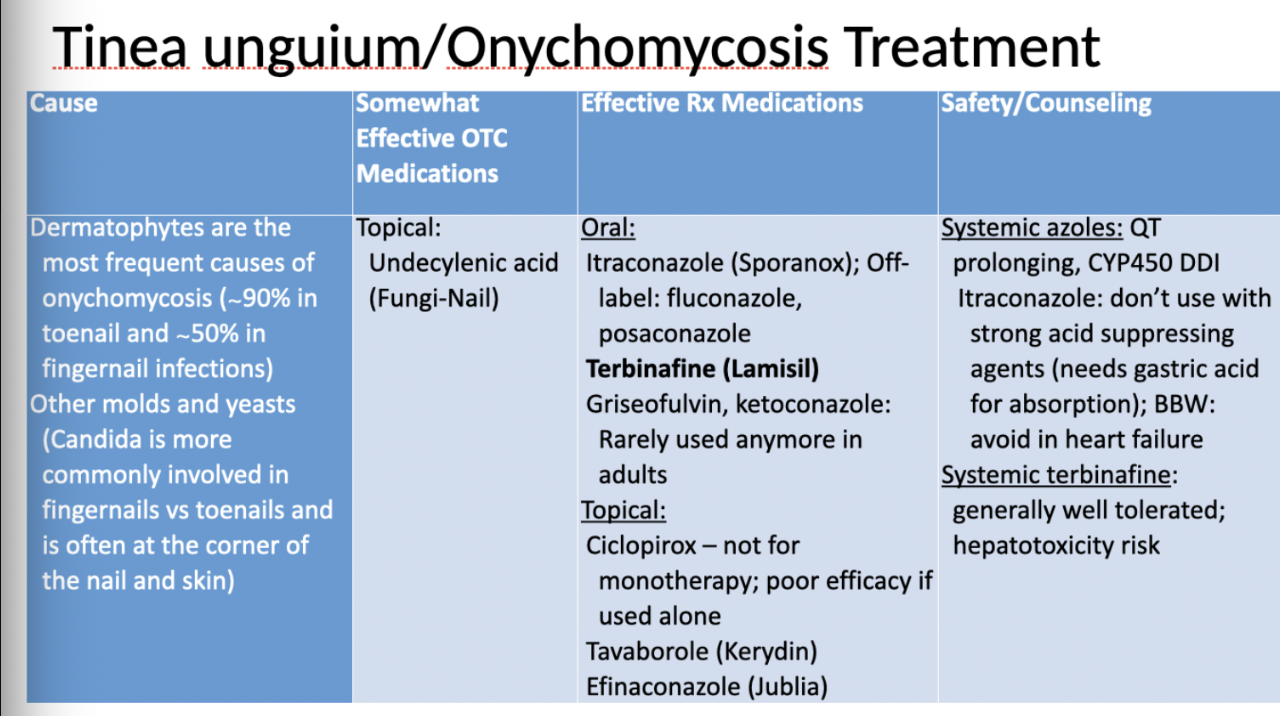
Oral therapy preferred when infection is extensive (covers as large skin area) or severe or when treating onychomycosis (nails)
OTC warning
Always check the Drug Facts label for the active ingredient in the product
The same brand name of OTC product does not always contain the same active ingredient
Eg. Lotrimin AF might have clotrimazole, miconazole, or tolnaftate
Differentiate between the antifungal OTC formulations and generations when selecting a product for a patient
Comparing OTCs for Tinea Pedis
Earlier gen antifungals
Clontrimazole (fungistatic)
Miconazole (fungistatic)
Tolnaftate (fungistatic)
> 2 years of age; twice daily for 4 weeks, less expensive
Second gen antifungals
Butenafine (mixed info on fungistatic vs fungicidal)
Terbinafine cream, spray (fungicidal)
> 12 years of age: twice daily for 1 weeks or once daily for 4 weeks
Terbinafien preferred if also on bottom/sides of feet
Third gen antifungal
Terbinafine GEL formulation (fungicidal)
> 12 years of age: once daily for 1 week
Recommend an OTC product and counsel a patient on proper treatment of tinea; recognize exclusions for self treatment
Self-care fungal infections
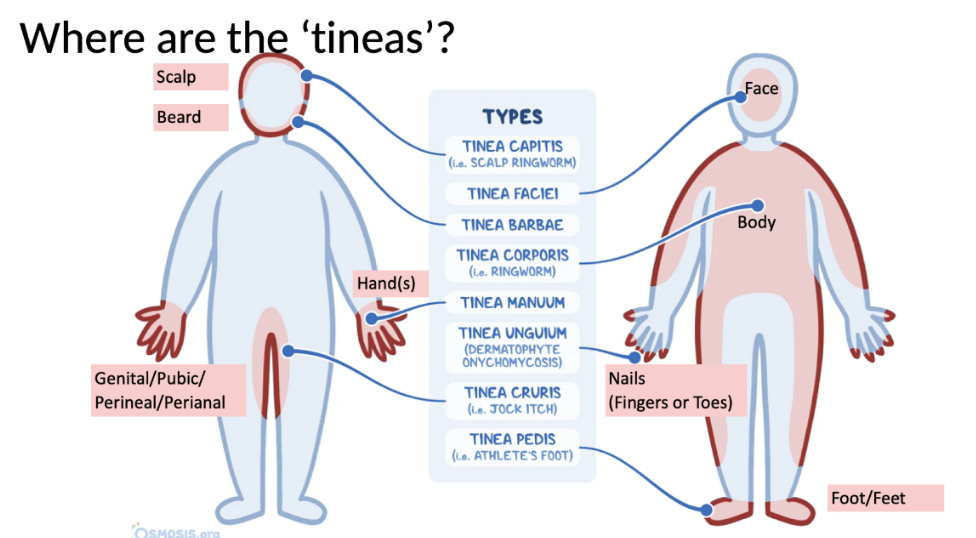
Tinea corporis (body)
Tinea cruris (jock itch)
Tinea pedis (athlete’s foot)
Exclusions to Self-Care
Patient has a weakened immune or blood circulation system
Patient with diabetes if not currently under the supervision of provider
Suspicion of systemic infection (eg. fever, malaise)
Suspicion of bacterial infection also present (eg. oozing, purulent)
If prior self-treatment failed to clear the rash and was used appropriately along with nondrug prevention measures
Stronger agent may be needed
Certain tinea locations:
Since topical agents do not penetrate the hair shaft, infections associated with hair and hair follicles (e.g. scalp and beard tinea)
Require oral prescription therapy
Fungal nail infections often respond better to oral therapy than topical therapy; if patient returns or has had before, likely best to refer to doctor
May require prescription for oral therapy or stronger topical polish
Mucus membranes are also involved (e.g. mouth, genitalia unless recurrent vulvovaginal candidiasis – not covered in this unit)