CM II Week 8 (HIV)
1/149
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
150 Terms
immune system review
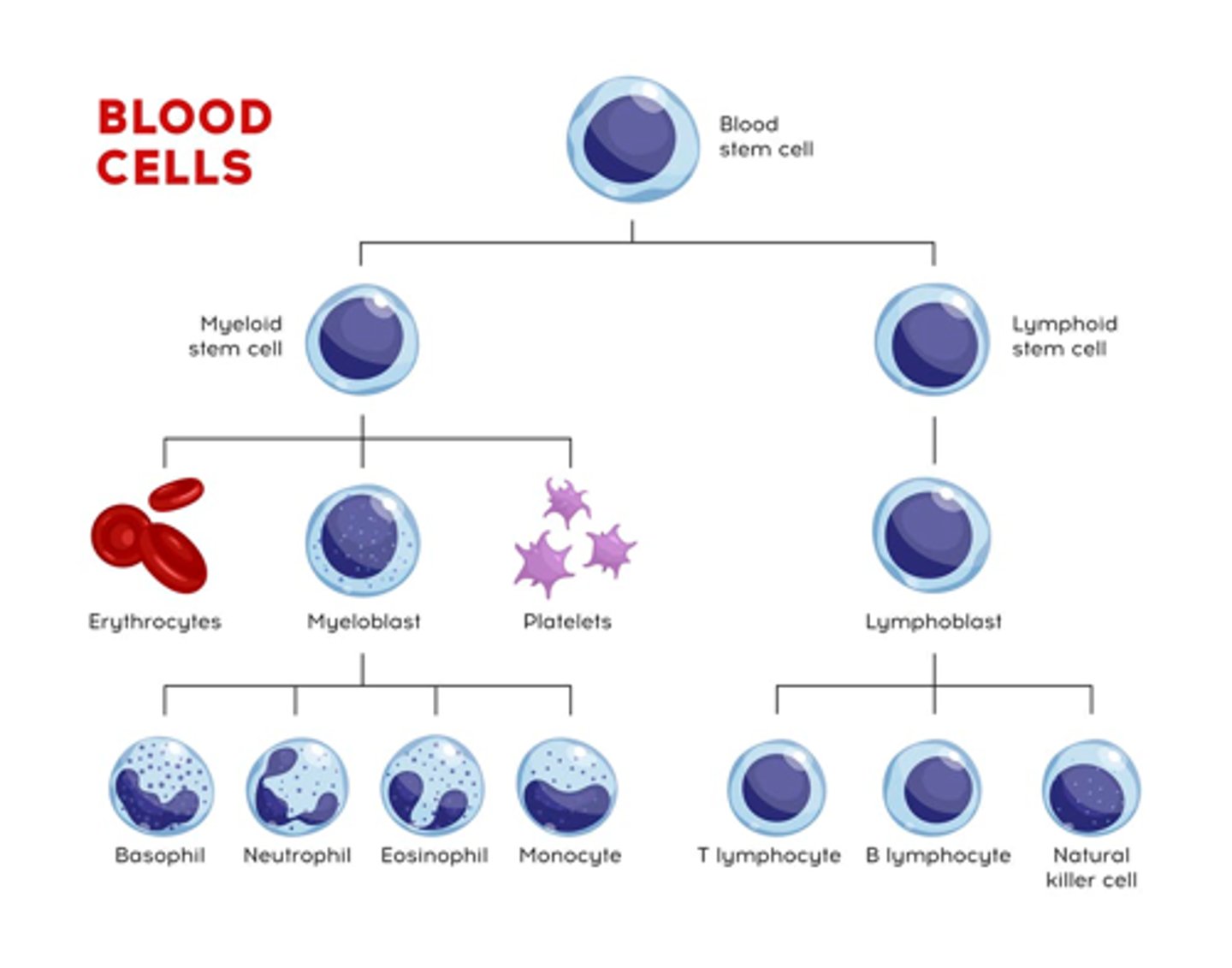
B cells
–Main function: humoral immunity (creating specific antibodies)
T cells
–Two main functions: regulating immune system and killing cells with specific target Ag’s
•CD4+ helper cells: activate B cells, killer cells, and macrophages
•CD8+ cells: two types
–Cytotoxic CD8+ cells which kills cells infected by viruses or bacteria
–T-suppressor cells which inhibit immune responses
HIV
what type of virus? types? where?
HIV is a retrovirus in the Retroviridae family (Lentivirus genus)
Two species: HIV-1 and HIV-2
‣ HIV-1 more virulent and more infective than HIV-2
Most patients in US are HIV-1 infected
HIV-2 mostly confined to West Africa
HIV structure & overall what does it cause?
HIV viruses are enveloped, single-stranded RNA viruses with a DNA intermediate
• DNA intermediate is an integrated viral genome (provirus) that persists within the host-cell DNA
HIV causes severe damage to the immune system and eventually destroys it
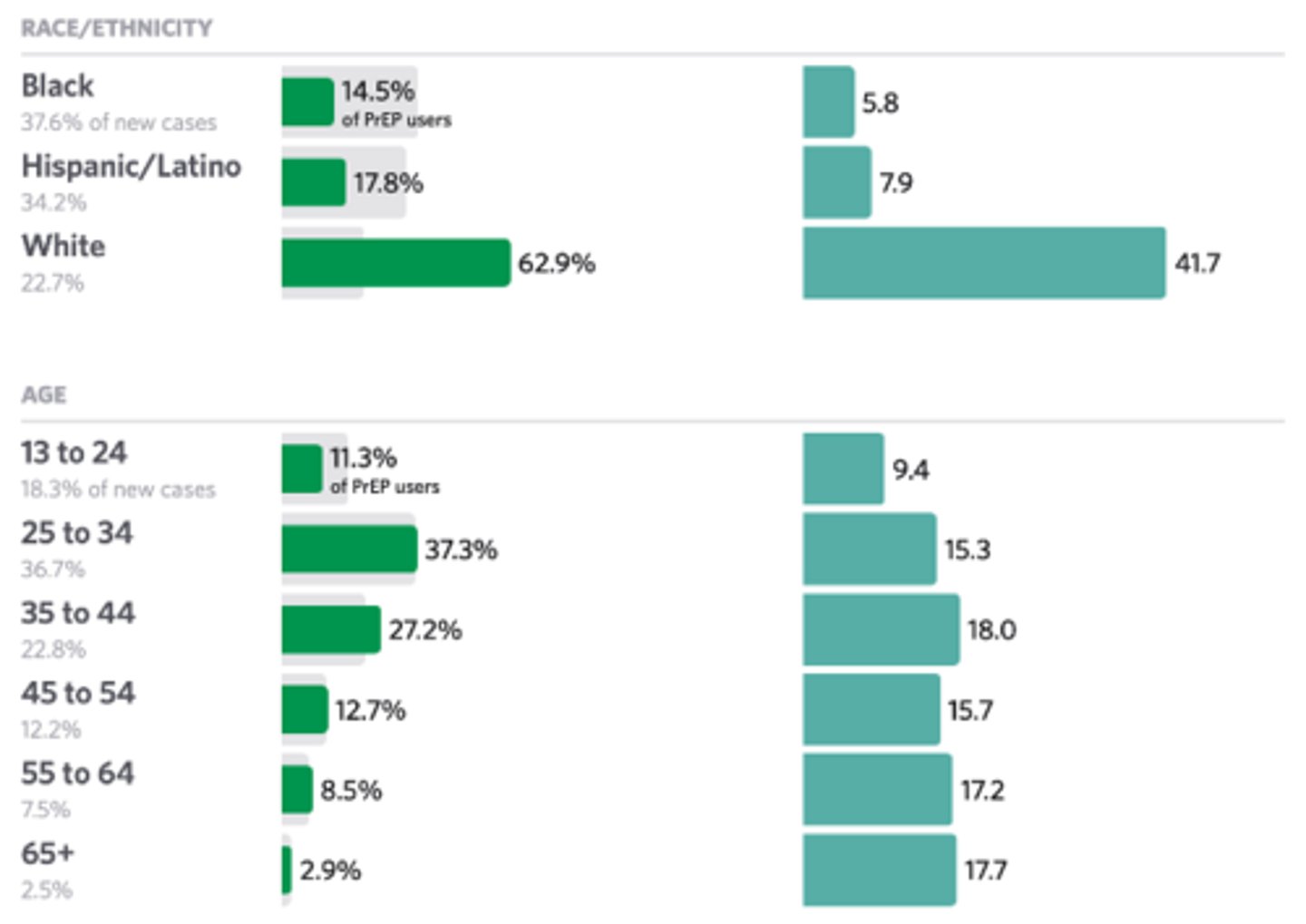
what population is at increased risk for HIV?
black males, females.
not high numbers on PrEP - we as providers need to recognize this in treatment
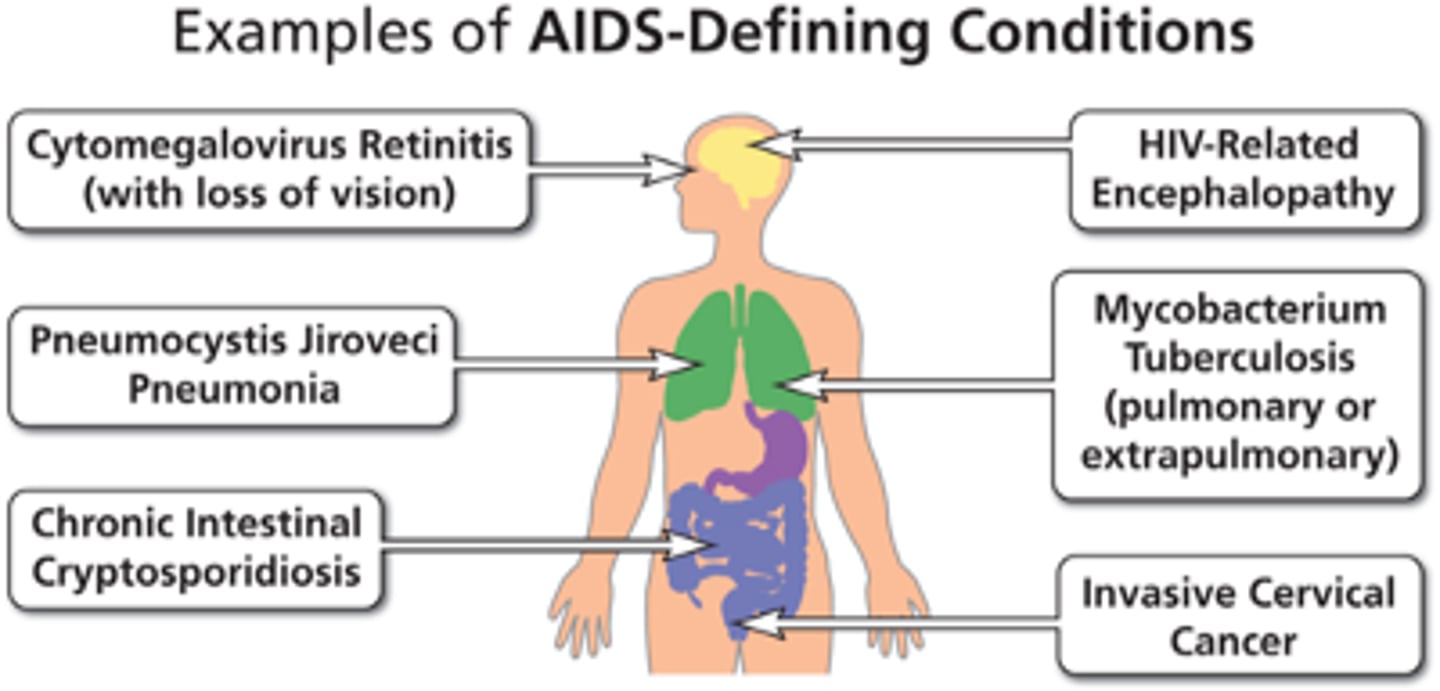
HIV vs AIDs definition
HIV – Human Immunodeficiency Virus: Virus which can lead to AIDS
AIDS – Acquired Immune Deficiency Syndrome
• Disease caused by the damage that HIV does to the immune system
• Defined as an absolute CD4+ count <200 cells/microL or presence of an AIDS-defining condition
• Most severe phase of HIV infection
HIV and AIDS are NOT the same thing
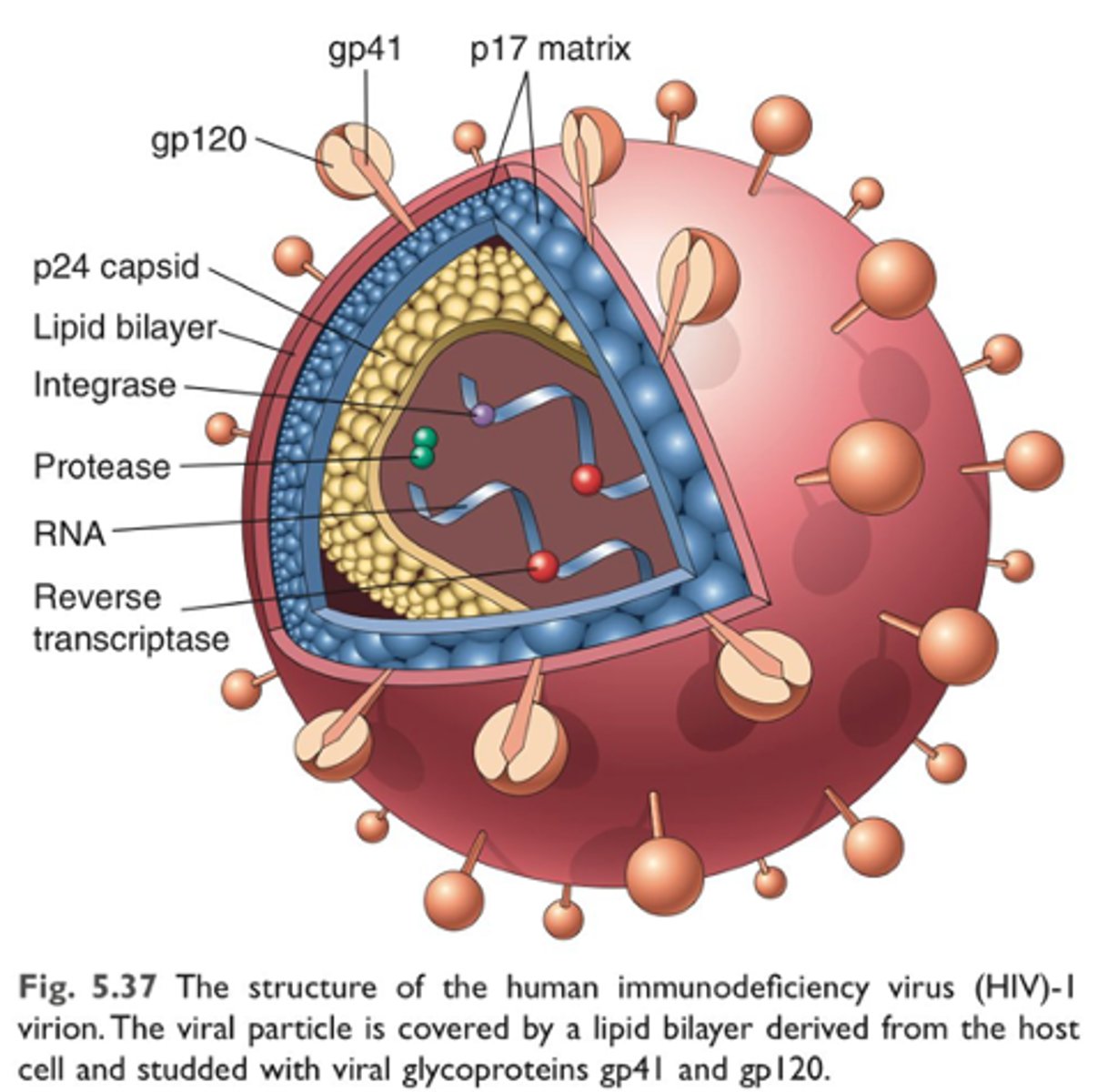
HIV Viral Structure
Cylindrical center surrounded by a sphere-shaped lipid bilayer envelope
Inner sphere contains 2 SS copies of RNA as well as multiple proteins and enzymes necessary for HIV replication and maturation
• p24, p17, reverse transcriptase, integrase, and protease
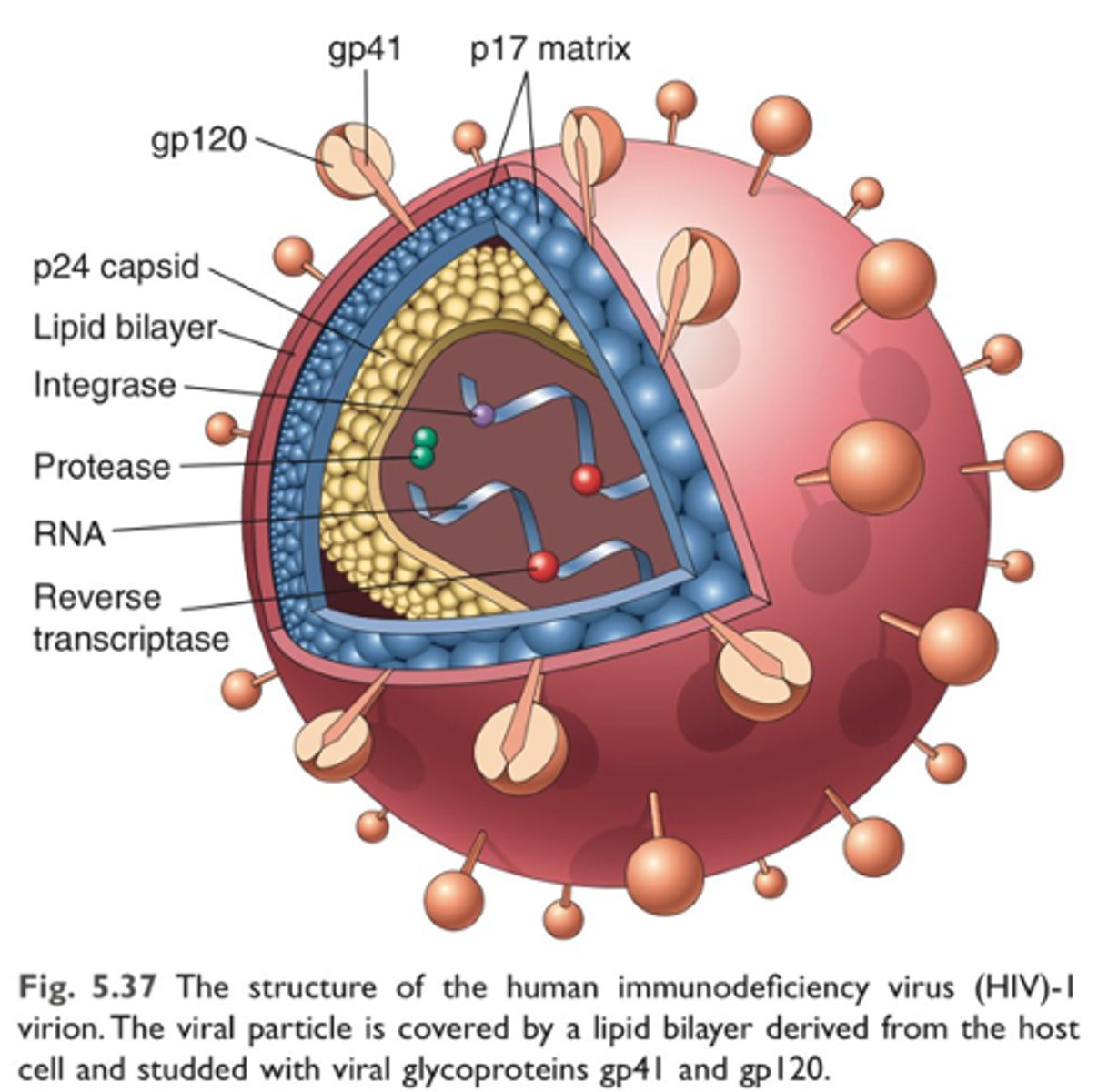
Two major viral glycoproteins in lipid bilayer of HIV
gp120 and gp41
help virus to attach to and invade CD4+ cells
Integrated HIV proviral DNA is _______ DNA flanked by _________
Integrated HIV proviral DNA is double-stranded DNA flanked by LTRs
Three principle genes of HIV
HIV contains 9 major genes that encode structural, enzymatic, regulatory, and accessory proteins
Three principle genes: Gag (structural), Pol (enzymatic), Env (envelope)
•Regulatory proteins: Tat, Rev
•Accessory proteins: Vpu, Vpr, Vif, Nef
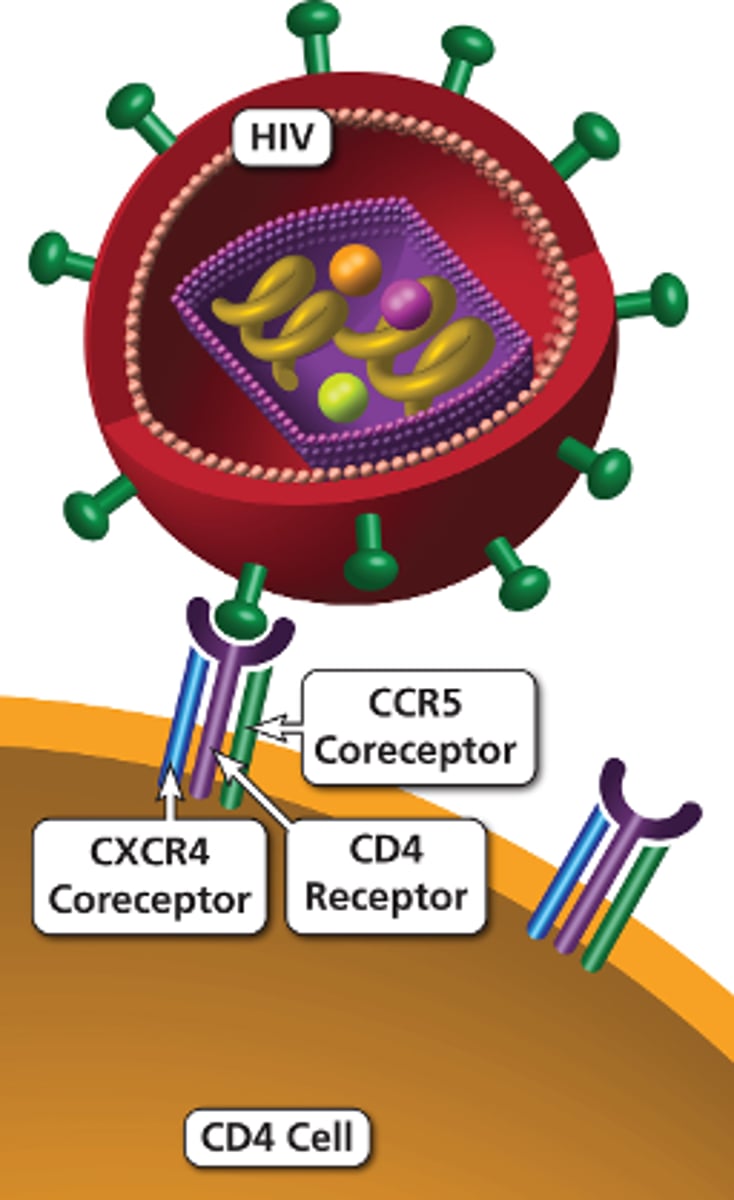
HIV Viral Entry
HIV gains access to its target cells via viral proteins w/ receptors on cell membrane
gp120 binds with high affinity to the CD4+ receptor (which normally fxns as co-R in activation of helper T cells)
CD4+ binding induces a conformational change in gp120, exposing its co-receptor binding sites on the host cell surface
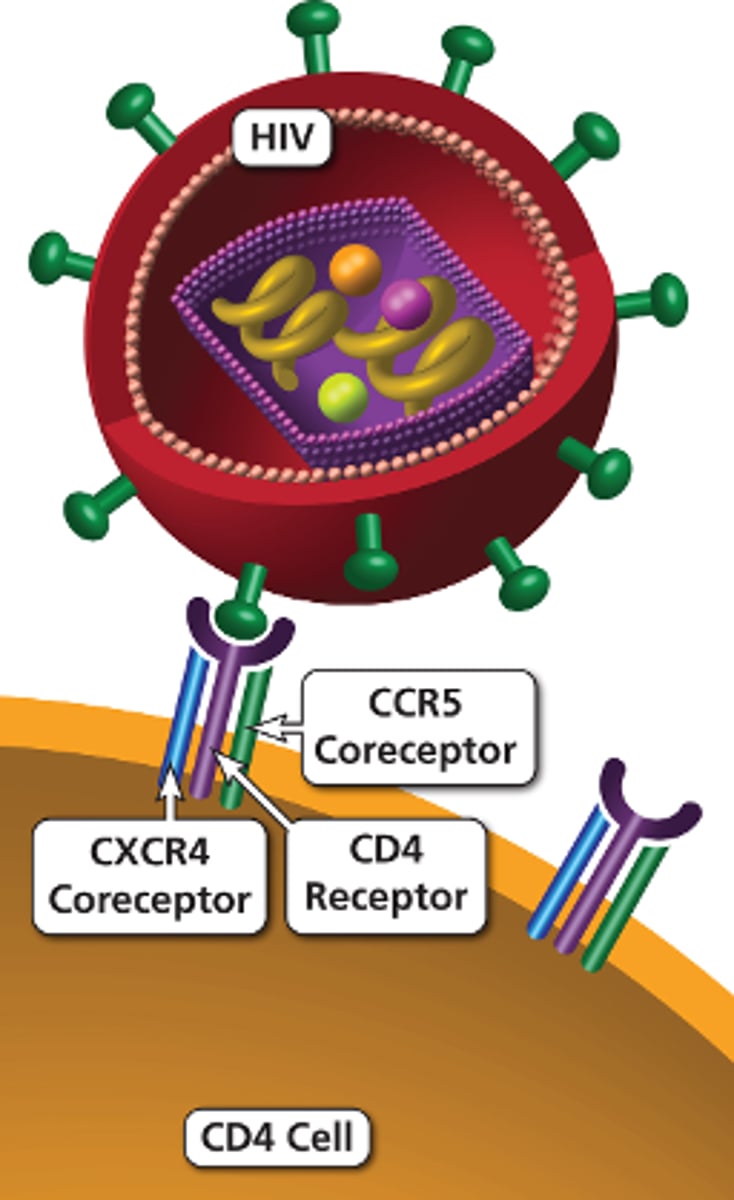
CD4+ binding induces a conformational change in gp120, exposing its co-receptor binding sites on the host cell surface... what are they?
Either CCR5 or CXCR4
Viral Entry - Binding of gp120 to the coreceptor exposes?
Binding of gp120 to the coreceptor exposes the fusion domain of gp41
gp41 then inserts its hydrophobic peptide into the target cell membrane
fusion - HIV viral entry
gp41 inserts its hydrophobic peptide into the target cell membrane
this then forms a pore through which the viral capsid enters
this process is known as fusion
Reverse Transcription and Integration
‣After fusion, viral disassembly occurs before reverse transcription can take place
‣RNA must undergo reverse transcription into DS-DNA and integrate into host genome
‣Reverse transcription begins when the viral RNA is released into the cytoplasm and un-coats
‣Reverse transcriptase (RT) then produces DS-DNA from the viral RNA template
‣The newly synthesized viral DNA then integrates into the hosts DNA via integrase (IN)
Viral Production
‣Once integrated into host DNA, viral genome can remain latent or undergo active expression
•Active expression is dependent on cellular and viral factors that activate viral promoters
•In active infection, viral DNA is first transcribed into mRNA which then make viral regulatory proteins
‣Gag protein mediates assembly of progeny virions by packing genomic RNA within viral particles
‣Finally, HIV protease (PR) catalyzes the cleavage of the gag-pol precursor protein (p55) yielding structural proteins that form the mature virion
‣Assembly of mature virus occurs at the cell membrane and the viral particles exit via budding
•Budding occurs in lipid raft areas along the cell membrane
HIV life cycle
1. Binding and entry
–gp120 and gp41 bind to CD4+ cell receptors
–HIV membrane fuses with the CD4+ cell membrane
2. Reverse transcription via reverse transcriptase enzyme
3. Integration
–Viral enzyme integrase inserts the viral DNA into the CD4+ cell’s DNA
4. Replication
5. Budding
6. Maturation
–HIV protease enzyme cuts the long HIV proteins of the virus into smaller functional units which then reassemble to form a mature virus
What 2 glycoproteins are found within the envelope of the HIV virus?
gp120 and gp41
What gene encodes for the enzymes reverse transcriptase, protease, and integrase?
Pol gene
Can you be infected with HIV without having AIDS?
Yes
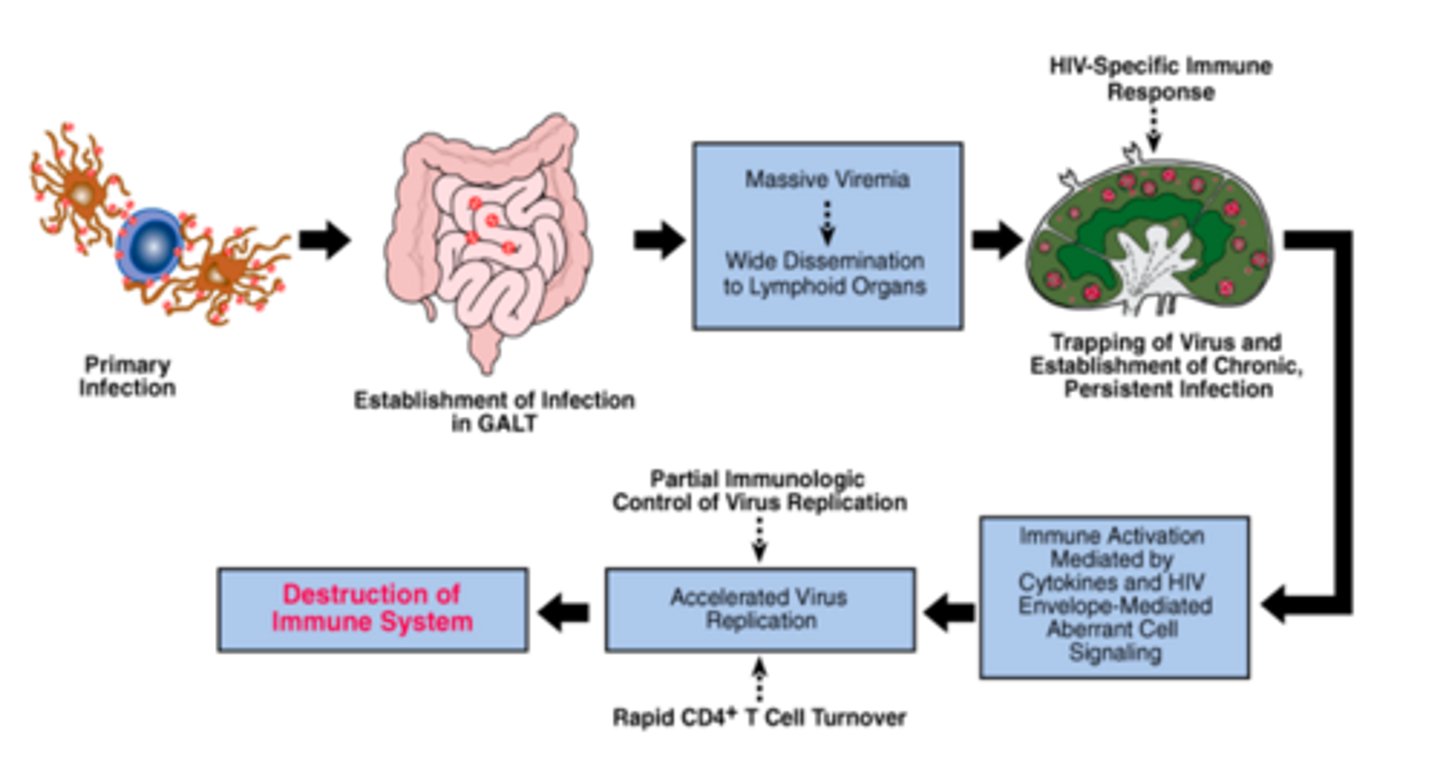
Stages of HIV infection
Viral transmission
Acute HIV infection
•Also called primary HIV infection or acute retroviral syndrome (ARS; bit outdated term but still used)
Chronic HIV infection
• Without AIDS
• With AIDS
–Absolute CD4+ count <200 cells/microL or presence of an AIDS-defining condition
HIV infection is usually acquired through?
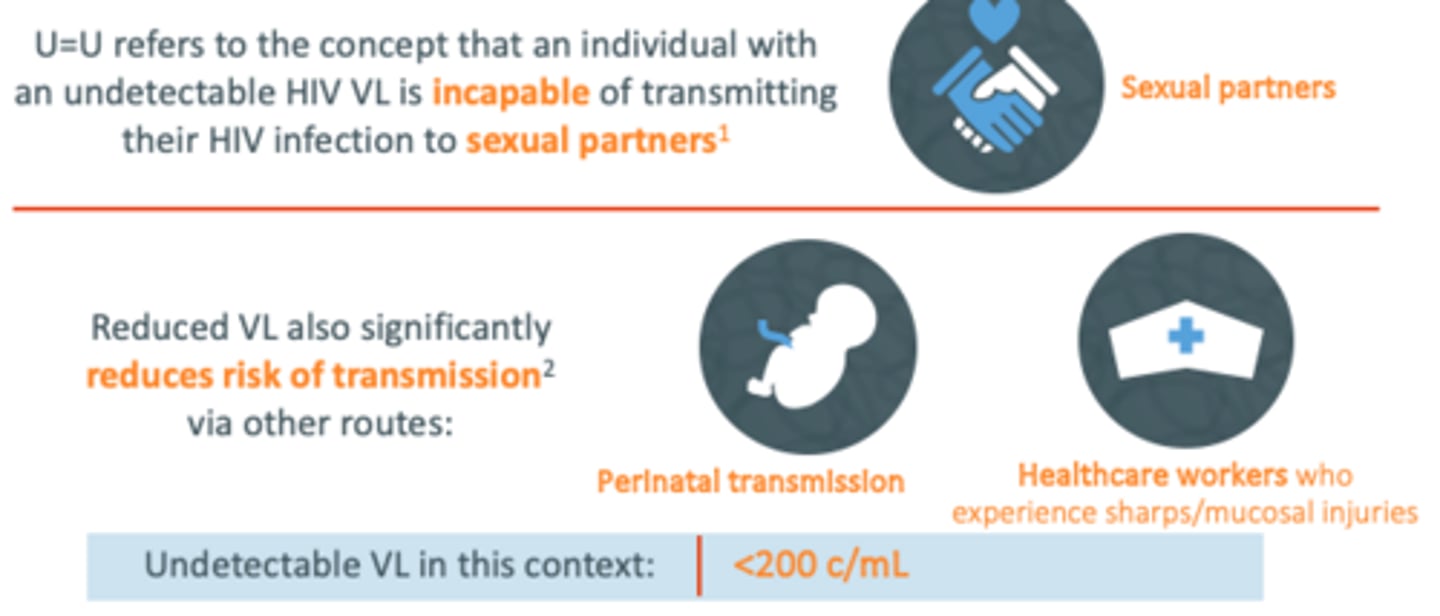
sexual intercourse, exposure to infected blood, or perinatal transmission
For all modes of transmission, a ______ viral load in the source individual living with HIV is associated with a ________ risk of transmission
For all modes of transmission, a higher viral load in the source individual living with HIV is associated with a greater risk of transmission
The risk of HIV transmission is higher during acute infection
Exposures that lead to mucosal disruption and bleeding are associated with higher risk than other exposures. Example of this?
Unprotected receptive anal intercourse conveys the greatest probability of sexual transmission of HIV
Concurrent_____ have been long known to increase the risk of both acquiring and transmitting HIV infection
Why?
STI's
•Why? Damage to mucus membranes allows for easier viral transmission
•STI such as herpes and syphilis can cause sores or ulcers on mucous membranes
Acute HIV Infection
time? benefit to early recognition?
6 month period from date of HIV acquisition
• Period of rapid viral replication
Benefit to early recognition: early antiretroviral therapy (ART) initiation!
Acute HIV Infection
Characterized by?
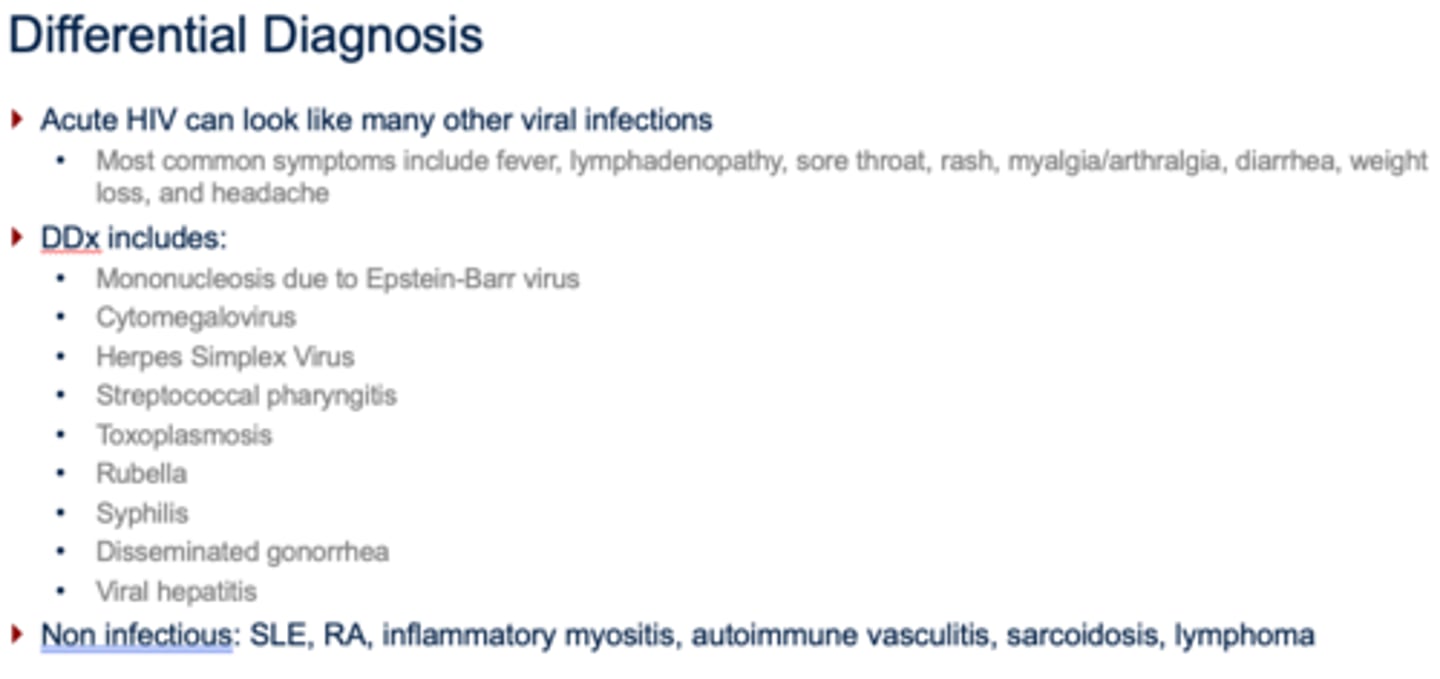
Characterized by fever, lymphadenopathy, sore throat, oral ulcers, rash, myalgia / arthralgia, diarrhea, and headache
•40-90% of patients will be symptomatic
•Commonly missed by medical professionals
‣High index of suspicion is critical

Acute HIV Infection
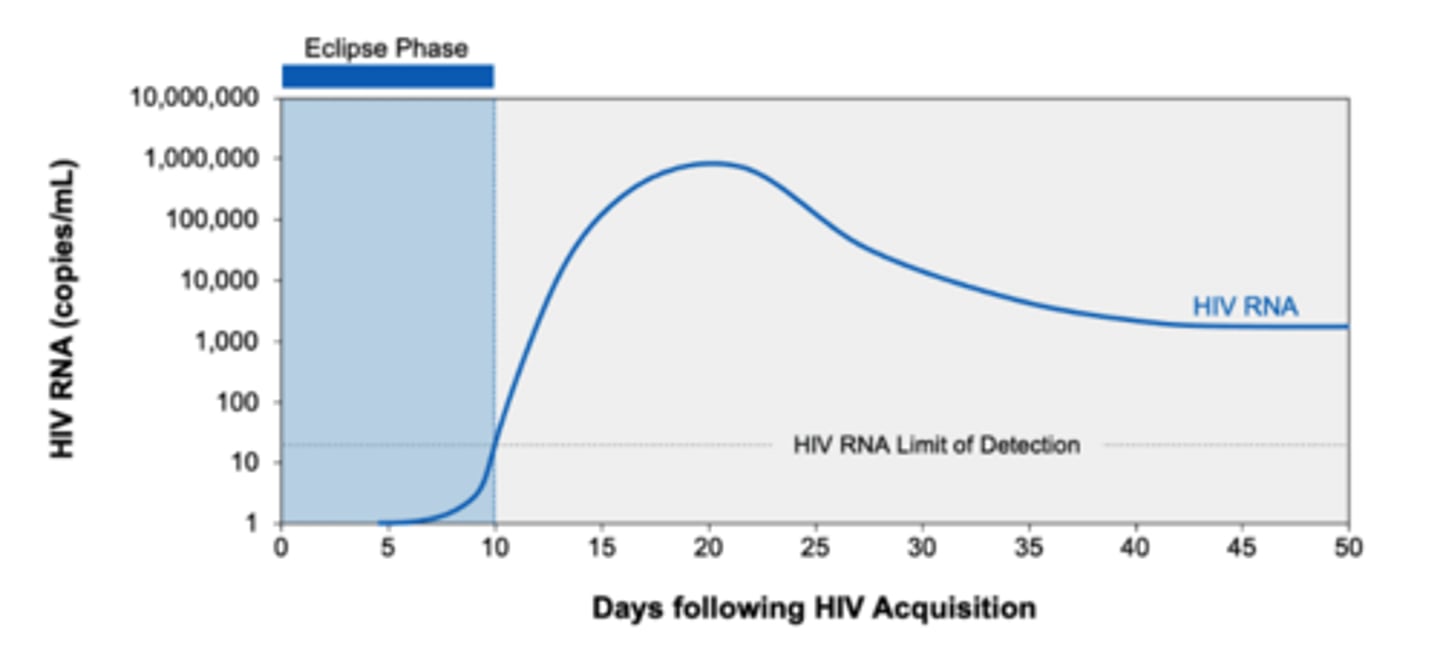
‣Plasma viral RNA level is typically ______
‣Plasma viral RNA level is typically very high
‣Seroconversion refers to?
‣Plasma viremia reaches a steady-state level by?
‣Seroconversion refers to the development of detectable antibodies against HIV antigens
‣Plasma viremia reaches a steady-state level by ~6 months
Chronic HIV Infection without AIDS
‣Characterized by relative stability of viremia and progressive decline in CD4+
‣Mostly ASX, but some might have non specific sx such as fatigue, sweats, or weight loss
‣Decline in CD4+ typically slow with considerable variation in rate of decline (months to years)
Chronic HIV Infection with AIDS
defined as?
survival?
AIDS is an outcome of chronic uncontrolled HIV infection
Defined as CD4+ <200 cells/microL or the presence of any AIDS-defining condition
In the absence of effective ART, the median survival of patients with advanced HIV infection (CD4+ <50 cells/microL) is 12-18 months
when does patient no longer have AIDS
Once CD4+ >200 cells/microL with ART and no AIDS-defining conditions present, patient no longer has AIDS
HIV Controllers (rare)
• ≤0.5% can maintain very low or undetectable levels of HIV RNA in the absence of ART
• These individuals may also maintain high CD4+ cell counts
• Those without detectable virus by standard assays are referred to as "non-viremic" or "elite" controllers
• Whether or not to start ART in HIV or elite controllers remains controversial
Routine Screening for HIV
CDC recommends HIV testing for everyone 13-64 at least once as part of routine health care
For higher risk individuals, CDC recommends testing at least annually:
•MSM with sexual partners who are HIV-infected or w/ unknown HIV status
- More frequent testing (q3-6 months) may be beneficial in this population
•PWID
•Persons who exchange sex for money or drugs
•Sex partners of persons who are HIV-infected/bisexual/inject drugs
•Persons who have sex with partners whose HIV status is unknown
•Anyone on PrEP (more on this later)
Early identification of HIV infection is important
•Initiate preventive care measures
•Reduce HIV transmission through reductions in viral load
•Change HIV risk behaviors
•Cost effective as demonstrated in multiple studies
~15% of HIV-infected individuals in the US are unaware of their status. Undiagnosed infections are responsible for majority of HIV transmissions.
DDX
T or F: HIV can be transmitted through saliva?
FALSE
A CD4+ count below what number indicates AIDS?
CD4+ count <200 cells/microL
T or F: people who smoke marijuana should be screened for HIV more frequently.
FALSE
People who inject drugs should be.
Establishing a Diagnosis of HIV
Clinicians should have a LOW threshold to suspect HIV infection given the wide range of symptoms
•When in doubt, check HIV screen!
Diagnosis is established by the detection of HIV virus in the blood
Establishing a Diagnosis of HIV
Two buckets of testing to consider:
•Screening tests
–Antibody only testing
–Combination HIV antigen and antibody testing
•Confirmatory tests
–HIV-1/HIV-2 differentiation assay
–Western blot
–Viral load
Screening Tests: Antibody (Ab)-only tests
ELISA can be used as an initial screen test
Detect presence of HIV-1 and HIV-2 antibodies as early as 3 weeks after viral exposure
More sensitive than rapid Ab tests
Positive test should be confirmed with HIV-1/HIV-2 differentiation assay*
Screening Tests: Combination Ag/Ab tests
MOST COMMONLY USED
Fourth-generation tests detect both HIV Ab and HIV p24 Ag
•Sensitivity and specificity near 100% (chronic HIV infection)
–Not as sensitive as HIV RNA testing
•These tests are able to identify acute/early infection in up to 80% of patients whose HIV dx would have been missed by Ab-only testing
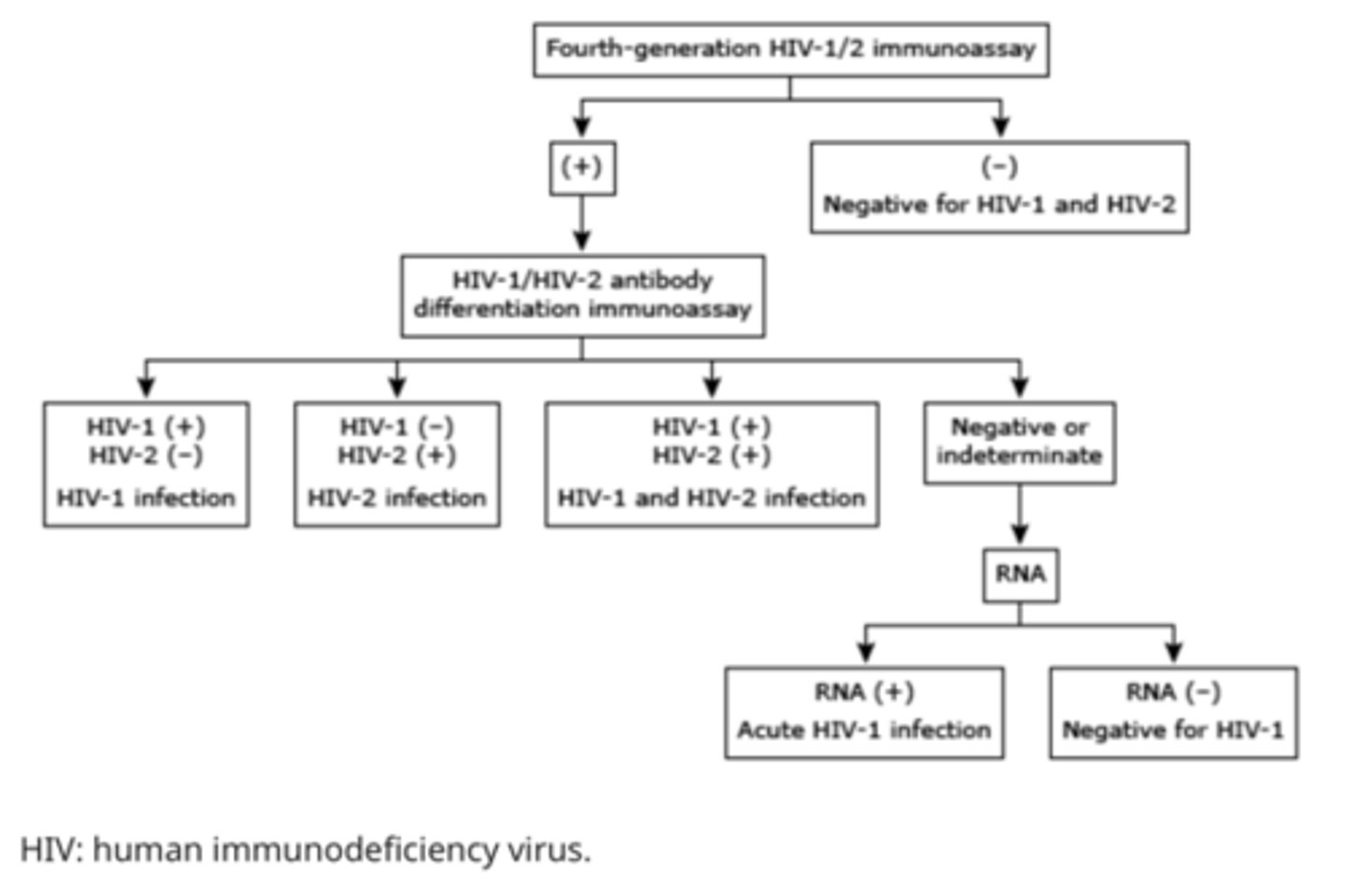
HIV-1/HIV-2 differentiation assay
Rapid laboratory-based test
•Used to confirm a positive fourth-generation test and to distinguish between HIV-1 and HIV-2 infection
•Turnaround time (TAT) is generally <20 minutes
•Preferred confirmatory test
Western blot (less utilized)
•Historically performed on +ELISA to exclude the possibility of a false-positive screening test
•Detects IgG antibody to HIV-1
– Can take up to 2 months after HIV acquisition for the test to turn fully positive
•Special HIV-2 Western blot must be requested if considering HIV-2 infection
•Most labs in US have ceased offering Western Blot testing
eclipse phase of HIV
HIV-1 begins to replicate in mucosa almost immediately after exposure; 7-21 days
NO HIV TEST IS POSITIVE DURING THIS PHASE
pathway for HIV screening
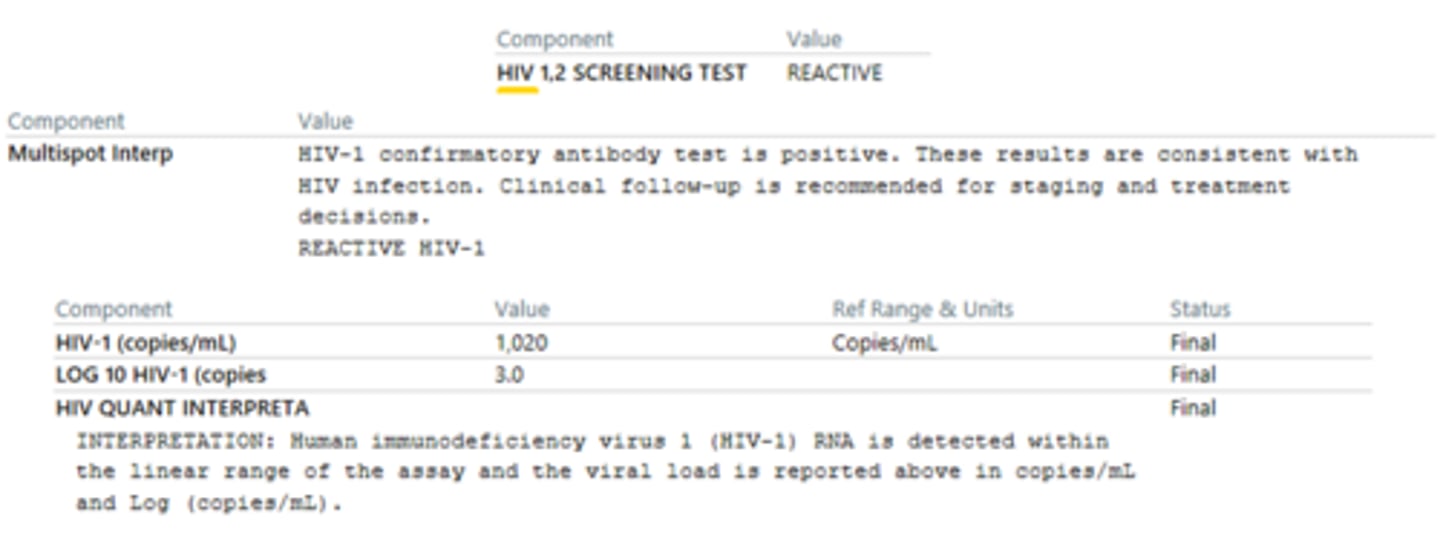
Example of HIV infected
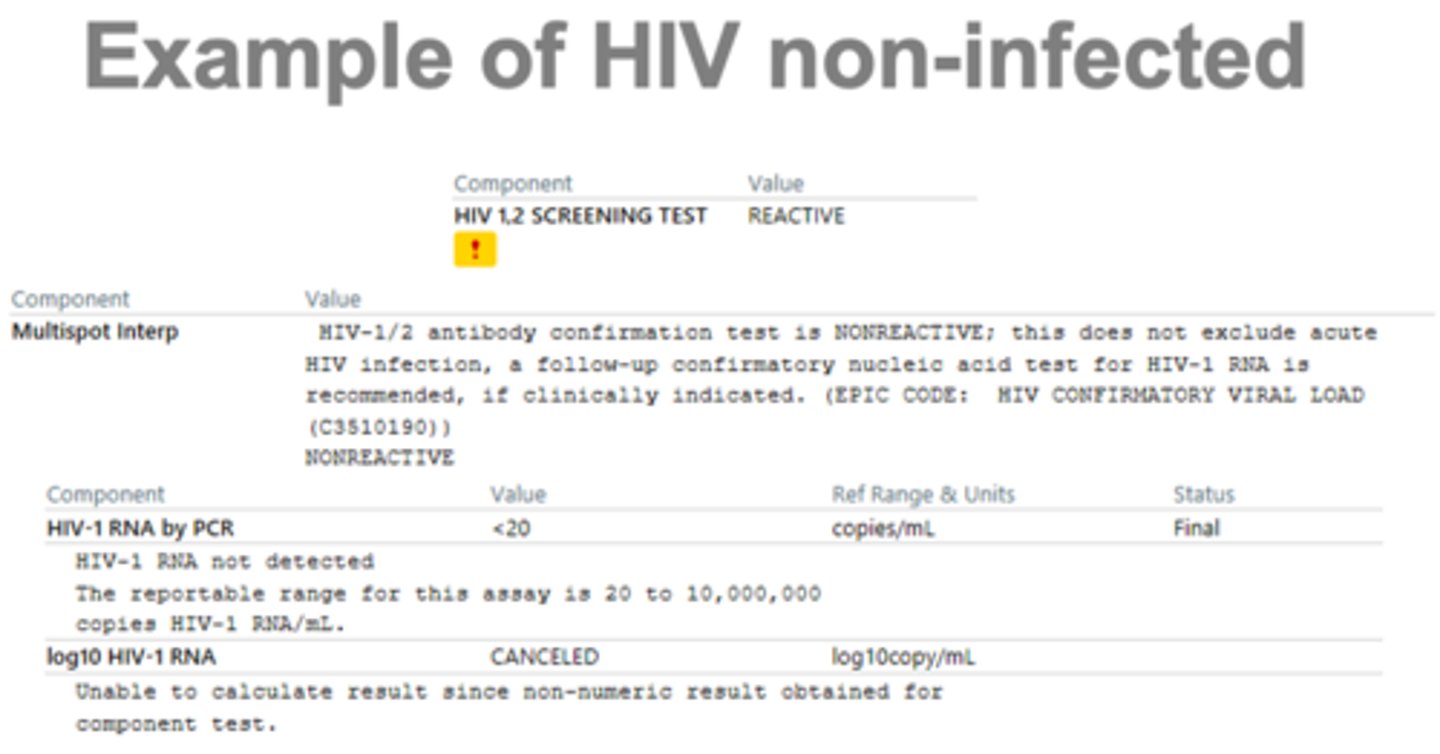
HIV non-infected example
can check viral load prior to the screeners when REALLY concerned.
when in doubt you can check it (but still try to follow step wise approach)
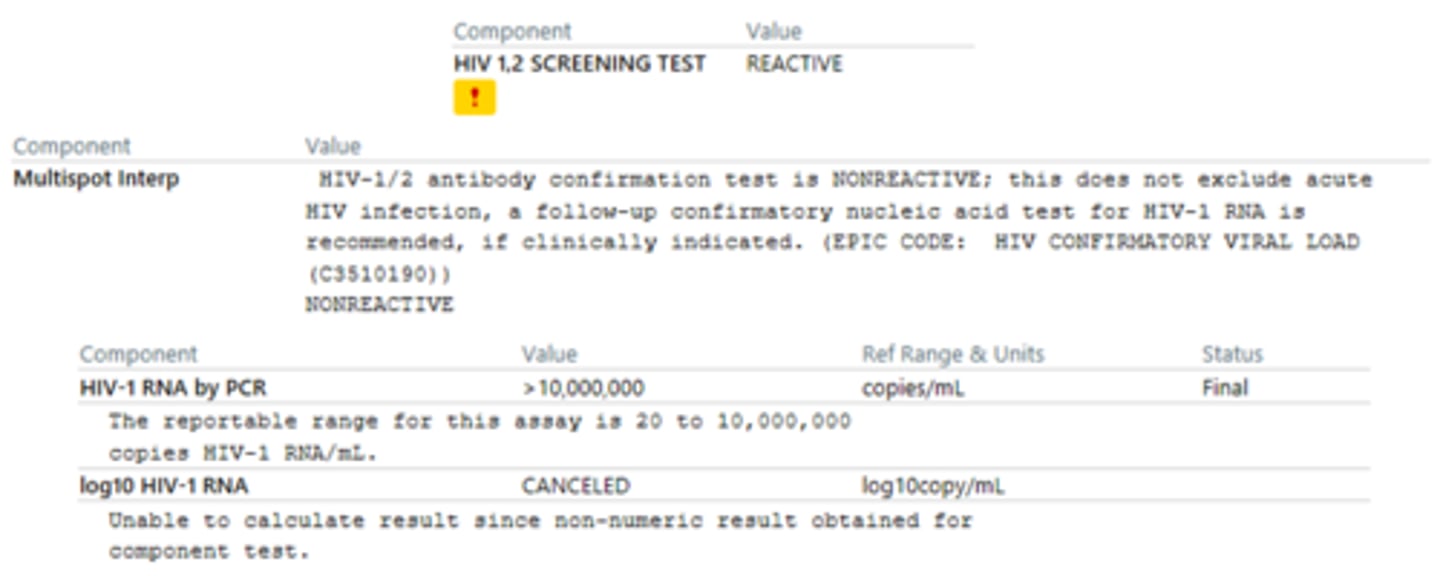
Example of HIV infected (acute infection)
viral load confirms dx
too early for high Ab development
Consent to Test in Pennsylvania?
•Written informed consent is no longer required for an HIV test
•Tests may now be offered in an “opt-out” format–HIV test will be given unless the patient specifically declines this
Negative tests results no longer need to be given in person, positive tests results still must be given in person
resistance testing
HIV susceptibility testing to guide therapy leads to better viral suppression
Genotypic assays are by far the most common resistance testing you will order as a PA.... detect the presence of specific drug resistance mutations
Obtain genotype testing for?
•On any treatment naïve patient
•On any PrEP patient who seroconverts
•On any patient who has fallen out of care/stopped taking ART for many months
•On any patient with an increasing viral load despite ART adherence
Resistance Testing: Genotype assays
•Require a viral load of at least 500-1,000 copies/mL
•Standard tests frequently include testing for NRTI’s, NNRTI’s, and PI resistance
• Assessing for integrase inhibitor resistance must be requested separately (though this is rare)
Resistance Testing: Phenotype assays
Most useful for complicated patients with multidrug resistant virus
Resistance Testing: Always look back at old genotypes in a treatment-experienced patient... why?
Once ART is discontinued, wild-type (WT) virus will reemerge to replace the drug-resistant virus
–Why? Mutations make virus less effective at replicating. In the presence of ART, resistant virus has a survival advantage. In the absence of ART, WT virus can outcompete resistant virus.
Absence of a detectable resistance mutation must be interpreted with caution in a patient who has recently discontinued ART ... consider proviral DNA assay test
Phenotype assays will always include a ______
Phenotype assays will always include a genotype
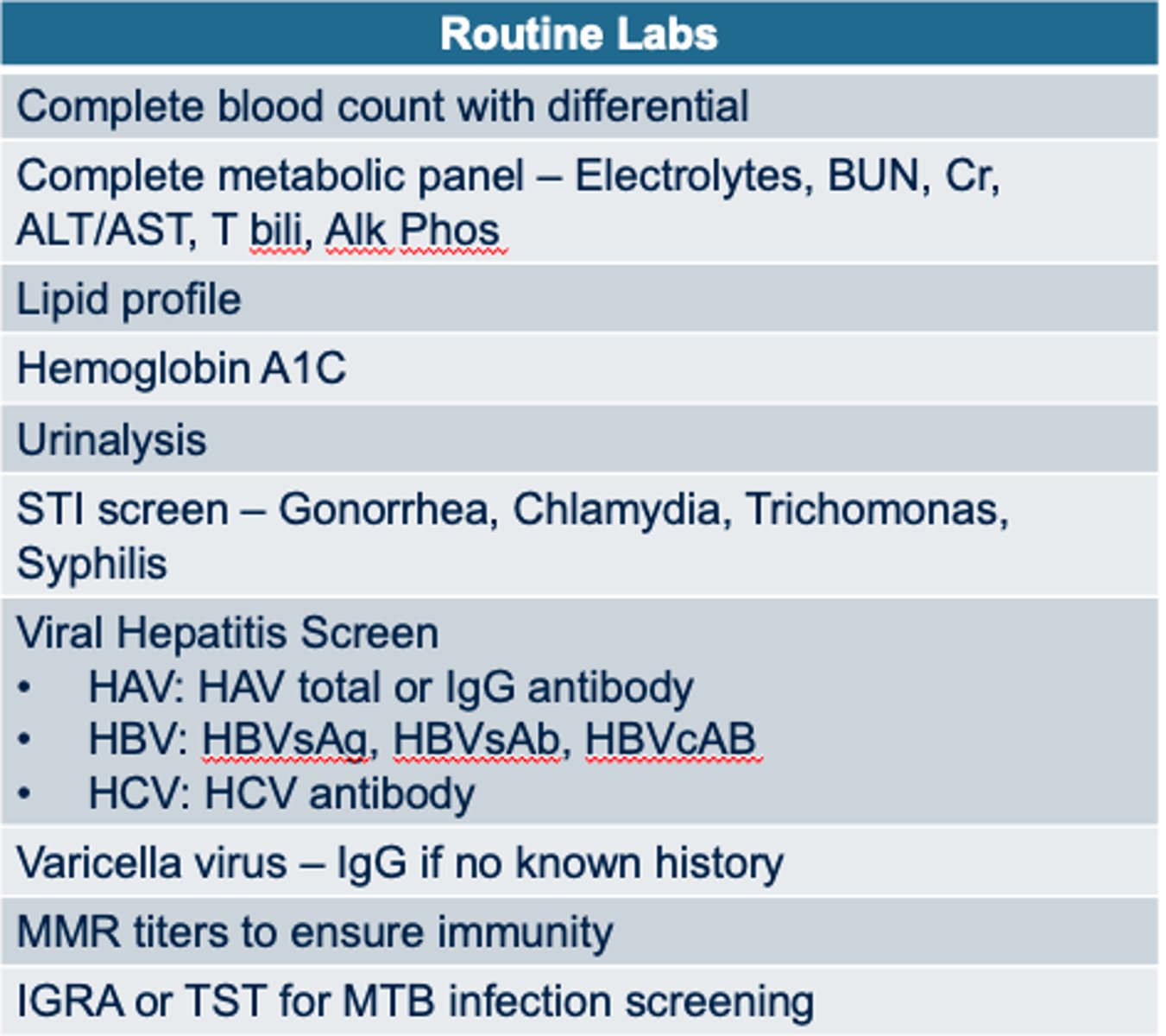
Baseline laboratory evaluation for ALL patients
HIV Specific Labs and Routine
HIV antigen/antibody screening test
CD4 count and percentage
HIV viral load
HIV resistance testing (INSTI recommended if suspicion for INSTI mutation transmission)
Tropism assay* (if CCR5 antagonist)
HLA B5701* (if abacavir)
routine labs in image
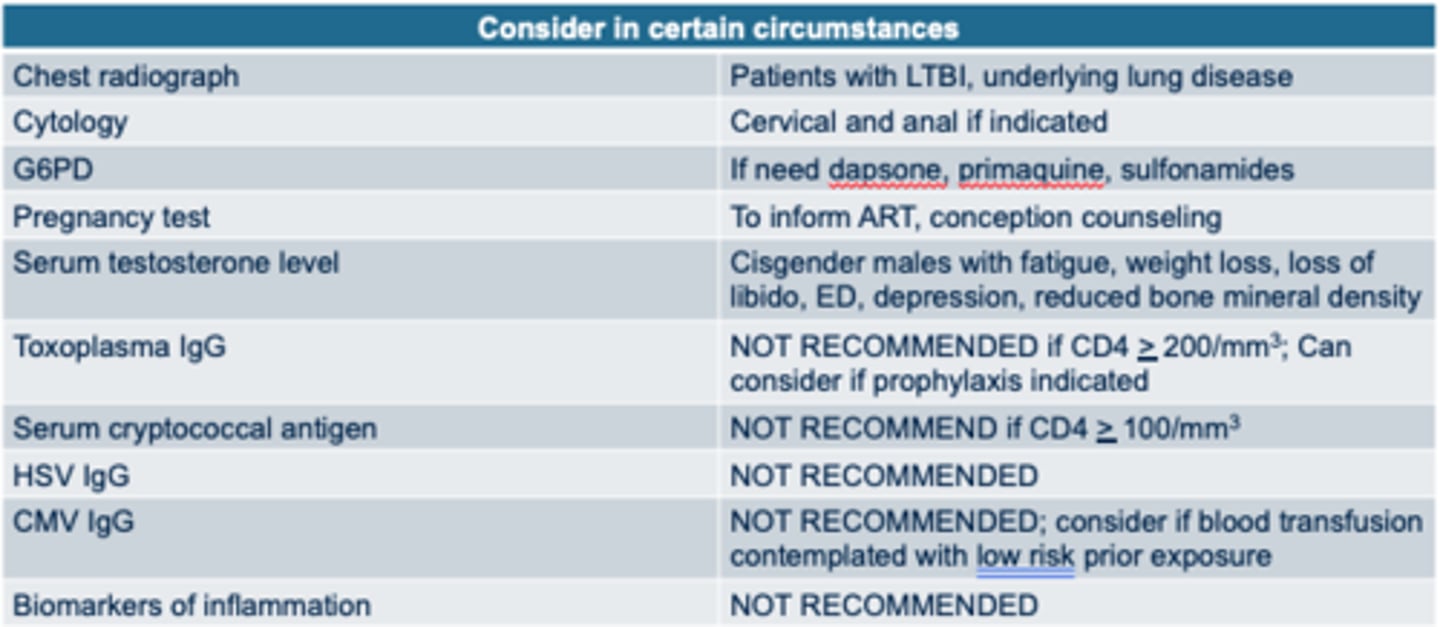
Tests that may be performed under certain circumstances
Follow up lab monitoring with what 2 labs
•HIV viral load
•CD4+ cell count
HIV viral load lab
- 2-4 weeks after initiation of ART (no longer than 8 weeks)
- q4-8 weeks until viral suppression, then
- q3-4 months for first 2 years
- q6 months in patients with stable CD4 and viral suppression for at least 2 years
CD4+ cell count lab
-q 3-6 months for the first 2 years of starting ART, if viremia develops or CD4+ < 300
-q 12 months if CD4+ 300-500 and viral suppression for at least 2 years
-Optional if CD4+ > 500 and viral suppression for at least 2 years
If a patient is overwhelmed, it’s OKAY to delay?
bloodwork, pharmacy consultations, and social/case management visits until the patient has had time to process
‣Remember to remain patient, calm, empathetic, and non-judgmental when delivering a new positive result
‣Allow open communication and collaborative decision making
‣Help patients modify behaviors that lead to poor retention in HIV care
If a fourth generation test is positive and subsequent antibody testing is indeterminate/negative, what should your next test be?
HIV viral load
In PA, do I need to obtain written consent prior to HIV testing?
No
T or F: HIV phenotype testing should be performed for every treatment naïve patient.
False
GENOTYPE = YES
When to Start ART
‣As soon as possible! NEED TO START MEDS as early as possible. multiple drugs often.
‣Concern for initiating ART during early infection is suboptimal adherence leading to resistance
• no clinical evidence that resistance is more likely in pts tx during early HIV infection than with long-est dz
The benefits to the individual and to public health outweigh the possible drawbacks of earlier ART
such as?
-Reduction on symptomatic disease
-Improved clinical markers of disease
-Decreased risk of transmission
-Decreased viral reservoir and improved markers of immune cell function
Immune Reconstitution Inflammatory Syndrome (IRIS)
inflammatory disorders associated w/ paradoxical worsening of preexisting infectious processes after starting antiretroviral therapy
sx usually develop within 1 week to a few months after the initiation of ART
likelihood and severity of IRIS correlates with 2 factors:
•The extent of CD4+ immune suppression prior to the initiation of ART
•The degree of viral suppression and immune recovery following the initiation of ART
Treatment Goals of HIV
‣Maximum and durable viral suppression to prevent resistance, tx failure, and opportunistic infections
‣Restoration/preservation of immune system
‣Reduction of HIV morbidity/mortality
‣Improvement in QoL
‣Prevent transmission of HIV transmission
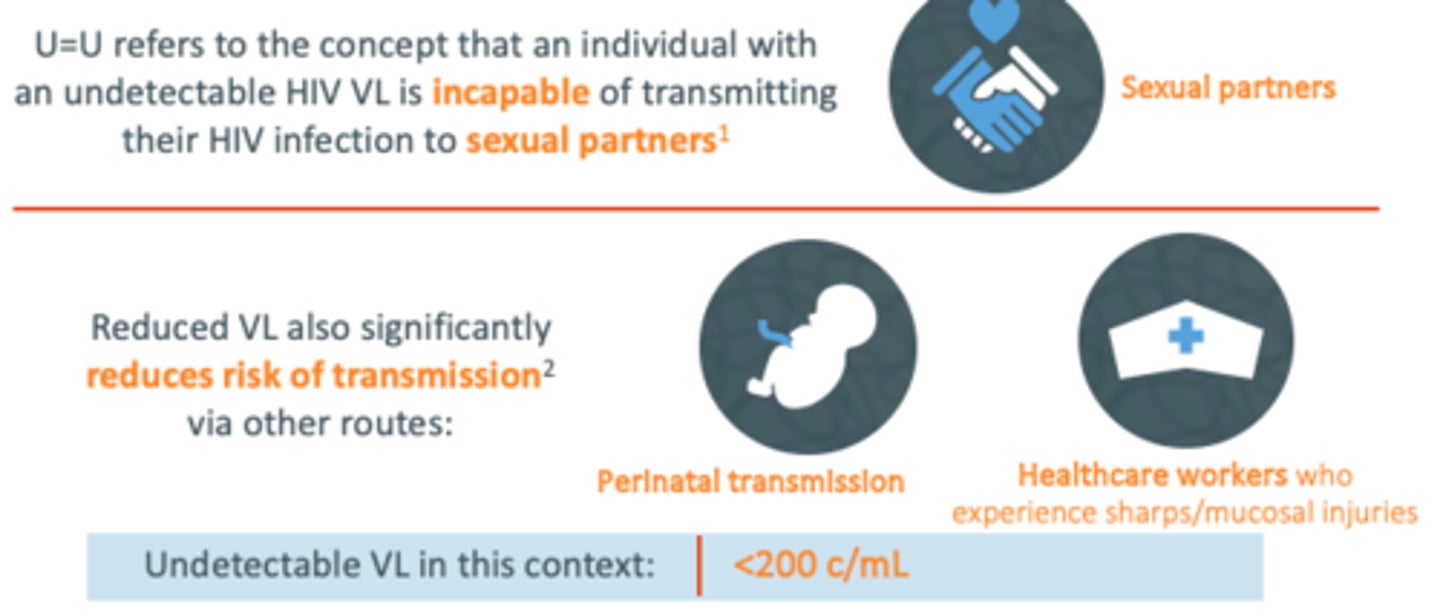
U = U
Undetectable = Untransmittable
goal!!
Undetectable VL in this context: <200c/mL
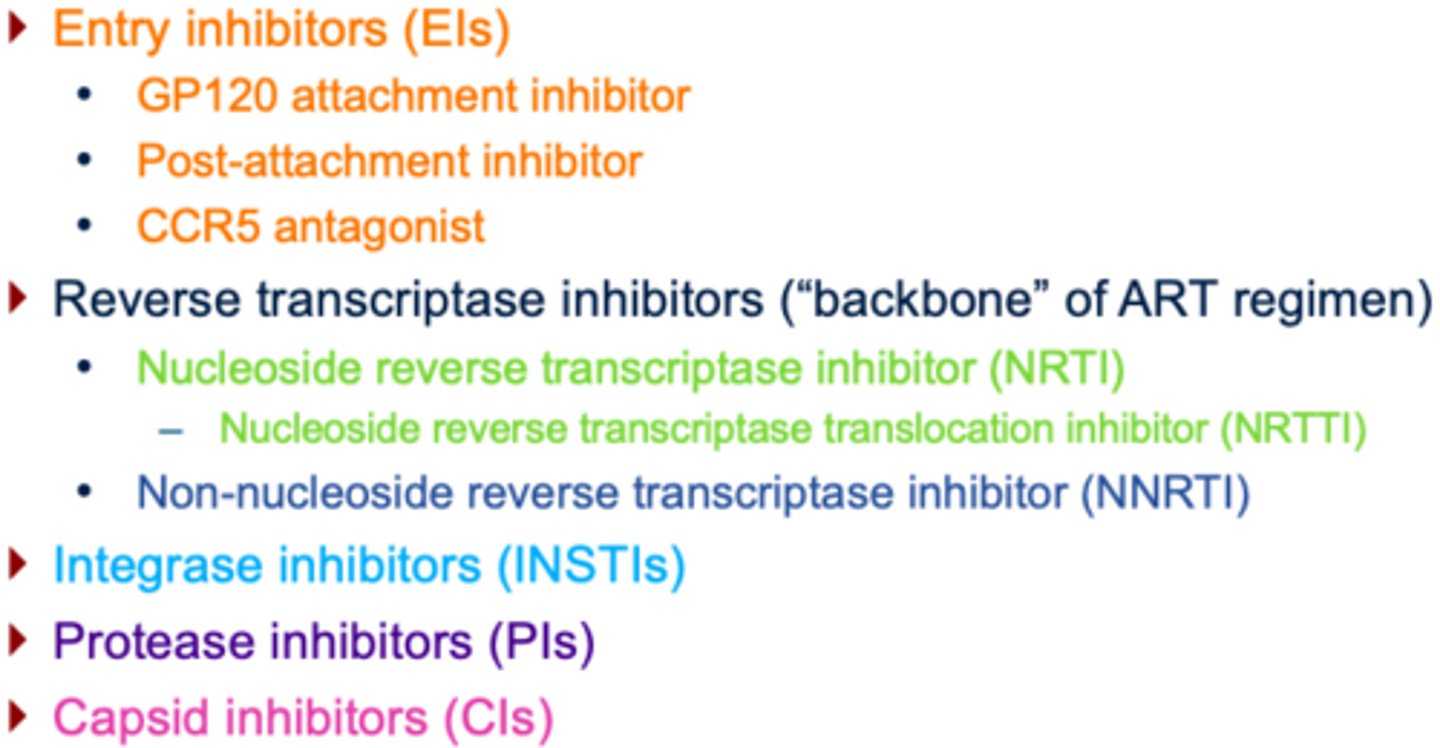
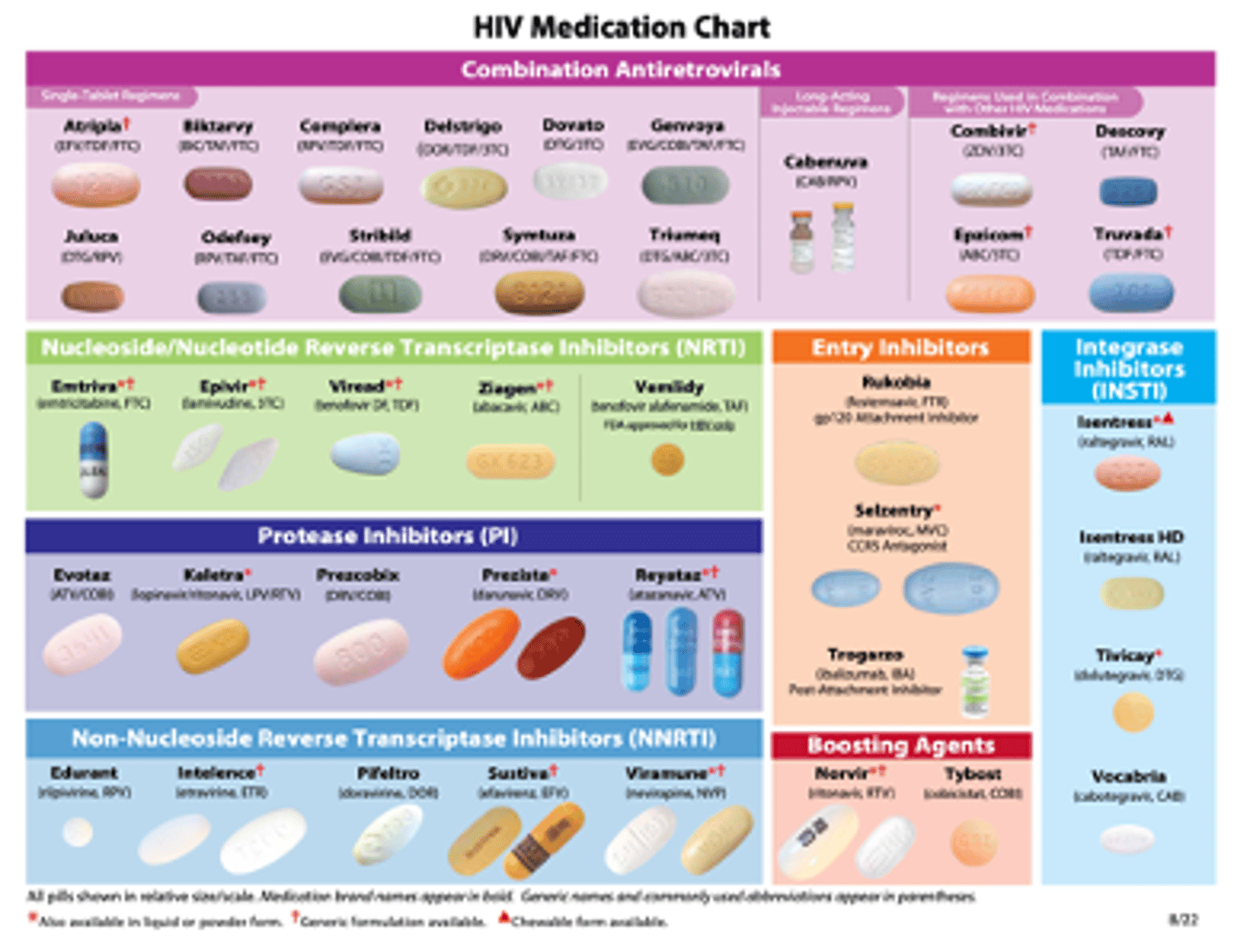
Classes of ART
HIV Regimen Basics
Each drug: generic, brand, and 3 letter name
•Ex. BIC/TAF/FTC (Biktarvy)
Most HIV regimens contain 3 active HIV drugs
•2NRTI + other class
•Exceptions
–A few regimens only use 2 drugs
–Protease inhibitors require boosters
Drug Abbreviations
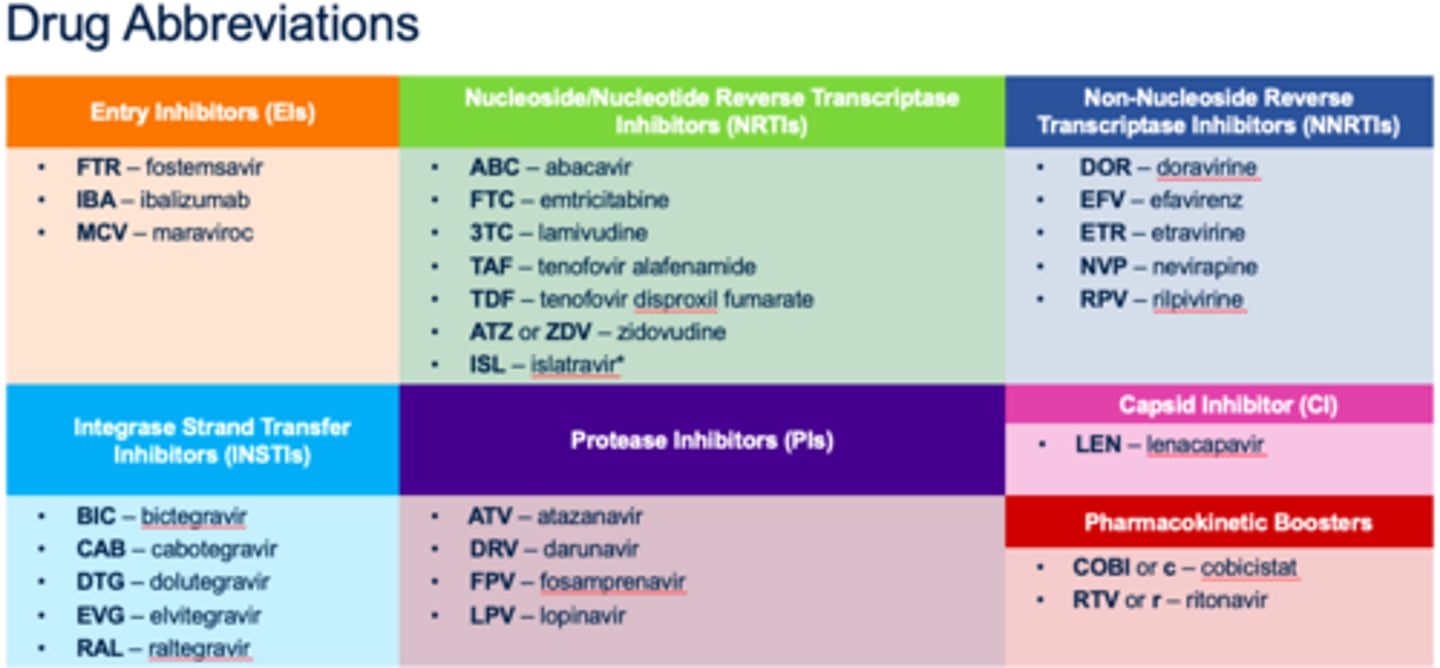
NRTIs
In general, very well tolerated with few drug interactions
BBW: lactic acidosis
NNRTIs
•Typically end in –virines
•CYP3A4 inducers (except rilpivirine and doravirine); rash and hepatotoxicity; cross-resistance within generations, but not necessarily between
INSTIs
•Typically end in –tegravir
•In general, well tolerated; AE’s include HA, weight gain, elevation in CK
PIs
•Typically end in –navir
•Need to be boosted with Cobicistat or low dose ritonavir
•AE’s include hyperlipidemia, insulin resistance, lipodystrophy, and elevated LFTs
most common drug used for treatment of HIV?
Biktarvy! (INSTI + 2 NRTIs)
3 drug regimens are most common starting off
HIV Dual therapy
benefits, efficacy?
•Benefits: fewer long-term toxicities and DDIs, better tolerability, financial cost
•Fewer number of drugs must achieve same efficacy as triple therapy
•Must block same number of intracellular sites (2) in HIV replication cycle
•High level of efficacy without resistance

When NOT to switch to dual therapy:
•Pregnancy
•HBV co-infection
•Evidence of drug resistance
Idvynso (doravirine/islatravir)
First non-INSTI, tenofovir-free, 2-drug regimen
‣For virologically suppressed PLWH with:
1.No history of virologic treatment failure and
2.No known resistance substitutions to doravirine
‣Non-inferior efficacy compared to Biktarvy in a head-to-head phase 3 trial
‣Available as of 5/11/26
**brand new
What NOT To Start
Single drug monotherapy
2 NNRTIs, 2 PIs, or 2 INSTIs together
Triple NRTI therapy
Emtricitabine (FTC) + lamivudine (3TC)
Un-boosted darunavir
Confirming Complete Regimen: Triple Therapy
•Nucleoside/tide backbone (2 nucleoside analogs)
–PLUS
•Anchor drug
–Integrase inhibitor or
–Protease inhibitor (boosted) or
–Non nucleoside reverse transcriptase inhibitor
BIKTARVY
BIC (INSTI)
FTC (NRTI)
TAF (NRTI)

Use a __________ ART regimen for patients who have chronic hepatitis B virus (HBV) infection
Use a tenofovir-containing ART regimen for patients who have chronic hepatitis B virus (HBV) infection
Avoid _______ and _________ containing regimens for patients with impaired kidney function
Avoid TDF and atazanavir (PI) containing regimens for patients with impaired kidney function
Limited data regarding preferred ART regimen for patients on hemodialysis; _________ can be used (administer after dialysis on dialysis days)
Biktarvy can be used
What class of ART are considered the "backbone" of a regimen?
Reverse transcriptase inhibitors
Name two classes of ART commonly used in first line regimens.
NRTI, INSTI
A ____ containing regimen should be used with co-HBV infection?
Tenofovir
Long Term Prognosis -Most patients who remain virologically suppressed can live a ?
• Live a near-normal lifespan
•This is IMPORTANT and key to remind patients who feel like HIV is a “death sentence”
also important to note:
‣Significant disparities in mortality and life expectancy exist based on sex/gender, race/ethnicity, transmission category, and other demographic variables
‣In the absence of effective ART, medial survival of patients with advanced HIV infection is 12-18 months
Non-Infectious HIV Complications
‣Weight loss
‣Increased susceptibility to cardiovascular/metabolic disease
‣HIV-associated dementia and neurocognitive disorders
‣HIV-related peripheral nervous system disease
‣HIV-related osteopenia/osteoporosis
‣Non-infectious oral disease
•Oral hairy leukoplakia
•Aphthous ulcers
HIV Wasting Syndrome
•Progressive and unintentional weight loss of more than 10% of body weight
•Often accompanied by chronic diarrhea or weakness
•Can occur despite adequate food intake
•Often due to metabolic disturbances, malabsorption, or chronic inflammation
Lipodystrophy
Abnormal fat redistribution
-Lipoatrophy in the face, arms, and legs or
-Lipohypertrophy in abdomen, neck (buffalo hump), or breasts
Increased Susceptibility to Cardiovascular/Metabolic Disease
such as
‣Atherosclerosis and CVD
‣Metabolic Syndrome
‣Increased risk of stroke
HIV-Associated Neurocognitive Disorder (HAND)
•Spectrum ranging from asx neurocognitive impairment (ANI) to mild neurocognitive disorder (MND) and HIV-associated dementia (HAD)
-Cognitive Impairment
-Motor Symptoms
-Behavioral Changes
HIV-Associated Dementia (HAD)
In most severe form, HAD characterized by marked cognitive, motor, and behavioral dysfunction, including confusion, memory loss, and severe motor deficits
Distal symmetric polyneuropathy (DSP)
Most common form of HIV-associated neuropathy
–Burning or tingling sensation in the feet and hands, progressing proximally
–Numbness and weakness sensory loss may affect balance and coordination; muscle weakness in advanced cases
Inflammatory demyelinating polyneuropathy
Resembles Guillain-Barré syndrome, rapid onset of muscle weakness and sensory loss