fluids electrolytes acid-base - lecture 16 FIRST LECTURE FOR EXAM 3
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
fluid amount
volume
fluid intake:
1100-1400 mL
fluid output:
1200-1500 mL (u/o)
100-200 mL (stool)
intake should equal output
concentration
osmolarity
mOsm/kg H2O:
285-295
# of particles/kg of total body water
solvent - water
solute - electrolytes
composition
electrolyte concentration
sodium 136-145 - brain
potassium 3.5-5.0 - heart
calcium 9.0-10.5
magnesium 1.3-2.1
pH
degree of acidity
blood pH 7.35-7.45
O2 saturation:
95%-100% - relative to comorbidity
PaCO2 35-45 - lungs, works immediately, acidic
HCO3 21-28 - kidneys, Alkalotic
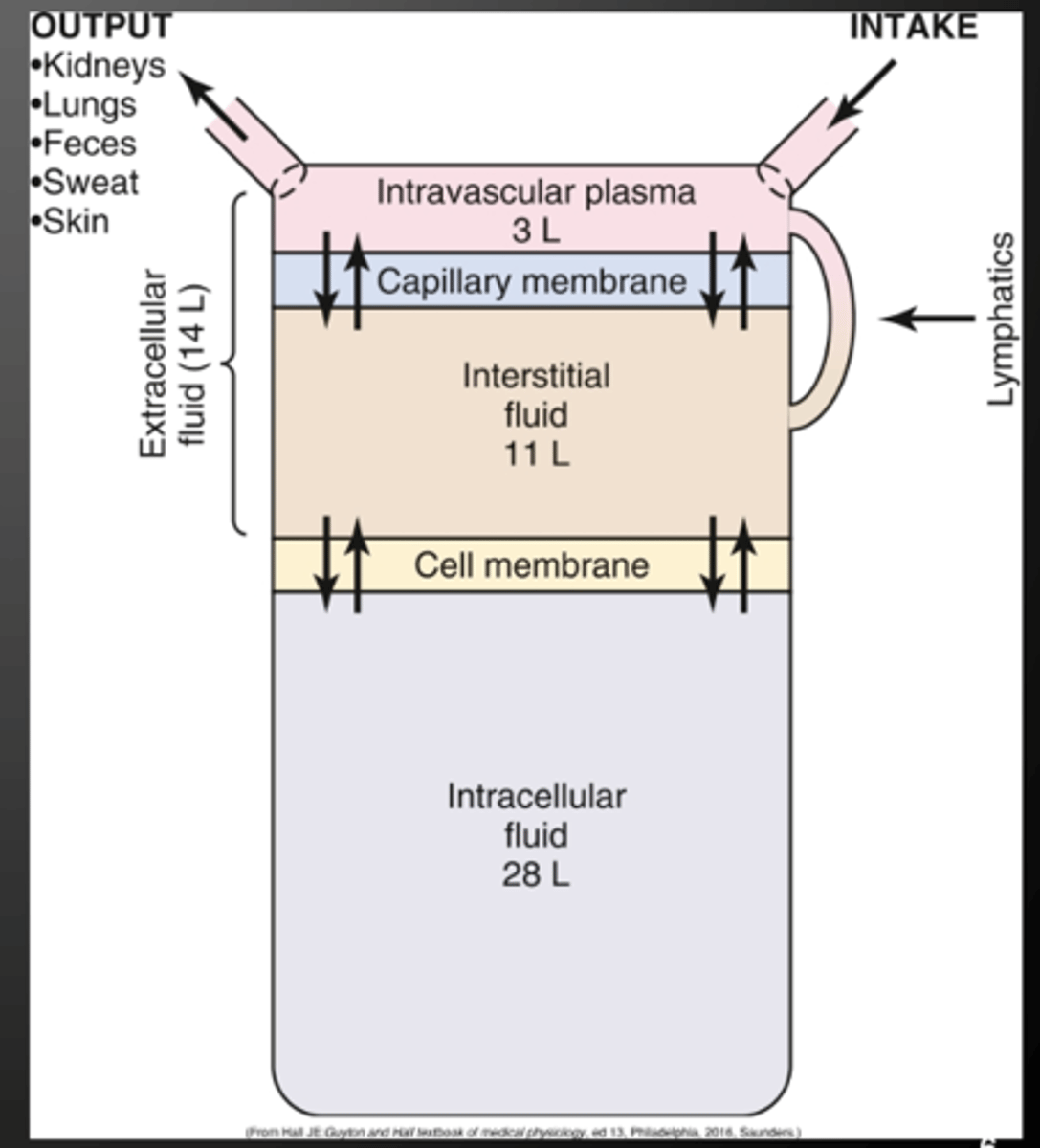
what are the two types of fluid distribution
Intracellular fluid (2/3 of total body water; major electrolyte is potassium)
Extracellular fluid (1/3 total body water; major electrolyte is sodium)
what are the composition of body fluids
Osmolality - number of particles per kg of water (285-295)
Isotonic (285-295)
-- Hypotonic (<285)
-- Hypertonic (>295)
isotonic solution
fluid with the same tonicity as blood (285-295)
dextrose 5% in water (D5W)
0.9% NaCl (NS)
Lactated Ringer (LR)
no shift change
NS + NS = STILL ISOTONIC - DONT GET THIS WRONG
hypotonic + isotonic = HYPERTONIC
hypotonic solution - swell
fluid is more dilute than blood (<285)
0.225% NaCl (1/4 NS)
0.45% NaCl (1/2 NS)
shift to intracellular space = swelling
hypertonic solution - shrink
more concentrated than blood (>295)
dextrose 10% in water (D10W)
dextrose 5% in LR (D5LR)
3% NaCl
5% NaCl
Dextrose 5% in 0.45% NaCl
Dextrose 5% in 0.9% NaCl
shift to extracellular = shrink
osmosis
movement of water from area of lower concentration to area of higher concentration
ex: red blood cells and plasma
active transport
movement of water from area of lower concentration to area of higher concentration with use of energy (ATP)
ex: sodium/potassium pump
diffusion
movement of electrolytes from higher concentration to lower concentration
ex: gas exchange in the lungs
filtration
movement of fluid in and out of the capillaries by way of hydrostatic pressure (pushing force) and oncotic pressure (pulling force)
ex: capillary filtration, glomerular filtration
can a patient with crackles and edema be dehydrated ?
YES
Fluid balance depends upon dynamic interplay, and it's based on fluid intake, absorption, distribution, and output. To maintain homeostasis, ....
fluid intake must equal fluid output.
Average Intake
2200-2700 mL/day
Fluids ingested
Foods (insensible w/solids)
Metabolism (insensible)
Average Output:
2200-2700 mL/day
Skin and sweat (insensible)
Lungs (insensible)
Gastrointestinal (loose stool only)
Urine
oral intake
water, juice, milk, tea, coffee, soup, broth, soft drinks, ensure, boost
ice chips (measured as half the volume of melted liquid ex: 1 cup of ice = 1/2 cup of water)
liquid oral medication
enteral (tube feeding) intake
tube feed formula, water flushes before/after feeding
medications administered via tube (if liquid)
intravenous (IV) fluids
IV maintenance, medication drips, blood transfusion, TPN
IV medication drips (antibiotics, pain meds)
other sources of intake
dialysis fluids (if retained)
irrigation fluids (if absorbed)
enema fluids count !!!!!!
why do we give ice chips?
to decrease fluid intake
urine output
foley catheter, urinal, bed pan, or bedside commode
gastrointestinal (GI) losses
vomitus (emesis), nasogastric (NG) tube drainage
fecal output (especially if diarrhea or from an ostomy bag) - loose stool
surgical drains
jackson-pratt (JP) drain, hemovac drain, chest tube drainage, wound vac output
negative pressure will increase blood flow
other body fluid losses
excessive bleeding (if measurable ex: from a wound or surgical site)
dialysis fluid removal
how do we calculate? what are the conversions we should know?
1kg = 2.2 lbs.
1000 mL = 1L
1L=1kg
Daily weights
an important indicator of fluid status. Fluid gains or losses indicate changes in the amount of total body fluid, usually ECF, but do not indicate shift between body compartments. Weigh patients with heart failure and those who are at high risk for or actually have ECV excess daily.
also useful for patients with clinical dehydration or other causes or risks for ECV deficit.
Have the patient void and weigh the patient at the same time each day with the same scale.
Sodium: 135-145
Hypernatremia:
1. decreased LOC
2. Coma
3. Lethargy
4. Confusion
5. Seizures
info:
- hypertonic solution
- water deprivation
- more sodium than water
- diabetes insipidus - - peeing but hold in the sodium
TREAT:
1. DRINK WATER
2. DILAYSIS - ESRD
3. IV hypotonic solution - ICU
Hyponatremia:
1. Decreased LOC
2. Coma
3. Lethargy
4. Confusion
5. Seizures
info:
- too little particles but lots of water
TREAT:
1. oral (salt, crackers)
2. DIALYSIS - ESRD
3. IV hypertonic solution - ICU
Potassium: 3.5-5
Hyperkalemia:
1. muscle weakness
2. abdominal cramps
3. diarrhea
4. cardiac arrest
5. dysrhythmias
info:
- spironolactone causes this
TREAT:
FUROSEMIDE/LASEX - NUMBER 1
ESRD - dialysis
Diabetic Ketoacidosis - insulin
Hypokalemia:
1. muscle weakness
2. abdominal cramps
3. constipation
4. dysrhythmias
info:
- excessive vomiting
-diarrhea
TREAT:
spironolactone
potassium tablets
IV mg sulfate to absorb K+
DISCONTINUE WHAT IS CAUSING THE ISSUE
Magnesium: 1.3-2.1
Hypermagnesemia:
1. Lethary
2. Hypoactive DTRs
3. Bradycardia
4. Hypotension
info:
laxatives/antacids/ESRD cause this
DTR - deep tendon reflexes
TREAT:
furosemide/lasex
IV calcium gluconate to help with Mg go to other cells
Hypomagnesemia:
1. + chvostek sign
2. hyperactive DTRs
3. muscle cramps
4. tetany
5. dysphagia
6. insomnia
calcium: 9-10.5
hypercalcemia:
1. decreased LOC
2. constipation
3. fatigue
4. cardiac arrest
5. personality change
info:
cause: immobility, osteoporosis, ESRD
TREAT:
Loop Diuretic
hypocalcemia:
1. + chovestek sign
2. numbness
3. tingling
4. laryngospasms
5. dysrhythmias
info:
cause: vitamin D deficiency
TREAT:
1. give vitamin D - orange juice
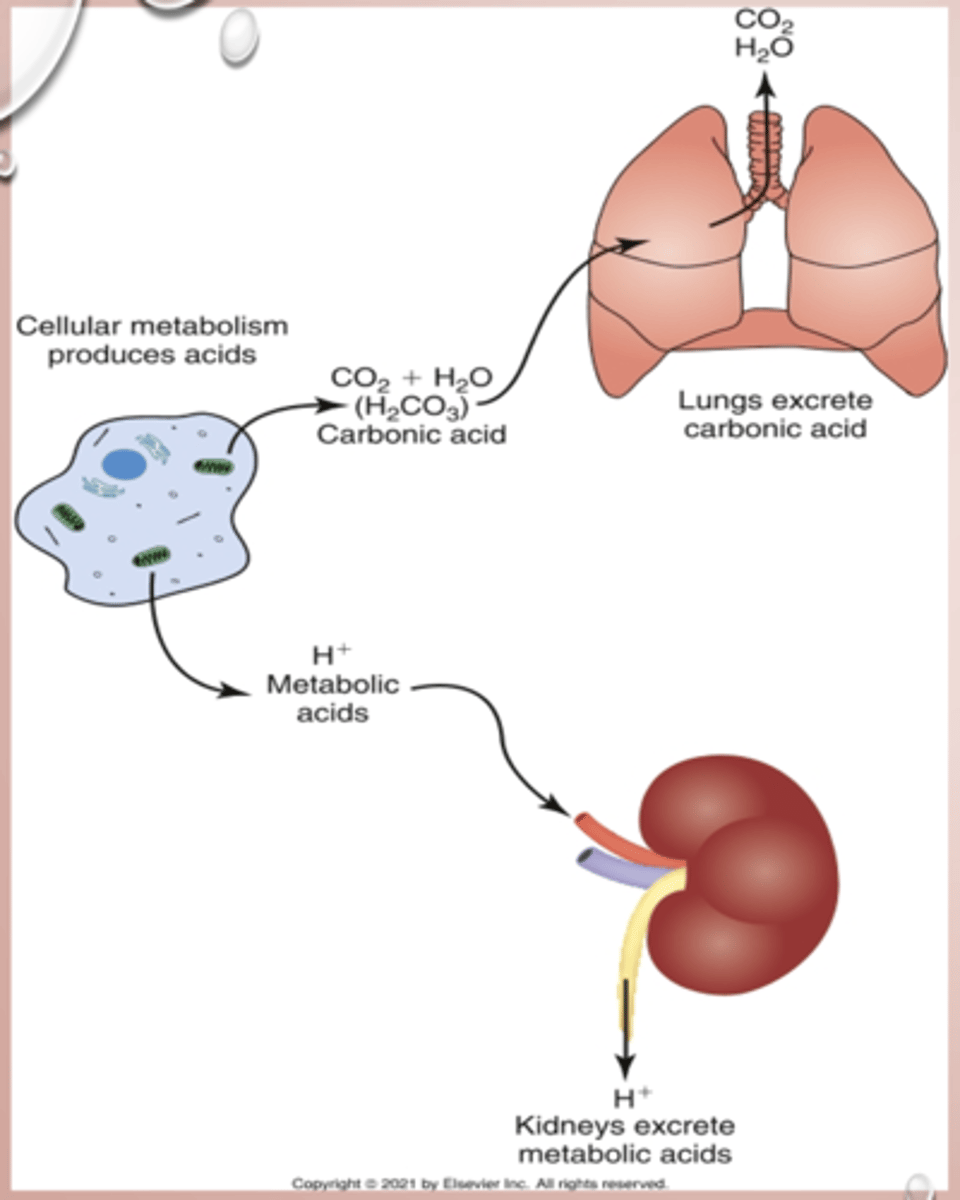
acid base balance
respiratory acidosis - lungs/PaCO2
s/s: light headedness, decreased loc, dysrhythmias
Cause: hypoventilation (COPD, bacterial pneumonia, airway obstruction, respiratory muscle fatigue, drug overdose
Treatment: Encourage deep breathing, oxygen therapy, mechanical ventilation (last resort)
respiratory alkalosis - lungs/PaCO2
s/s: Light headedness, decreased loc, dysrhythmias
Cause: hyperventilation (anxiety, psychological distress, head injury, aspirin overdose, meningitis)
Treatment: Encourage paper-bag breathing, relaxation, oxygen therapy, mechanical ventilation (last resort)
metabolic acidosis - kidneys
s/s: decreased loc, dysrhythmias, abdominal pain
Cause: ketoacidosis, circulatory shock, burns, severe infection, ingestion of acid, ESRD
Treatment: iv fluids, oxygen therapy, oral sodium bicarb, dialysis,
metabolic alkalosis - kidney
s/s: decreased loc, dysrhythmias, abdominal pain
Cause: massive blood transfusion, administration of sodium bicarb
Treatment: iv fluids, IV POTASSIUM, IV ACETALZOLAMIDE, dialysis
what are some lab studies to assess for imbalances
1. Complete blood count (cbc) - RBC, hematocrit
2. Comprehensive Metabolic Panel - Na, K
3. Serum electrolytes, blood urea nitrogen, and creatinine levels - kidneys, GFR <15 = ESRD
4. Urine pH and specific gravity - concentration of solute in urine, how well kidney is filtering urine
5. Arterial blood gas (ABG) - both kidneys and lungs
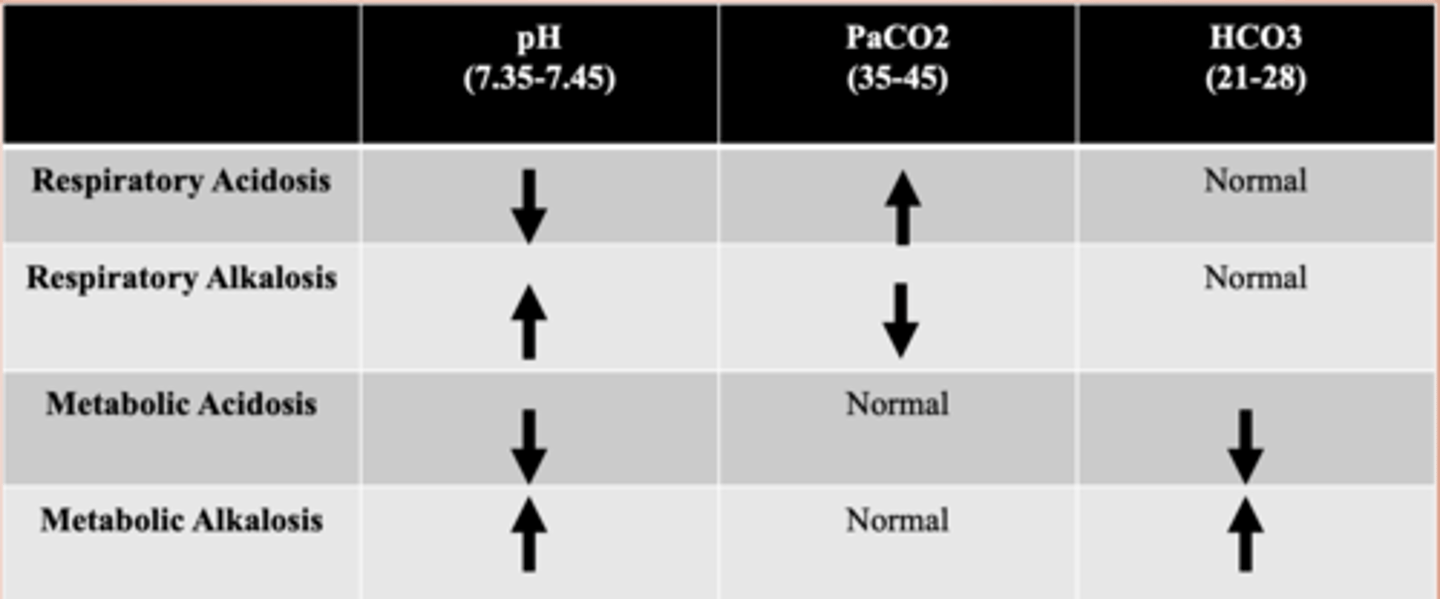
arterial blood gas
respiratory acidosis: PaCO2/Low pH
respiratory alkalosis: PaCO2/High pH
metabolic acidosis: Kidneys/Low pH/Normal PaCO2
metabolic alkalosis: Kidneys/High pH/Normal PaCO2
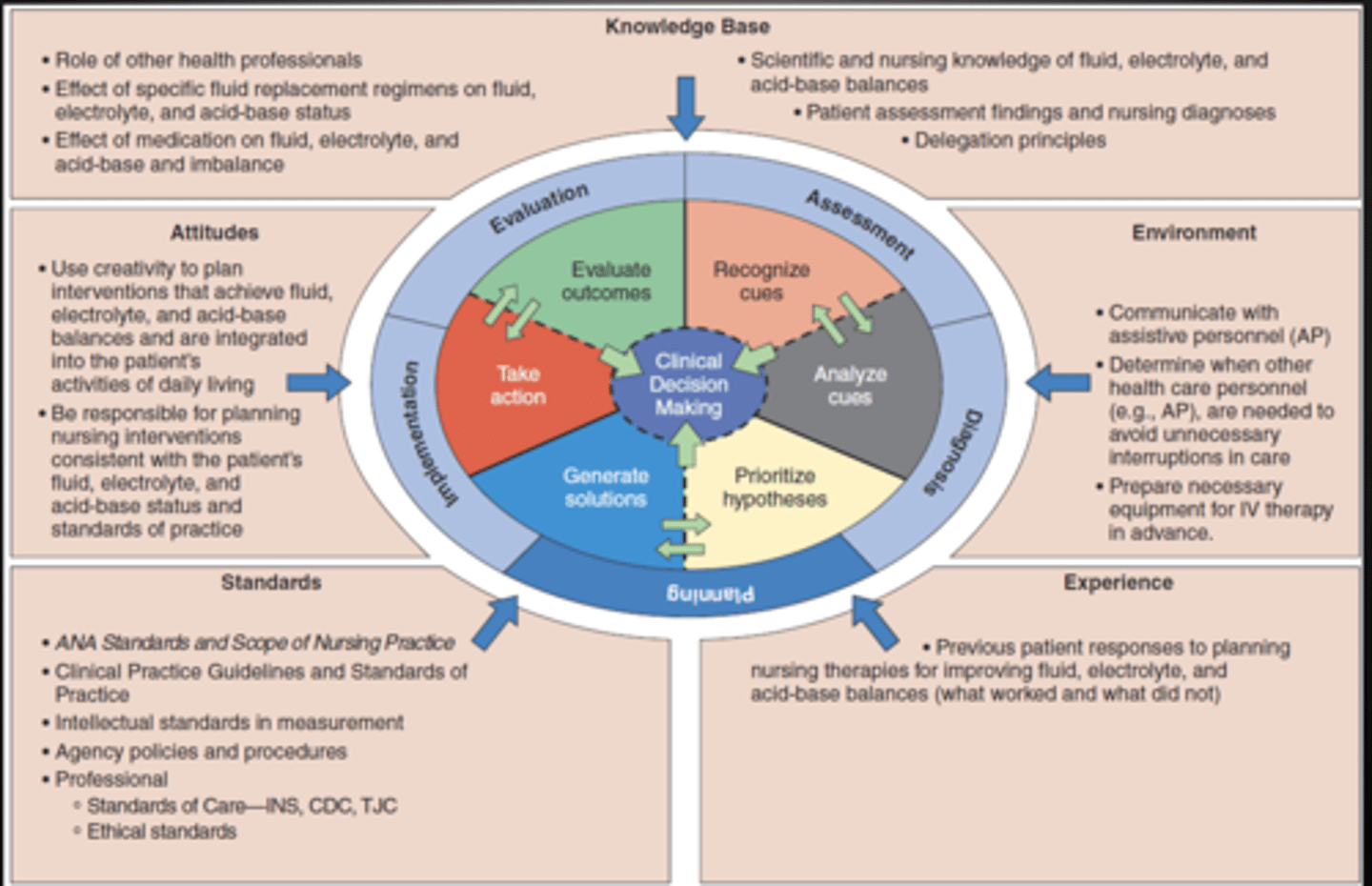
A walk through the Nursing process
Ms. Dorothy is a 65 y/o presenting to the ER with complaints of dizziness, fatigue, shortness of breath, and swelling in her lower extremities. She has been experiencing increased urination over the past 48 hours.
Medical History: Hypertension, Type 2 Diabetes, Chronic Kidney Disease (stage 2)Current
Medications: Lisinopril, Metformin, Furosemide (diuretic)
Vital Signs:
- BP: 140/90 mmHg
- Heart Rate: 98 bpm
- Respiratory Rate: 20 breaths/min
- Temperature: 98.7°F
- O2 Saturation: 94% (on room air)
General Appearance: Pale, fatigued, appears dehydrated, and has mild swelling (edema) in both ankles.
Cardiovascular: Tachycardia, no murmurs.
Respiratory: Shortness of breath with exertion, no wheezing or crackles on auscultation.
Musculoskeletal: Mild weakness in the lower extremities, limited range of motion due to edema.
Abdomen: Soft, non-tender, no distension.
Urine Output: Slightly reduced, dark amber in color.
CBC:
- Hemoglobin: 12.5 g/dL (low-normal)
- Hematocrit: 37% (normal)
Electrolytes:
- Sodium (Na): 132 mEq/L (low)
- Potassium (K): 5.2 mEq/L (elevated)
- Chloride (Cl): 98 mEq/L (normal)
- Bicarbonate (HCO₃): 22 mEq/L (normal)
Renal Function:
- Blood Urea Nitrogen (BUN): 25 mg/dL (elevated)
- Creatinine: 1.5 mg/dL (elevated)
- Glomerular Filtration Rate (GFR): 50 mL/min (stage 2 kidney disease)
Arterial Blood Gases (ABGs):
- pH: 7.25
- PaCO₂: 58 mmHg
- HCO₃: 22 mEq/L
- Capillary blood sugar 320 DG/l
what are the nursing diagnosis?
- Fluid Imbalance
- Dehydration
- Electrolyte imbalance
- Acid Base Imbalance
- Lack of Knowledge of Fluid Regimen
Ms. Dorothy is a 65 y/o presenting to the ER with complaints of dizziness, fatigue, shortness of breath, and swelling in her lower extremities. She has been experiencing increased urination over the past 48 hours.
Medical History: Hypertension, Type 2 Diabetes, Chronic Kidney Disease (stage 2)Current
Medications: Lisinopril, Metformin, Furosemide (diuretic)
Vital Signs:
- BP: 140/90 mmHg
- Heart Rate: 98 bpm
- Respiratory Rate: 20 breaths/min
- Temperature: 98.7°F
- O2 Saturation: 94% (on room air)
General Appearance: Pale, fatigued, appears dehydrated, and has mild swelling (edema) in both ankles.
Cardiovascular: Tachycardia, no murmurs.
Respiratory: Shortness of breath with exertion, no wheezing or crackles on auscultation.
Musculoskeletal: Mild weakness in the lower extremities, limited range of motion due to edema.
Abdomen: Soft, non-tender, no distension.
Urine Output: Slightly reduced, dark amber in color.
CBC:
- Hemoglobin: 12.5 g/dL (low-normal)
- Hematocrit: 37% (normal)
Electrolytes:
- Sodium (Na): 132 mEq/L (low)
- Potassium (K): 5.2 mEq/L (elevated)
- Chloride (Cl): 98 mEq/L (normal)
- Bicarbonate (HCO₃): 22 mEq/L (normal)
Renal Function:
- Blood Urea Nitrogen (BUN): 25 mg/dL (elevated)
- Creatinine: 1.5 mg/dL (elevated)
- Glomerular Filtration Rate (GFR): 50 mL/min (stage 2 kidney disease)
Arterial Blood Gases (ABGs):
- pH: 7.25
- PaCO₂: 58 mmHg
- HCO₃: 22 mEq/L
- Capillary blood sugar 320 DG/l
what are the interventions
- Monitor vital signs frequently, especially blood pressure, heart rate, and respiratory rate.
- Assess urine output and characteristics to monitor for changes in fluid balance.
- Administer fluids as prescribed, considering electrolyte balance and kidney function.
- Monitor serum electrolytes and renal function to assess treatment efficacy and adjust medications as needed.
- Administer medications as ordered (e.g., diuretics, antihypertensives), ensuring proper dosage and patient tolerance.
- Provide education on diet, emphasizing the importance of low-sodium and balanced potassium intake to prevent further electrolyte imbalances.
Ms. Dorothy is a 65 y/o presenting to the ER with complaints of dizziness, fatigue, shortness of breath, and swelling in her lower extremities. She has been experiencing increased urination over the past 48 hours.
Medical History: Hypertension, Type 2 Diabetes, Chronic Kidney Disease (stage 2)Current
Medications: Lisinopril, Metformin, Furosemide (diuretic)
Vital Signs:
- BP: 140/90 mmHg
- Heart Rate: 98 bpm
- Respiratory Rate: 20 breaths/min
- Temperature: 98.7°F
- O2 Saturation: 94% (on room air)
General Appearance: Pale, fatigued, appears dehydrated, and has mild swelling (edema) in both ankles.
Cardiovascular: Tachycardia, no murmurs.
Respiratory: Shortness of breath with exertion, no wheezing or crackles on auscultation.
Musculoskeletal: Mild weakness in the lower extremities, limited range of motion due to edema.
Abdomen: Soft, non-tender, no distension.
Urine Output: Slightly reduced, dark amber in color.
CBC:
- Hemoglobin: 12.5 g/dL (low-normal)
- Hematocrit: 37% (normal)
Electrolytes:
- Sodium (Na): 132 mEq/L (low)
- Potassium (K): 5.2 mEq/L (elevated)
- Chloride (Cl): 98 mEq/L (normal)
- Bicarbonate (HCO₃): 22 mEq/L (normal)
Renal Function:
- Blood Urea Nitrogen (BUN): 25 mg/dL (elevated)
- Creatinine: 1.5 mg/dL (elevated)
- Glomerular Filtration Rate (GFR): 50 mL/min (stage 2 kidney disease)
Arterial Blood Gases (ABGs):
- pH: 7.25
- PaCO₂: 58 mmHg
- HCO₃: 22 mEq/L
- Capillary blood sugar 320 DG/l
what are the evaluations
- Fluid Volume Status: dizziness and fatigue improved with IV fluid administration, and she showed signs of improved hydration with better urine output.
- Electrolyte Imbalance: Sodium levels increased slightly after 24 hours of fluid replacement; potassium remained elevated, requiring close monitoring and adjustments to her diuretic regimen.
- Gas Exchange: Shortness of breath improved with supplemental oxygen, and O2 saturation increased to 96%.
- Skin Integrity: Swelling in the lower extremities was reduced with elevation and compression stockings, preventing further skin breakdown to prevent further electrolyte imbalances.